
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Vidyaniketan College of Pharmacy, Anjangaon Surji, Amravati, Maharashtra 444705
Hemorrhoids, commonly known as piles, are a prevalent anorectal disorder affecting a significant proportion of the global population and are associated with symptoms such as pain, bleeding, itching, prolapse, and discomfort, which markedly impair quality of life. Conventional treatment approaches, including pharmacological agents and surgical procedures, provide symptomatic relief but are often associated with adverse effects, recurrence, and limited long-term efficacy. This has led to increasing interest in herbal and botanical therapies as safer and more holistic alternatives. The present review highlights the etiology, classification, risk factors, and pathophysiology of hemorrhoids, with particular emphasis on the therapeutic potential of medicinal plants used in traditional systems such as Ayurveda, Traditional Chinese Medicine, and Unani medicine. Various medicinal plants including Terminalia chebula, Aloe vera, Curcuma longa, Eclipta prostrata, and Leucas aspera are discussed for their phytochemical constituents such as flavonoids, tannins, saponins, terpenoids, and polyphenols, which exhibit anti-inflammatory, antioxidant, venotonic, analgesic, and wound-healing activities. The review also explores their pharmacological mechanisms, formulation development, standardization parameters, and comparison with synthetic drugs. Clinical and experimental studies indicate that herbal formulations, especially polyherbal preparations, offer promising efficacy with minimal side effects and improved patient compliance. Thus, standardized evidence-based herbal therapies may serve as effective complementary or alternative approaches for the management of hemorrhoids, supporting the integration of traditional knowledge with modern pharmaceutical research
Hemorrhoids, often known as piles, are among the most frequent anorectal conditions that affect people all over the world. They are described as symptomatic distal displacement and expansion of the typical anal cushions, which are vascular structures in the anal canal that aid in continence. An estimated 40% of adults will experience symptoms at some point in their lives, especially those between the ages of 45 and 65 [1]. This disease is a major worldwide health burden. Hemorrhoids are not life-threatening, but they can significantly lower quality of life due to pain, bleeding, discomfort, and social shame. Depending on nutritional, occupational, and geographic factors, the precise worldwide frequency ranges from 4.4% to 36% [2]. Urbanized and industrialized societies tend to report higher prevalence rates due to sedentary lifestyles and low-fiber diets. In developing countries, hemorrhoids are often underreported owing to stigma and lack of healthcare access. Studies have revealed that the condition contributes significantly to healthcare expenditure due to the need for long-term treatment, repeated consultations, and potential surgical interventions [3].
Conventional treatments primarily include pharmacological management and surgical procedures. Synthetic medications such as corticosteroids, vasoconstrictors, local anesthetics, and flavonoid-based venotonic agents offer symptomatic relief but often produce side effects like mucosal thinning, allergic reactions, and rebound inflammation upon prolonged use [4]. Moreover, surgical options such as hemorrhoidectomy, rubber band ligation, and sclerotherapy, while effective in severe cases, are associated with pain, infection risk, and postoperative recurrence [5]. In recent years, there has been a growing shift toward herbal and phytotherapeutic interventions for hemorrhoids management. Herbal remedies, used in traditional systems such as Ayurveda, Siddha, Unani, and Traditional Chinese Medicine (TCM), are valued for their multi-targeted mechanisms, minimal side effects, and cost-effectiveness. Plants rich in flavonoids, tannins, saponins, and phenolic compounds have demonstrated promising anti-inflammatory, venotonic, analgesic, and wound-healing properties [6,7].
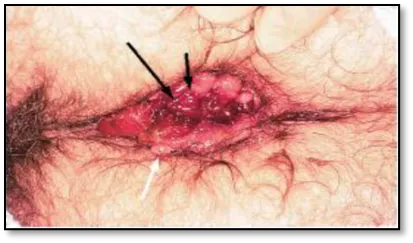
Figure 1:close-up hemorrhoidal
Overview of Hemorrhoids:
Etiology and Pathogenesis
The pathological dilatation and distal displacement of the anal canal's vascular cushions cause hemorrhoids [8]. These cushions, which make up of smooth muscle fibers, connective tissue, and arteriovenous channels, contribute 15–20% of the resting anal pressure to preserve anal continence. When these cushions experience structural degradation and venous engorgement as a result of elevated intra-abdominal pressure or a weakening of the supporting connective tissue, the illness arises. Chronic constipation, prolonged straining during feces, diarrhea, pregnancy, obesity, and a sedentary lifestyle are some of the variables that lead to the development of hemorrhoids [9]. Anal mucosal prolapse, inflammation, and vascular hyperplasia are the results of repeated mechanical stress.
Classification of Hemorrhoids
Hemorrhoids are categorized according to the degree of prolapse and their anatomical position in relation to the dentate line. Internal hemorrhoids are covered in columnar epithelium and develop above the dentate line. They may bleed, but they are painless. Stratified squamous epithelium covers external hemorrhoids, which are located below the dentate line and frequently cause discomfort because of somatic innervation. Both areas are affected by mixed hemorrhoids [8]. Internal hemorrhoids are classified as follows according to Goligher's classification:
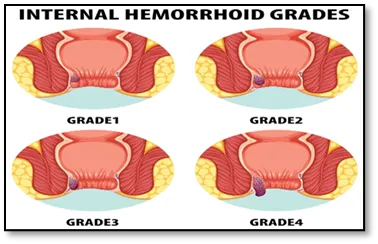
Figure 2:Internal hemorrhoids grades [51]
Grade I: bleeding without prolapse.
Grade II: prolapse when straining but spontaneously diminish.
Grade III: require manual reduction.
Grade IV: Irreducible prolapse that is unpleasant and frequently thrombosed [8,9].
Signs and Symptoms
Risk Elements
Constipation and straining: Prolonged constipation and straining during bowel movements raise intra-abdominal and venous pressure, which causes venous prolapse and dilatation.
Pregnancy: Women are more susceptible to hemorrhoids, particularly in the third trimester, due to venous stasis and smooth muscle relaxation brought on by the growing uterus and hormonal changes
Obesity and Sedentary Lifestyle: Venous pooling is exacerbated by decreased physical activity, which weakens the rectal support tissues and pelvic floor [9].
Dietary habits: Diets heavy in fat and low in fiber cause stool hardness and delayed bowel movements, which result in excessive straining.
Age and Genetics: Hemorrhoidal vulnerability is influe.
Liver cirrhosis and portal hypertension: Hemorrhoidal congestion may worsen if venous pressure is elevated.
The clinical manifestations of hemorrhoids vary depending on the grade and type. Common symptoms include rectal bleeding during or after defecation, pain, itching (pruritus ani), mucus discharge, prolapse, and perianal swelling [3,8]
Need for Alternative and Botanical Remedies:
The chronic and recurrent character of hemorrhoids cannot be addressed by synthetic or surgical treatments, notwithstanding their effectiveness in acute care. Furthermore, there is a resurgence of interest in herbal remedies due to modern lifestyles, dietary changes, and the emergence of drug resistance. Among the many pharmacological advantages of botanicals are their anti-inflammatory, antioxidant, and vasoprotective properties. Phytochemicals like tannins, saponins, and flavonoids (including diosmin, hesperidin, and rutin) maintain capillary permeability, lower inflammation, and aid in healing. Many plant species, including Terminalia chebula, Eclipta prostrata, Houttuynia cordata, Leucas aspera, Aloe vera, Curcuma longa, and Psidium guajava, have been used to treat hemorrhoids in traditional medicine systems around the world, including Ayurveda, Unani, Siddha, and TCM.Many of these plants have been scientifically validated for their anti-inflammatory and wound-.restorative qualities, indicating the therapeutic potential of phytotherapy in the treatment of piles [6,10].
Ayurveda and Indian Traditional Medicine
In Ayurvedic literature, hemorrhoids are called Arsha (meaning "enlargement near the rectal passage"). Based on the predominance of biological humors (doshas), they are classified into Vataja, Pittaja, Kaphaja, and Sannipataja categories[11]. The illness is believed to be caused by digestive issues and improper excretion, which results in pressure building up in the rectal veins (Agni Mandya). Even now, traditional Ayurvedic treatments like Arshoghna and Triphala Guggulu are often advised. Herbs such as Terminalia chebula, Terminalia bellirica, Emblica officinalis, Curcuma longa, Cassia fistula, and Aloe vera are commonly used because of their astringent, anti-inflammatory, and wound-healing properties.
Traditional Chinese Medicine (TCM)
Hemorrhoids are referred to as "Zhi Chuang" in TCM, and they are mostly linked to Qi stagnation and blood heat in the rectal area. The main goals of remedies are to increase blood flow, remove heat, and lessen swelling. Herbs including Radix Scutellariae, Coptis chinensis, Aesculus hippocastanum, Rheum officinale, and Sophora japonica (Huai Hua) are used topically or in decoctions [14].
Western Herbal Traditions and Unani
Hemorrhoids (Bawasir) are regarded in Unani medicine as a sign of disturbed humor (balgham and dam). Herbs such as Plantago ovata, Ficus religiosa, Commiphora mukul, Mimosa pudica, and Cinnamomum zeylanicum are used to treat venous engorgement and restore humoral equilibrium [16]. Roghan-e-Khar-e-Khasak (herbal oil) and Habb-e-Muqil (tablets based on guggul) are among the preparations.
Need for Alternative and Botanical Remedies
Inflammation, oxidative stress, venous insufficiency, and mucosal healing are among the mechanisms linked to hemorrhoid etiology that are targeted by herbal therapy. Flavonoids, tannins, saponins, alkaloids, and terpenoids are just a few of the many bioactive phytochemicals found in medicinal plants that work in concert to relieve ailments.
Anti-Inflammatory and Venotonic Effects
A key factor in hemorrhoidal disease is inflammation. By blocking the cyclooxygenase (COX), lipoxygenase (LOX), and NF-κB pathways, phytochemicals such as quercetin, rutin, diosmin, and hesperidin demonstrate strong anti-inflammatory properties [19]. These substances lessen tissue irritation and vascular congestion by downregulating pro-inflammatory mediators like prostaglandins, IL-1β, and TNF-α. Citrus species include diosmin and hesperidin, which are utilized clinically as venotonic drugs to improve venous return.
Important Medicinal Plants and Their Phytochemical Profile in Hemorrhoid:
|
Plant Name & Family |
Active Phytochemicals |
Mechanism of Action |
Experimental / Clinical Evidence |
Reference |
|
Terminalia chebula (Combretaceae) |
Tannins, chebulagic acid, gallic acid |
Astringent, antioxidant, antimicrobial, mucosal protection |
In vitro antioxidant and wound healing efficacy |
21 |
|
Eclipta prostrata (Asteraceae) |
Wedelolactone, ecliptine, flavonoids |
Anti-inflammatory, hepatoprotective, antioxidant |
Shown to enhance epithelial regeneration |
22 |
|
Houttuynia cordata (Saururaceae) |
Quercitrin, decanoyl acetaldehyde |
Antibacterial, anti-inflammatory, antioxidant |
Used in polyherbal formulations; reduces rectal inflammation |
6 |
|
Leucas aspera (Lamiaceae) |
Steroids, alkaloids, β-sitosterol, flavonoids |
Anti-inflammatory, analgesic, antioxidant |
Demonstrated significant anti-inflammatory activity in animal models |
6,23 |
|
Aloe vera (Asphodelaceae) |
Polysaccharides (acemannan), aloin, anthraquinones |
Wound healing, anti-inflammatory, laxative |
Clinical efficacy in anorectal wound repair and pain reduction |
24 |
|
Curcuma longa (Zingiberaceae) |
Curcumin, demethoxycurcumin, turmerones |
Anti-inflammatory, antioxidant, wound healing |
Downregulates COX-2 and TNF-α; enhances tissue repair |
28 |
Phytochemical Profile and Therapeutic Correlation
Tannins and Polyphenols
The main class of bioactives found in plants associated to hemorrhoids are tannins and polyphenolic chemicals. They have hemostatic and astringent properties that encourage the constriction of inflammatory tissues and lessen bleeding. Hydrolyzable and condensed tannins found in Terminalia chebula, Hamamelis virginiana, and Psidium guajava precipitate proteins to create a barrier that protects mucosal surfaces [21,29]. Furthermore, polyphenols have the ability to scavenge free radicals, preventing oxidative stress in vascular tissues.
Flavonoids: One of the phytochemical groups with the highest pharmacological activity in hemorrhoidal therapy is flavonoids. Venotonic, anti-inflammatory, and antioxidant effects are possessed by compounds including rutin, quercetin, diosmin, and hesperidin [25,27]. They lower vascular permeability, stabilize capillary walls, and prevent the release of prostaglandins and histamine.
Saponins and Terpenoids
Saponins have venotonic and surface-active characteristics, such as aescin in Aesculus hippocastanum. They lessen edema, enhance lymphatic drainage, and prevent extracellular matrix breakdown by enzymes [25]. Terpenoids such as turmerones (from Curcuma longa) and β-sitosterol (from Leucas aspera) have anti-inflammatory and collagen-stimulating properties that facilitate mucosal healing[ 23,28].
Alkaloids and Sterols
Leucas aspera and Houttuynia cordata contain alkaloids that have analgesic and antibacterial properties [23]. By preventing prostaglandin formation, β-sitosterol, a plant sterol structurally identical to cholesterol, lowers inflammation. Additionally, these components support tissue healing and epithelial regeneration.
Anthraquinones and Glycosides
Anthraquinone derivatives (aloin, rhein) found in plants like Aloe vera and Cassia fistula function as moderate laxatives, promoting bowel movements and lessening straining during defecation [24]. Aloe vera glycosides, such as acemannan, have wound-healing and immunomodulatory qualities that hasten the healing of damaged mucosa.
Pharmacological Activities, Mechanisms of Action, and Comparison with Synthetic Drugs:
Numerous mechanisms of action that together target inflammation, oxidative stress, vascular fragility, and mucosal degeneration have been identified by pharmacological studies of medicinal plants used to treat hemorrhoids. Herbal treatments work in concert through a variety of metabolic routes, unlike synthetic single-target medications. These botanicals' bioactive components—flavonoids, saponins, alkaloids, and polyphenols—have fewer adverse effects and a wide range of therapeutic possibilities. The pharmacological properties of well-known anti-hemorrhoidal plants, their molecular mechanisms of action, and a comparison with traditional allopathic treatments are described in this section.
Pharmacological Activities of Medicinal Plants
Anti-Inflammatory Activity
The onset and development of hemorrhoids are mostly dependent on inflammation. Herbal medicines reduce inflammation by modifying important inflammatory mediators and signaling pathways, including NF-κB, COX-2, LOX, and TNF-α. Curcuma longa (curcumin) reduces prostaglandin synthesis and nitric oxide generation by downregulating COX-2 and inducible nitric oxide synthase (iNOS) [31]. Triterpenoids and flavonoids found in Leucas aspera and Houttuynia cordata limit the production of prostaglandin E₂ (PGE₂), hence preventing the inflammatory cascade [6].
Antioxidant and Cytoprotective Effects
In hemorrhoids, oxidative stress plays a role in the deterioration of vascular and connective tissue. Terminalia chebula, Eclipta prostrata, and Phanera aureifolia all include flavonoid and phenolic chemicals that are powerful antioxidants that improve endogenous defense mechanisms and scavenge free radicals.
Analgesic and Anti-Pruritic Actions
Pain and itching are major symptomatic concerns in hemorrhoids. The topical application of herbal ointments containing Lidocaine analogs or tannin-rich extracts reduces sensory irritation.
Hamamelis virginiana (witch hazel) exerts analgesic effects through peripheral nerve inhibition [26]. Leucas aspera methanolic extract demonstrated significant analgesic activity in hot plate and tail-flick models, indicating modulation of the opioid receptor system [23].The combination of Aloe vera gel and Curcuma longa oil has been shown to reduce itching and pain synergistically due to anti-inflammatory and cooling effects [24,31]. These botanicals are promising substitutes for artificial anesthetics due to their multiple analgesic processes.
Wound Healing and Tissue Regeneration
In hemorrhoidal therapy, mucosal and vascular repair is essential. Angiogenesis, collagen synthesis, and fibroblast proliferation are all aided by herbal extracts. Aloe vera polysaccharides speed up epithelial closure in wound locations by promoting fibroblast proliferation and collagen deposition [24]. Curcuma longa (curcumin) aids in tissue regeneration by stimulating collagen production mediated by transforming growth factor-beta (TGF-β) [32].
Venotonic and Hemostatic Effects
Hamamelis virginiana tannins constrict tiny blood capillaries, offering quick relief from bleeding and edema [26]. Citrus flavonoids (diosmin and hesperidin) strengthen capillary walls and encourage lymphatic drainage, hence lowering swelling and bleeding [19,20].These venotonic herbs have greatly improved patient outcomes when incorporated into formulations like Daflon, herbal suppositories, and topical creams..
Molecular Mechanisms of Herbal Bioactives
Herbal bioactives exert their pharmacological effects via multiple biochemical and molecular pathways. The following mechanisms are particularly relevant in hemorrhoid management.
Inhibition of NF-κB and MAPK Pathways
The NF-κB signaling pathway plays a critical role in inflammation by regulating cytokine production. Curcumin from Curcuma longa and quercetin from Sophora japonica inhibit IKKβ phosphorylation, preventing NF-κB nuclear translocation and reducing transcription of pro-inflammatory genes such as TNF-α, IL-1β, and IL-6 [31,32].
Modulation of Oxidative Stress Enzymes
By increasing the expression of Nrf2, a transcription factor that encourages the production of antioxidant enzymes (SOD, catalase, and GPx), polyphenolic substances enhance antioxidant defense mechanisms. Studies on Phanera aureifolia revealed significant upregulation of Nrf2 and downregulation of oxidative markers such as MDA (malondialdehyde) [27].
Collagen Remodeling and Tissue Integrity
Curcumin and Aloe vera bioactives regulate TGF-β and VEGF signaling, facilitating extracellular matrix remodeling and angiogenesis [24,32]. Enhanced collagen deposition accelerates repair of damaged rectal mucosa, thereby improving vascular resilience.
Five Mechanisms of Antimicrobial and Cytotoxic Action
Through bacterial enzyme system suppression and cell membrane rupture, herbal extracts have antimicrobial action. For instance, under scanning electron microscopy, Phanera aureifolia extracts caused Staphylococcus aureus cells to visibly distort and inflate, suggesting direct cytotoxic impact on bacterial membranes [7]. By preventing subsequent infections, this antimicrobial characteristic facilitates quicker and cleaner wound healing.
Comparison Between Herbal and Synthetic Drugs
Synthetic drugs like hydrocortisone, lidocaine, benzocaine, and phenylephrine are commonly used for symptomatic hemorrhoidal relief. Even though these medications act fast, prolonged usage often causes mucosal thinning, tolerance development, and local pain. Herbal alternatives, on the other hand, function in a number of ways and are usually safer to use for longer.
Table 2: Comparison of Synthetic and Herbal Medicines for the Treatment of Hemorrhoids
|
Parameter |
Herbal Agents |
Herbal Agents |
|
Mechanism of Action |
Multi-targeted (anti-inflammatory, antioxidant, venotonic, wound healing |
Single-target (vasoconstrictor, corticosteroid, or anesthetic) |
|
Major Examples |
Curcuma longa, Aesculus hippocastanum, Hamamelis virginiana, Aloe vera, Terminalia chebula |
Hydrocortisone, Lidocaine, Phenylephrine, Benzocaine |
|
Pharmacological Effects |
Anti-inflammatory, antioxidant, hemostatic, analgesic, mucosal healing |
Anti-inflammatory, antioxidant, hemostatic, |
|
Side Effects |
Minimal; rare allergic reactions |
Skin thinning, hypersensitivity, rebound inflammation |
|
Onset of Action |
Moderate (requires few days) |
Rapid (few minutes to hours) |
|
Duration of Effect |
Sustained and preventive |
Short-term and symptomatic |
Pharmacodynamic Synergy
In results. For example, topical hydrocortisone combined with flavonoid intake (from Citrus several circumstances, combining synthetic and herbal medications has produced better bioactives) minimizes steroid dosage while shortening the duration of acute symptoms [19,20]. In a similar vein, medicinal ointments containing extracts of aloe vera and hamamelis enhance the anti-inflammatory properties of traditional medications without escalating adverse effects.
Toxicological Considerations
The majority of herbal anti-hemorrhoidal plants are safe within therapeutic levels, according to toxicological assessments. Although Aesculus hippocastanum extract is usually well tolerated, the aescin concentration of raw seeds may irritate the gastrointestinal system in large quantities [25]. Both acute and chronic toxicity models have demonstrated the safety of Curcuma longa and Aloe vera [24,31]. Before being used in a therapeutic setting, polyherbal combinations are pharmacognostically evaluated to rule out toxins and heavy metals [6].
Herbal Formulation Development and Standardization
vesting therapeutic plants. Quality and environmental Standardized formulation development is necessary for the shift from traditional herbal use to evidence-based phytotherapeutics. Many dose forms, including tablets, ointments, suppositories, powders (churna), gutika (polyherbal balls), and nanoformulations, have been created in hemorrhoidal therapy to improve patient compliance, stability, and therapeutic efficacy. Moisture content, pH, total ash, extractive values, and chromatographic fingerprinting (HPLC, TLC, FTIR) are among the pharmacognostic, physicochemical, and phytochemical parameters that are evaluated during standardization. This guarantees that pharmacological results are consistent and repeatable [41].
Polyherbal Gutika Formulations
In Ayurvedic hemorrhoidal therapy, polyherbal formulations are essential. Because of the synergistic combination of Leucas aspera, Houttuynia cordata, and Eclipta prostrata, the Gutika formulation standardized by Borah and Saikia [6] showed exceptional antioxidant and antibacterial properties. The formulation validated the idea of synergistic phytotherapy by displaying superior phenolic (310 mg GAE/g) and flavonoid (142 mg QE/g) contents when compared to individual extracts. Methanol was used as an extraction solvent to optimize the Gutika, resulting in increased yield and stability. Peaks corresponding to O–H (phenolics), C–H (terpenes), and C=C (flavonoids) were identified by analytical analysis using FTIR spectroscopy, showing the existence of important bioactives with anti-inflammatory and antibacterial properties [41].
Herbal Ointments and Suppositories
Because topical formulations directly touch the afflicted tissue, they are essential to the management of hemorrhoids. When applied to the anal area, aloe vera-based gels have calming, anti-inflammatory, and wound-healing qualities [24]. Hamamelis virginiana extracts had quick hemostatic and astringent effects when added to ointments [26]. Plant mucilage, beeswax, and Curcuma longa oil provide a barrier that improves epithelial healing [31].Aloe vera, Curcuma longa, and Aesculus hippocastanum extracts are used in contemporary herbal suppositories to promote mucosal absorption and extend contact with hemorrhoidal veins, which increases venotonic and anti-inflammatory activity [42].
Novel Delivery Systems: Nanoformulations and Phytosomes
The goal of recent pharmaceutical developments is to use nanotechnology to increase the bioavailability of herbal actives. It has been demonstrated that curcumin-loaded nanoparticles increase systemic absorption and intestinal permeability by two to three times [42].
Aloe vera-based nanoemulsions speed up the healing of wounds by efficiently delivering polysaccharides across mucosal membranes. Phytosomes, lipid-compatible polyphenol molecular complexes, enhance the stability and bioefficacy of flavonoids like hesperidin and diosmin [44].
Flavonoid-Based Treatments
Hemorrhoidal symptoms have significantly improved in clinical trials using micronized purified flavonoid fraction (MPFF), a combination of diosmin and hesperidin produced from Citrus species. After 14 days of MPFF therapy, 67% less bleeding and pain relief were found in a multicenter research by Cospite [20]. Additionally, patients showed improvements in venous tone and microcirculation, as seen by decreased anal discharge and edema. The outcomes validate the venotonic and anti-inflammatory properties of flavonoids in the treatment of hemorrhoids.
Polyherbal Ayurvedic Formulations
Triphala Guggulu, a mixture of Terminalia chebula, T. bellirica, Emblica officinalis, and Commiphora mukul, was found to be just as successful in treating Grade I–II hemorrhoids as hydrocortisone suppositories in comparative research [33]. Without producing rebound symptoms, the herbal formulation dramatically decreased pain, pruritus, and bleeding. Similarly, Pilex (Himalaya Herbal Healthcare) and Arshoghna Vati shown significant therapeutic efficacy, especially in cases of chronic hemorrhoids. Their blend of laxative, hemostatic, and astringent herbs offers a comprehensive strategy that addresses both symptoms and underlying causes [45].
Topical Herbal Applications
In a double-blind randomized study, topical use of Hamamelis virginiana ointment showed comparable symptom management to hydrocortisone cream [46]. When used after a hemorrhoidectomy, aloe vera and curcuma longa gels similarly showed better healing scores and lower recurrence rates, highlighting their importance in postoperative care [47].
Potential Herb–Drug Interactions
Interactions with concurrent usage of allopathic drugs are rare but can happen. The effects of anticoagulants like warfarin may be amplified by Aesculus hippocastanum extract, necessitating careful observation [35]. When combined with nonsteroidal anti-inflammatory medicines (NSAIDs), curcuma longa may increase a person's propensity to bleed [31]. With careful dosage and expert advice, these hazards can be reduced.
Quality Control and Standardization
In unregulated herbal products, toxic pollutants including heavy metals, microbiological load, or adulterants continue to be a concern. Testing for pollutants, pesticide residues, and microbiological purity is required in order to comply with WHO and AYUSH guidelines [49]. HPLC and ICP-MS are examples of analytical instruments that guarantee phytochemical consistency and product safety.
Future Prospect: Promising with research focusing on developing standardized evidence based therapies and integrating traditional knowledge with mordern technology to creat effective treatment with fewer side effect than conventional option.
CONCLUSION:
For the treatment of hemorrhoids, botanical treatments offer a holistic, safe, and effective alternative. The complex pathophysiology of hemorrhoids, which includes vascular inflammation, oxidative stress, sand mucosal injury, is addressed by the pharmacological synergy of bioactive phytochemicals including flavonoids, tannins, saponins, terpenoids, and polyphenols. Modern pharmacological validation has demonstrated the persistent efficacy of traditional formulations such as Triphala Guggulu, Pilex, and polyherbal Gutika. Herbal remedies have the potential to supplement or even replace synthetic therapies because to developments in standardization, nanotechnology, and clinical research. Future studies that incorporate contemporary analytical techniques, regulatory standardization, and clinical validation will hasten the conversion of these traditional treatments into widely recognized evidence-based phytopharmaceuticals for the treatment of haemorrhoids.
REFERENCES





Maithili Kalbande, Rupeshri Netkar, Vaishnavi Gole, Roshani Kale, Deshna Khartad, Pranali Bhande, Botanical Treatment for Piles: An Extensive Analysis of Plants Used to Treat Hemorrhoids, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 8284-8296. https://doi.org/10.5281/zenodo.20472530
 10.5281/zenodo.20472530
10.5281/zenodo.20472530