
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3 Department of Pharmacy, COMSATS University Islamabad, Abbottabad Campus, 22010, Pakistan
4 Department of Zoology, Hazara University, Mansehra, 21120, Pakistan
5 Shanxi Medical University, China
6,8 University Of Haripur, Haripur
7 Cloud Solutions Specialist – Microsoft, Karachi ,75500, Pakistan
Preterm birth (PTB) remains a leading cause of neonatal morbidity globally, with an etiology often linked to complex environmental and microbial interactions. This study aimed to evaluate the association between intrauterine microbial burden, virulent gene expression, and toxic heavy metal exposure in the pathogenesis of PTB. We analyzed placental tissue and dietary patterns to quantify exposure to heavy metals (Cu, Cd, Hg, Pb, Co) using atomic mass spectroscopy and estimated chronic daily intake (CDI) based on soil and dietary sources. Concurrently, polymerase chain reaction (PCR) was employed to detect specific pathogens (Escherichia coli, Staphylococcus aureus, Gardnerella vaginalis, Fusobacterium nucleatum, Ureaplasma parvum) and virulence genes (mecA, PVL, fadA). Risk assessment indicated elevated chronic exposure to Hg, Cd, Cu, Pb, and Co, with fish consumption showing a significant correlation with metal accumulation. Spectroscopic analysis of placental tissue confirmed high metal residues in PTB cases for all analyzed metals except Cd. Microbial screening identified the prevalence of pathogenic flora, including S. aureus, E. coli, G. vaginalis, F. nucleatum, and U. parvum. Virulence analysis detected the S. aureus mecA gene in both normal and PTB samples, while the F. nucleatum fadA adhesin gene was exclusively amplified in PTB samples. These findings suggest that cumulative exposure to toxic heavy metals, particularly through dietary intake, and colonization by virulent periodontal and urogenital pathogens contribute significantly to PTB etiology. This underscores the need for integrated prenatal screening for environmental toxins and microbial dysbiosis to mitigate PTB risks.
Preterm birth (PTB), defined as delivery before 37 completed weeks of gestation, constitutes a critical global health crisis. It affects approximately 15 million infants annually, representing a prevalence of 5–18% of live births worldwide [1] . PTB is not merely a singular obstetric event but a syndrome with severe short-term and long-term consequences, ranging from neonatal respiratory distress to permanent neurodevelopmental impairment [2] . As the leading cause of morbidity and mortality in children under five years of age, complications arising from prematurity account for approximately 35% of the world’s 3.1 million annual neonatal deaths [3] .
The burden of PTB is disproportionately distributed, with the highest rates observed in low-to-middle-income countries in Sub-Saharan Africa and South Asia [4] . Pakistan, specifically, ranks fourth globally in the number of preterm births, contributing significantly to the country’s high neonatal mortality rate of 49 per 1000 live births [5] . Despite these alarming statistics, the specific etiological drivers within this demographic remain under-explored, particularly regarding the interplay between environmental exposures and biological factors.
The etiology of PTB is multifactorial, involving a complex interaction of genetic, immunological, and environmental components. While traditional risk factors such as maternal hypertension, diabetes, and multiple gestations are well-documented [6] , recent research has pivoted toward the impact of anthropogenic environmental stressors. Pregnancy acts as a window of susceptibility where exposure to environmental pollutants can trigger adverse gestational outcomes through oxidative stress and endocrine disruption [7] .
Among environmental toxicants, heavy metals pose a significant threat due to their persistence and bioaccumulative nature. Metals such as cadmium (Cd), lead (Pb), mercury (Hg), and arsenic (As) are ubiquitous in the environment, originating from industrial emissions, contaminated water, and dietary sources [8] . These metals have been detected in placental tissue and cord blood, indicating their ability to breach the placental barrier.
Chronic exposure to these metals, even at low concentrations, can compromise the feto-maternal unit. For instance, cadmium accumulation in the placenta has been linked to structural damage and restricted nutrient transfer, while lead and mercury are known neurotoxicants that induce oxidative stress [9] . The accumulation of these toxins may sensitize the intrauterine environment, potentially lowering the threshold for other pathological processes, such as infection.
Parallel to environmental toxicity, microbial dysbiosis is a dominant factor in the pathogenesis of spontaneous PTB. Historically, the amniotic cavity was considered a sterile environment; however, advanced molecular techniques have revealed that the placenta and amniotic fluid harbor low-abundance but metabolically active microbiomes [10] . Dysbiosis, or the imbalance of these microbial communities, is strongly implicated in triggering premature labor.
The vaginal microbiome plays a sentinel role in maintaining reproductive health. A healthy vaginal ecosystem is dominated by Lactobacillus species, which produce lactic acid to inhibit pathogen growth [11] . The disruption of this balance leads to bacterial vaginosis (BV), characterized by the overgrowth of anaerobes such as Gardnerella vaginalis. This shift is consistently associated with an increased risk of ascending infection and preterm premature rupture of membranes (PPROM) [12] .
Beyond the vagina, specific opportunistic pathogens have been identified as high-risk agents for PTB. Escherichia coli, a common commensal of the gastrointestinal tract, can colonize the genitourinary system. Virulent strains of E. coli associated with extraintestinal infections have been isolated from cases of neonatal sepsis and chorioamnionitis, suggesting a direct link to premature delivery [13] .
Similarly, oral pathogens have emerged as unexpected contributors to intrauterine infection. Fusobacterium nucleatum, a gram-negative anaerobe prevalent in periodontal disease, possesses unique virulence factors such as the fadA adhesin. This adhesin allows the bacterium to bind to vascular endothelial cadherin, increasing permeability and enabling the translocation of bacteria from the maternal circulation to the placenta [14] .
Staphylococcus aureus and Ureaplasma parvum are also frequently implicated in adverse pregnancy outcomes. S. aureus is capable of biofilm formation on gestational tissues, utilizing alpha-hemolysin to disrupt cellular integrity [15] . Meanwhile, U. parvum, often found in the amniotic fluid of women delivering preterm, is associated with a robust inflammatory response that can precipitate early labor [16] .
Despite the established individual roles of heavy metal toxicity and microbial infection in PTB, there is a paucity of data examining these factors concurrently, particularly in high-burden regions like Pakistan. It is plausible that environmental pollutant exposure weakens the maternal immune defense or compromises placental integrity, thereby facilitating microbial invasion and colonization.
Currently, most studies focus on these variables in isolation. There is a critical need to characterize the specific pathogenic bacterial profiles and their virulence genes in the context of the local environmental "exposome." Understanding this relationship is vital for developing targeted prenatal screening and intervention strategies.
This study aims to bridge this knowledge gap by isolating and genotypically characterizing microorganisms associated with preterm delivery in Pakistani women. Furthermore, we seek to quantify the concurrent burden of toxic heavy metals and environmental stressors in this population to elucidate the potential multifaceted etiology of preterm birth.
2. MATERIAL AND METHODS:
2.1. Study Design and Population :
A case-control study was conducted involving women admitted to the Maternal and Child Health (MCH) units of the Pakistan Institute of Medical Sciences (PIMS) and Holy Family Hospital, Rawalpindi/Islamabad, during 2019. The study cohort comprised women delivering preterm (gestational age 24–36 weeks) with a history of preterm complications. The control group consisted of women with term deliveries (>37 weeks) and no history of adverse pregnancy outcomes.
Inclusion criteria for the case group were spontaneous or induced labor between 28 and 36 weeks. Exclusion criteria included premature rupture of membranes (PROM) or preterm PROM (PPROM) prior to labor, multiple gestations, intrauterine fetal death, fetal anomalies, and cesarean sections. Patients with a recent history of antibiotic use (excluding UTI or bacterial vaginosis treatment) were also excluded to prevent confounding of microbial data. Written informed consent was obtained from all participants. The study protocol was approved by the institutional ethical review board.
2.2. Data Collection and Clinical Sampling :
Demographic and clinical data were collected using a structured questionnaire, capturing maternal age, BMI, antibiotic history, dietary supplements, and environmental exposures (proximity to industrial zones, occupational hazards).
Clinical specimens, including high vaginal swabs and placental tissue, were collected under aseptic conditions. Vaginal swabs were obtained prior to delivery, while placental tissue was harvested immediately post-partum. Samples were transported in sterile containers; placental biopsies were preserved in RNAlater™ (Invitrogen, Thermo Fisher Scientific) for molecular analysis, while swabs were stored in transport media. All samples were maintained at -20°C until processing.
2.3. Microbiological Culturing and Identification :
Vaginal swabs were inoculated onto MacConkey agar (for Escherichia coli), Columbia Blood Agar, and Mannitol Salt Agar (MSA) (for Staphylococcus aureus) and incubated at 37°C. S. aureus was identified by observing hemolysis on blood agar and fermentation on MSA, confirmed by catalase, oxidase, and indole biochemical testing. Gram staining was performed for morphological verification. Stock cultures were preserved in Brain Heart Infusion (BHI) broth with 20% glycerol at -20°C.
2.4. Genomic DNA Extraction :
Genomic DNA was extracted from placental tissue and bacterial isolates. For placental tissue (20 mg), the WizPrep™ gDNA Mini Kit was employed according to the manufacturer’s instructions, involving proteinase K digestion and spin-column purification. For bacterial isolates and vaginal swabs, DNA was isolated using a modified ethanol precipitation method involving SDS lysis and proteinase K digestion, followed by solubilization in TE buffer.
2.5. Molecular Characterization of Pathogens :
PCR amplification was performed to identify specific pathogens and virulence factors using the primers listed in Table 1.
2.6. Heavy Metal Analysis :
2.6.1. Sample Digestion and Quantification
Placental tissue (1 g) was subjected to acid digestion using a (1:1 v/v) until a transparent solution was obtained. The digestate was filtered and diluted with deionized water. Concentrations of heavy metals (Cr, Cu, Pb, Hg, As) were quantified using Flame Atomic Absorption Spectrometry (FAAS) (Perkin-Elmer Analyst 200) equipped with single-element hollow cathode lamps.
2.6.2. Exposure Assessment
To assess chronic environmental exposure, the Estimated Daily Intake (EDI) of heavy metals via dietary sources (wheat, fish, meat, vegetables) and water was calculated using the following equation:
EDI= C x IR x EF x ED /BW x AT
EDI: Estimated Daily Intake (mg/kg/day)
C: Heavy metal concentration (mg/kg)
IR: Ingestion rate (mg/day)
EF: Exposure frequency (days/year)
ED: Exposure duration (years)
BW: Body weight (kg)
AT: Averaging time (days)
Table 2.1 : Molecular Characterization of Pathogens
|
Target Bacteria |
Gene |
Primer Sequence (5’–3’) |
Amplicon (bp) |
|
G. vaginalis |
16S rRNA |
F: TTACTGGTGTATCACTGTAAGG R: CCGTCACAGGCTGAACAGT |
331 |
|
F. nucleatum |
16S rRNA |
F: GGATTTATTGGGCGTAAAGC R: GGCATTCCTACAAATATCTACGAA |
163 |
|
fadA |
F: CAAATCAAGAAGAAGCAAGATTCAAT R: GCTTGAAGTCTTTGAGCTCT |
121 |
|
|
S. aureus |
mecA |
F: GTAGAAATGACTGAACGTCCGATAA R: CCAATTCCACATTGTTTCGGTCTAA |
310 |
|
PVL |
F: ATCATTAGGTAAAATGTCTGGACATGATCCA R: GCATCAAGTGTATTGGATAGCAAAAGC |
433 |
|
|
E. coli |
clbA |
F: AAGCCGTATCCTGCTCAAAA R: GCTTCTTTGAGCGTCCACAT |
342 |
|
clbQ |
F: GCACGATCGGACAGGTTAAT R: TAGTCTCGGAGGGATCATGG |
308 |
3. RESULTS :
3.1. Socio-demographic Determinants of Preterm Birth :
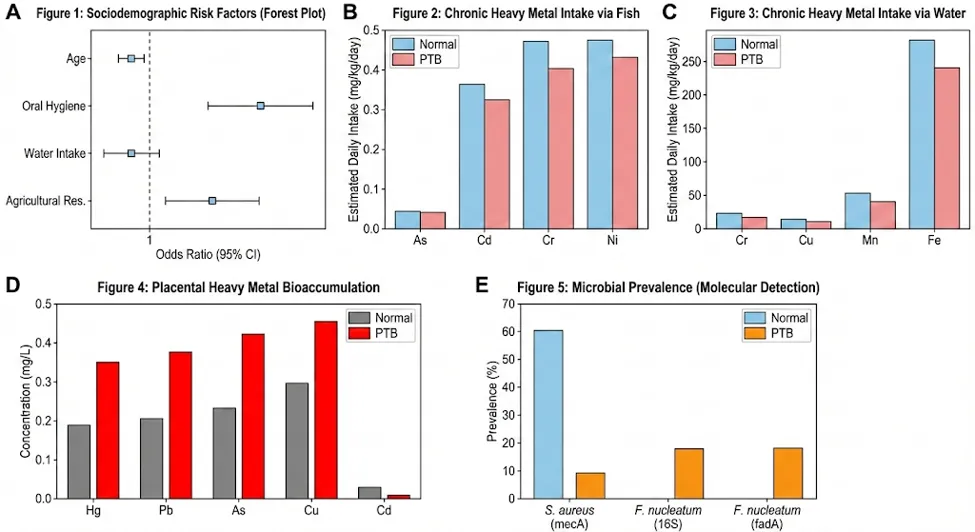
A binary logistic regression analysis was performed to evaluate the association between sociodemographic variables and the incidence of preterm birth (PTB). As presented in Table 2, maternal age (p < 0.001), socioeconomic status (p < 0.001), and oral hygiene (p < 0.001) emerged as the most significant predictors. Notably, residence in agricultural zones (p = 0.002) and daily water intake (p < 0.001) were statistically significant environmental contributors. Conversely, factors such as household structure, physical health, and previous history of preterm delivery did not show a statistically significant association in this cohort.
|
Variable |
Coefficient (β) |
Standard Error |
Wald Statistic |
P-value |
Significance (95% CI) |
|
Age |
-0.959 |
0.173 |
30.62 |
$< 0.001$ |
Significant |
|
Socio-economic Status |
-1.017 |
0.123 |
68.48 |
$< 0.001$ |
Significant |
|
Oral Hygiene |
1.281 |
0.135 |
89.60 |
$< 0.001$ |
Significant |
|
Education |
-0.257 |
0.072 |
12.84 |
$< 0.001$ |
Significant |
|
Water Intake (L) |
-0.464 |
0.095 |
23.95 |
$< 0.001$ |
Significant |
|
Agricultural Residence |
0.203 |
0.067 |
9.08 |
0.002 |
Significant |
|
Parity (No. of Children) |
-0.209 |
0.052 |
16.18 |
$< 0.001$ |
Significant |
|
Delivery Method |
-0.639 |
0.131 |
23.87 |
$< 0.001$ |
Significant |
|
Smoking |
0.300 |
0.213 |
1.98 |
0.160 |
NS |
|
UTI History |
-0.250 |
0.137 |
3.34 |
0.068 |
NS |
|
Household Structure |
0.319 |
0.175 |
3.31 |
0.069 |
NS |
|
Ethnicity |
-0.077 |
0.082 |
0.87 |
0.350 |
NS |
3.2. Assessment of Chronic Heavy Metal Exposure:
The Estimated Daily Intake (EDI) of heavy metals was quantified across multiple exposure pathways. The comparative analysis between term (normal) and PTB groups revealed distinct exposure profiles (Table 3).
|
Source |
Metal |
Mean EDI (Normal) |
Mean EDI (PTB) |
T-test (P-value) |
|
Wheat |
Cadmium (Cd) |
0.030 |
0.077 |
0.001 |
|
Mercury (Hg) |
0.020 |
0.028 |
0.038 |
|
|
Copper (Cu) |
0.263 |
0.335 |
0.044 |
|
|
Chromium (Cr) |
0.069 |
0.062 |
0.016 |
|
|
Fish |
Arsenic (As) |
0.502 |
0.437 |
$< 0.001$ |
|
Cadmium (Cd) |
6.211 |
5.403 |
$< 0.001$ |
|
|
Chromium (Cr) |
5.435 |
4.728 |
$< 0.001$ |
|
|
Nickel (Ni) |
7.855 |
6.833 |
$< 0.001$ |
|
|
Water |
Chromium (Cr) |
10.098 |
7.825 |
0.001 |
|
Copper (Cu) |
7.037 |
3.883 |
$< 0.001$ |
|
|
Manganese (Mn) |
59.569 |
45.119 |
0.002 |
|
|
Iron (Fe) |
293.025 |
253.489 |
0.002 |
|
|
Selenium (Se) |
0.678 |
0.507 |
0.007 |
3.3. Bioaccumulation in Placental Tissue:
Atomic Absorption Spectroscopy (AAS) analysis of placental tissue confirmed the bioaccumulation of toxic metals. As detailed in Table 4, the mean concentrations of mercury (Hg), lead (Pb), copper (Cu), and arsenic (As) were markedly higher in the placental tissues of women delivering preterm compared to term controls. Conversely, cadmium (Cd) levels appeared slightly lower in the PTB group in this specific subset.
|
Heavy Metal |
Normal (Term) Mean ± SD |
Preterm (PTB) Mean ± SD |
Trend in PTB |
|
Mercury (Hg) |
6.31 |
7.38 |
Elevated |
|
Lead (Pb) |
0.53 |
0.75 |
Elevated |
|
Arsenic (As) |
1.15 |
1.92 |
Elevated |
|
Copper (Cu) |
0.27 |
0.53 |
Elevated |
|
Cadmium (Cd) |
0.019 |
0.016 |
Lower |
3.4. Microbial Identification and Virulence Profiling :
3.4.1. Culture and Biochemical Characterization :
Bacterial culturing of vaginal swabs and placental tissue yielded positive growth on Columbia Blood Agar (CBA) and Mannitol Salt Agar (MSA) for a subset of samples. Isolates presenting as Gram-positive cocci in clusters, catalase-positive, and exhibiting beta-hemolysis on CBA and mannitol fermentation on MSA were presumptively identified as Staphylococcus aureus (Figure 1). Culture on MacConkey agar for Escherichia coli was negative for all samples.
3.4.2. Molecular Detection of Pathogens:
PCR amplification of the 16S rRNA gene and specific virulence factors provided definitive identification of microbial isolates (Figure 2).
|
Target Organism |
Gene Target |
Normal Group (n=5) |
PTB Group (n=11) |
Outcome |
|
Staphylococcus aureus |
mecA |
Positive (3/5) |
Positive (1/11) |
MRSA trait detected in both groups |
|
PVL |
Negative |
Negative |
Virulence factor not detected |
|
|
Fusobacterium nucleatum |
16S rRNA |
Negative |
Positive (2/11) |
Exclusive to PTB |
|
fadA |
Negative |
Positive (2/11) |
Virulence factor confirmed |
|
|
Gardnerella vaginalis |
16S rRNA |
Negative |
Negative |
Not detected |
|
Ureaplasma parvum |
16S rRNA |
Negative |
Negative |
Not detected |
|
Escherichia coli |
clbA / clbQ |
Negative |
Negative |
Colibactin genes not detected |
DISCUSSION:
Preterm birth (PTB) remains complex syndrome with a multifactorial etiology, disproportionately affecting developing nations like Pakistan. This study provides a novel, integrated assessment of the environmental "exposome" and microbial virulence factors contributing to PTB. Our principal finding is the identification of a potential "double-hit" mechanism: chronic bioaccumulation of toxic heavy metals (specifically Mercury, Lead, and Arsenic) combined with placental invasion by virulent Fusobacterium nucleatum and Methicillin-Resistant Staphylococcus aureus (MRSA).
Our logistic regression analysis initially highlighted oral hygiene and agricultural residence as critical determinants of PTB. The strong association with poor oral hygiene supports the "focal infection theory," where periodontal pathogens enter the systemic circulation pathway we confirmed via the detection of oral bacteria in the placenta. Furthermore, the significance of agricultural residence aligns with our environmental findings. In Pakistan, untreated industrial effluents are frequently used for irrigation, leading to the bioaccumulation of heavy metals in soil and crops. This creates a direct route of exposure for pregnant women living in these zones, significantly increasing their toxic burden compared to urban counterparts.
A disturbing finding of this study is the high Estimated Daily Intake (EDI) of heavy metals through dietary fish and drinking water. While fish is a vital source of omega-3 fatty acids, our data suggests that in this region, it serves as a vehicle for Mercury (Hg) and Chromium (Cr) toxicity. This is consistent with global findings regarding neurotoxic accumulation in the fetus. Crucially, our placental tissue analysis confirms that these metals are crossing the placental barrier. We observed significantly elevated levels of Hg, As, and Pb in preterm placentas compared to term controls. The high placental load of Mercury is particularly alarming, as it is a potent inducer of oxidative stress; it depletes placental glutathione peroxidase, leading to mitochondrial dysfunction and trophoblast apoptosis, which can trigger premature labor. Similarly, Chromium exposure linked to water intake is known to induce DNA damage and inflammation in gestational tissues, potentially sensitizing the uterus to contraction.
While heavy metals compromise placental integrity, microbial infection appears to be a definitive trigger. We report the exclusive detection of Fusobacterium nucleatum in preterm cases. F. nucleatum is an oral commensal, and its presence in the placenta strongly supports hematogenous translocation from the oral cavity, consistent with our sociodemographic finding regarding poor oral hygiene. Most significantly, we identified the virulence gene fadA in these isolates. The FadA adhesin is a critical virulence factor that binds to vascular endothelial cadherin (VE-cadherin), loosening cell-to-cell junctions. This "unlocking" of the endothelial barrier likely facilitates the bacteria's crossing from maternal blood into the amniotic space. We also detected the mecA gene in vaginal and placental S. aureus samples, indicating the presence of MRSA. While S. aureus was found in both term and preterm groups, its presence in the reproductive tract poses a severe risk for neonatal sepsis and suggests that standard prophylactic antibiotics may be insufficient for these patients.
We propose a synergistic relationship between these environmental and microbial factors. Heavy metals like Cadmium and Mercury are known to weaken the integrity of the placental barrier and impair macrophage function. It is biologically plausible that this metal-induced immunotoxicity creates a "permissive" environment, making it easier for opportunistic pathogens like F. nucleatum (via fadA) to invade the placenta and trigger the inflammatory cascade leading to labor. This study identifies a distinct pathogenic profile for preterm birth in Pakistan, characterized by high environmental heavy metal exposure and specific microbial invasion. The detection of the fadA gene in preterm placentas underscores the need for integrated prenatal care that includes periodontal health screening and environmental toxin monitoring. Public health strategies must address water quality and dietary safety to mitigate these preventable risks.
CONCLUSION
This study elucidates a multifactorial etiology for preterm birth (PTB) in the Pakistani population, characterized by a synergistic burden of environmental toxicity and microbial infection. We identified a significant correlation between chronic dietary exposure to heavy metals specifically Mercury, Arsenic, and Chromium via fish and water consumption and their subsequent bioaccumulation in placental tissue. Concurrently, molecular profiling revealed the exclusive presence of Fusobacterium nucleatum harboring the virulent fadA adhesin gene in preterm placentas, alongside the detection of Methicillin-Resistant Staphylococcus aureus (MRSA) carrying the mecA gene. These findings suggest that metal-induced compromise of the placental barrier may facilitate invasion by opportunistic periodontal and urogenital pathogens. Consequently, effective PTB prevention strategies must integrate environmental biomonitoring with targeted screening for periodontal health and specific microbial biomarkers like fadA. Future longitudinal studies are warranted to establish the precise toxicological thresholds that trigger this pathogenic cascade.
REFERENCES





Sarah Malik, Raja Waleed Sajjad, Sundus Javed, Saba Manzoor, Moazzam Ali Malik, Dr. Khalil Ahmed Hashmi, Raja Ahmed Sajjad, Dr. Jaweria Hashmi, Analysis of Environmental and Microbial Determinants of Preterm Birth in Pakistani Woman, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 3584-3593. https://doi.org/10.5281/zenodo.21423622
 10.5281/zenodo.21423622
10.5281/zenodo.21423622