
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,5 Base Hospital Sammanthurai
2 Regional Director of Health Services, Monaragala
3 Ministry of Health
4 Registrar in Medical Administration, PGIM, University of Colombo
Effective documentation and file management play a vital role in ensuring patient safety, continuity of care, and efficient communication among healthcare professionals. However, challenges related to maintaining and retrieving patient records continue to affect the quality of healthcare services in many hospital wards. This study aimed to assess the problems associated with existing documentation and file management practices and to identify possible recommendations for improvement among nursing officers at Base Hospital Sammanthurai. A quantitative descriptive cross-sectional study was conducted among 80 nursing officers selected through convenience sampling. Data were collected using a structured self-administered questionnaire that included demographic information, current documentation practices, challenges encountered, and suggested improvements. The collected data were analysed using descriptive statistics, including frequencies and percentages. The findings revealed that the most common challenges were difficulty in retrieving patient information (90%), time-consuming document searches (72%), overcrowded files (54%), communication issues during patient handover (52%), and misplacement of documents (50%). Most participants believed that improving documentation systems would enhance patient care quality. Key recommendations included introducing standardized file formats (95%), providing better staff training (88%), strengthening file materials (100%), and implementing electronic documentation systems (55%). The study concluded that existing documentation and file management practices require improvement to enhance healthcare efficiency, reduce errors, and promote patient safety. Strengthening documentation systems through standardization, training, and improved monitoring can contribute significantly to better patient care outcomes.
Documentation is one of the most important responsibilities of nursing officers in healthcare settings. It involves recording patient information, nursing interventions, treatments, observations, and outcomes in a clear and accurate manner. Proper documentation helps ensure continuity of care, supports effective communication among healthcare professionals, and serves as a legal record of the care provided to patients. Therefore, maintaining accurate and complete documentation is essential for delivering safe and high-quality healthcare services.
File management is another important aspect of healthcare administration. Patient records need to be properly organized, stored, and maintained so that information can be easily retrieved whenever required. Effective file management enables healthcare professionals to access important patient information quickly, make timely clinical decisions, and provide appropriate care. A well-organized documentation system also reduces errors, improves efficiency, and enhances patient safety.
Despite the importance of documentation and file management, many healthcare institutions continue to experience challenges in maintaining effective record-keeping systems. Nursing officers often face difficulties such as incomplete documentation, misplaced records, overcrowded files, damaged documents, and delays in retrieving patient information. These issues can increase workload, affect communication among healthcare staff, and negatively influence the quality of patient care.
In hospital wards, where patient information is frequently updated and shared among healthcare professionals, efficient documentation and file management are particularly important. Any weakness in these systems may lead to misunderstandings, treatment delays, and reduced quality of healthcare services. Therefore, it is important to assess the existing documentation and file management practices and identify areas that require improvement. This study was conducted among nursing officers at Base Hospital Sammanthurai to assess the problems associated with current documentation and file management practices and to identify practical recommendations that can improve healthcare efficiency, patient safety, and the overall quality of nursing care.
Accurate documentation and effective file management are essential for providing safe, efficient, and high-quality patient care. Nursing officers rely on patient records to communicate important information, monitor patient progress, and make appropriate clinical decisions. When documentation is incomplete, inaccurate, or difficult to access, it can negatively affect the continuity and quality of care provided to patients. In many hospital wards, nursing officers experience various challenges related to documentation and file management. These challenges may include difficulty in retrieving patient information, misplaced documents, incomplete records, poor organization of files, overcrowded filing systems, and communication issues during patient handovers. Such problems can increase the workload of nursing staff, delay healthcare services, and potentially compromise patient safety.
Although documentation plays a critical role in healthcare delivery, there is limited information regarding the specific challenges faced by nursing officers in managing ward documentation and patient records at Base Hospital Sammanthurai. Understanding these challenges is important for identifying weaknesses in the current system and developing practical strategies for improvement. Therefore, this study was conducted to assess the problems associated with existing documentation and file management practices among nursing officers in hospital wards and to identify recommendations that may improve healthcare efficiency, patient safety, and the quality of patient care.
General Objective
The main objective of this study was to assess the problems associated with existing documentation and file management practices in hospital wards and to identify possible ways of improving these systems among nursing officers at Base Hospital Sammanthurai.
Specific Objectives
1.5 Significance of the Study
This study is important because effective documentation and file management are essential for ensuring patient safety, continuity of care, and the delivery of quality healthcare services. By identifying the challenges faced by nursing officers in maintaining patient records and managing ward files, this study provides valuable information that can help improve existing documentation practices.
The findings of this study may benefit nursing officers by increasing awareness of common documentation problems and encouraging the adoption of better record-keeping practices. Improved documentation systems can help nurses access patient information more easily, reduce errors, and enhance communication among healthcare professionals.
Hospital administrators and nursing managers may also benefit from this study, as the findings can assist them in identifying weaknesses in current documentation systems and developing appropriate strategies to improve file management practices. The recommendations provided may support the implementation of standardized documentation procedures, staff training programs, and improved monitoring systems.
Patients are expected to benefit indirectly from this study through improved quality of care, enhanced patient safety, and better communication among healthcare providers. Efficient documentation and file management systems can contribute to timely clinical decision-making and reduce the risk of errors in patient care.
Furthermore, this study may serve as a useful reference for students, researchers, and healthcare professionals who are interested in conducting future research related to nursing documentation, healthcare management, and patient safety. It can also contribute to the existing body of knowledge on documentation and file management practices in healthcare settings.
1.6 Scope and Delimitations
Scope of the Study
This study focused on assessing the problems associated with documentation and file management practices among nursing officers working in selected wards at Base Hospital Sammanthurai. The study examined the current methods used for maintaining patient records, the challenges encountered in documentation and file management, and the possible improvements that could enhance the quality and efficiency of healthcare services.
The research specifically explored issues related to record keeping, retrieval of patient information, organization of files, communication during patient handovers, and the overall effectiveness of existing documentation systems. Information was collected directly from nursing officers because they are the primary healthcare professionals responsible for maintaining ward documentation and patient records.
Delimitations of the Study
To ensure that the study remained focused and manageable, certain boundaries were established. The study was limited to nursing officers working in selected wards at Base Hospital Sammanthurai and did not include nurses from other hospitals or healthcare institutions. Other healthcare professionals, such as doctors, pharmacists, and administrative staff, were not included in the study.
The research focused only on documentation and file management practices and did not assess other aspects of nursing performance or patient care. In addition, the findings were based on information collected during the study period and reflected the experiences and perceptions of the participants at that time. Therefore, the results of this study should be interpreted within the context of the selected hospital setting and may not be fully generalizable to all healthcare institutions.
1.7 Definition of Terms
Communication
The process of sharing information among healthcare professionals to ensure coordinated and effective patient care.
Documentation
Documentation refers to the process of accurately recording patient information, nursing assessments, treatments, interventions, and outcomes in a systematic manner. It serves as an important source of information for healthcare providers and supports continuity of care.
File Management
File management is the process of organizing, storing, maintaining, and retrieving patient records and related documents in a healthcare setting. Effective file management helps ensure that patient information is easily accessible when needed.
Healthcare Quality
Healthcare quality refers to the degree to which healthcare services improve patient outcomes, ensure patient safety, and meet established professional standards.
Nursing Officer
A nursing officer is a qualified healthcare professional who provides direct patient care and is responsible for maintaining accurate patient records and documentation within the hospital ward.
Patient Record
A patient record is a collection of documents containing important information about a patient’s medical history, diagnosis, treatment, nursing care, and progress during hospitalization.
Patient Safety
Patient safety refers to the prevention of errors, injuries, and harm that may occur during the delivery of healthcare services.
Retrieval of Information
Retrieval of information refers to the process of locating and accessing patient records or specific information from documentation systems when required for patient care.
Ward Documentation
Ward documentation includes all written or recorded information maintained within a hospital ward regarding patient care, treatment plans, observations, investigations, and nursing activities.
Ward File System
The ward file system refers to the method used for organizing, storing, and managing patient records and related documents within hospital wards to facilitate easy access and effective record keeping.
2.1 Conceptual Framework
A conceptual framework provides a clear understanding of the main concepts involved in a study and illustrates how these concepts are related to one another. It serves as a guide for the researcher by explaining the factors that influence the research problem and the expected outcomes.
In this study, the conceptual framework is based on the idea that effective documentation and file management practices are essential for ensuring quality patient care, patient safety, and efficient communication among healthcare professionals. Nursing officers play a key role in maintaining patient records, and the quality of documentation largely depends on how accurately and systematically information is recorded and managed.
However, several challenges may affect documentation and file management practices in hospital wards. These challenges include incomplete documentation, misplaced records, poor file organization, overcrowded files, difficulties in retrieving patient information, and inadequate supervision. Such problems can lead to communication gaps among healthcare providers, delays in clinical decision-making, increased workload, and reduced quality of patient care.
The framework further suggests that implementing appropriate interventions, such as standardized documentation formats, regular staff training, documentation audits, improved supervision, stronger file management systems, and electronic documentation systems, can help overcome these challenges. As a result, healthcare organizations may experience improved efficiency, better communication, enhanced patient safety, and higher quality patient care. Therefore, this study examines the existing documentation and file management challenges faced by nursing officers and explores how recommended improvements can contribute to more effective healthcare delivery.
Challenges in Documentation and File Management
Effects on Healthcare Delivery
Recommended Interventions
Expected Outcomes
2.2 Review of Related Literature
Documentation in Nursing Practice
Documentation has long been recognized as an essential component of nursing practice. According to the American Nurses Association (2010), accurate documentation supports continuity of care, improves communication among healthcare professionals, and serves as a legal record of patient care. Proper documentation enables nurses to record patient conditions, treatments, and outcomes systematically, ensuring that important information is available whenever needed.
Similarly, Burns and Grove (2011) emphasized that nursing documentation plays a significant role in evidence-based practice and quality healthcare delivery. They noted that accurate records help healthcare professionals make informed clinical decisions and reduce the likelihood of medical errors.
Challenges in Documentation Practices
Several studies have identified challenges associated with nursing documentation. Ellis and Hartley (2012) reported that incomplete documentation and inconsistent record-keeping practices remain common problems in healthcare settings. These issues often affect communication among healthcare providers and may compromise patient safety. According to Timby (2013), heavy workloads, staff shortages, and time constraints are major factors contributing to poor documentation practices among nurses.
The author highlighted that nurses frequently struggle to balance direct patient care responsibilities with documentation requirements. Furthermore, Yoder-Wise (2014) found that inadequate training and lack of supervision can negatively influence the quality of nursing documentation. Nurses who do not receive sufficient guidance may experience difficulties maintaining complete and accurate records.
File Management Practices in Healthcare Settings
Effective file management is important for maintaining accessible and organized patient records. Huber (2014) stated that well-organized filing systems improve healthcare efficiency by allowing healthcare professionals to retrieve patient information quickly and accurately. Poor file management, on the other hand, may lead to misplaced records, delays in treatment, and increased workload.
Similarly, Marquis and Huston (2015) reported that ineffective file management systems contribute to communication gaps among healthcare professionals and reduce the overall quality of healthcare services. They emphasized the importance of maintaining organized and standardized record systems within healthcare institutions.
Impact of Documentation Problems on Patient Care
The World Health Organization (2016) highlighted that poor documentation practices can compromise patient safety and increase the risk of healthcare errors. Accurate documentation is considered a key component of safe and effective healthcare delivery. Likewise, the Royal College of Nursing (2016) reported that incomplete documentation may result in communication failures, delays in patient care, and difficulties in monitoring patient progress. The organization stressed that maintaining accurate records is a professional responsibility of every nurse.
Strategies for Improving Documentation and File Management
Several researchers have suggested strategies to improve documentation and file management practices. Joint Commission International (2017) recommended the implementation of standardized documentation systems, regular monitoring, and continuous staff training to improve the quality of healthcare records.
Similarly, Polit and Beck (2017) emphasized that healthcare institutions should provide ongoing education and support to healthcare workers to strengthen documentation practices. They also highlighted the benefits of electronic documentation systems in reducing errors and improving accessibility to patient information.
Recent studies have shown that electronic health record systems can improve the efficiency of healthcare services by reducing paperwork, improving communication, and enhancing patient safety. These systems have become increasingly important in modern healthcare settings as organizations strive to improve the quality and efficiency of patient care.
Summary of the Literature
The reviewed literature demonstrates that documentation and file management are essential for maintaining patient safety, continuity of care, and healthcare quality. Previous studies consistently identify challenges such as incomplete records, poor file organization, difficulties in retrieving information, and inadequate staff training. The literature further suggests that standardized documentation systems, continuous education, regular audits, and electronic record management systems can significantly improve documentation practices and healthcare outcomes.
2.3 Synthesis and Research Gap
The literature reviewed highlights the important role of documentation and file management in ensuring patient safety, continuity of care, effective communication, and overall healthcare quality. Previous studies have consistently shown that accurate and well-organized documentation supports clinical decision-making and reduces the risk of healthcare errors. Researchers such as the American Nurses Association (2010), Burns and Grove (2011), and the World Health Organization (2016) emphasized that proper documentation is a fundamental component of professional nursing practice and quality healthcare delivery.
The reviewed studies also identified several common challenges related to documentation and file management. These include incomplete records, misplaced documents, poor file organization, difficulties in retrieving patient information, inadequate staff training, and lack of standardization in documentation practices. Such challenges have been reported to negatively affect communication among healthcare professionals, increase workload, and compromise patient safety.
Furthermore, the literature suggests several strategies to improve documentation and file management systems, including the introduction of standardized documentation formats, continuous staff training, regular documentation audits, effective supervision, and electronic documentation systems. These interventions have been found to improve accessibility of information, reduce documentation errors, and enhance healthcare efficiency.
Although many studies have examined documentation and file management practices in healthcare settings, there is limited evidence specifically focusing on the experiences of nursing officers working in hospital wards at Base Hospital Sammanthurai. Most previous studies have been conducted in different healthcare settings and may not fully reflect the challenges faced within the local context. In addition, there is insufficient information regarding the specific documentation problems encountered by nursing officers and the practical improvements required in this setting.
Therefore, this study aims to fill this gap by assessing the existing documentation and file management practices among nursing officers at Base Hospital Sammanthurai. The findings of this research are expected to provide valuable information for improving documentation systems, enhancing patient safety, strengthening communication among healthcare professionals, and improving the overall quality of patient care.
METHODOLOGY
3.1 Research design
A quantitative descriptive cross-sectional research design was used in this study to assess the problems associated with documentation and file management practices among nursing officers at Base Hospital Sammanthurai.
A quantitative approach was selected because it allows the researcher to collect numerical data from a larger group of participants and analyse the information using statistical methods. This approach helps provide an objective understanding of the current situation regarding documentation and file management practices.
The descriptive research design was considered appropriate because the study aimed to describe and understand the existing documentation practices, challenges, and recommendations for improvement rather than testing a specific intervention or establishing a cause-and-effect relationship. It enabled the researcher to obtain a clear picture of the issues experienced by nursing officers in their daily work environment.
A cross-sectional design was adopted because data were collected from participants at a single point in time. This design was useful in assessing the current status of documentation and file management practices within the hospital wards during the study period.
The selected research design was suitable for achieving the study objectives, as it provided a systematic and efficient method for gathering information about the experiences, perceptions, and challenges faced by nursing officers regarding documentation and file management practices.
3.2 Population and Sample
Population
The population refers to the entire group of individuals who possess the characteristics relevant to the study and from whom the researcher intends to obtain information. For this study, the target population consisted of all nursing officers working in selected wards at Base Hospital Sammanthurai. Nursing officers were chosen as the study population because they are directly involved in maintaining patient records, documentation activities, and file management practices within the hospital wards.
Sample
A sample is a subset of the population selected to participate in the study. For this research, a total of 80 nursing officers were selected from the target population to participate in the study. A convenience sampling technique was used to recruit participants. This method was chosen because it allowed the researcher to collect data from nursing officers who were readily available and willing to participate during the data collection period. Convenience sampling was considered appropriate due to the accessibility of participants and the practical limitations of time and resources. To ensure that the study remained focused on individuals directly involved in documentation activities, specific inclusion and exclusion criteria were applied.
Inclusion Criteria
Exclusion Criteria
The selected sample provided valuable information regarding the existing documentation and file management practices, challenges encountered by nursing officers, and possible recommendations for improvement within the hospital setting.
3.3 Research Instruments
A research instrument is a tool used by the researcher to collect relevant information from study participants. In this study, data were collected using a structured self-administered questionnaire developed by the researcher based on the study objectives and a review of related literature. The questionnaire was designed to gather information about the existing documentation and file management practices among nursing officers, the challenges they experience, and their suggestions for improvement. A questionnaire was selected as the research instrument because it allows data to be collected from a large number of participants in a relatively short period of time while ensuring consistency in the information obtained.
The questionnaire consisted of four sections:
Section A: Demographic Information
This section collected background information about the participants, including age, gender, years of nursing experience, current working ward or unit, and current position.
Section B: Existing Documentation Practices
This section assessed participants’ views and experiences regarding the current documentation practices in their wards. It included questions related to the organization of patient records, accessibility of information, and effectiveness of the existing documentation system.
Section C: Challenges in File Management
This section focused on identifying the common problems encountered by nursing officers in managing patient records and files. Questions addressed issues such as incomplete documentation, misplaced records, difficulties in retrieving patient information, overcrowded files, and communication problems during patient handovers.
Section D: Recommendations for Improvement
This section explored participants’ opinions regarding possible strategies to improve documentation and file management practices. It included suggestions such as staff training, standardized documentation formats, documentation audits, improved supervision, and electronic documentation systems. Most of the questions were close-ended and used a five-point Likert scale ranging from strongly disagree to strongly agree. This format enabled participants to express their level of agreement with each statement and facilitated the statistical analysis of responses. The structured questionnaire provided a systematic and efficient method for collecting reliable information related to the objectives of the study.
3.4 Validity and Reliability
Validity
Validity refers to the extent to which a research instrument accurately measures what it is intended to measure. In this study, the validity of the questionnaire was ensured through expert review. The questionnaire was carefully developed based on the study objectives and relevant literature related to documentation and file management practices in healthcare settings.
To ensure that the questionnaire adequately covered all aspects of the research topic, it was reviewed by experienced professionals in the fields of nursing and healthcare management. Their feedback and recommendations were considered when revising the questionnaire. Necessary modifications were made to improve the clarity, relevance, and appropriateness of the questions. This process helped ensure that the instrument accurately measured the problems associated with documentation and file management practices among nursing officers.
Reliability
Reliability refers to the consistency and stability of a research instrument in measuring a particular concept. A reliable instrument produces similar results when used under similar conditions. In this study, reliability was maintained by using a structured questionnaire with standardized questions and clear instructions for all participants. The questions were designed in a simple and understandable manner to minimize misunderstanding and ensure consistency in responses.
In addition, all participants received the same questionnaire and completed it under similar conditions. The use of standardized procedures throughout the data collection process helped improve the reliability of the instrument and ensured that the information collected was consistent and dependable. Therefore, the questionnaire was considered suitable for assessing documentation and file management practices among nursing officers.
3.5 Data Collection Procedure
The data collection process was carried out in a systematic and organized manner to ensure the accuracy and quality of the information obtained. Prior to data collection, permission to conduct the study was obtained from the relevant authorities at Base Hospital Sammanthurai. Ethical principles and institutional guidelines were followed throughout the research process.
After receiving approval, the researcher visited the selected wards and explained the purpose, objectives, and importance of the study to the nursing officers. Participants were informed that their participation was entirely voluntary and that the information provided would be kept confidential and used only for research purposes.
Written informed consent was obtained from all participants before distributing the questionnaires. Nursing officers who met the inclusion criteria and agreed to participate were provided with a structured self-administered questionnaire. Clear instructions were given on how to complete the questionnaire, and participants were encouraged to answer all questions honestly and independently.
The questionnaires were completed during designated times that were convenient for the participants and did not interfere with their routine nursing duties. After completion, the questionnaires were collected by the researcher and checked for completeness to ensure that all necessary information had been provided.
The collected questionnaires were then carefully organized, coded, and prepared for data entry and analysis. Throughout the data collection process, the privacy, anonymity, and confidentiality of all participants were strictly maintained.
3.6 Data Analysis Plan
After the completion of data collection, the questionnaires were carefully checked to ensure that all responses were complete and suitable for analysis. The collected data were then coded and entered into the Statistical Package for Social Sciences (SPSS) software for analysis.
The data were analysed using descriptive statistical methods because the main purpose of the study was to describe the existing documentation and file management practices among nursing officers and identify the challenges they experience. Descriptive statistics helped summarize and present the collected information in a clear and meaningful manner.
The statistical techniques used in this study included:
The analysed data were presented according to the objectives of the study. The findings were interpreted and discussed to identify common documentation and file management challenges, assess the effectiveness of current practices, and explore possible recommendations for improvement.
The use of SPSS and descriptive statistical methods enabled the researcher to present accurate, organized, and meaningful findings that addressed the research objectives.
3.7 Ethical Consideration
Ethical considerations were given high priority throughout the research process to protect the rights, dignity, and well-being of the participants. Prior to conducting the study, permission was obtained from the relevant authorities at Base Hospital Sammanthurai to carry out the research.
Before data collection, the purpose, objectives, and procedures of the study were clearly explained to all participants. Nursing officers were informed that their participation in the study was entirely voluntary and that they had the right to refuse participation or withdraw from the study at any stage without any negative consequences. Written informed consent was obtained from all participants before distributing the questionnaires. Participants were assured that the information they provided would be used solely for academic and research purposes.
To maintain confidentiality and anonymity, participants were not required to provide their names or any personal identifiers on the questionnaire. All collected information was treated with strict confidentiality and was stored securely to prevent unauthorized access.
The principles of autonomy, confidentiality, anonymity, beneficence, and non-maleficence were maintained throughout the study. Every effort was made to ensure that the research process caused no physical, psychological, or professional harm to the participants. By adhering to these ethical principles, the researcher ensured that the study was conducted in a responsible, respectful, and professional manner while safeguarding the rights and privacy of all participants.
RESULTS AND DISCUSSION
4.1 Presentation of Results
This chapter presents the findings of the study according to the research objectives. The results are organized into demographic characteristics, documentation and file management practices, challenges experienced by nursing officers, and recommendations for improvement.
4.1.1 Demographic Characteristics of Participants
Table 4.1: Demographic Characteristics
|
Variable |
Category |
Frequency (%) |
|
Age |
20–30 years |
25% |
|
31–40 years |
37.5% |
|
|
41–50 years |
25% |
|
|
Above 50 years |
12.5% |
|
|
Gender |
Male |
15% |
|
Female |
85% |
|
|
Working Area |
General Wards |
80% |
|
Special Units |
20% |
|
|
Experience |
Less than 5 years |
23% |
|
5–10 years |
40% |
|
|
11–20 years |
26% |
|
|
More than 20 years |
11% |
The majority of participants were female nursing officers (85%). Most participants were between 31 and 40 years of age (37.5%), and many had between 5 and 10 years of nursing experience (40%).
4.1.2 Common Documentation and File Management Problems
Table 4.2: Common Documentation and File Management Problems
|
Problem Identified |
Percentage |
|
Difficulty retrieving patient information |
90% |
|
Time-consuming document searches |
72% |
|
Overcrowded files |
54% |
|
Communication issues during handover |
52% |
|
Misplacement of documents |
50% |
|
Incomplete records |
45% |
|
Poor organization of files |
45% |
|
Damaged documents |
42% |
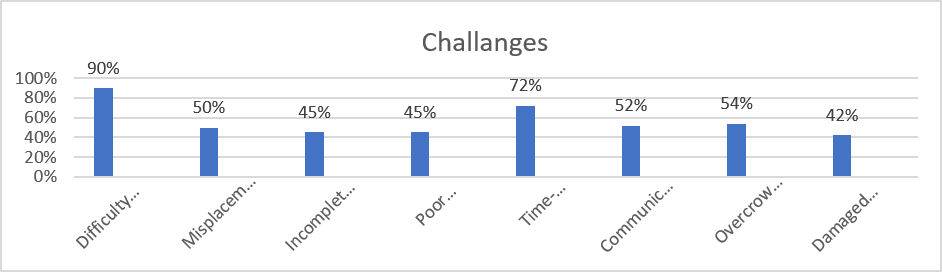
Figure 4.1: Common Documentation and File Management Problems
The findings indicate that difficulty in retrieving patient information was the most commonly reported challenge, followed by time-consuming document searches and overcrowded files.
4.1.3 Suggested Improvements
Table 4.3: Suggested Improvements
|
Recommendation |
Percentage |
|
Stronger file materials |
100% |
|
Standardized file formats |
95% |
|
Better staff training |
88% |
|
Colour-coded file sections |
65% |
|
Improved supervision and monitoring |
65% |
|
Documentation audits |
60% |
|
Electronic documentation systems |
55% |
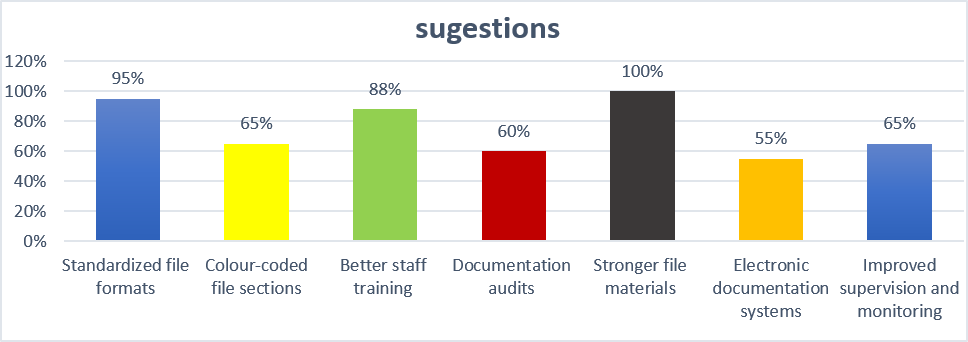
Figure 4.2: Suggested Improvements
Most participants strongly supported the introduction of stronger file materials, standardized documentation formats, and staff training programs.
4.2 Analysis and Interpretation
The findings suggest that nursing officers experience several challenges related to documentation and file management within hospital wards. The high percentage of participants reporting difficulty in retrieving patient information (90%) indicates that the current filing system may not adequately support efficient access to patient records.
Similarly, the finding that 72% of participants reported time-consuming document searches suggests that existing documentation systems may increase workload and reduce productivity. Overcrowded files, misplaced documents, and incomplete records further indicate weaknesses in file organization and record maintenance practices.
The results also demonstrate that documentation problems affect communication among healthcare professionals, particularly during patient handovers. Communication issues reported by more than half of the participants highlight the importance of maintaining accurate and accessible patient records. The recommendations provided by participants indicate a strong need for improvements in documentation systems. The majority believed that standardized file formats, stronger file materials, and staff training could help reduce documentation errors and improve patient care.
4.3 Discussion
The findings of this study are consistent with previous literature that emphasizes the importance of effective documentation and file management in healthcare settings. Similar to the findings reported by the American Nurses Association (2010), this study confirms that documentation plays a vital role in ensuring continuity of care and effective communication among healthcare professionals.
The challenges identified in this study, including incomplete documentation, poor file organization, and difficulties in retrieving patient information, are consistent with the findings of Ellis and Hartley (2012), who reported that inadequate documentation practices continue to be a major concern in healthcare institutions. The finding that many nursing officers experience difficulties retrieving patient information supports the observations of Huber (2014), who noted that ineffective file management systems often contribute to delays in patient care and reduced healthcare efficiency.
Furthermore, participants strongly supported staff training and standardized documentation systems as methods of improvement. This finding is consistent with the recommendations of Polit and Beck (2017), who emphasized that education, supervision, and standardized procedures are essential for improving documentation quality.
The relatively lower support for electronic documentation systems may be due to limited resources, lack of technological infrastructure, or unfamiliarity with digital record systems within the study setting. Overall, the findings demonstrate that strengthening documentation and file management practices has the potential to improve patient safety, communication, and healthcare quality.
4.4 Limitations of the Study
Several limitations were encountered during this study.
First, the study was conducted only among nursing officers working in selected wards at Base Hospital Sammanthurai. Therefore, the findings may not be representative of all healthcare institutions or nursing populations.
Second, the sample size was limited to 80 participants, which may affect the generalizability of the results to a larger population.
Third, the study relied on self-reported information obtained through questionnaires. As a result, responses may have been influenced by personal perceptions, experiences, or recall bias.
Finally, the study was conducted within a limited period of time and focused only on documentation and file management practices. Other factors that may influence healthcare quality were not examined.
Despite these limitations, the study provides valuable insights into the challenges associated with documentation and file management practices and offers practical recommendations for improvement.
CONCLUSION
5.1 Summary of Findings
This study was conducted to assess the problems associated with documentation and file management practices among nursing officers at Base Hospital Sammanthurai and to identify possible recommendations for improvement.
The major findings of the study are summarized as follows:
Overall, the findings indicate that improvements in documentation and file management practices are necessary to support effective healthcare delivery and patient safety.
Documentation and file management are essential components of quality nursing care and healthcare service delivery. The findings of this study revealed that nursing officers experience several challenges related to maintaining and managing patient records within hospital wards. Difficulties in retrieving information, misplaced documents, overcrowded files, and communication issues were among the most commonly reported problems.
These challenges can increase the workload of nursing officers, reduce healthcare efficiency, and potentially affect patient safety and continuity of care. The study highlights the need for strengthening existing documentation and file management systems to ensure that patient information is accurate, organized, and easily accessible when needed.
Based on the findings, it can be concluded that improving documentation and file management practices through proper training, standardization, supervision, and system improvements can contribute significantly to better communication, improved patient safety, and higher quality healthcare services. Therefore, healthcare institutions should give greater attention to strengthening documentation systems as an important component of quality patient care.
5.2 Recommendations
Practical Recommendations
Based on the findings of this study, the following recommendations are proposed:
Recommendations for Future Research
In conclusion, strengthening documentation and file management systems is essential for improving patient safety, enhancing communication among healthcare professionals, and ensuring the delivery of high-quality healthcare services.
REFERENCES

Prabashankar Dharmalingam, Mohamed Ibrahim Siyath Ismail, Ruwan Srilal Dalpadado, Yathavan Selvarajan, Mohamed Ismail Mohamed Asher, Assessment of Documentation and Record Management Challenges Among Nursing Officers at Base Hospital Sammanthurai, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 4778-4795. https://doi.org/10.5281/zenodo.20752161
 10.5281/zenodo.20752161
10.5281/zenodo.20752161