
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy Practice, Hillside College of Pharmacy and Research Centre, Raghuvanahalli, Kanakpura Main Road, Bengaluru 560062, Karnataka, India.
Background: Postoperative shoulder tip pain remains a common complication after cholecystectomy, affecting patient comfort and recovery despite advances in analgesic management.Objective: To evaluate the incidence of postoperative shoulder tip pain and to analyse analgesic prescribing trends following cholecystectomy.Methods: A prospective observational study was conducted over six months at a tertiary care hospital, involving adult patients undergoing cholecystectomy. Clinical and demographic data, postoperative pain outcomes, and analgesic prescribing patterns were collected and statistically analysed using SPSS version 26.Results: Of 182 enrolled patients, 166 completed follow-up and were included in the final analysis. Postoperative shoulder tip pain was observed in 48.2% of patients. A statistically significant association was found between higher body mass index (BMI) and pain severity, with Obese Class II/III patients demonstrating a greater burden of severe pain (F = 6.72, p = 0.0003). No significant association was found between gender and pain incidence or severity (p > 0.05). Analgesic prescribing predominantly favoured multimodal therapy (65.1%) over monotherapy (34.9%), with paracetamol incorporated into 91.0% of treatment regimens. Female patients showed significantly higher utilisation of adjunctive analgesics, including NSAIDs, dexamethasone, and opioids, compared with males (p < 0.05).Conclusion: Shoulder tip pain remains a frequent postoperative complication after cholecystectomy, with BMI significantly influencing pain severity. Multimodal analgesia, particularly paracetamol-based regimens, predominated in postoperative management, underscoring the need for individualised pain-control strategies.
Gallstones are a relatively common digestive-system disorder, particularly among adults. Approximately 10-15% of individuals develop gallstones annually, although only a small proportion become symptomatic. Gallstone formation results from a chemical imbalance in bile - a digestive fluid produced by the liver and stored in the gallbladder - in which cholesterol and other constituents solidify into stone-like deposits[1]. While most affected individuals remain asymptomatic, approximately 20% eventually require surgical intervention[2].
Two surgical approaches are employed for cholecystectomy: the traditional open method, which involves a large abdominal incision and is associated with prolonged recovery and greater postoperative discomfort, and laparoscopic cholecystectomy (LC)[3]. LC is a minimally invasive technique that uses specialised instruments and small incisions, offering reduced pain, shorter hospital stays, and faster recovery. Owing to these benefits - including lower morbidity, fewer complications, and improved cosmetic outcomes - LC has become the gold standard for cholecystectomy[4]. However, up to 15-30% of patients may develop post-cholecystectomy syndrome (PCS)[5].
Postoperative shoulder tip pain remains a significant concern following LC despite the minimally invasive nature of the procedure. This pain typically manifests within the first 24-48 hours after surgery and is widely recognised as referred pain resulting from phrenic nerve irritation secondary to diaphragmatic and peritoneal stimulation. One of the critical intraoperative factors influencing the incidence of shoulder tip pain is the pressure of carbon dioxide insufflation used to create pneumoperitoneum[6]. High-pressure pneumoperitoneum (typically 12-15 mmHg) is associated with greater peritoneal stretching and diaphragmatic irritation, intensifying phrenic nerve stimulation and producing more severe referred shoulder pain. In contrast, low-pressure insufflation (approximately 7-8 mmHg) has been shown to significantly reduce both the intensity and frequency of shoulder tip pain without compromising the surgical field or procedural safety[7].
In clinical practice, low-pressure pneumoperitoneum is often preferred for patients who are young, lean, or otherwise predisposed to postoperative discomfort, such as those with a low pain threshold or prior visceral sensitivity, and is increasingly used in patients with cardiopulmonary comorbidities because lower intra-abdominal pressures minimise haemodynamic and respiratory changes. Conversely, standard-pressure insufflation (12-14 mmHg) is conventionally used in the general population and in cases where optimal surgical-field visibility is prioritised, particularly in patients with obesity, previous abdominal surgery, or anticipated intraoperative difficulty[8]. The choice between low- and standard-pressure insufflation is therefore individualised, based on patient factors, surgeon preference, and intraoperative findings[9].
LC, a common minimally invasive procedure for gallstone disease, is frequently associated with postoperative pain that requires effective analgesic management. Agents such as intravenous paracetamol, NSAIDs, dexamethasone, magnesium sulfate, gabapentinoids, and alpha-2 agonists have demonstrated clinical efficacy in controlling postoperative pain while reducing opioid consumption. Regional techniques, including transversus abdominis plane (TAP) blocks and intraperitoneal local anaesthetic administration, have also gained attention for their role in targeted pain relief[10]. Despite the increasing focus on postoperative pain management after LC, there is currently no well-established method for the prevention and treatment of shoulder tip pain, and the published literature shows considerable variation and conflicting evidence regarding the effectiveness of different analgesic strategies. Furthermore, despite its substantial influence on patient comfort and surgical recovery, shoulder tip pain is frequently overshadowed by incisional and visceral pain in clinical attention. Consequently, identifying the optimal analgesic regimen for shoulder tip pain following cholecystectomy remains an area of ongoing research and discussion.
2. MATERIALS AND METHODS
2.1 Study Design
A prospective observational design was used to assess postoperative recovery in real time.
2.2 Study Duration
The study was conducted over a period of six months.
2.3 Study Setting
The study was conducted in the Department of Gastroenterology and General Surgery at BGS Global Institute of Medical Sciences (BGS GIMS), Bengaluru.
2.4 Sources of Data
Clinical and demographic information was obtained through a detailed review of patients' medical records. Additional data were gathered through direct observation of patients during routine ward rounds, allowing real-time assessment of postoperative symptoms and recovery.
2.5 Eligibility Criteria
Inclusion criteria:
Exclusion criteria:
2.6 Study Procedure
This prospective observational study was conducted in the surgery department of a tertiary care hospital in Bengaluru. Patients above 18 years of age diagnosed with biliary colic and undergoing cholecystectomy (open or laparoscopic) were enrolled according to the predefined inclusion and exclusion criteria.
Informed consent was obtained from each patient or an attendee prior to data collection, which was conducted using a structured data-collection form. Data were gathered from a combination of medical records, direct ward-round observation, and discussion with the treating healthcare professional. Each patient was followed from admission to discharge, and data on demographics, clinical history, laboratory investigations, and treatment were recorded.
Outcomes including postoperative nausea and vomiting, shoulder tip pain, length of hospital stay, analgesic use, and overall recovery were recorded in Microsoft Excel and subsequently analysed.
2.7 Statistical Analysis
Data were analysed using IBM SPSS Statistics, version 26. Categorical variables were summarised as frequencies and percentages and compared using the Chi-square test. Continuous variables were expressed as mean ± standard deviation and compared across groups using one-way analysis of variance (ANOVA), with Tukey's honestly significant difference (HSD) test applied for post-hoc pairwise comparisons. A p-value < 0.05 was considered statistically significant.
3. RESULTS
A minimum sample size of 162 was calculated a priori and subsequently adjusted to 182 to accommodate anticipated attrition. A total of 182 patients were enrolled from the General Surgery and Gastroenterology departments of BGS GIMS, Bengaluru. Of these, 166 patients (91.2%) completed the study and were included in the final analysis, while 16 patients (8.8%) were lost to follow-up and classified as dropouts.
3.1 Demographic Profile
The majority of patients were in the 28-47-year age range, which together accounted for over half of the study population (Table 1). Females constituted the majority of the cohort (60.84%), compared with males (39.16%) (Table 2). This age and gender distribution is broadly representative of the population typically presenting for cholecystectomy at tertiary care centres in India, supporting the applicability of the study findings to routine surgical practice in comparable hospital settings.
Table 1. Age distribution of the study population (N = 166)
|
Age Group (years) |
Number of Patients |
Percentage |
|
18-27 |
24 |
14.46% |
|
28-37 |
42 |
25.30% |
|
38-47 |
45 |
27.11% |
|
48-57 |
32 |
19.28% |
|
58-67 |
13 |
7.83% |
|
68-77 |
10 |
6.02% |
|
Total |
166 |
100.00% |
Table 2. Gender distribution of the study population (N = 166)
|
Gender |
Number of Patients |
Percentage |
|
Male |
65 |
39.16% |
|
Female |
101 |
60.84% |
|
Total |
166 |
100.00% |
3.2 Incidence of Shoulder Tip Pain by Body Mass Index
Table 3. Incidence of shoulder tip pain by BMI category
|
BMI Category |
BMI Range (kg/m²) |
Total Patients |
Pain Present |
Pain Absent |
Pain Incidence |
|
Underweight |
< 18.5 |
2 |
2 |
0 |
100.0% |
|
Normal weight |
18.5-24.9 |
66 |
29 |
37 |
43.9% |
|
Overweight |
25.0-29.9 |
50 |
20 |
30 |
40.0% |
|
Obese Class I |
30.0-34.9 |
18 |
12 |
6 |
66.7% |
|
Obese Class II |
35.0-39.9 |
13 |
9 |
4 |
69.2% |
|
Obese Class III |
≥ 40.0 |
17 |
8 |
9 |
47.1% |
|
Total |
|
166 |
80 |
86 |
48.2% |
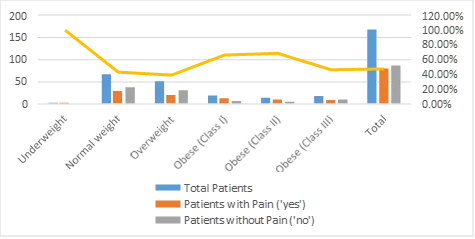
Figure 1. Incidence of shoulder tip pain across BMI categories
Overall, 48.2% of the 166 patients assessed experienced postoperative shoulder tip pain. When stratified by BMI category, incidence was highest among underweight (100.0%) and Obese Class II (69.2%) patients, followed by Obese Class I (66.7%). The lowest incidence was observed in the overweight group (40.0%), while Obese Class III patients showed an incidence of 47.1%. A Chi-square test of independence found no statistically significant association between BMI category and pain incidence (χ²(5) = 8.75, p = 0.12). Nonetheless, from a bedside perspective, a nearly one-in-two incidence of shoulder tip pain indicates that this complication remains a routine, foreseeable event after cholecystectomy rather than an occasional occurrence, supporting its inclusion as a standard counselling point during preoperative patient education and consent.
3.3 Pain Incidence and Severity by Gender
Table 4. Shoulder tip pain severity by gender
|
Pain Severity |
Female |
Male |
Total |
|
None |
80 |
54 |
134 |
|
Mild |
8 |
5 |
13 |
|
Moderate |
6 |
5 |
11 |
|
Severe |
7 |
1 |
8 |
|
Total |
101 |
65 |
166 |
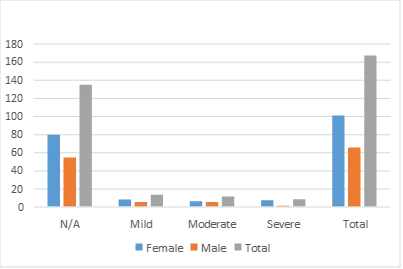
Figure 2. Distribution of shoulder tip pain severity by gender
The association between gender and shoulder tip pain incidence (present/absent) was assessed using a Chi-square test of independence, which revealed no statistically significant association (χ²(1, N = 166) = 0.43, p = 0.51), with a small effect size (Cramér's V = 0.05). The relationship between gender and ordinal pain-severity levels (none, mild, moderate, severe) was further examined using a Chi-square test for trend, which likewise showed no significant association (χ²(1) = 0.36, p = 0.55). In practical terms, this indicates that clinicians need not stratify shoulder tip pain surveillance or analgesic planning by patient sex alone; both male and female patients warrant equivalent vigilance for this complication in routine postoperative care.
3.4 Association Between BMI and Pain Severity
Table 5. Mean BMI by pain severity category
|
Pain Severity |
Count |
Mean BMI (kg/m²) |
SD |
|
No Pain |
126 |
26.2 |
4.8 |
|
Mild |
18 |
27.1 |
5.6 |
|
Moderate |
14 |
28.9 |
7.1 |
|
Severe |
8 |
33.5 |
8.9 |
|
Total |
166 |
26.8 |
5.6 |
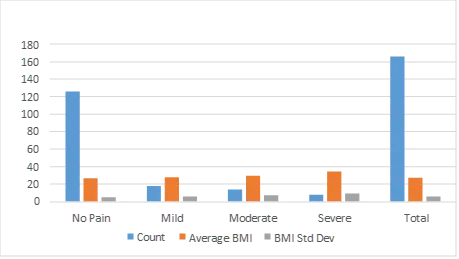
Figure 3. Mean BMI across pain severity categories
A one-way ANOVA revealed a statistically significant difference in mean BMI across pain-severity groups (F = 6.72, p = 0.0003). Post-hoc Tukey's HSD testing confirmed that the severe-pain group (mean BMI = 33.5) had a significantly higher BMI than both the no-pain (mean BMI = 26.2) and mild-pain (mean BMI = 27.1) groups. Categorisation of BMI further indicated a trend of increasing pain likelihood and severity with higher BMI. Although the underweight category showed a 100% pain incidence, this finding was based on a very small subgroup (n = 2). Clinically, the most notable finding was that the Obese Class II/III group (BMI > 35) accounted for 75% (6/8) of all severe pain cases recorded in the study. From a practice standpoint, this finding supports incorporating BMI into preoperative risk stratification for postoperative pain, and suggests that patients with a BMI above 35 may benefit from pre-emptive, escalated multimodal analgesia rather than a reactive, as-needed approach.
3.5 Analgesic Prescribing Patterns
Table 6Analgesic prescribing trends (N = 166)
|
Therapy |
Count |
Percentage |
|
Combination Therapy |
108 |
65.10% |
|
Paracetamol + NSAID + Dexamethasone |
42 |
25.30% |
|
Paracetamol + Dexamethasone |
31 |
18.70% |
|
Paracetamol + NSAID |
26 |
15.70% |
|
Other Combinations |
9 |
5.40% |
|
Monotherapy |
58 |
34.90% |
|
Paracetamol only |
43 |
25.90% |
|
Other single agent |
15 |
9.00% |
|
Total |
166 |
100.00% |
3.6 Analgesic Prescribing by Gender
Table 7. Adjunctive analgesic use by gender
|
Analgesic Category |
Males (n = 65) |
Females (n = 101) |
|
Dexamethasone |
25 (38.5%) |
56 (55.4%) |
|
NSAIDs |
20 (30.8%) |
51 (50.5%) |
|
Opioids (tramadol, morphine, fentanyl) |
3 (4.6%) |
21 (20.8%) |
A total of 166 patient records were analysed for analgesic prescribing patterns, comprising 101 females (60.8%) and 65 males (39.2%), reflecting a significant gender imbalance in the cohort (χ²(1) = 7.81, p < 0.01). Combination analgesic regimens predominated overall, accounting for 108 cases (65.1%) compared with 58 cases (34.9%) for monotherapy. Paracetamol served as the foundational agent, present in 151 cases (91.0%).
A significant gender-based disparity was observed in the use of multimodal analgesia. Female patients were significantly more likely than males to receive adjunctive medications: dexamethasone (55.4% vs 38.5%, p < 0.05), NSAIDs (50.5% vs 30.8%, p < 0.01), and opioids (tramadol, morphine, fentanyl) (20.8% vs 4.6%, p < 0.005). In everyday practice, this disparity was not explained by a corresponding difference in objective pain severity between the sexes (Section 3.3), raising the possibility that prescribing decisions were influenced by clinician assumptions about pain tolerance or by differences in how patients communicated discomfort, rather than by pain severity alone.
3.7 Summary of Clinical Relevance
Taken together, the results reflect prescribing and pain-management patterns as they occur in routine, day-to-day surgical practice rather than under trial conditions, which strengthens the real-world applicability of the findings. Three practice-relevant signals emerge. First, shoulder tip pain affects roughly half of all patients undergoing cholecystectomy, confirming it as an expected rather than exceptional postoperative event that merits routine anticipation, monitoring, and patient counselling. Second, elevated BMI - and in particular Obese Class II/III status - identifies a subgroup of patients at demonstrably higher risk of severe pain, offering a simple, readily available bedside parameter (height and weight) that could be used to flag patients for more proactive, multimodal analgesic planning. Third, current prescribing already reflects a strong shift toward paracetamol-based multimodal therapy, but the unexplained gender disparity in adjunctive drug use points to an opportunity for a standardised, criteria-based analgesic protocol that reduces variability driven by clinician discretion rather than clinical need. These signals collectively indicate meaningful potential for translating the study's findings into a practical, low-cost risk-stratification and prescribing checklist that could be piloted at the study institution and evaluated in future multi-centre work.
4. DISCUSSION
The initial sample-size calculation yielded a requirement of 162 subjects, which was subsequently inflated to 182 to accommodate an expected rate of attrition. Enrolment achieved this target, with 182 patients recruited from the specified departments. At study conclusion, 166 participants (91.2%) had completed all follow-up requirements, while the remaining 16 patients (8.8%) were lost to follow-up and classified as dropouts.
The pronounced female predominance observed in this study (60.84%) is consistent with the well-established global epidemiological trend for gallstone disease requiring cholecystectomy. This finding is corroborated by the larger study of Kaleem Ullah et al., who reported a comparable, though more pronounced, female majority of 77.76% (male-to-female ratio of 1:3)[11]. The similarity between the two studies underscores the well-recognised female predisposition to gallstone disease, attributed primarily to hormonal factors: oestrogen increases biliary cholesterol secretion and decreases bile-acid synthesis, promoting cholesterol supersaturation and nucleation. Additional risk factors, including multiparity and oral contraceptive use, further elevate risk in females[11].
In this study, 48.2% of patients reported postoperative shoulder pain, with incidence varying across BMI categories. The highest rates were observed at both extremes of the BMI range - underweight (100%) and Obese Class II (69.2%) - while overweight patients showed the lowest incidence (40%). A Chi-square test found this association not to be statistically significant (χ²(5) = 8.75, p = 0.12), suggesting a possible U-shaped relationship between BMI and pain, in which both low and high BMI are associated with a greater prevalence of discomfort. These findings differ from previous reports: Jiang et al. identified low BMI (< 24 kg/m²) as a significant independent predictor of shoulder pain, and while the present data likewise show elevated pain among underweight individuals, low BMI could not be confirmed as an independent risk factor in this cohort. Other studies have instead reported that higher average BMI correlates with more severe pain; the present findings, showing elevated pain at both ends of the BMI spectrum, suggest a more complex relationship[13].
This contrast is further highlighted when comparing the present results with those of Menegassi et al., who reported a strong association between morbid obesity and shoulder pain. The discrepancy may reflect differences in study populations: the present study included a mixed surgical cohort across all BMI categories, whereas Menegassi et al. focused specifically on morbidly obese patients within a bariatric-surgery context[14].
No significant association was observed between gender and either the incidence or severity of shoulder tip pain, indicating that male and female patients experienced postoperative pain in a broadly comparable manner. This contrasts with Rau et al., who identified notable sex-related differences in the qualitative description of shoulder pain, a divergence that may reflect differences in the subjective expression of pain rather than in its objective incidence or severity[15]. The absence of a gender effect in the present study may be attributable to the standardised, acute nature of postoperative pain assessment, which tends to minimise variability in reporting. Collectively, these findings suggest that while gender may not alter the measurable severity of pain, it may influence the language and descriptors used to communicate the pain experience - highlighting the value of considering both quantitative pain scores and qualitative descriptors when evaluating gender-related differences in pain perception[15].
The present study demonstrated a predominant use of combination therapy (65.1%) over monotherapy (34.9%) in postoperative pain management, with paracetamol the most frequently prescribed agent (91.0% of regimens). Significant gender-based variation was observed, with female patients more frequently receiving adjunctive agents such as dexamethasone, NSAIDs, and opioids compared with males. These findings highlight the increasing reliance on multimodal analgesia and the influence of demographic factors on prescribing practice. In a related investigation of pre-emptive analgesia in laparoscopic cholecystectomy, ketamine was shown to reduce postoperative pain scores and analgesic requirements, with a lower dose (0.5 mg/kg) providing optimal efficacy while avoiding adverse effects. Whereas the present study assessed broad prescribing patterns across a large cohort, this comparator study focused on the efficacy of a specific pharmacological intervention; together, the two lines of evidence indicate that postoperative pain can be managed through complementary approaches - either by optimising prescribing practice through multimodal regimens or by introducing evidence-based pharmacological strategies such as pre-emptive ketamine[16].
In a different approach, Radaideh et al. directly tested a specific two-drug combination - intravenous paracetamol and tramadol - in patients undergoing laparoscopic cholecystectomy, and found this combination more effective than placebo in reducing postoperative pain; patients receiving the combination required less rescue medication and reported no major adverse effects. Whereas the present study describes real-world prescribing habits, Radaideh et al. conducted a controlled trial establishing the efficacy of a specific treatment[17]. Together, these studies provide complementary evidence: the present study describes how clinicians prescribe analgesia in real-world practice and how patient factors such as gender influence these choices, while Radaideh et al. provide experimental evidence that a specific paracetamol-tramadol combination is safe and effective. Both lines of evidence affirm that paracetamol is a fundamental component of modern analgesic practice, and that its use within a multimodal strategy is important for optimal patient care after laparoscopic cholecystectomy[17].
5. CONCLUSION
This study, conducted in 166 patients who underwent cholecystectomy at a tertiary care teaching hospital in Bengaluru, provides a comprehensive assessment of demographic distribution, postoperative complications, recovery patterns, and analgesic prescribing practice. All statistical analyses were performed using SPSS software (version 26), ensuring robust and reliable computation of results.
Pain analysis revealed that 48.2% of patients experienced postoperative shoulder tip pain, with incidence and severity strongly associated with higher BMI categories. Although underweight patients showed a 100% incidence, this finding was based on a very small subgroup. Obese Class II/III patients not only had a higher pain prevalence but also accounted for the majority of severe pain cases, reinforcing the clinical relevance of BMI as a predictor of postoperative shoulder pain. Gender showed no statistically significant association with pain incidence or severity.
Analysis of analgesic prescribing patterns highlighted a marked shift toward multimodal therapy, with 65.1% of patients receiving combination regimens. Paracetamol emerged as the cornerstone analgesic, prescribed in over 90% of cases. A significant gender-based disparity was observed, with female patients more frequently receiving multimodal therapy, including higher rates of dexamethasone, NSAID, and opioid administration compared with males.
6. LIMITATIONS
1. Single-centre study design: The study was conducted at BGS GIMS, Bengaluru, which may limit the generalisability of findings to other populations or healthcare settings with different patient demographics and clinical practices.
2. Sample size constraints: Although 166 patients were included, subgroup analyses (e.g., underweight, Obese Class II/III) involved small numbers, which may have inflated percentages and reduced the statistical reliability of those observations.
3. Observational and cross-sectional nature: As the study was observational rather than randomised, causal relationships cannot be firmly established between BMI, pain, and recovery outcomes.
4. Potential reporting and measurement bias: Pain and recovery assessment relied partly on patient self-report, which may be subject to individual perception, recall bias, or under- or over-reporting of symptoms.
5. Confounding variables not fully controlled: Factors such as comorbidities, anaesthesia technique, intraoperative medications, and postoperative care variation were not controlled in detail and may have influenced pain, nausea, or recovery outcomes.
6. Limited follow-up period: The study assessed early postoperative recovery and complications but did not capture long-term outcomes such as chronic pain, late-onset post-cholecystectomy syndrome, or quality of life beyond discharge.
7. Analgesic prescribing influenced by physician discretion: Analgesic regimens were not standardised but based on clinician judgement, which may have introduced variability and potential bias in prescribing patterns.
8. Statistical limitations: Although SPSS version 26 was used for analysis, some subgroup comparisons had reduced statistical power due to small sample sizes, and multiple testing may have increased the risk of Type I error.
7. FUTURE DIRECTIONS
1. Multi-centre validation: Conduct a large, multi-centre study to confirm the associations between BMI, pain, and recovery quality across diverse populations.
2. Interventional trials: Design randomised controlled trials (RCTs) to test BMI-stratified perioperative protocols for analgesia and antiemetic prophylaxis.
3. Long-term follow-up: Extend the research timeline to assess long-term outcomes, including chronic pain and quality of life at 6 and 12 months post-surgery.
4. Mechanistic studies: Investigate the physiological mechanisms (e.g., pharmacokinetics, inflammatory biomarkers) underlying the relationship between BMI and pain severity.
5. Qualitative exploration: Use patient interviews to gain deeper insight into the subjective experiences underlying pain outcomes, particularly in high-BMI patients.
6. Standardisation and implementation: Develop and implement an evidence-based, standardised analgesic protocol to address the prescribing variability observed in this study.
7. Larger subgroup samples: Replicate the study with a sufficiently large sample to allow robust, adequately powered analysis of all BMI subcategories (e.g., underweight, Obese Class III).
CONFLICT OF INTEREST
The authors declare no conflicts of interest regarding this investigation.
ACKNOWLEDGMENTS
The authors thank Dr. S. N. Sriharsha, Principal, Hillside College of Pharmacy and Research Centre, Bengaluru, for his support and guidance throughout this study.
REFERENCES


Md Farhan, Deeksha V, Arpita Roy Barman, Dr. Saba Farooqui, Dr. Jesindha Beyatricks, Beyond the Incision: Shoulder Tip Pain and Evolving Analgesic Strategies After Cholecystectomy, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2255-2266, https://doi.org/10.5281/zenodo.21305680
 10.5281/zenodo.21305680
10.5281/zenodo.21305680