
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutical Quality Assurance, Aditya Bangalore Institute of Pharmacy Education & Research.
Corrective and Preventive Actions (CAPA) are central to Quality Management Systems (QMS) in regulated sectors such as pharmaceuticals, medical devices, and biotechnology, where patient safety and compliance are essential. When effectively implemented, CAPA extends beyond correcting nonconformities to drive risk mitigation and continuous improvement. This review highlights best practices, including structured procedures, cross-functional collaboration, risk-based prioritization, robust root cause analysis, and closed-loop effectiveness verification. The adoption of digital quality management systems (eQMS), along with proactive training and feedback loops, improves transparency and operational efficiency. Case studies show that weak CAPA execution leads to recurring deviations and costly recalls, while risk-informed approaches reduce defects and enhance compliance. Aligning CAPA with risk-based thinking (RBT) enables optimal resource allocation, regulatory readiness, and a stronger culture of quality, making CAPA both a compliance tool and a driver of sustained improvement. The findings underscore CAPA’s dual role as both a regulatory requirement and a strategic driver of sustainable quality improvement
Corrective and Preventive Actions (CAPA) are a structured methodology within quality management systems aimed at detecting, analysing, and addressing the root causes of both existing and potential non-conformities in
processes, products, or systems. Corrective actions are implemented to eliminate the causes of identified non-conformities and prevent their recurrence, whereas preventive actions are designed to recognize and mitigate the causes of possible non-conformities before they occur.1 In industries such as pharmaceuticals, medical devices, and food manufacturing, where regulatory oversight is stringent, product quality and patient safety remain paramount. To uphold these priorities, organizations rely on Quality Management Systems (QMS) that ensure consistent adherence to international standards and regulatory requirements. Among the key components of a QMS, the Corrective and Preventive Action (CAPA) process plays a pivotal role. More than just a compliance requirement, CAPA serves as a strategic mechanism for uncovering systemic issues, preventing the recurrence of deviations, and fostering a culture of continuous improvement. Its significance is reinforced by its inclusion in major global quality frameworks, such as FDA 21 CFR Part 820 for medical devices, ICH Q10 for pharmaceutical quality systems, and ISO 9001 for general quality management.1, 2An effective CAPA program typically follows a structured approach—identifying the problem, performing in-depth root cause analysis, formulating corrective and preventive measures, implementing them, and verifying their effectiveness.3 However, successful CAPA implementation depends on more than just following procedures. Regulatory findings and industry reports consistently reveal shortcomings such as weak root cause investigations and poor documentation that can lead to recurring nonconformities, regulatory non-compliance, and financial setbacks.4 This review examines CAPA’s dual role in risk mitigation and quality enhancement, exploring regulatory expectations, proven methodologies, technological innovations, and practical case studies to guide quality professionals in optimizing CAPA systems for compliance, efficiency, and long-term improvement.
OVERVIEW OF CAPA:
Corrective and Preventive Actions (CAPA) are systematic and structured processes within a Quality Management System (QMS) that aim to identify, analyse, and resolve the root causes of existing or potential non-conformities in products, processes, or systems. Corrective actions target the elimination of causes behind identified non-conformities or undesirable events to prevent their recurrence, whereas preventive actions address the causes of potential non-conformities or issues to avert their occurrence.5
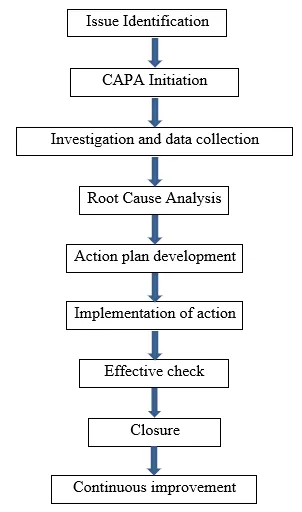
A ROBUST CAPA PROCESS TYPICALLY INVOLVES THE FOLLOWING SEQUENTIAL STAGES:
Issue Identification – Detection of non-conformities, deviations, or potential risks via audits, complaints, monitoring, or inspections.
Evaluation & Risk Assessment – Assessing severity, frequency, and impact using tools like FMEA or risk matrices.
Root Cause Analysis (RCA) – Systematic identification of underlying causes through methods such as 5 why’s, Fishbone, Fault Tree Analysis.
Action Plan Development – Designing corrective measures to resolve current issues, and preventive strategies to detour future occurrences.
Implementation – Executing the action plan within set timelines and assigned responsibilities.
Verification of Effectiveness – Ensuring actions have successfully addressed the root cause and prevented recurrence.
Documentation & Closure – Recording all CAPA steps and outcomes to fulfill regulatory compliance and enable continuous improvement.6
An effective CAPA process is data-driven, cross-functional, and integrated into an organization’s risk management strategy. Its success depends on timely execution, clear accountability, and continuous monitoring to ensure sustained improvement.
CAPA WORKFLOW IN QMS:
Regulatory and Guideline Framework:
FDA
The U.S. Food and Drug Administration (FDA) mandates that regulated industries, including medical devices and pharmaceuticals, establish and maintain robust Corrective and Preventive Actions (CAPA) systems as outlined in 21 CFR Part 820,7 100 for medical devices and supported by current Good Manufacturing Practice (camp) requirements in 21 CFR Parts 210–211 for pharmaceuticals.8 These regulations require documented procedures for identifying, investigating, and addressing actual or potential quality issues through data analysis, root cause determination, corrective and preventive action planning, verification or validation of effectiveness, and comprehensive documentation for management review. FDA inspection guidelines further emphasize trend analysis, proactive prevention, and thorough record keeping, ensuring CAPA serves not only as a compliance mechanism but also as a strategic tool for continual improvement and risk mitigation in quality management systems.9
ICH Q10:
ICH Q10 establishes Corrective and Preventive Actions (CAPA) as a core element of the Pharmaceutical Quality System (PQS), integrating them across the entire product lifecycle—from development and technology transfer to commercial manufacturing and discontinuation to proactively identify and address actual or potential issues through trend analysis, risk management, and knowledge management. By linking CAPA activities to Quality Risk Management (QRM) and continuous process performance monitoring, ICH Q10 ensures both reactive corrective measures and proactive preventive actions are prioritized based on risk, documented, and reviewed through management oversight, thereby fostering continual improvement, maintaining a state of control, and enhancing product quality and compliance within regulated pharmaceutical operations.10
ISO STANDARDS:
ISO 9001:2015 embeds CAPA principles within its Quality Management System framework, with Clause 10.2 mandating organizations to react to nonconformities by controlling and correcting the issue, investigating and determining root causes, implementing corrective actions to prevent recurrence, reviewing their effectiveness, updating risk assessments, and maintaining documented records. Preventive thinking is addressed through Clause 6.1, which emphasizes proactive, risk-based actions to address risks and opportunities, while Clause 9.1 requires ongoing monitoring, measurement, analysis, and evaluation to detect trends and trigger CAPA.11 ISO 13485:2016, specific to medical devices, adopts a more prescriptive, risk-oriented approach: Clause 8.5.2 requires prompt elimination of root causes of nonconformities, documentation of review processes, implementation and monitoring of corrective actions, verification of their effectiveness, and record retention; Clause 8.5.3 mandates identification of potential nonconformities, evaluation of the need for preventive action, planning and documentation, safe implementation ensuring regulatory compliance, verification of effectiveness, and retention of records These frameworks collectively ensure that CAPA serves not only as a compliance tool but also as a driver of continuous improvement in regulated industries.12,13
WHO GMP GUIDELINES:
The World Health Organization’s GMP guidelines, particularly Annex 2 of the WHO Technical Report Series 981 on Quality Risk Management, recommend that manufacturers apply CAPA in response to deviations, complaints, and audit findings, integrate CAPA within inspection planning and routine follow-up, assess complaints and findings through a risk-based lens, and track corrective and preventive measures systematically until verified closure to uphold consistent product quality and regulatory compliance.14
TOOLS AND TECHNIQUES FOR EFFECTIVE CAPA:
ROOT CAUSE ANALYSIS (RCA) TOOLS:
5 WHYS
The 5 why's is a straightforward root cause analysis method that works by repeatedly asking “Why?” usually around five times to trace a problem from its visible symptom to its underlying actionable cause. It is most effective for simple or moderately complex issues that follow a single causal chain and is often applied as an initial diagnostic tool before more advanced analyses. The process starts with a well-defined, measurable problem statement and continues through iterative questioning until a cause that is within control and supported by evidence is identified, leading to corrective actions with clear accountability. Its advantages include being quick, easy to apply, and useful for fostering causal thinking; however, it can be overly simplistic if it stops at assumptions instead of evidence, may miss multiple contributing factors due to facilitator bias, and is less suitable for complex sociotechnical problems without the support of additional methods.15
FISHBONE (ISHIKAWA) DIAGRAM
The Fishbone Diagram, also called the Ashikaga or Cause-and-Effect Diagram, is a visual root cause analysis tool that categorizes potential factors contributing to a problem into groups such as People, Methods, Machines, Materials, Measurement, and Environment. It is particularly valuable for complex issues with multiple contributing factors, as it enables teams to brainstorm collectively and organize ideas in a structured manner. The process starts by placing the problem at the “head” of the fish, then mapping major categories along the “bones” and breaking them down into sub-causes, which are further examined and validated with data before prioritization. Its key advantages lie in fostering collaboration, promoting comprehensive exploration of possible causes, and offering a clear visual framework, though it can become overly detailed, remain descriptive rather than analytical, and lose focus without careful facilitation.16
FAULT TREE ANALYSIS (FTA)
Fault Tree Analysis (FTA) is a deductive, top-down technique that uses logic gates (AND/OR) to trace the combinations of basic events that can lead to an undesired top event, such as a failure or hazard. It is particularly suited to safety-critical industries like aerospace, nuclear, and healthcare where understanding failure pathways and quantifying risks are essential. The process starts with a clearly defined top event, followed by mapping contributory events into a hierarchical tree and calculating probabilities to determine minimal cut sets and dominant contributors to failure. Its major strengths are its structured logical reasoning and ability to quantify risks, but it requires significant expertise, data, and effort, and may overlook partial or interacting failures if not combined with other methods.17
FAILURE MODE AND EFFECTS ANALYSIS (FMEA)
FMEA is an inductive, bottom-up method used to identify potential failure modes in components, processes, or systems, assess their effects and causes, and prioritize them for corrective or preventive action. It is widely applied in industries such as automotive, aerospace, and healthcare, especially during design and process development, to proactively reduce risk. The workflow involves listing failure modes, rating each by Severity, Occurrence, and Detection, calculating a Risk Priority Number (RPN) or Action Priority, and targeting high-risk items with mitigation plans. FMEA’s strengths include its systematic, preventive approach and ability to prioritize risks, while its drawbacks include being resource-intensive and sometimes inconsistent due to subjective scoring.18
RISK ASSESSMENT INTEGRATION:
Risk assessment tools, such as hazard analysis and risk matrices, are often applied before finalizing CAPA actions to ensure resources are focused on high-impact issues. Integration with ICH Q9 Quality Risk Management principles ensures that CAPA addresses both actual and potential quality threats.
Hazard Analysis forms the foundation of risk assessment by identifying potential system hazards, analysing how adverse events may occur, and determining their severity and likelihood. This structured evaluation, whether qualitative or quantitative, ensures risks are systematically assessed. When conducted early during CAPA initiation, hazard analysis allows investigations to be framed around potential failure scenarios and their consequences, ensuring corrective actions are guided by risks rather than symptoms.19
Risk matrices are another widely used tool that visually plots the likelihood of occurrence against the severity of consequences, providing quick prioritization of risks. They are especially popular in pharmaceuticals and manufacturing due to their simplicity and intuitive nature. However, risk matrices have notable limitations such as poor granularity, range compression, misleading comparisons between risks of differing scales, and subjectivity in categorization. To avoid misallocation of efforts, best practice in CAPA is to apply risk matrices as a preliminary triage tool and confirm decisions with more quantitative or structured assessments.20
More advanced layered risk assessment techniques include HAZOP, LOPA, and E-HAZOP. A HAZOP (Hazard and Operability Study) is a structured, qualitative method for exploring deviations from intended operations, commonly applied in process safety and early hazard identification. LOPA (Layers of Protection Analysis) bridges qualitative and quantitative assessments by evaluating how multiple independent safeguards prevent hazards from escalating, thereby providing a more robust risk profile. E-HAZOP further enhances this process by integrating decision-matrix risk assessment and the Analytical Hierarchy Process (AHP) to systematically identify critical control points and prioritize risks. Within CAPA, these tools enable escalation of actions when quantified risks or safeguard failures are detected, triggering detailed root cause analysis or preventive redesign.21
Integration of these approaches supports a shift from purely reactive CAPA, which addresses only failures that have already occurred, to proactive CAPA that anticipates and prevents latent risks. A structured workflow involves performing hazard analysis and applying risk matrices or LOPA at the initiation stage, prioritizing CAPA actions based on quantified risk and control measures, escalating high-risk cases to full root cause analysis with design or procedural improvements, and updating organizational risk registers to strengthen future controls.22
Finally, regulatory and quality frameworks, such as ICH Q9 in the pharmaceutical sector, emphasize that CAPA must address both actual and potential threats to product quality and patient safety. Embedding risk assessment tools within CAPA not only ensures compliance with Quality Risk Management (QRM) principles but also enhances efficiency by focusing resources on the most significant risks. This integration further supports continuous improvement and audit readiness, thereby strengthening both organizational resilience and product quality.23
DOCUMENTATION AND TRACKING SYSTEMS
Electronic Quality Management Systems (eQMS) are integral to modern quality assurance, providing a centralized and secure platform for managing documents, corrective and preventive actions (CAPA), and compliance processes. A key advantage is centralized document control with version management, ensuring that staffs access only the latest SOPs, policies, and training materials while maintaining a complete audit history for transparency. eQMS further streamline the CAPA lifecycle by automating workflows such as task assignment, progress tracking, reminders, and closure verification, thereby reducing errors and delays.24 Robust audit trails with time-stamped entries and electronic signatures enable compliance with regulatory requirements, including FDA 21 CFR Part 11, while ensuring data integrity and accountability during inspections. These systems also enhance audit readiness by allowing rapid retrieval of records and verification of compliance, supported by features such as role-based access controls, change management, and acknowledgment tracking. Cloud-based eQMS platforms extend these benefits by enabling collaboration across distributed teams, offering scalability, and supporting real-time process monitoring. Additionally, built-in analytics facilitate trend analysis and continuous improvement, allowing organizations to proactively identify risks and strengthen quality systems.25 Collectively, these capabilities improve efficiency, reinforce compliance, and enhance organizational resilience by integrating document control, CAPA management, audit trails, and regulatory requirements.
CAPA IN RISK MITIGATION
Corrective and Preventive Action (CAPA) represents a structured mechanism for risk mitigation and is widely recognized as a cornerstone of quality assurance, particularly within the pharmaceutical sector. Operating as a dual-loop system, CAPA is both reactive—addressing deviations once they occur and proactive preventing their recurrence through systemic improvements. Its principles are strongly aligned with international standards such as ISO 9001 and ICH Q10, which emphasize not only error correction but also the integration of preventive strategies into organizational processes. The CAPA framework typically unfolds across three stages: correction, corrective action, and preventive action, each supported by rigorous root cause analysis and problem-solving methodologies ensuring issues are resolved at their source. Beyond short-term corrective measures, CAPA drives the shift from reactive to proactive quality management by applying structured methods that include cross-functional collaboration, precise problem definition, rapid containment, root cause identification through approaches like the 5 Whys or Fishbone diagrams, validation of permanent solutions, and institutionalization of improvements through updated procedures or mistake-proofing designs. In the context of risk-based standards,[1] ISO 9001:2015 integrates preventive thinking across its clauses, notably Clause 6.1, which calls for actions to address risks and opportunities, and Clause 10.2, which requires systematic investigation of nonconformities to avoid recurrence. Although the term “preventive action” has been removed, the standard embeds proactive risk management throughout the QMS framework.26
In parallel, ISO 13485:2016 mandates documented CAPA procedures that include identifying nonconformities, investigating their causes, implementing corrective and preventive actions, and assessing their effectiveness, while FDA’s 21 CFR Part 820.100 establishes nearly identical requirements, highlighting CAPA’s essential role in medical device compliance. For pharmaceuticals, ICH Q10 requires CAPA systems to address deviations, trends, audits, and recalls, ensuring that investigations are rooted in cause analysis and that documentation is proportionate to the level of risk involved. Research further demonstrates that mature quality management systems based on ISO 9001 enhance risk prevention by embedding CAPA processes into systematic planning, process control, and deviation analysis. Techniques such as Failure Mode and Effects Analysis (FMEA) are often employed to proactively identify, assess, and eliminate risks during both design and operational stages.27
Finally, management reviews are integral to sustaining CAPA effectiveness in risk mitigation. ISO 9001:2015 stresses the importance of evaluating the results of risk-mitigation measures during these reviews, where organizations analyze data from risk assessments, propose targeted improvements, discuss findings in structured forums, and allocate resources for follow-up actions. In this way, CAPA extends beyond immediate problem-solving to form a continuous improvement cycle that strengthens organizational resilience, ensures regulatory compliance, and drives long-term quality enhancement.
PREVENTING RECURRENCE OF NONCONFORMITIES
By focusing on eliminating root causes rather than addressing superficial symptoms, CAPA plays a crucial role in reducing the recurrence of deviations, audit findings, and customer complaints. This structured approach not only strengthens process reliability but also delivers measurable cost benefits by minimizing rework, product recalls, and regulatory penalties. Comparative studies of ISO 13485:2016 and FDA 21 CFR Part 820 highlight that CAPA frameworks proactively target root causes, reduce defect recurrence, ensure regulatory compliance, and contribute to broader business gains such as lowering operational costs and recall risks.28 Similarly, research in pharmaceutical quality management emphasizes CAPA as a vital tool that follows a systematic, stepwise process to investigate, document, and resolve issues, thereby preventing repetition and fostering continuous quality improvement in line with regulatory requirements.29 Further reviews in both pharmaceutical and medical device industries confirm that CAPA is specifically designed to uncover system weaknesses, implement corrective and preventive measures, and prevent future nonconformities.30 In this way, CAPA extends beyond immediate corrections by institutionalizing long-term improvements such as revising SOPs, strengthening employee training, and introducing error-proofing mechanisms-ultimately preventing recurrence, safeguarding revenue, and reinforcing organizational compliance.31
LINK BETWEEN CAPA AND RISK-BASED THINKING IN QMS
In ISO 9001:2015, the traditional “preventive action” clause was replaced by risk-based thinking (RBT), requiring organizations to consider risks and opportunities when planning and executing CAPA so that actions are proportional to the likelihood and severity of potential failures. Systematic literature on ISO 9001:2015 demonstrates that effective CAPA depends on embedding risk-based thinking into routine practices, ensuring that identification, prioritization, implementation, and verification of actions are driven by explicit risk. Peer-reviewed reviews in pharmaceuticals emphasize that CAPA should follow a closed-loop, risk-led cycle, beginning with signal detection and trending, followed by root-cause analysis, risk-prioritized action selection, and effectiveness verification, which together prevent recurrence and reduce residual risk.32
In the pharmaceutical sector, ICH Q10 explicitly requires that the level of effort, formality, and documentation in CAPA investigations should be commensurate with the level of risk, there by aligning CAPA depth with the probability and impact of failures as defined in ICH Q9 Quality Risk Management .Under ICH Q10, CAPA is positioned as a core element of the Pharmaceutical Quality System (PQS), deployed across the entire product lifecycle, with risk-based prioritization guiding which deviations, complaints, or trends warrant deeper investigation and stronger controls. ICH Q9 provides the methodological foundation for CAPA by defining risk assessment tools such as FMEA, fault-tree analysis, and hazard analysis—that allow structured evaluation of probability, severity, and detectability, enabling transparent risk ranking prior to selecting corrective or preventive measures. Applied studies of FMEA show how Risk Priority Numbers (RPNs) are used to prioritize CAPA tasks, implement targeted controls, and then reassess residual risks to confirm that the interventions lowered the overall risk profile, thereby operationalizing the CAPA– risk-based thinking link.33
In the medical device industry, regulators and standards bodies advocate a risk-based CAPA approach, where high-risk issues receive more extensive investigation and documentation while low-risk problems are managed with streamlined responses, thereby improving both efficiency and compliance.34
CASE STUDY: CAPA IN PHARMACEUTICAL RISK MITIGATION
A case study reported in The TQM Journal by Power and McDermott (2022) examined CAPA practices in Irish MedTech and pharmaceutical firms, where one company experienced repeated equipment-related deviations in sterile manufacturing, such as HVAC filter failures and autoclave malfunctions. Initially, the organization relied on short-term fixes; however, these measures proved insufficient, and the risks persisted, ultimately resulting in regulatory audit observations. To address this, the company adopted a structured CAPA process using Failure Modes and Effects Analysis (FMEA), which enabled them to identify root causes including inadequate preventive maintenance and gaps in staff training. Corrective actions were implemented by redesigning maintenance schedules, replacing critical components before failure, and retraining operators, while preventive measures involved integrating a risk-prioritization tool into the quality management system so that equipment-related deviations received higher priority. Effectiveness verification was conducted by trending deviation data over a 12-month period, which demonstrated a 70% reduction in recurrence along with improved regulatory audit outcomes. This case highlights that when CAPA is risk-informed and systematically verified, it effectively mitigates risks, strengthens organizational processes, and prevents costly recalls and reputational damage.
CAPA IN QUALITY IMPROVEMENT
Corrective and Preventive Actions (CAPA) serve as a cornerstone for quality improvement within regulated industries by ensuring that both existing and potential issues are resolved and prevented systematically. Far beyond being a mere compliance checkbox, an effective CAPA system actively drives continuous quality enhancements by identifying root causes, streamlining workflows, and embedding risk-awareness into organizational culture.
1. Structural Elements Enabling Quality Improvement
A robust CAPA process begins with standardized workflows and templates for documentation and execution, ensuring continuity even across complex quality events. This consistency reduces ambiguity and promotes clarity during investigations.
Embedding risk-based prioritization within CAPA leads to focusing efforts on high-impact issues, optimizing use of organizational resources for maximum quality benefit.
Using Key Performance Indicators (KPIs) such as CAPA resolution time, recurrence rates of deviations, and reductions in audit findings enables tracking system performance and demonstrating tangible quality improvements over time.36
2. Process Levers That Drive Impact
Digitalization and automation (e.g., via eQMS platforms) centralize CAPA tracking and documentation, automate workflow approvals and reminders, and allow analytics-driven insights that help detect emerging trends resulting in improved efficiency and consistency.
Cross-functional engagement spanning QA, production, regulatory, and engineering teams ensures that CAPA plans are practical, comprehensive, and successfully integrated into daily operations.
Training and culture are vital. Empowering staff through CAPA education and feedback loops nurtures a proactive quality mindset, enabling personnel to detect and act on improvement opportunities early and effectively.37
3. Real-World Impact: Case Example
A pharmaceutical manufacturer strengthened quality performance by implementing a structured CAPA system aligned with Continuous Improvement (CI) principles.
After redesigning CAPA workflows and integrating risk-based approaches, the facility achieved a 35% reduction in deviations, a 40% drop in audit findings, and a 25% faster CAPA resolution time.
This outcome underscores CAPA’s capacity to drive measurable quality gains when embedded within QMS and supported by leadership and technology.38
4. Sustaining Improvement Over Time
CAPA must be positioned as a continuous improvement tool, not a one-off fix. Regular review of outcomes using Plan–Do–Check–Act (PDCA) cycles helps refine processes, preventing stagnation and adapting to evolving quality challenges.
Leadership oversight is essential. When senior management engages actively reviewing CAPA data, allocating resources, and enforcing completion improvements become sustainable and aligned with strategic goals. Without leadership buy-in, even well-designed systems can erode.39
Effective metrics must extend beyond implementation to measure impact such as recurrence data, effectiveness verification outcomes, and operational efficiencies. These insights enable continuous feedback and adjustment.40
IMPLEMENTING BEST PRACTICES FOR EFFECTIVE CAPA:
Implementing CAPA effectively requires a structured approach that aligns with both regulatory expectations and organizational objectives, beginning with well-defined procedures that clearly delineate objectives, scope, process flow, roles, responsibilities, and terms this foundational clarity is critical, as inadequate CAPA procedures are among the most common causes of regulatory citations such as FDA Form 483s and warning letters Equally important is the establishment of cross-functional teams, which bring together diverse perspectives from quality assurance, manufacturing, regulatory affairs, and other departments to ensure that CAPA plans are both effective and practically implementable.
Implementing a proactive CAPA methodology is also essential: rather than only addressing detected problems, organizations should act preventively when trends, control limits, or emerging data indicate potential failure this shift from reactive to preemptive action enhances risk mitigation.40
Training and education are indispensable, requiring comprehensive instruction so that all personnel understand how to identify issues, participate in root cause analysis, and contribute to CAPA execution—this helps foster a culture of quality and compliance across the organization.41
Adopting a risk-based approach ensures that CAPAs are prioritized based on their impact on patient safety, product quality, and compliance tools such as FMEA, HACCP, and risk-ranking matrices support informed decision-making and efficient resource allocation
Equally, automation and digital solutions such as electronic QMS (eQMS), CAPA software, and workflow tools can streamline operations by routing tasks, sending reminders, generating analytics, and reducing manual burden, thus improving timeliness and visibility of CAPA activities.41
CAPA must operate within a closed-loop system, where effectiveness is verified through quantitative and qualitative measures and actions are only closed once proof of resolution and non-recurrence is evident .Finally, continuous review and improvement must be embedded in CAPA systems through regular audits, performance monitoring, and management reviews this ensures that CAPA remains dynamic, effective, and aligned with organizational learning and regulatory evolution.42
Documentation must be inspection-ready and transparent, with structured investigation plans, consistent recording of methodologies used, decision-making events, and action rationale this level of documentation not only supports traceability but also builds trust with regulators. At the core of effective CAPA lies rigorous root cause analysis, which must utilize structured, evidence-based techniques like the “5 Whys” or fishbone diagrams, and be thoroughly documented to avoid superficial fixes that fail to prevent recurrence Once root causes are identified, it’s crucial to convert those insights into action plans that are specific, measurable, assigned, and time-bound these action plans must be documented with clear responsibilities, deadlines, and success criteria to drive accountability and enable tracking.42
CONCLUSION
CAPA remains one of the most powerful tools for ensuring product quality, compliance, and patient safety in regulated industries. Its effectiveness lies in transforming nonconformities into opportunities for systemic risk reduction and continuous improvement. When integrated with risk-based thinking, CAPA ensures that organizational resources are focused on the most critical quality issues, thereby optimizing both compliance and efficiency. Embedding Case evidence confirms that ineffective CAPA often results in recurring deviations and regulatory penalties, whereas risk-informed and well-verified CAPA programs prevent recurrence, reduce variability, and build resilience into organizational processes. Ultimately, CAPA should not be viewed as a corrective mechanism alone, but as a strategic, risk-oriented process that supports long-term quality improvement, regulatory readiness, and the cultivation of a culture of quality across the product lifecycle.
REFERENCES


Bhavana B, Ruthu G K, Capa Effectiveness in Risk Mitigation and Quality Improvement: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2109-2121, https://doi.org/10.5281/zenodo.21294443
 10.5281/zenodo.21294443
10.5281/zenodo.21294443