
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Assistant Professor, Gawande College of Pharmacy, Sakharkherda, Buldhana
2Department of Pharmacology, Institute of Pharmaceutical Education and Research, Borgaon meghe, Wardha.
Pharmacovigilance has evolved from a predominantly manual process of adverse drug reaction (ADR) monitoring to a data-driven discipline that increasingly relies on artificial intelligence (AI) and real-world evidence (RWE). The growing volume of safety reports, electronic health records, insurance claims, biomedical literature, social media content, and wearable device data has challenged conventional pharmacovigilance systems, necessitating more efficient computational approaches. AI technologies, including machine learning, deep learning, natural language processing, large language models, and explainable AI, have demonstrated considerable potential for automating case processing, identifying safety signals, improving adverse event coding, and supporting benefit–risk assessment. Simultaneously, RWE derived from routine clinical practice provides complementary insights into long-term drug safety across diverse patient populations that are often underrepresented in clinical trials. The integration of AI with RWE enables earlier detection of rare adverse events, strengthens regulatory decision-making, and facilitates personalized drug safety monitoring. Despite these advances, several challenges remain, including data heterogeneity, algorithmic bias, limited model interpretability, privacy concerns, and the absence of globally harmonized regulatory frameworks. Emerging technologies such as multimodal AI, federated learning, digital twins, and generative AI are expected to further transform pharmacovigilance by enabling scalable, transparent, and patient-centered safety surveillance. This review summarizes the evolution of AI-driven pharmacovigilance, explores current applications of AI and RWE across the drug safety lifecycle, discusses regulatory and ethical considerations, highlights existing research gaps, and outlines future directions for next-generation pharmacovigilance systems
1.1 Evolution of Pharmacovigilance
Pharmacovigilance is the science and practice of detecting, assessing, understanding, and preventing adverse effects or any other medicine-related problems. Since the establishment of international drug safety programs following the thalidomide tragedy, pharmacovigilance has become a fundamental component of public health. Traditional pharmacovigilance primarily relied on spontaneous adverse drug reaction (ADR) reporting by healthcare professionals and patients. Although spontaneous reporting systems remain the cornerstone of post-marketing surveillance, they are frequently affected by underreporting, delayed submissions, incomplete clinical information, and reporting bias. These limitations reduce the efficiency of conventional safety monitoring, particularly for rare adverse events and newly marketed medicines.
The rapid expansion of healthcare data, together with advances in digital technologies, has transformed pharmacovigilance into a data-intensive discipline. Electronic health records, health insurance claims, patient registries, clinical trial databases, biomedical literature, wearable devices, and social media platforms now generate large volumes of real-world health information that complement traditional reporting systems. Consequently, modern pharmacovigilance has shifted toward continuous, evidence-driven safety surveillance supported by computational analytics and artificial intelligence. This transition has created opportunities for earlier signal detection, improved causality assessment, and more comprehensive evaluation of medicine safety across diverse patient populations1.
1.2 Digital Transformation of Pharmacovigilance
The digitalization of healthcare has fundamentally changed how drug safety information is generated, collected, and analyzed. Traditional pharmacovigilance relied heavily on spontaneous reporting systems, which remain valuable but often suffer from underreporting and delayed signal identification (1,2). The widespread adoption of electronic health records, insurance claims databases, patient registries, and digital health platforms has created unprecedented opportunities for continuous safety monitoring across large and diverse populations.
Modern pharmacovigilance increasingly incorporates real-world data obtained during routine clinical practice. These data sources provide insights into medicine use in populations that are frequently underrepresented in randomized clinical trials, including elderly individuals, patients with multiple comorbidities, and those receiving complex drug combination. As a result, digital pharmacovigilance has evolved from a passive reporting model to a proactive surveillance system capable of identifying emerging safety concerns earlier in the product lifecycle2.
1.3 Artificial Intelligence in Healthcare
Artificial intelligence (AI) refers to computational methods that enable machines to perform tasks traditionally requiring human intelligence, including pattern recognition, prediction, language processing, and decision support. In healthcare, AI has demonstrated substantial potential in diagnostics, medical imaging, clinical decision-making, and drug development.
In pharmacovigilance, machine learning and deep learning algorithms can analyze large volumes of structured and unstructured data to identify adverse event patterns that may be difficult to detect through conventional methods (8). Natural language processing (NLP) has become particularly important because a large proportion of safety information is contained within free-text narratives, clinical notes, and biomedical literature (9). Recent advances in large language models and generative AI have further expanded the possibility of automating case processing, literature screening, and safety signal prioritization while maintaining human oversight3.
1.4 Real-World Evidence in Drug Safety
Real-world evidence (RWE) refers to clinical evidence regarding the use, benefits, or risks of medical products derived from real-world data. Regulatory agencies such as the
U.S. Food and Drug Administration and the European Medicines Agency increasingly recognize the value of RWE in supporting post-marketing safety evaluations and regulatory decision-making.
RWE is particularly useful for detecting rare adverse events, evaluating long-term safety outcomes, and assessing drug performance in heterogeneous patient populations. By integrating AI with RWE, pharmacovigilance systems can process millions of healthcare records, identify temporal associations, and generate hypotheses for further clinical and epidemiological investigation. This integration represents a major step toward personalized and continuously learning drug safety systems4.
1.5 Scope of the Review
This review provides a comprehensive overview of AI-driven pharmacovigilance with a focus on the integration of real-world evidence for next-generation drug safety. The review discusses the evolution of pharmacovigilance, major AI technologies, real-world data sources, applications across the pharmacovigilance workflow, regulatory considerations, ethical challenges, emerging trends, research gaps, and future perspectives. Particular emphasis is placed on explainable AI, multimodal AI, federated learning, and generative AI, which are increasingly shaping the future of pharmacovigilance research and practice5.
2. EVOLUTION OF PHARMACOVIGILANCE
2.1 Traditional Pharmacovigilance
Pharmacovigilance has evolved considerably since the establishment of global drug safety monitoring systems following the thalidomide tragedy. For several decades, post-marketing surveillance depended primarily on spontaneous reporting systems (SRS), where healthcare professionals, pharmaceutical companies, and patients voluntarily submitted adverse drug reaction (ADR) reports. Databases such as the FDA Adverse Event Reporting System (FAERS), the WHO Programme for International Drug Monitoring (VigiBase), and EudraVigilance became the foundation of global drug safety surveillance. Although these systems remain indispensable, they are frequently affected by underreporting, duplicate reports, incomplete clinical information, delayed reporting, and reporting bias, limiting their ability to detect rare or emerging safety signals promptly. These limitations stimulated the development of more advanced pharmacovigilance approaches6.
2.2 Transition to Digital Pharmacovigilance
The widespread adoption of electronic healthcare systems has transformed pharmacovigilance into a data-intensive discipline. Electronic health records, insurance claims databases, clinical registries, biomedical literature, wearable devices, and patient-generated health data now complement spontaneous reporting systems by providing longitudinal information from routine clinical practice. These real-world data sources enable continuous monitoring of medicine safety across diverse patient populations and improve the identification of uncommon adverse events that may not become apparent during pre-marketing clinical trials. Digital pharmacovigilance therefore supports a more proactive approach to post-marketing surveillance by integrating heterogeneous healthcare data into routine safety assessment7.
2.3 Emergence of Artificial Intelligence in Pharmacovigilance
The exponential growth of healthcare data has exceeded the capacity of conventional manual pharmacovigilance workflows. Artificial intelligence has emerged as an effective solution for managing large-scale safety information through automation and predictive analytics. Machine learning algorithms can identify hidden relationships within structured datasets, while deep learning models recognize complex patterns associated with adverse drug reactions. Natural language processing enables automated extraction of clinically relevant information from case narratives, electronic medical records, scientific literature, and social media. These technologies substantially reduce manual workload while improving the consistency and speed of safety assessments8.
2.4 Current Landscape: AI-Driven Pharmacovigilance
Contemporary pharmacovigilance is shifting from reactive signal detection toward intelligent, continuous safety surveillance. AI applications now support multiple pharmacovigilance activities, including individual case safety report processing, MedDRA coding, duplicate detection, signal detection, literature screening, causality assessment, and benefit–risk evaluation. The integration of AI with real-world evidence further strengthens regulatory decision-making by enabling the analysis of large and heterogeneous healthcare datasets. Importantly, regulatory agencies continue to emphasize that AI should complement rather than replace expert clinical judgment, with human oversight remaining essential for high-impact safety decisions9.
2.5 Future Evolution Toward Next-Generation Pharmacovigilance
Next-generation pharmacovigilance is expected to combine explainable artificial intelligence, multimodal foundation models, federated learning, digital health technologies, and real-world evidence into an integrated safety ecosystem. Explainable AI addresses the "black-box" nature of complex algorithms by providing transparent and interpretable predictions that improve clinician and regulator confidence. Emerging regulatory frameworks increasingly emphasize transparency, traceability, fairness, and continuous performance monitoring for AI systems used in pharmacovigilance. These developments are expected to enable earlier signal detection, personalized safety monitoring, and more efficient regulatory decision-making while maintaining patient safety and public trust10.
3. ARTIFICIAL INTELLIGENCE TECHNOLOGIES IN PHARMACOVIGILANCE
Artificial intelligence (AI) has become a transformative technology in pharmacovigilance by enabling automated analysis of large, heterogeneous healthcare datasets. Unlike conventional statistical approaches, AI algorithms can recognize complex relationships among drugs, patient characteristics, clinical outcomes, and adverse drug reactions (ADRs). Current pharmacovigilance systems increasingly employ machine learning, deep learning, natural language processing (NLP), knowledge graphs, and explainable AI to improve the efficiency and accuracy of safety surveillance. Recent reviews indicate that AI applications are expanding beyond signal detection to support data ingestion, case processing, literature surveillance, and regulatory decision-making11.
3.1 Machine Learning
Machine learning (ML) is the most widely applied AI approach in pharmacovigilance. ML algorithms learn patterns from historical safety data and generate predictions without explicit programming. Supervised learning models such as random forests, support vector machines, logistic regression, and gradient boosting are commonly used for adverse event classification, duplicate case identification, and signal prioritization. Unsupervised learning methods facilitate clustering of similar safety reports and detection of unexpected drug-event associations. Compared with traditional disproportionality analysis, ML models can integrate multiple clinical variables simultaneously, improving predictive performance in complex datasets12.
3.2 Deep Learning
Deep learning employs multilayer neural networks to identify complex nonlinear relationships within large datasets. These models are particularly effective for extracting information from electronic health records, biomedical literature, medical images, and free-text case narratives. Architectures such as recurrent neural networks, long short-term memory networks, convolutional neural networks, and Transformer-based models have improved adverse drug event extraction and clinical text analysis. Recent benchmark studies consistently report superior performance of Transformer models, particularly BERT-based architectures, for named-entity recognition and relation extraction in pharmacovigilance13.
3.3 Natural Language Processing
A substantial proportion of pharmacovigilance information exists as unstructured text, including Individual Case Safety Reports (ICSRs), discharge summaries, physician notes, scientific publications, and social media posts. NLP converts these narratives into structured clinical information by identifying drugs, adverse events, indications, and temporal relationships. Automated NLP pipelines substantially reduce manual review while improving consistency in adverse event coding and literature screening. Systematic reviews have demonstrated that NLP can effectively complement traditional spontaneous reporting systems by identifying ADRs from user-generated online content and clinical narratives14.
3.4 Large Language Models and Generative AI
Large Language Models (LLMs) represent the latest advancement in AI-driven pharmacovigilance. These foundation models can summarize clinical documents, support literature surveillance, assist in MedDRA coding, draft case narratives, and facilitate safety report review. Generative AI also has potential to automate routine pharmacovigilance workflows and improve knowledge retrieval from extensive biomedical literature. Nevertheless, hallucinated outputs, limited transparency, and regulatory concerns necessitate rigorous human oversight before clinical implementation. Current regulatory discussions emphasize validation, documentation, and expert review for all AI-assisted pharmacovigilance activities15.
3.5 Knowledge Graphs
Knowledge graphs integrate information from multiple biomedical resources by representing relationships among drugs, diseases, genes, proteins, and adverse events. These graph-based frameworks improve the identification of indirect safety associations that may remain undetected using isolated datasets. Knowledge graphs also facilitate causal inference, drug repurposing studies, and mechanistic interpretation of adverse drug reactions by combining structured and unstructured biomedical knowledge.
3.6 Explainable Artificial Intelligence
Although advanced AI models often achieve excellent predictive performance, many operate as “black-box” systems with limited interpretability. Explainable Artificial Intelligence (XAI) addresses this limitation by providing transparent explanations for model predictions. Techniques such as SHAP and LIME quantify the contribution of individual variables to predicted adverse outcomes, allowing clinicians and regulators to understand why a safety signal was generated. Improved explainability enhances confidence in AI-assisted regulatory decision-making and supports responsible adoption of AI within pharmacovigilance16.
3.7 Graph Neural Networks
Graph Neural Networks (GNNs) extend conventional graph-based analysis by learning complex interactions among biomedical entities. GNNs have demonstrated promising applications in predicting drug–drug interactions, identifying previously unknown adverse drug reactions, and modeling biological networks. Their ability to incorporate molecular, clinical, and pharmacological information simultaneously makes them valuable for next-generation pharmacovigilance research, although routine regulatory implementation remains limited17.
3.8 Agentic AI: An Emerging Paradigm
Agentic AI represents an emerging class of intelligent systems capable of autonomously performing sequential pharmacovigilance tasks under predefined human supervision. Future agentic systems may automatically retrieve safety reports, screen biomedical literature, prioritize safety signals, generate preliminary regulatory summaries, and recommend follow-up analyses. Despite its considerable potential, this technology remains in its early stages, and robust governance, validation, cybersecurity, and regulatory oversight will be essential before widespread adoption in pharmacovigilance practice18.
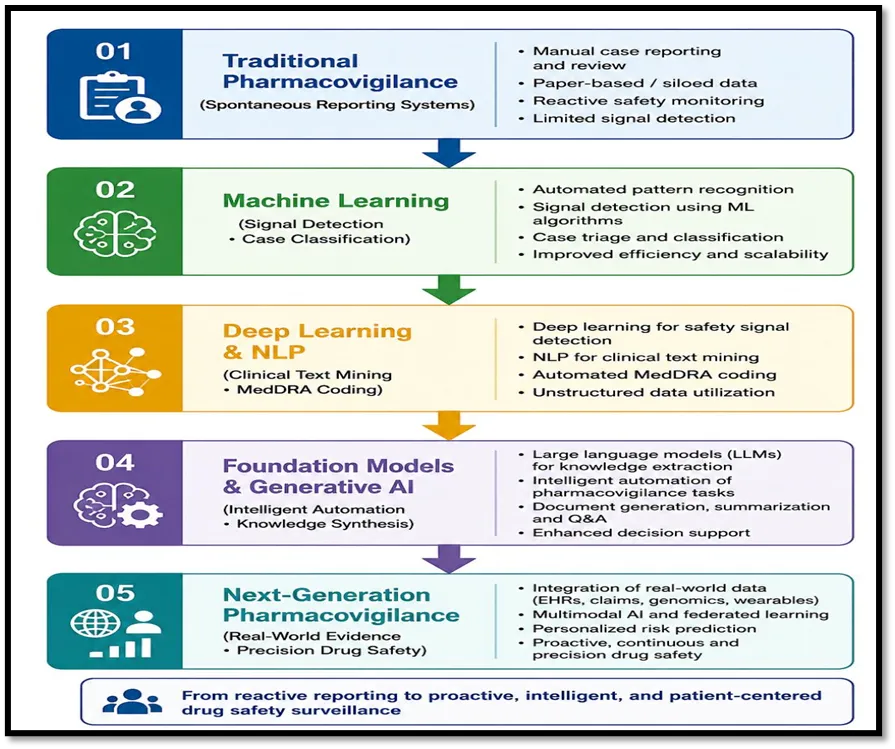
Fig No. 1 Evolution of AI in Pharmacovigilance
4. DATA SOURCES FOR AI-DRIVEN PHARMACOVIGILANCE
High-quality data are fundamental to the performance of artificial intelligence (AI) in pharmacovigilance. AI algorithms rely on diverse healthcare datasets to detect adverse drug reactions (ADRs), identify safety signals, evaluate benefit–risk profiles, and support regulatory decision-making. No single data source is sufficient to capture all safety events; therefore, integrating multiple real-world data sources provides a more comprehensive understanding of drug safety throughout the product lifecycle. Recent advances in data integration and interoperability have further strengthened AI-driven pharmacovigilance by enabling continuous learning from heterogeneous clinical environments19.
4.1 Spontaneous Reporting Systems
Spontaneous reporting systems (SRS) remain the cornerstone of global pharmacovigilance. Major databases, including the WHO Programme for International Drug Monitoring (VigiBase), the U.S. FDA Adverse Event Reporting System (FAERS), and EudraVigilance, collect millions of Individual Case Safety Reports (ICSRs) submitted by healthcare professionals, pharmaceutical companies, and patients. These databases are widely used for statistical signal detection and regulatory safety assessment.
AI techniques, particularly machine learning and natural language processing (NLP), improve the analysis of spontaneous reports by automating duplicate detection, identifying missing information, prioritizing safety signals, and supporting MedDRA coding. Nevertheless, underreporting, incomplete case narratives, reporting bias, and variable data quality remain significant limitations of spontaneous reporting systems20.
4.2 Electronic Health Records
Electronic Health Records (EHRs) provide longitudinal clinical information, including diagnoses, laboratory findings, medication history, imaging results, and physician notes. Compared with spontaneous reports, EHRs offer richer clinical context and enable the evaluation of temporal relationships between drug exposure and adverse events.
AI-driven analysis of EHRs facilitates early detection of rare ADRs, identification of high-risk patient populations, and assessment of long-term treatment outcomes. Deep learning and NLP algorithms are increasingly used to extract clinically relevant information from structured and unstructured HER data, improving pharmacovigilance efficiency and supporting personalized drug safety monitoring21.
4.3 Administrative Claims Databases
Administrative claims databases contain healthcare utilization information, including prescription records, hospital admissions, outpatient visits, diagnostic procedures, and reimbursement claims. These datasets provide valuable information on medicine utilization patterns across large populations.
Although claims databases contain limited clinical detail, their extensive population coverage makes them particularly useful for pharmacoepidemiological studies, comparative safety analyses, and evaluation of rare adverse events. AI algorithms enhance these analyses by identifying complex associations and reducing manual data processing22.
4.4 Biomedical Literature
Scientific publications remain an essential source of emerging drug safety information. Thousands of pharmacovigilance-related articles are published annually, making manual literature surveillance increasingly challenging.
Natural language processing and large language models can automatically screen biomedical literature, extract adverse event information, identify drug–event relationships, and prioritize publications requiring expert review. Automated literature surveillance substantially reduces workload while maintaining comprehensive safety monitoring23.
4.5 Social Media and Patient-Generated Data
Patients increasingly share medication experiences through social media platforms, online forums, health communities, and mobile applications. These platforms provide valuable real-world insights into medication tolerability, treatment adherence, and patient-reported adverse events.
AI-powered NLP techniques can identify potential ADRs from informal language and detect emerging safety concerns before they are widely reported through conventional pharmacovigilance systems. However, misinformation, inconsistent terminology, duplicate content, and uncertainty regarding clinical validity require careful interpretation and human verification24.
4.6 Wearable Devices and Digital Health Technologies
Wearable sensors, smartwatches, and remote monitoring devices continuously generate physiological measurements such as heart rate, blood pressure, electrocardiographic signals, physical activity, oxygen saturation, and sleep patterns.
These digital health technologies support continuous safety monitoring by enabling early detection of physiological changes associated with adverse drug reactions. AI algorithms analyze these high-frequency data streams to identify abnormal trends and provide near real-time safety surveillance, particularly for cardiovascular and metabolic therapies25.
4.7 Genomic and Multi-Omics Data
Advances in genomics, transcriptomics, proteomics, metabolomics, and other omics technologies have expanded opportunities for precision pharmacovigilance. Integration of multi-omics data with clinical information improves understanding of biological mechanisms underlying ADRs and supports identification of genetic susceptibility factors.
Machine learning models combining genomic biomarkers with real-world clinical data may facilitate individualized risk prediction and personalized medication safety strategies26.
4.8 Patient Registries and Disease-Specific Databases
Patient registries collect standardized longitudinal data for individuals with specific diseases or receiving particular therapies. These databases provide valuable evidence regarding long-term safety, treatment effectiveness, and rare adverse events that may not be captured during clinical trials.
AI-assisted analysis of registry data enables risk stratification, subgroup identification, and evaluation of medicine safety in vulnerable populations such as pediatric, geriatric, pregnant, and oncology patients27.
4.9 Integration of Real-World Evidence
The integration of multiple real-world data sources represents the foundation of next-generation pharmacovigilance. AI enables simultaneous analysis of spontaneous reports, EHRs, claims data, literature, wearable device outputs, patient registries, and genomic information to generate a more comprehensive assessment of medicine safety.
This integrated approach enhances signal detection, improves causal inference, supports regulatory decision-making, and facilitates continuous benefit–risk evaluation throughout the product lifecycle. As interoperability standards and data governance frameworks continue to evolve, integrated real-world evidence is expected to become a central component of future AI-enabled pharmacovigilance systems28.
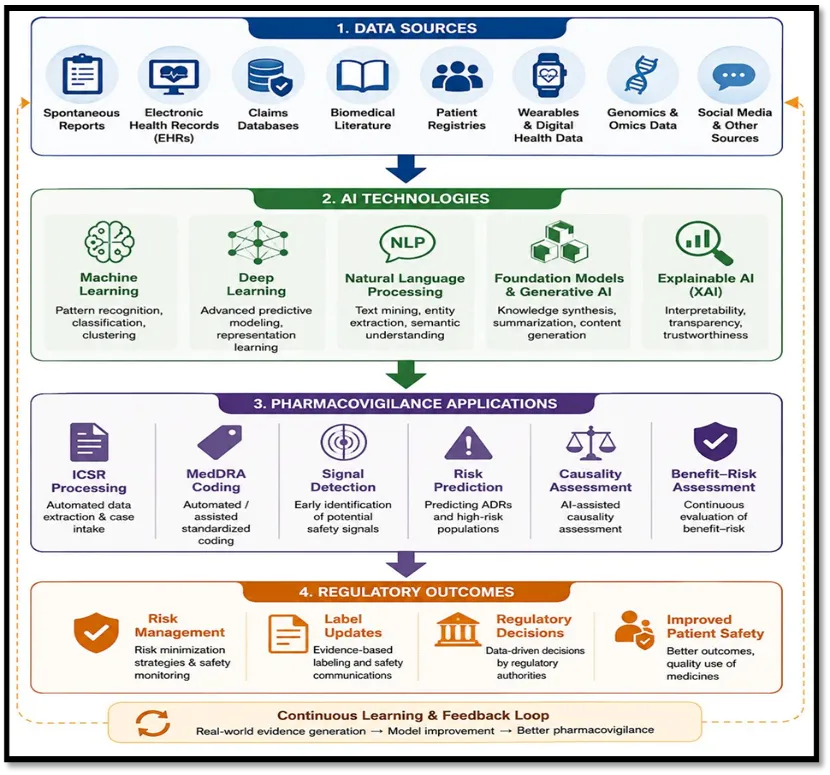
Fig No. 2 AI Driven Pharmacovigilance Ecosystem
5. AI APPLICATIONS ACROSS THE PHARMACOVIGILANCE WORKFLOW
Artificial intelligence (AI) is transforming the pharmacovigilance workflow by automating repetitive tasks, improving data quality, and enabling faster identification of potential safety concerns. Unlike conventional pharmacovigilance, which relies heavily on manual review, AI supports continuous analysis of structured and unstructured data from multiple sources. These technologies improve operational efficiency while allowing pharmacovigilance professionals to focus on expert evaluation and regulatory decision-making. Importantly, AI is intended to augment rather than replace human expertise, particularly for high-impact clinical and regulatory decisions29.
5.1 Individual Case Safety Report (ICSR) Processing
Individual Case Safety Reports (ICSRs) form the foundation of post-marketing drug safety surveillance. Manual processing of ICSRs is time-consuming because each report requires validation, data extraction, coding, medical review, and regulatory assessment.
Machine learning and natural language processing (NLP) automate several stages of ICSR processing by extracting relevant patient information, identifying suspected drugs and adverse events, verifying report completeness, and organizing data into structured formats. Automated workflows reduce processing time, improve consistency, and minimize transcription errors while maintaining compliance with regulatory requirements. Human review remains essential for complex cases requiring clinical judgment30.
5.2 Automated MedDRA Coding
Accurate coding of adverse events using the Medical Dictionary for Regulatory Activities (MedDRA) is a critical component of pharmacovigilance. Manual coding is labor-intensive and may result in variability between reviewers.
AI-based NLP systems recognize clinical terminology within case narratives and automatically assign appropriate MedDRA terms. Continuous model training improves coding accuracy while reducing manual workload. Automated coding also enhances data standardization, facilitating more reliable signal detection across global pharmacovigilance databases31.
5.3 Case Prioritization and Triage
The increasing volume of safety reports presents significant operational challenges for pharmacovigilance centers. AI algorithms classify incoming reports according to clinical seriousness, expectedness, data completeness, and regulatory priority.
Risk-based prioritization enables pharmacovigilance teams to rapidly identify reports requiring immediate expert assessment, thereby improving resource allocation and reducing delays in regulatory reporting. Intelligent triage systems are particularly valuable during public health emergencies when large numbers of safety reports are submitted within a short period32.
5.4 Duplicate Detection
Duplicate reports frequently occur when the same adverse event is submitted by multiple reporters or through different reporting pathways. Duplicate cases may distort statistical analyses and increase manual review workload.
Machine learning models compare demographic information, drug exposure, event descriptions, dates, and clinical characteristics to identify probable duplicate reports. Automated duplicate detection improves database quality and strengthens the reliability of signal detection analyses33.
5.5 AI-Assisted Signal Detection
Signal detection remains one of the most important applications of AI in pharmacovigilance. Conventional disproportionality methods are effective but may overlook complex relationships within large healthcare datasets.
Machine learning algorithms integrate information from spontaneous reports, electronic health records, biomedical literature, and real-world data to identify emerging safety signals more efficiently. Deep learning models further improve detection by recognizing nonlinear associations that may not be apparent using traditional statistical approaches. Earlier signal identification supports timely regulatory interventions and enhances patient safety34.
5.6 Literature Surveillance
Continuous monitoring of biomedical literature is required to identify newly reported adverse drug reactions and emerging safety concerns. Manual literature review is increasingly difficult because of the rapid growth in scientific publications.
Natural language processing and large language models automate literature screening by identifying relevant publications, extracting adverse event information, summarizing key findings, and prioritizing articles for expert review. These technologies improve surveillance efficiency while maintaining comprehensive coverage of published evidence34.
5.7 Causality Assessment
Determining whether a medicine is responsible for an adverse event remains one of the most challenging aspects of pharmacovigilance. Traditional causality assessment methods depend largely on expert clinical evaluation.
AI supports causality assessment by integrating multiple sources of evidence, including patient characteristics, medication history, laboratory findings, temporal associations, previous reports, and published literature. Although AI improves analytical consistency, final causality assessment continues to require clinical expertise and regulatory judgment35.
5.8 Benefit–Risk Assessment
Benefit–risk evaluation integrates evidence regarding medicine efficacy and safety throughout the product lifecycle. AI facilitates benefit–risk assessment by simultaneously analyzing diverse clinical and real-world datasets.
Predictive models identify patient populations with increased susceptibility to adverse reactions while estimating expected therapeutic benefits. These analyses support personalized treatment decisions and evidence-based regulatory evaluations36.
5.9 Regulatory Reporting and Compliance
Global regulatory authorities require timely submission of safety information in accordance with established pharmacovigilance guidelines. AI-assisted automation improves regulatory compliance by supporting case validation, document preparation, quality control, and submission workflows.
Automated systems reduce administrative burden, minimize reporting errors, and improve consistency across international pharmacovigilance operations. Nevertheless, regulatory agencies emphasize that final regulatory decisions must remain under qualified human supervision37.
5.10 Clinical Decision Support
AI-enabled pharmacovigilance increasingly contributes to clinical decision support systems integrated within electronic health records. These systems generate real-time alerts regarding potential adverse drug reactions, drug–drug interactions, contraindications, and individualized patient risks.
Clinical decision support enhances medication safety by providing healthcare professionals with evidence-based recommendations at the point of care. Integration of pharmacogenomic information and real-world evidence further strengthens individualized prescribing and precision pharmacovigilance38.
Table No. 1 AI Technologies in Pharmacovigilance
|
AI technology |
Key application |
Major benefit |
|
Machine Learning |
Signal detection |
Early ADR identification |
|
Deep Learning |
ADR prediction |
Improved accuracy |
|
NLP |
Literature & ICSR processing |
Workflow automation |
|
Generative AI/LLMs |
Safety narratives, report drafting |
Intelligent documentation |
|
Explainable AI |
Decision support |
Transparent predictions |
|
Federated Learning |
Multi-center data analysis |
Privacy-preserving AI |
6. MULTIMODAL AI, FOUNDATION MODELS, AND GENERATIVE AI IN NEXT-GENERATION PHARMACOVIGILANCE
Artificial intelligence (AI) is rapidly evolving beyond traditional machine learning toward foundation models capable of processing multiple data modalities simultaneously. These models integrate structured clinical data, free-text narratives, laboratory findings, medical images, genomic information, and real-world evidence (RWE) to provide a more comprehensive understanding of drug safety. Compared with earlier AI systems designed for single tasks, foundation models support multiple pharmacovigilance activities within a unified framework, improving efficiency and facilitating continuous learning. Recent evidence suggests that multimodal and generative AI have the potential to transform pharmacovigilance workflows, although robust validation, transparency, and regulatory oversight remain essential39.
6.1 Foundation Models in Pharmacovigilance
Foundation models are large AI systems trained on extensive biomedical and clinical datasets before being adapted to specific downstream tasks. Their ability to learn generalized representations enables application across diverse pharmacovigilance activities, including case processing, literature surveillance, signal detection, and safety summarization.
Unlike conventional machine learning algorithms that require task-specific training, foundation models can be fine-tuned for multiple pharmacovigilance applications while maintaining high analytical flexibility. Their scalability makes them particularly attractive for organizations managing large global safety databases40.
6.2 Multimodal Artificial Intelligence
Multimodal AI combines information from different data sources, including clinical narratives, electronic health records, laboratory results, imaging studies, wearable devices, and genomic data. Integrating these heterogeneous datasets provides a more complete representation of patient health than any individual data source alone.
In pharmacovigilance, multimodal AI can improve adverse drug reaction (ADR) detection by simultaneously evaluating medication exposure, laboratory abnormalities, physician notes, and diagnostic findings. This integrated approach enhances signal detection, supports individualized risk prediction, and strengthens benefit–risk assessment across diverse patient populations41.
6.3 Large Language Models
Large Language Models (LLMs) have demonstrated considerable potential for processing unstructured pharmacovigilance information. These models can summarize Individual Case Safety Reports (ICSRs), extract adverse events from scientific literature, support MedDRA coding, generate clinical narratives, and answer domain-specific safety queries.
Despite these advantages, LLMs may generate inaccurate or unsupported information ("hallucinations"), making expert validation essential before regulatory use. Consequently, LLMs should currently be considered decision-support tools rather than autonomous decision-makers42.
6.4 Generative AI
Generative AI extends the capabilities of conventional language models by creating new text, summaries, structured reports, and analytical outputs. Within pharmacovigilance, generative AI has applications in literature review, safety narrative generation, periodic safety update reports, risk management documentation, and regulatory communication.
These technologies substantially reduce administrative workload while improving documentation consistency. However, generated outputs require careful medical review to ensure factual accuracy, regulatory compliance, and patient confidentiality43.
6.5 Retrieval-Augmented Generation (RAG)
Retrieval-Augmented Generation (RAG) combines language models with external knowledge repositories to improve response accuracy. Instead of relying solely on information learned during model training, RAG retrieves relevant evidence from validated databases before generating responses.
For pharmacovigilance, RAG can integrate information from scientific literature, regulatory guidance, safety databases, and product labels, reducing hallucinations while improving transparency and evidence traceability. This architecture is increasingly recognized as a promising approach for trustworthy AI-assisted regulatory decision support44.
6.6 AI Copilots for Pharmacovigilance
AI copilots are interactive systems designed to assist pharmacovigilance professionals throughout routine workflows. Rather than replacing experts, these systems provide real-time recommendations during case assessment, literature review, signal prioritization, and regulatory documentation.
Potential applications include:
Human oversight remains essential to verify recommendations and ensure compliance with pharmacovigilance regulations45.
6.7 Agentic AI
Agentic AI represents the next stage of intelligent automation, where AI systems perform coordinated sequences of tasks under predefined governance frameworks. In pharmacovigilance, agentic AI could automatically retrieve safety reports, identify duplicates, extract relevant clinical information, perform preliminary signal assessment, generate regulatory summaries, and recommend follow-up investigations.
Although these systems offer considerable potential to improve operational efficiency, current regulatory guidance emphasizes that autonomous AI should remain under continuous human supervision until its safety, reliability, and accountability are fully established46.
6.8 Challenges in Implementing Foundation Models
Despite rapid technological progress, several barriers continue to limit widespread implementation of multimodal AI and foundation models in pharmacovigilance. Major challenges include heterogeneous healthcare data, limited interoperability, algorithmic bias, model drift, inadequate explainability, privacy concerns, computational costs, and evolving regulatory requirements. Reliable clinical validation across diverse healthcare settings remains necessary before routine deployment in regulatory practice47.
7. REAL-WORLD EVIDENCE FOR DRUG SAFETY AND REGULATORY DECISION-MAKING
Real-world evidence (RWE) has become a central component of modern pharmacovigilance by complementing evidence generated from randomized clinical trials. Unlike controlled trials, which evaluate medicines under predefined conditions, RWE reflects the effectiveness and safety of therapies in routine clinical practice. The integration of artificial intelligence (AI) with real-world data (RWD) has significantly enhanced the ability to detect adverse drug reactions (ADRs), evaluate long-term safety, and support regulatory decision-making across the medicine lifecycle. Recent reviews emphasize that RWE is increasingly being incorporated into regulatory assessments when randomized trials are infeasible, insufficient, or require complementary evidence48.
7.1 Real-World Data Sources
Real-world evidence is generated from diverse real-world data sources collected during routine healthcare delivery. These include electronic health records, electronic medical records, administrative claims databases, disease registries, pharmacy databases, spontaneous reporting systems, wearable devices, mobile health applications, and patient-reported outcomes. Compared with traditional clinical trials, these data capture broader patient populations, including older adults, pregnant women, pediatric patients, and individuals with multiple comorbidities who are often underrepresented in randomized studies49.
7.2 AI-Enabled Real-World Evidence Analytics
The increasing volume and complexity of RWD require advanced analytical methods for effective interpretation. Machine learning, deep learning, and natural language processing enable automated processing of structured and unstructured healthcare data, improving signal detection and safety evaluation.
AI algorithms identify hidden associations among drug exposure, patient characteristics, laboratory findings, and clinical outcomes that may not be detected using conventional statistical approaches. Recent scoping reviews indicate that AI applied to structured RWD is particularly promising for adverse event prediction, risk stratification, and pharmacovigilance signal management, although greater emphasis is needed on explainable AI, causal AI, and standardized data preprocessing50.
7.3 Role of RWE in Drug Safety Monitoring
RWE enables continuous assessment of medicine safety throughout the post-marketing period. Long-term surveillance allows regulators and healthcare professionals to identify rare adverse events, delayed toxicities, medication errors, and drug–drug interactions that may not become evident during pre-approval clinical trials.
By combining multiple healthcare databases, AI-driven RWE supports earlier detection of emerging safety concerns while improving the characterization of adverse event frequency, severity, and patient-specific risk factors. These analyses contribute to more informed benefit–risk evaluations and timely regulatory actions51.
7.4 Regulatory Applications of Real-World Evidence
Global regulatory agencies increasingly recognize the value of RWE in supporting medicine evaluation. RWE contributes to post-marketing safety surveillance, label modifications, evaluation of rare diseases, pediatric indications, long-term effectiveness studies, and assessment of medicines used in routine clinical practice.
Recent European regulatory pilot programs demonstrated that RWE is particularly valuable for addressing questions related to medicine safety, drug utilization, disease epidemiology, and clinical management. These initiatives highlight the growing acceptance of RWE as complementary evidence for regulatory decision-making52.
7.5 Comparative Effectiveness and Benefit–Risk Assessment
AI-integrated RWE enables comparative evaluation of therapeutic alternatives in routine clinical settings. Unlike randomized trials with strict eligibility criteria, RWE captures treatment outcomes across heterogeneous populations and real-world prescribing patterns.
These analyses improve understanding of medicine effectiveness, adherence, persistence, and long-term safety while supporting dynamic benefit–risk assessment throughout the product lifecycle. Advanced analytical methods also facilitate subgroup analyses that identify patients most likely to benefit from specific therapies while minimizing treatment-related risks53.
7.6 Personalized Pharmacovigilance
The integration of RWE with AI is advancing personalized pharmacovigilance by identifying individual patient characteristics associated with increased ADR susceptibility. Predictive models combine demographic information, comorbidities, laboratory parameters, medication history, pharmacogenomic biomarkers, and lifestyle factors to estimate individualized safety risks.
Personalized pharmacovigilance supports precision medicine by enabling clinicians to optimize therapeutic decisions according to each patient's unique clinical profile, thereby improving treatment safety and effectiveness54.
7.7 Challenges in Using RWE
Despite its considerable potential, several challenges continue to limit the widespread use of RWE. These include heterogeneous data formats, missing information, inconsistent coding systems, residual confounding, selection bias, privacy concerns, and limited interoperability across healthcare databases.
Methodological rigor, transparent study design, standardized data models, and robust validation remain essential to ensure that RWE generated through AI is reliable for clinical and regulatory decision-making55.
8. AI IN SPECIAL PHARMACOVIGILANCE AREAS
The application of artificial intelligence (AI) has expanded beyond conventional pharmacovigilance to address safety challenges in specialized therapeutic areas. These settings often involve complex treatment regimens, vulnerable patient populations, or limited clinical evidence, making continuous safety surveillance particularly important. By integrating real-world evidence (RWE), AI enables more precise detection of adverse drug reactions (ADRs), supports individualized risk assessment, and improves regulatory decision-making across diverse clinical scenarios56.
8.1 Oncology Pharmacovigilance
Cancer therapies, including targeted agents, immunotherapies, and antibody-drug conjugates, are frequently associated with complex and sometimes delayed adverse events. Conventional pharmacovigilance approaches may not adequately capture these toxicities because of heterogeneous treatment regimens and combination therapies.
AI-driven analysis of electronic health records, oncology registries, and spontaneous reporting systems enables earlier identification of immune-related adverse events, cardiotoxicity, hepatotoxicity, and hematological toxicities. Machine learning models also support prediction of treatment-related complications and facilitate personalized safety monitoring throughout cancer therapy57.
8.2 Vaccine Pharmacovigilance
Vaccines require continuous post-marketing safety monitoring due to their widespread use across healthy populations. During the COVID-19 pandemic, AI-assisted pharmacovigilance demonstrated its value by rapidly analyzing millions of adverse event reports submitted to national and international surveillance systems.
Natural language processing (NLP) and machine learning improved automated case processing, duplicate detection, and identification of rare adverse events such as myocarditis, thrombosis with thrombocytopenia syndrome, and anaphylaxis. AI-supported surveillance also enhanced vaccine safety communication and strengthened regulatory decision-making during large-scale immunization programs58.
8.3 Pediatric Pharmacovigilance
Children exhibit developmental differences in drug absorption, distribution, metabolism, and elimination, making extrapolation of adult safety data challenging. In addition, pediatric clinical trials often involve limited sample sizes.
AI enables integration of pediatric electronic health records, prescription databases, and patient registries to identify age-specific ADRs and evaluate medicine safety across different developmental stages. Predictive models also assist clinicians in identifying children at increased risk of adverse reactions and optimizing individualized treatment strategies59.
8.4 Pregnancy Pharmacovigilance
Pregnant women are commonly excluded from pre-marketing clinical trials, resulting in limited evidence regarding medicine safety during pregnancy. Consequently, post-marketing surveillance plays a critical role in evaluating maternal and fetal outcomes.
AI facilitates analysis of pregnancy registries, electronic health records, birth outcome databases, and spontaneous reports to identify potential teratogenic effects, pregnancy complications, and neonatal adverse outcomes. Integration of multiple real-world data sources improves the detection of rare safety events while supporting evidence-based prescribing during pregnancy60.
8.5 Rare Diseases and Orphan Drugs
Rare diseases present unique pharmacovigilance challenges because of limited patient populations, small clinical trials, and restricted long-term safety data. AI assists by integrating global patient registries, electronic health records, and international pharmacovigilance databases to improve safety signal detection.
Machine learning algorithms identify uncommon adverse events, characterize long-term treatment outcomes, and support benefit–risk assessment for orphan medicines. International collaboration and real-world evidence are particularly valuable in this setting due to the limited availability of conventional clinical data61.
8.6 Biologics and Biosimilars
Biological medicines are structurally complex and may produce immunogenic reactions that differ from those associated with conventional small-molecule drugs. Continuous pharmacovigilance is therefore essential following market authorization.
AI-assisted surveillance integrates laboratory findings, electronic health records, and spontaneous reporting data to monitor infusion reactions, hypersensitivity, immunogenicity, and loss of therapeutic response. These approaches support comparative safety assessment between reference biologics and biosimilars while improving long-term monitoring62.
8.7 Precision Medicine and Pharmacogenomics
Advances in pharmacogenomics have accelerated the development of precision medicine, where treatment decisions are tailored according to individual genetic profiles. AI integrates genomic biomarkers with clinical and real-world data to identify patients at increased risk of adverse drug reactions.
Predictive models combining pharmacogenomic information, laboratory data, medication history, and demographic characteristics enable personalized risk prediction and optimize medicine selection. This approach supports safer prescribing practices while reducing preventable adverse drug reactions63.
8.8 Public Health Emergency Pharmacovigilance
Emerging infectious diseases, pandemics, and humanitarian emergencies require rapid pharmacovigilance systems capable of processing large volumes of safety data in real time. AI facilitates automated case processing, signal prioritization, and integration of global surveillance data during public health crises.
Experiences gained during recent pandemic responses demonstrated that AI-supported pharmacovigilance can improve the speed of regulatory assessment while maintaining continuous monitoring of newly introduced medicines and vaccines. These capabilities are expected to become increasingly important for future emergency preparedness64.
9. REGULATORY LANDSCAPE AND GLOBAL GUIDELINES FOR AI-DRIVEN PHARMACOVIGILANCE
The successful implementation of artificial intelligence (AI) in pharmacovigilance depends not only on technological innovation but also on robust regulatory oversight. Regulatory agencies increasingly recognize the potential of AI to improve drug safety while emphasizing that AI systems must remain transparent, validated, reliable, and subject to appropriate human oversight. Current regulatory frameworks continue to evolve as AI becomes integrated into routine pharmacovigilance activities, including case processing, signal detection, benefit–risk assessment, and regulatory reporting65.
9.1 Global Regulatory Framework for Pharmacovigilance
International pharmacovigilance is governed by harmonized regulatory frameworks developed by organizations such as the World Health Organization (WHO), the International Council for Harmonisation (ICH), the U.S. Food and Drug Administration (FDA), and the European Medicines Agency (EMA). These organizations establish standards for adverse event reporting, signal management, risk management, and post-marketing surveillance.
Current pharmacovigilance regulations were primarily developed for conventional safety monitoring systems. As AI technologies become increasingly integrated into pharmacovigilance, regulators are adapting existing frameworks to address algorithm validation, data governance, explainability, cybersecurity, and continuous model monitoring66.
9.2 U.S. FDA Perspective
The U.S. FDA supports the responsible use of AI and real-world evidence (RWE) throughout the medicine lifecycle. Regulatory initiatives encourage the use of machine learning for safety surveillance while emphasizing transparency, reproducibility, and scientific validity.
The FDA also promotes the use of RWE for regulatory decision-making through its Real-World Evidence Program. AI-generated evidence should be supported by appropriate validation, documentation, and expert review before influencing regulatory actions. Human oversight remains essential for decisions involving patient safety67.
9.3 European Medicines Agency
The European Medicines Agency (EMA) has developed strategies to facilitate the safe adoption of AI across the medicines regulatory network. The agency encourages innovation while maintaining high standards for data quality, patient privacy, and regulatory transparency.
EMA initiatives emphasize trustworthy AI, lifecycle monitoring of AI models, explainability, and continuous performance evaluation. Collaboration among regulatory authorities, academia, healthcare institutions, and industry is considered essential for responsible AI implementation68.
9.4 International Council for Harmonisation
The International Council for Harmonisation (ICH) provides internationally accepted guidelines for pharmacovigilance, including Individual Case Safety Reports (ICSRs), periodic safety reporting, signal management, and risk management planning.
Although most ICH guidelines were established before widespread AI adoption, their principles remain applicable to AI-supported pharmacovigilance. Future revisions are expected to incorporate recommendations regarding AI validation, algorithm transparency, and governance while maintaining existing standards for data quality and patient safety69.
9.5 Good Machine Learning Practice
Good Machine Learning Practice (GMLP) provides guiding principles for the development, validation, deployment, and continuous monitoring of AI systems used in healthcare. These principles emphasize high-quality training data, robust model development, independent validation, cybersecurity, and continuous post-deployment monitoring.
Within pharmacovigilance, adherence to GMLP helps ensure that AI systems remain accurate, reliable, reproducible, and clinically relevant throughout their operational lifecycle70.
9.6 Validation of AI Systems
Before AI systems can be integrated into pharmacovigilance practice, rigorous validation is required to demonstrate analytical accuracy, clinical relevance, reproducibility, and regulatory compliance.
Validation should include internal testing, external validation using independent datasets, prospective evaluation, and continuous performance monitoring following deployment. Periodic model updates should be accompanied by revalidation to ensure sustained reliability as healthcare data evolve over time71.
9.7 AI Governance and Risk Management
Effective governance frameworks are essential for ensuring responsible AI implementation. Governance includes clearly defined accountability, documentation, auditability, data stewardship, risk management, and ethical oversight throughout the AI lifecycle.
Organizations implementing AI in pharmacovigilance should establish multidisciplinary governance committees involving pharmacovigilance experts, clinicians, data scientists, regulatory specialists, cybersecurity professionals, and ethicists. Such collaborative governance promotes responsible innovation while protecting patient safety72.
9.8 International Harmonization
Variation in healthcare systems, reporting standards, data formats, and regulatory requirements presents significant challenges for global AI implementation. International harmonization of terminology, interoperability standards, validation procedures, and regulatory expectations will facilitate wider adoption of AI-driven pharmacovigilance.
Global collaboration among regulatory agencies, pharmaceutical companies, healthcare providers, and academic institutions will be critical for developing internationally accepted standards that enable trustworthy AI-assisted drug safety surveillance73.
10. CHALLENGES, LIMITATIONS, ETHICAL CONSIDERATIONS, AND RESPONSIBLE AI IN PHARMACOVIGILANCE
Despite remarkable advances in artificial intelligence (AI), several scientific, technical, regulatory, and ethical challenges continue to limit its widespread implementation in pharmacovigilance. Addressing these limitations is essential to ensure that AI systems remain accurate, transparent, reliable, and clinically meaningful. Responsible AI requires a balance between technological innovation and patient safety, with continuous human oversight throughout the pharmacovigilance lifecycle74.
10.1 Data Quality and Heterogeneity
The performance of AI models depends largely on the quality of the underlying data. Pharmacovigilance data originate from multiple sources, including spontaneous reporting systems, electronic health records, administrative claims, biomedical literature, patient registries, wearable devices, and social media. These datasets frequently differ in structure, coding standards, completeness, and clinical quality.
Missing information, duplicate reports, inconsistent terminology, and reporting bias may reduce model performance and generate inaccurate safety predictions. Standardized data models, interoperability frameworks, and rigorous data curation are therefore essential for reliable AI-driven pharmacovigilance75.
10.2 Algorithmic Bias
AI systems may unintentionally learn biases present within historical healthcare datasets. Unequal representation of age groups, ethnic populations, geographic regions, disease severity, or prescribing practices can influence model predictions and reduce generalizability.
Algorithmic bias may result in underestimation of adverse drug reactions in vulnerable populations or overestimation of risk in others. Developing diverse training datasets, performing fairness assessments, and conducting external validation across multiple healthcare settings are important strategies for minimizing bias76.
10.3 Limited Explainability
Many advanced deep learning models function as complex “black-box” systems, making it difficult for clinicians and regulators to understand how predictions are generated. Limited interpretability reduces confidence in AI-assisted safety decisions and may delay regulatory acceptance.
Explainable Artificial Intelligence (XAI) addresses this challenge by providing transparent explanations for model outputs. Techniques such as feature attribution and interpretable visualization improve understanding of AI predictions while supporting evidence-based clinical and regulatory decision-making77.
10.4 Privacy and Data Security
AI-driven pharmacovigilance requires access to large volumes of patient information collected from multiple healthcare systems. Although these datasets provide valuable safety insights, they also increase concerns regarding patient confidentiality, data ownership, and unauthorized access.
Compliance with national and international data protection regulations, implementation of secure data-sharing mechanisms, encryption technologies, anonymization procedures, and privacy-preserving AI approaches such as federated learning are essential for protecting sensitive health information78.
10.5 Regulatory and Legal Challenges
Regulatory frameworks governing AI continue to evolve. Current pharmacovigilance regulations provide limited guidance regarding validation of adaptive algorithms, continuous learning systems, and generative AI applications.
Important regulatory considerations include algorithm transparency, documentation, reproducibility, accountability, post-deployment monitoring, and auditability. Harmonized international guidance will be required to facilitate safe and consistent implementation of AI across global pharmacovigilance systems79.
10.6 Validation and Generalizability
AI models frequently demonstrate excellent performance during internal validation but may perform differently when applied to external healthcare settings with different patient populations, prescribing patterns, and clinical practices.
Comprehensive validation using independent datasets, prospective evaluation, and continuous performance monitoring are necessary before routine implementation. Periodic model updates should be accompanied by systematic revalidation to ensure sustained reliability80.
10.7 Human Oversight and Clinical Expertise
Although AI can automate numerous pharmacovigilance tasks, expert clinical judgment remains indispensable. Safety signal evaluation, causality assessment, benefit–risk analysis, and regulatory decision-making require clinical interpretation that extends beyond algorithmic prediction.
Human-in-the-loop frameworks combine computational efficiency with expert oversight, ensuring that AI recommendations are critically evaluated before influencing patient care or regulatory action81.
10.8 Ethical Considerations
Responsible AI implementation requires adherence to fundamental ethical principles, including transparency, fairness, accountability, patient autonomy, privacy, and non-maleficence. AI systems should be designed to support equitable healthcare while minimizing unintended harm.
Clear documentation of model development, validation procedures, data sources, and decision-making processes improves transparency and strengthens trust among clinicians, patients, regulators, and the pharmaceutical industry82.
10.9 Sustainable Implementation of AI
Successful integration of AI into pharmacovigilance depends not only on technological capability but also on workforce development, institutional readiness, infrastructure, and interdisciplinary collaboration.
Healthcare professionals require appropriate training in AI applications, while organizations should establish governance frameworks, quality assurance programs, and continuous monitoring strategies to ensure sustainable implementation over time83.
Table 2. Challenges and Future Directions
|
Challenges |
Future direction |
|
Poor data quality |
Standardized RWD |
|
Algorithmic bias |
Fair and explainable AI |
|
Limited validation |
Prospective multicenter studies |
|
Privacy concerns |
Federated learning |
|
Regulatory uncertainty |
Global AI governance |
|
Clinical implementation |
Human–AI collaboration |
11. EMERGING TRENDS AND FUTURE TECHNOLOGIES IN AI-DRIVEN PHARMACOVIGILANCE
The continuous evolution of artificial intelligence (AI), digital health technologies, and real-world evidence (RWE) is redefining the future of pharmacovigilance. Emerging technologies are moving beyond simple automation toward intelligent, adaptive, and patient-centered safety surveillance systems. These innovations have the potential to improve the timeliness, accuracy, and scalability of drug safety monitoring while supporting evidence-based regulatory decision-making. Although many technologies remain under active development, their integration into pharmacovigilance is expected to accelerate over the coming decade84.
11.1 Generative AI for Pharmacovigilance
Generative AI has emerged as a promising tool for automating knowledge-intensive pharmacovigilance activities. Unlike conventional machine learning models, generative AI can summarize scientific literature, draft Individual Case Safety Reports (ICSRs), generate safety narratives, assist in MedDRA coding, and support preparation of aggregate safety reports.
Future applications may include automated preparation of Periodic Safety Update Reports (PSURs), Development Safety Update Reports (DSURs), Risk Management Plans (RMPs), and regulatory briefing documents. Despite these advantages, all AI-generated outputs should undergo expert medical and regulatory review to ensure scientific accuracy, regulatory compliance, and patient safety85.
11.2 Explainable Artificial Intelligence
The growing complexity of AI models has increased the need for transparent and interpretable decision-making. Explainable Artificial Intelligence (XAI) enables users to understand how AI systems generate predictions by identifying the variables contributing to each decision.
Future pharmacovigilance platforms are expected to integrate explainability directly into signal detection and risk prediction workflows, improving clinician confidence and facilitating regulatory acceptance. Explainability will also support model auditing, quality assurance, and continuous performance monitoring86.
11.3 Federated Learning
Federated learning is an emerging privacy-preserving AI approach that enables multiple healthcare institutions to collaboratively develop machine learning models without sharing patient-level data. Instead of transferring sensitive information to a central repository, only model parameters are exchanged.
This decentralized framework improves data security, supports international collaboration, and facilitates analysis of geographically diverse populations while maintaining compliance with privacy regulations. Federated learning is expected to play an increasingly important role in multinational pharmacovigilance studies87.
11.4 Digital Twins
Digital twins are virtual computational representations of individual patients that continuously integrate clinical, physiological, genomic, and treatment-related information. These models simulate patient-specific responses to medicines and may enable prediction of adverse drug reactions before they occur.
Although digital twin technology remains in its early stages, future integration with pharmacovigilance systems may support individualized benefit–risk assessment, treatment optimization, and proactive safety monitoring88.
11.5 Wearable Devices and Continuous Safety Monitoring
Wearable sensors and remote patient monitoring technologies are generating continuous streams of physiological information outside traditional healthcare settings. Heart rate, blood pressure, electrocardiographic signals, physical activity, sleep patterns, and glucose measurements provide valuable indicators of treatment safety.
AI algorithms can analyze these longitudinal data in near real time, enabling earlier detection of adverse drug reactions and supporting continuous post-marketing surveillance. Integration of wearable technologies with electronic health records is expected to strengthen personalized pharmacovigilance89.
11.6 Pharmacogenomics and Precision Pharmacovigilance
Advances in genomic medicine are shifting pharmacovigilance toward individualized safety assessment. Integration of pharmacogenomic biomarkers with clinical and real-world data enables prediction of patient-specific susceptibility to adverse drug reactions.
Future AI models will combine genomic information, laboratory findings, medication history, environmental factors, and lifestyle characteristics to guide personalized medicine and optimize therapeutic decision-making while minimizing treatment-related risks90.
11.7 Blockchain for Pharmacovigilance
Blockchain technology offers a secure and transparent framework for managing pharmacovigilance data. Its decentralized architecture provides immutable records, enhances data integrity, and improves traceability of safety information throughout the medicine lifecycle.
Potential applications include secure sharing of Individual Case Safety Reports, verification of data provenance, audit trails for regulatory inspections, and improved collaboration among healthcare institutions, pharmaceutical companies, and regulatory agencies91.
11.8 Internet of Medical Things (IoMT)
The Internet of Medical Things (IoMT) connects wearable sensors, medical devices, mobile health applications, and healthcare information systems through secure digital networks. Continuous collection of patient-generated health data expands opportunities for proactive safety surveillance.
AI-driven analysis of IoMT data may facilitate early recognition of treatment-related complications, improve medication adherence monitoring, and strengthen post-marketing safety evaluation in real-world clinical practice92.
11.9 Agentic AI and Autonomous Pharmacovigilance
Agentic AI represents the next stage of intelligent automation, where AI systems coordinate multiple pharmacovigilance tasks with minimal human intervention while remaining under predefined governance frameworks.
Future applications may include autonomous literature surveillance, automated case intake, duplicate detection, signal prioritization, benefit–risk summarization, and preparation of regulatory documentation. However, regulatory authorities continue to emphasize that autonomous systems should function under continuous expert supervision until sufficient evidence regarding safety, reliability, and accountability becomes available93.
11.10 Learning Health Systems
Future pharmacovigilance is expected to become an integral component of learning health systems, in which clinical practice continuously generates new evidence that improves patient care. AI will facilitate rapid integration of clinical outcomes, electronic health records, registries, genomic information, and pharmacovigilance databases into continuously updating safety models.
Such adaptive systems will support real-time benefit–risk assessment, personalized treatment recommendations, and rapid identification of emerging safety concerns throughout the product lifecycle94.
12. RESEARCH GAP
Despite substantial advances in artificial intelligence (AI)-driven pharmacovigilance, several critical research gaps continue to limit its translation into routine regulatory and clinical practice. Most published studies rely on retrospective datasets, single-center analyses, or spontaneous reporting systems, with relatively few investigations integrating diverse real-world data sources such as electronic health records, claims databases, patient registries, wearable devices, and pharmacogenomic data into unified AI frameworks. Furthermore, many AI models prioritize predictive performance over interpretability, limiting clinician confidence and regulatory acceptance. External validation across geographically diverse populations and healthcare systems remains insufficient, raising concerns regarding model generalizability and reproducibility. Emerging technologies, including multimodal AI, foundation models, retrieval-augmented generation, federated learning, and agentic AI, have shown considerable promise but lack robust prospective evaluation in real-world pharmacovigilance settings. In addition, standardized methodologies for model validation, benchmarking, and reporting are still evolving, while regulatory guidance for adaptive and generative AI remains limited. Future research should focus on developing explainable, trustworthy, and clinically validated AI systems that integrate high-quality real-world evidence, incorporate privacy-preserving data-sharing approaches, and align with harmonized international regulatory frameworks. Addressing these challenges will be essential to establish scalable, transparent, and patient-centered next-generation pharmacovigilance systems capable of supporting reliable drug safety decision-making.
DISCUSSION
Artificial intelligence (AI) is reshaping pharmacovigilance by enabling rapid analysis of large-scale real-world data and supporting evidence-based drug safety surveillance. Unlike conventional pharmacovigilance, which primarily depends on spontaneous reporting systems and manual review, AI integrates multiple data sources, including electronic health records, administrative claims, biomedical literature, patient registries, wearable devices, and patient-generated health data. This multidimensional approach enhances the identification of adverse drug reactions (ADRs), strengthens safety signal detection, and supports continuous benefit–risk assessment throughout the medicine lifecycle.
Current evidence indicates that machine learning, deep learning, and natural language processing have substantially improved several pharmacovigilance activities, including Individual Case Safety Report (ICSR) processing, MedDRA coding, duplicate detection, literature surveillance, and signal prioritization. More recently, foundation models, multimodal AI, and generative AI have expanded these capabilities by facilitating automated knowledge extraction, clinical document summarization, and intelligent decision support. However, these technologies should be viewed as complementary tools that augment, rather than replace, the expertise of pharmacovigilance professionals and regulatory authorities.
The integration of AI with real-world evidence (RWE) represents one of the most significant advances in next-generation pharmacovigilance. Real-world data provide insights into medicine safety across heterogeneous populations, including older adults, pediatric patients, pregnant women, individuals with multiple comorbidities, and patients receiving long-term therapies. AI enables efficient analysis of these complex datasets, improving the detection of rare and delayed adverse events that may not be identified during pre-marketing clinical trials. Consequently, AI-supported RWE has become increasingly valuable for regulatory decision-making, label updates, and post-marketing risk management.
Despite these advances, important challenges remain. Data heterogeneity, incomplete reporting, algorithmic bias, limited explainability, privacy concerns, and inconsistent regulatory requirements continue to hinder widespread implementation. In addition, many published AI models have been evaluated using retrospective datasets with limited external validation, reducing confidence in their generalizability across different healthcare systems. Future research should therefore prioritize prospective multicenter validation, standardized benchmarking, explainable AI, and robust governance frameworks to ensure reliable clinical performance and regulatory acceptance.
Looking ahead, emerging technologies such as federated learning, multimodal foundation models, digital twins, retrieval-augmented generation, and agentic AI are expected to further transform pharmacovigilance by enabling secure data sharing, personalized safety prediction, and intelligent workflow automation. Successful implementation will require close collaboration among healthcare professionals, data scientists, pharmaceutical companies, regulatory agencies, and academic researchers. Such multidisciplinary efforts will facilitate the development of transparent, trustworthy, and continuously learning pharmacovigilance systems that improve patient safety while supporting efficient regulatory decision-making.
CONCLUSION
Artificial intelligence (AI) is transforming pharmacovigilance from a predominantly reactive surveillance system into a proactive, data-driven, and continuously learning framework for drug safety monitoring. The integration of AI with real-world evidence (RWE) has significantly enhanced the detection of adverse drug reactions, automated safety case processing, improved signal detection, and strengthened benefit–risk assessment throughout the medicine lifecycle. Technologies such as machine learning, deep learning, natural language processing, explainable AI, multimodal AI, and foundation models have demonstrated considerable potential to improve the efficiency, accuracy, and scalability of pharmacovigilance activities while supporting evidence-informed regulatory decision-making.
Despite these advancements, important challenges remain, including heterogeneous data sources, variable data quality, limited external validation, algorithmic bias, privacy concerns, and evolving regulatory frameworks. Addressing these limitations will require standardized data governance, robust model validation, transparent AI methodologies, and harmonized international regulatory guidance. Importantly, AI should complement rather than replace clinical expertise, with human oversight remaining essential for safety assessment and regulatory decision-making.
Overall, the convergence of AI, real-world evidence, and digital health technologies represents a major step toward next-generation pharmacovigilance. Continued interdisciplinary collaboration among healthcare professionals, researchers, industry, and regulatory agencies will be crucial for developing trustworthy, explainable, and patient-centered AI systems capable of improving global drug safety and supporting precision medicine.
FUTURE PERSPECTIVES
The future of pharmacovigilance will be shaped by the integration of advanced AI technologies with increasingly diverse real-world data sources. Emerging innovations, including multimodal foundation models, generative AI, federated learning, digital twins, graph neural networks, and retrieval-augmented generation, are expected to enable more accurate, scalable, and personalized drug safety surveillance. These technologies will facilitate continuous analysis of electronic health records, wearable device data, genomics, biomedical literature, and patient-reported outcomes, allowing earlier identification of safety signals and more precise prediction of adverse drug reactions.
Future pharmacovigilance systems are also expected to evolve into intelligent learning health ecosystems, where AI continuously updates safety knowledge from routine clinical practice while maintaining transparency and regulatory compliance. Explainable AI and privacy-preserving approaches will become increasingly important for improving clinician confidence, ensuring ethical implementation, and supporting international regulatory acceptance. In parallel, harmonized global standards for AI validation, benchmarking, governance, and lifecycle monitoring will be essential for widespread clinical adoption.
As AI technologies continue to mature, future research should prioritize prospective multicenter validation, integration of multimodal real-world evidence, and development of trustworthy AI frameworks that balance innovation with patient safety. These advances have the potential to establish a globally connected, adaptive, and patient-centered pharmacovigilance ecosystem capable of improving medicine safety, optimizing therapeutic decision-making, and advancing precision healthcare.
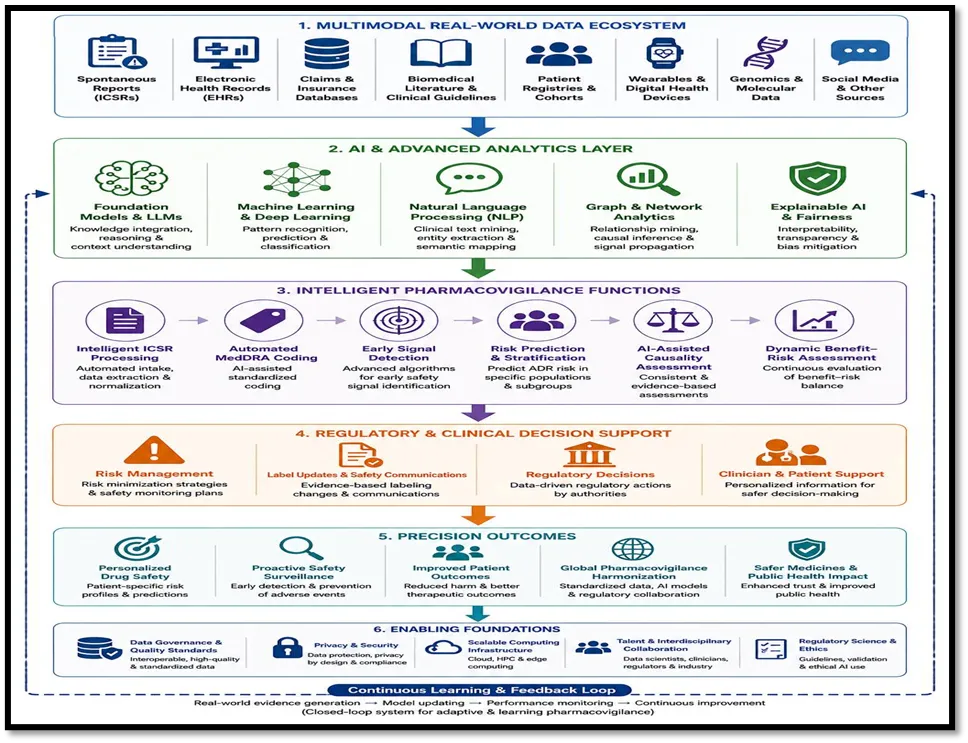
Fig No. 3 Future Framework for AI Enabled Precision Pharmacovigilance
REFERENCES

Yash Kothikar, Tanveer Patel, Artificial Intelligence-Driven Pharmacovigilance: Integrating Real-World Evidence for Next-Generation Drug Safety, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 1407-1436, https://doi.org/10.5281/zenodo.21242169
 10.5281/zenodo.21242169
10.5281/zenodo.21242169