
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3,4,5 Department of Pharmacy Practice, Bharat School of Pharmacy, Mangalpally, Hyderabad, Telangana, India 501510
6 Department of General Surgery, Durgabhai Deshmukh Hospital and Research Centre (DDHRC), Hyderabad, Telangana, India
Background: Soft tissue infections (STIs) constitute a significant cause of bacterial morbidity in India, accounting for 10–20% of all hospital admissions. Effective antibiotic selection remains critical for favourable clinical outcomes. Objective: To compare the clinical and inflammatory marker-based efficacy of cefoperazone (a third-generation cephalosporin) and clindamycin (a lincosamide antibiotic) in patients with soft tissue infections. Methods: A six-month prospective, open-label, comparative study was conducted in the Department of General Surgery at Durgabhai Deshmukh Hospital and Research Centre (DDHRC), Hyderabad, enrolling 60 patients (26 on cefoperazone; 34 on clindamycin) meeting predefined inclusion criteria. Efficacy was assessed via white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) measured over three consecutive days. Results: Clindamycin demonstrated a statistically superior reduction in WBC (p < 0.001 on Days 2 and 3) and CRP (p < 0.001 on all three days) compared with cefoperazone. ESR showed a non-significant downward trend favouring clindamycin. Clindamycin was also prescribed significantly more often in abscess cases (p = 0.043). Conclusion: Clindamycin exhibits superior anti-inflammatory and antibacterial efficacy over cefoperazone in the management of soft tissue infections, particularly in abscess cases and high-risk comorbid patients.
Soft tissue infections (STIs) are among the most prevalent bacterial infections encountered in clinical practice, representing 10–20% of all hospital admissions in India.[1] They encompass a broad clinical spectrum — from superficial, uncomplicated presentations such as cellulitis and folliculitis to life-threatening necrotizing fasciitis — and are characterized by microbial invasion of the skin, subcutaneous tissue, fascia, and underlying muscle.[2]
The most frequently implicated pathogens are Staphylococcus aureus and Streptococcus pyogenes, with methicillin-resistant S. aureus (MRSA) emerging as a critical therapeutic challenge.[3] Polymicrobial infections, particularly aerobic-anaerobic combinations, are characteristic of necrotizing soft tissue infections (NSTIs), which carry mortality rates ranging from 23% to 46% without prompt surgical and antimicrobial intervention.[4]
The global incidence of skin and soft tissue infections (SSTIs) is estimated at 24.6 per 1,000 person-years, making SSTIs the third most common reason for emergency department attendance. Approximately 70–75% of cases are managed in an outpatient setting, though complex and necrotizing infections necessitate inpatient care with broad-spectrum intravenous antibiotics.[3]
CLASSIFICATION OF SOFT TISSUE INFECTIONS:
CEFOPERAZONE:
Cefoperazone is a third-generation semisynthetic cephalosporin that exerts bactericidal activity by irreversibly binding to penicillin-binding proteins (PBPs), thereby inhibiting bacterial cell wall synthesis. It demonstrates broad-spectrum efficacy against Gram-negative organisms, including Pseudomonas aeruginosa, and is particularly useful in biliary tract infections owing to its predominantly hepatobiliary excretion.[5]
CLINDAMYCIN:
Clindamycin, a lincosamide antibiotic, suppresses bacterial protein synthesis by binding to the 23S rRNA of the 50S ribosomal subunit, thereby preventing peptide chain elongation. Its efficacy against Gram-positive aerobes (S. aureus, Streptococcus spp.) and anaerobes, combined with a distinctive anti-toxin effect and superior tissue penetration, renders it particularly valuable in necrotizing and deep-seated infections.[6,7]
RATIONALE FOR THE STUDY:
Despite the extensive clinical use of both agents, comparative evidence specific to soft tissue infections — particularly using objective inflammatory markers as endpoints — remains limited in the Indian patient population. This prospective study was therefore designed to rigorously evaluate and compare the efficacy of cefoperazone and clindamycin, using WBC count, ESR, and CRP as surrogate markers of therapeutic response.
MATERIALS AND METHODS
AIM:
To compare the clinical and inflammatory marker-based efficacy of cefoperazone and clindamycin in the management of soft tissue infections.
OBJECTIVES:
MATERIALS AND METHODOLOGY:
RESULT AND DISCUSSION:
A total of 60 patients with soft tissue infections were evaluated, comparing cefoperazone and clindamycin using demographic parameters, diagnosis distribution, and the inflammatory markers WBC, ESR, and CRP.
Table 1: Distribution Based on Age and Gender by Treatment Group
|
Parameter |
Cefoperazone (n=26) |
Clindamycin (n=34) |
Total (n=60) |
P value |
|
Mean age ± SD (years) |
53.65 ± 8.04 |
54.44 ± 9.54 |
– |
0.736 |
|
Female n (%) |
14 (53.8%) |
15 (44.1%) |
29 (48.3%) |
0.455 |
|
Male n (%) |
12 (46.2%) |
19 (55.9%) |
31 (51.7%) |
– |
(SD = Standard Deviation; no statistically significant difference in age or gender distribution between groups)
RESULT:
The mean age of patients in the cefoperazone and clindamycin groups was comparable (53.65 ± 8.04 years vs. 54.44 ± 9.54 years; p = 0.736). Gender distribution was similarly balanced between the two groups (48.3% female, 51.7% male; p = 0.455), confirming baseline demographic comparability and supporting the validity of subsequent efficacy comparisons. The most prevalent comorbidities were diabetes mellitus, which was significantly more common in the clindamycin group (41.2% vs. 7.7%; p = 0.029), and hypertension (30.8% in the cefoperazone group vs. 17.6% in the clindamycin group). Immunosuppression was present in 38.5% of the cefoperazone group compared with 20.6% of the clindamycin group.
Table 2: Diagnosis Distribution by Treatment Group
|
Diagnosis |
Cefoperazone n (%) |
Clindamycin n (%) |
Total n (%) |
P value |
|
Abscess |
1 (3.8%) |
10 (29.4%) |
11 (18.3%) |
0.043* |
|
Cellulitis |
13 (50.0%) |
9 (26.5%) |
22 (36.7%) |
– |
|
Erysipelas |
3 (11.5%) |
6 (17.6%) |
9 (15.0%) |
– |
|
Necrotizing Fasciitis |
9 (34.6%) |
9 (26.5%) |
18 (30.0%) |
– |
(*Statistically significant; p < 0.05)
RESULT:
Cellulitis was the most frequent diagnosis overall (36.7%), followed by necrotizing fasciitis (30.0%), abscess (18.3%), and erysipelas (15.0%). A statistically significant difference was observed in abscess cases, with clindamycin prescribed considerably more often (29.4%) than cefoperazone (3.8%; p = 0.043), reflecting clinician preference for clindamycin's superior tissue penetration in deep-seated, purulent infections. No statistically significant inter-group difference was observed in overall presenting-symptom distribution (p = 0.384), indicating comparable baseline clinical severity between the two groups.
Table 3: Distribution Based on Mean WBC Count by Treatment Group
|
Day |
Treatment |
Mean (cells/µL) |
Std. Deviation |
P value |
|
Day 1 |
Cefoperazone |
13,312.38 |
4165.27 |
0.009 |
|
|
Clindamycin |
10,942.88 |
— |
|
|
Day 2 |
Cefoperazone |
14,296.04 |
3522.19 |
<0.001 |
|
|
Clindamycin |
8,086.09 |
— |
|
|
Day 3 |
Cefoperazone |
12,335.65 |
4527.53 |
<0.001 |
|
|
Clindamycin |
6,516.71 |
— |
|
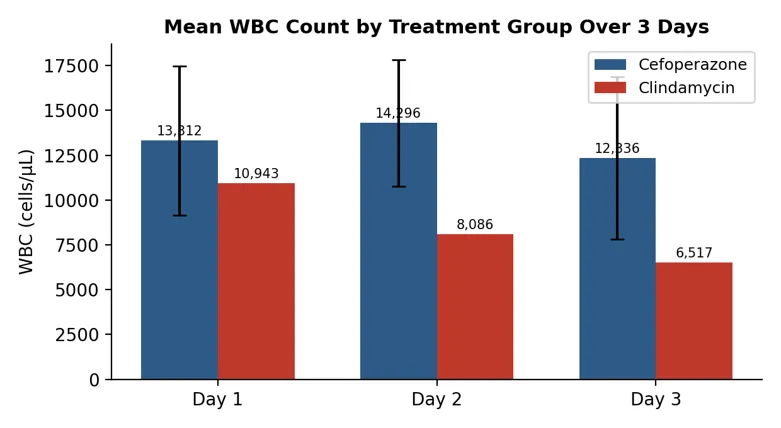
Figure 1: Bar graph depicting mean WBC count by treatment group over three days.
RESULT:
On Day 1, mean WBC was higher in the cefoperazone group (13,312 cells/µL) than in the clindamycin group (10,943 cells/µL; p = 0.009). By Day 3, the clindamycin group showed a significantly greater reduction, to 6,517 cells/µL, versus 12,336 cells/µL in the cefoperazone group (p < 0.001), indicating markedly faster control of systemic inflammation with clindamycin therapy.
Table 4: Distribution Based on Mean ESR by Treatment Group
|
Day |
Treatment |
Mean (mm/hr) |
Std. Deviation |
P value |
|
Day 1 |
Cefoperazone |
34.54 |
12.30 |
0.093 |
|
|
Clindamycin |
29.32 |
— |
|
|
Day 2 |
Cefoperazone |
30.54 |
12.74 |
0.659 |
|
|
Clindamycin |
32.06 |
— |
|
|
Day 3 |
Cefoperazone |
31.12 |
10.47 |
0.233 |
|
|
Clindamycin |
28.18 |
— |
|
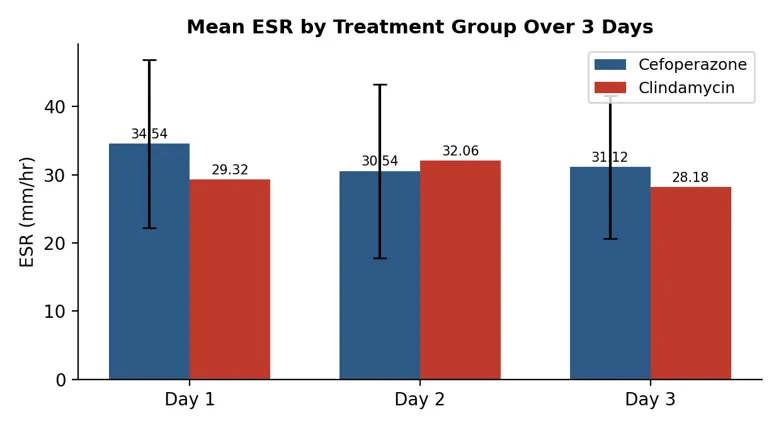
Figure 2: Bar graph depicting mean ESR by treatment group over three days.
RESULT:
ESR values showed a numerical decline in the clindamycin group across the three days; however, between-group differences did not reach statistical significance (p = 0.093, 0.659, and 0.233 on Days 1, 2, and 3, respectively). This is attributable to the inherently slower kinetics of ESR as an inflammatory marker, which responds more gradually than WBC or CRP within a short observation window.
Table 5: Distribution Based on Mean CRP by Treatment Group
|
Day |
Treatment |
Mean (mg/dL) |
Std. Deviation |
P value |
|
Day 1 |
Cefoperazone |
26.45 |
15.59 |
<0.001 |
|
|
Clindamycin |
19.84 |
— |
|
|
Day 2 |
Cefoperazone |
32.17 |
11.98 |
<0.001 |
|
|
Clindamycin |
17.53 |
— |
|
|
Day 3 |
Cefoperazone |
31.16 |
14.78 |
<0.001 |
|
|
Clindamycin |
13.29 |
— |
|
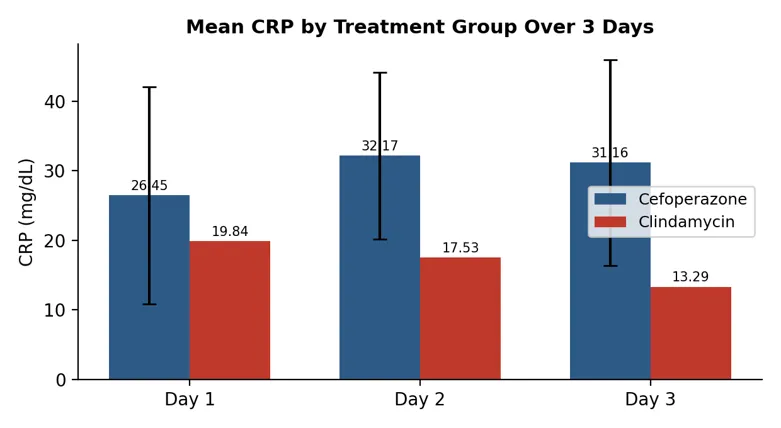
Figure 3: Bar graph depicting mean CRP by treatment group over three days.
RESULT:
CRP demonstrated the most striking inter-group difference among all markers assessed. On Day 1, mean CRP was 26.45 mg/dL in the cefoperazone group versus 19.84 mg/dL in the clindamycin group (p < 0.001). The divergence widened progressively, with Day 3 values of 31.16 mg/dL versus 13.29 mg/dL respectively (p < 0.001), confirming clindamycin's superior anti-inflammatory efficacy as measured by this sensitive acute-phase reactant.
DISCUSSION:
This prospective study represents a head-to-head comparison of two widely used antibiotics in soft tissue infection management — cefoperazone and clindamycin — using objective laboratory markers as the primary efficacy endpoints. The well-matched demographic baseline (age and gender) strengthens the internal validity of the comparative analysis.
The superior performance of clindamycin in reducing WBC count and CRP over three days is consistent with its well-established pharmacological advantages in soft tissue infection. Clindamycin's mechanism of action — inhibition of the 50S ribosomal subunit — not only arrests bacterial protein synthesis but also suppresses production of bacterial exotoxins, including streptococcal pyrogenic exotoxins and staphylococcal toxins.[6] This anti-toxin effect is particularly relevant in necrotizing and abscess-forming infections, explaining why clindamycin was the preferred agent for abscess cases in this cohort.
The markedly superior CRP reduction in the clindamycin group (Day 3: 13.29 vs. 31.16 mg/dL; p < 0.001) is a clinically meaningful finding, as CRP is a sensitive, real-time marker of systemic inflammatory response that responds rapidly to effective antibiotic therapy.[9] The progressively widening CRP gap between groups suggests that clindamycin's anti-inflammatory effect is not merely additive, but amplifies over time as toxin suppression accumulates.
Diabetes mellitus was significantly more prevalent in the clindamycin group (41.2% vs. 7.7%; p = 0.029) — a population that is inherently harder to treat owing to impaired immunity, microvascular compromise, and poor wound healing — which makes the superior efficacy outcomes observed with clindamycin even more noteworthy. This finding aligns with existing evidence supporting the use of clindamycin in immunocompromised and high-risk patient groups.
Cefoperazone, while demonstrating clinical utility — particularly in cellulitis (50% of its cohort) and in settings requiring Gram-negative or polymicrobial coverage — showed a paradoxical rise in mean WBC on Day 2 (14,296 cells/µL from a Day 1 baseline of 13,312 cells/µL). This transient worsening of the inflammatory index may reflect cefoperazone's bactericidal mechanism, which involves rapid bacterial lysis and consequent release of endotoxins triggering a transient inflammatory surge — a phenomenon well documented with beta-lactam antibiotics.[5]
The non-significant ESR trend observed in this study is attributable to the physiology of ESR as a marker: it responds more slowly to resolution of inflammation compared with CRP, often lagging by days to weeks, and is therefore less sensitive for capturing short-term (3-day) antibiotic efficacy differences.
These findings are consistent with the broader literature. Swartz established the importance of tissue-penetrant antibiotics with anti-toxin effects in necrotizing infections.[10] May, and Ustin and Malangoni, similarly emphasized that broad-spectrum anaerobic coverage and toxin inhibition are critical determinants of outcome in complicated soft tissue infections.[11,12] The present data extend this evidence by quantifying inflammatory-response kinetics between the two agents in an Indian tertiary-care setting.
A limitation of this study is the relatively short three-day observation window for inflammatory markers, which precludes assessment of complete clinical resolution. The non-randomized allocation to treatment groups — based on physician preference — also represents a potential selection bias, as reflected in the unequal group sizes (n = 26 vs. n = 34). Future studies with randomized allocation, longer follow-up, and culture-sensitivity data would further strengthen the evidence base.
CONCLUSION
Therefore, we conclude that clindamycin is a safe and effective empiric choice for soft tissue infections, offering measurable advantages in inflammatory-marker resolution over cefoperazone, particularly among high-risk and comorbid patients.
CONFLICT OF INTEREST:
The authors declare no conflict of interest.
ACKNOWLEDGMENT:
The authors acknowledge the management of Bharat School of Pharmacy, Mangalpally, Hyderabad, and the faculty and staff of Durgabhai Deshmukh Hospital and Research Centre (DDHRC), Hyderabad, for their support in facilitating this study.
REFERENCES

Haritha Pasupulati, Vedant Bhoskar, V. Mounika, V. Kapil Sibal, A. Siva Prasad, Comparative Efficacy of Cefoperazone and Clindamycin in the Management of Soft Tissue Infections: A Prospective Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 3129-3136. https://doi.org/10.5281/zenodo.21381098
 10.5281/zenodo.21381098
10.5281/zenodo.21381098