
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy, Bharat Institute of Pharmacy, Mangalpally, Hyderabad, 501510.
AIM: To analyse the drug prescription patterns, titrations and adverse effects of patients with ADHFOBJECTIVESWhen analyzing drug prescription patterns, titrations, and adverse effects for inpatients admitted with acute decompensated heart failure (ADHF), the following objectives should guide the analysis:I. ASSESS PRESCRIPTION PATTERNS:• Identify Commonly Prescribed Medications: Determine which medications (e.g. diuretics, vasodilators, inotropes, beta-blockers, ACE inhibitors, ARBs, ARNIs, aldosterone antagonists) are frequently used.• Evaluate Alignment with Guidelines: Examine whether these prescriptions adhere to clinical guidelines (e.g., ACC/AHA, ESC) for managing ADHF.• Review Medication Combinations: Analyze common combinations of drugs and their appropriateness for different patient profiles.• Analyze Titration Practices: Evaluate Initial Dosing: Review the initial dosages of medications and the rationale behind these decisions.• Monitor Titration Strategies: Assess how and when medications are titrated, including increments, frequency, and goals.• Identify Barriers to Titration: Explore any challenges encountered during titration, such as adverse effects or clinical instability. II.DOCUMENT AND ANALYS ADVERSE EFFECTS:• Record Adverse Effects: Track the frequency and types of adverse effects experienced by patients, such as hypotension, renal dysfunction, or electrolyte imbalances.• Analyze Relationship to Medications: Investigate how specific medications and their dosages contribute to adverse effects.• Identify Risk Factors: Examine patient-specific factors (e.g., age, comorbid conditions) that may increase the risk of adverse effects. III. EVALUTE TREATMENT EFFICACY:• Assess Clinical Outcomes: Reviewclinical outcomes, including symptom relief, hemodynamic improvements, and overall stabilization.• Monitor Biomarkers: Analyze changes in biomarkers (e.g., BNP, NT-proBNP) to.evaluate the effectiveness of treatment IMPACTONHOSPITALIZATION:• Analyze Length of Stay: Examine how different prescription and titration practices affect the length of hospital stay.• Review Readmission Rates; Investigate whether certain prescribing patterns or titration strategies are associated with higher or lower rates of readmission.V. EXAMINE DRUG-DRUG INTERACTIONS• Identify Potential Interactions: Assess potential interactions between prescribed drugs that may impact efficacy or safety.• Evaluate Impact of Interactions: Determine how drug interactions affect patient outcomes and the incidence of adverse effects•Assess Patient Adherence and Education: Evaluate Adherence During Hospitalization: Monitor patient adherence to prescribed regins and the effectiveness of any adherence strategies.VI. DEVELOP RECOMMENDATIONS FOR PRACTICE IMPROVEMENT:• Identify Gaps and Opportunities: Use the analysis to identify areas for improvement in drug prescription and titration practices.• Formulate Evidence-Based Guidelines: Develop or refine clinical guidelines and or protocols based on findings to enhance patient care and outcomes.MATERIALS AND METHODS:The study is conducted as prospective observational study in the department of out and in patient unit of cardiology at Krishna Institute of Medical Sciences {KIMS}hospital in secunderabad. The study duration is 6 months, the sample size consists of 60 subjects.RESULTS AND DISCUSSIONS:Among 60 ADHF patients, 51.7% were male, with an average age of 66 years. Key clinical parameters showed significant variability, with a mean NT-proBNP of 8,285.36 pg/mL and an ejection fraction of 35.78%, indicating predominant HFrEF. Diabetes (65%) and hypertension (60%) were the most common comorbidities. ADHF severity varied, with 65% in the general category and 45% having severe LV dysfunction. Beta-blockers (68.3%) were the most prescribed drugs, followed by MRAs (43.3%) and ARNI/ARB/ACEi (25%). Ivabradine had the highest adverse event rate (100%), while Dapagliflozin 10mg was the most used SGLT-2 inhibitor (43.3%). These findings highlight diverse treatment patterns, disease severity, and drug tolerability in ADHF management.CONCLUSION:By summarizing the statistical data of our study, we have observed that most patients had reduced ejection fraction, with diabetes (65%) and hypertension (60%) being the most prevalent comorbidities. Beta-blockers (68.3%) were the most commonly prescribed medications, with slight titrations observed, particularly in Metoprolol Succinate and Bisoprolol doses. MRAs (43.3%) and ARNI/ARB/ACEi (25%) were also utilized, with adjustments in Sacubitril/Valsartan and Ramipril doses. SGLT-2 inhibitors were prescribed in 21.7% of cases. Among adverse effects, Ivabradine had the highest incidence (100%), followed by Carvedilol and Valsartan (50%).
HEART FAILURE:
The World Health Organization (WHO) defines heart failure as a clinical syndrome with symptoms caused by structural or functional abnormalities of the heart. It is also characterized by elevated natriuretic peptide levels and/or evidence of congestion.[1]
STAGES OF HEART FAILURE:
STAGE A:
Stage A heart failure has no noticeable symptoms. While some risk factors, like genetics and family history, cannot be controlled, others are modifiable.[2] These include hypertension, diabetes, obstructive heart disease, and obesity. Additionally, the risk of heart failure increases with exposure to certain medications or toxic substances, such as alcohol, cocaine, and methamphetamines. Cancer treatments, including radiation and specific chemotherapy drugs, can also contribute to the risk.[3]
Treatment of stage A Heart failure:
Managing Stage A heart failure requires progressive lifestyle changes, including controlling blood pressure, blood sugar, and cholesterol. Adopting a healthy diet, exercising regularly, and avoiding excessive alcohol consumption and smoking are also essential.
Non-invasive imaging techniques, such as Doppler echocardiography, and invasive hemodynamic testing can help identify excessive filling pressures.
STAGE B:
Stage B heart failure, also called pre-heart failure, has no symptoms but shows structural or functional heart abnormalities. These include valve issues, reduced heart wall thickness, diastolic dysfunction, and decreased ejection fraction (systolic heart failure). Elevated heart markers like BNP, creatine kinase, and troponin may also indicate risk.
Treatment of stage B Heart failure:
Like Stage A, Stage B heart failure requires lifestyle changes. Additionally, patients with a history of heart attacks or reduced ejection fraction may benefit from ACE inhibitors, ARBs, or beta blockers.[4]
STAGE C:
Stage C, or symptomatic heart failure, is commonly known as congestive heart failure. It involves cardiac impairment leading to symptoms such as shortness of breath (including at night), coughing, swelling in the legs or abdomen, weight gain, palpitations, dizziness, and reduced appetite.[5]
Treatment of stage C Heart failure:
ACE inhibitors, ARBs, or ARB + neprilysin inhibitor Diuretics. SGLT-2inhibitor, aldosterone antagonist, and beta-blockers.
STAGE D:
End-stage or advanced heart failure often requires medical intervention and hospitalization. The survival rate for individuals with stage D heart failure is only 20%, resulting in a poor prognosis for these patients.
Treatment of stage D Heart failure:
Stage D heart failure is treated with the same medications as Stage C, though low blood pressure and side effects may limit tolerance. Additional treatments include LVADs, inotropes (which aid heart contraction but may cause arrhythmias), heart transplant, and palliative care.[6]
PREVALENCE AND MORTALITY OF HEART FAILURE:
Heart Failure (HF) is a prevalent and debilitating syndrome, leading to significant hospitalization rates, particularly among adults. Its overall prevalence is about 2%, but it affects over 10% of the elderly population (≥ 65 years).[7] HF is often described as a "malignant condition" due to its high mortality rate, which surpasses that of many cancers,[8],[9] with a nearly 100% 10-year mortality rate for newly admitted patients.[10] Common symptoms include dyspnea, congestion, and fatigue, but HF is a heterogeneous condition, categorized into HF with reduced ejection fraction (HFrEF) and HF with preserved ejection fraction (HFpEF).
Recent studies indicate that most re-hospitalizations for heart failure occur shortly after discharge and in the months leading to death, with readmission rates reaching 15–25% within 30 days.[11],[12] Early readmissions are primarily linked to volume overload, while later ones are due to progressive cardiac remodeling.[13],[14],[15],[16] This early post discharge phase is critical for potential interventions. The aim is to review factors that precipitate acute decompensated heart failure (ADHF), identify prognostic factors for higher re-hospitalization rates, and explore interventions that could impact early readmissions and mortality. Updated guidelines on heart failure treatment were also released during this review.[17],[18].
ACUTE DECOMPENSATED HEART FAILURE
Acute decompensated heart failure, often referred to as ADHF, is a critical condition where the heart suddenly cannot pump enough blood to meet the body's needs. ADHF also referd as the sudden or gradual occurrence of signs and symptoms of heart failure. People with ADHF present with various indications of heart failure including blood flow issues and fluid build-up in the body. These require urgent medical treatment. Research suggest that ADHF is not just a worsening of chronic heart failure but a separate clinical condition with certain underlying causes. As such, it requires specific treatment.
EPIDEMILOGY
Epidemiology represents a significant cause of hospital admissions and is associated with considerable morbidity and mortality worldwide.
Global Epidemiology
ADHF is a leading cause of hospitalization among individuals aged 65 and older. In the United States, heart failure affects approximately 6.7 million adults over 20 years of age, with projections indicating an increase to 8.7 million by 2030. The condition accounts for over 1 million hospitalizations annually in the U.S. alone. In Europe, similar trends are observed, with ADHF contributing significantly to cardiovascular-related hospital admissions.
Epidemiology in India
In India, the burden of heart failure, including ADHF, is substantial. Estimates suggest a prevalence ranging from 1.3 million to 4.6 million cases, with an annual incidence between 491,600 and 1.8 million. Notably, patients in India tend to present with ADHF at a younger age compared to Western populations, and they experience higher in-hospital and follow-up mortality rates.[19]
The National Heart Failure Registry of India identifies ischemic heart disease as the predominant cause of heart failure (72%), followed by dilated cardiomyopathy (18%). Rheumatic valvular heart disease accounts for 5.9% of cases. Common comorbidities among these patients include hypertension (48.9%) and diabetes (42.3%).[20]
Risk Factors and Demographics
ADHF primarily affects older adults, with a higher incidence observed in men, though the gender disparity decreases with age. Key risk factors include:
Hypertension Diabetes mellitus
Coronary artery disease Chronic kidney disease Obesity Atrial fibrillation
In India, the younger age of onset for ADHF may be linked to a higher prevalence of risk factors such as hypertension, diabetes, and ischemic heart disease. Additionally, limited access to advanced medical care and delayed diagnosis contribute to poorer outcomes.[21]
Hospitalization and Mortality Rates
ADHF is a leading cause of hospitalization among patients over 65 years old. In-hospital mortality rates for ADHF range from 4% to 10% in Western countries. However, in India, mortality rates are notably higher, with reports indicating rates as high as 30.8%. The majority of these deaths are due to progressive heart failure (92%), with the remainder resulting from intractable arrhythmias (6%) or renal failure.[22]
Economic and Public Health Impact
The economic burden of ADHF is considerable, primarily due to frequent hospitalizations and the costs associated with long-term management. In low- and middle-income countries like India, the impact is exacerbated by inadequate healthcare infrastructure and limited access to advanced therapies.
ADHF poses a significant public health challenge globally, with a particularly heavy burden in developing countries such as India. Addressing this issue requires a comprehensive approach, including early detection, optimal medical therapy, lifestyle modifications, and improved healthcare access. Efforts to control risk factors and enhance healthcare infrastructure are essential steps toward reducing the burden of ADHF worldwide.
CLINICAL MANIFESTATIONS
ADHF presents with a wide spectrum of signs and symptoms due to volume overload, pulmonary congestion, and decreased cardiac output. The clinical manifestations can be categorized into: Symptoms of Pulmonary Congestion and Fluid Overload
Symptoms of Low Cardiac Output and Hypoperfusion General Symptoms and Non-specific Findings
1. Symptoms of Pulmonary Congestion and Fluid Overload:
These symptoms occur due to elevated left ventricular filling pressures, leading to increased pulmonary capillary pressure and fluid leakage into the alveoli.
Dyspnea:
Most common symptom in ADHF.
Occurs due to pulmonary congestion and reduced lung compliance. Can present as:
Exertional Dyspnea: Shortness of breath during physical activity.
Orthopnea: Difficulty breathing while lying flat, relieved by sitting up or propping pillows.
Paroxysmal Nocturnal Dyspnea (PND): Sudden, severe breathlessness at night, causing the patient to awaken and sit up for relief.
Cough:
Typically non-productive or frothy sputum if pulmonary edema is present. Caused by fluid accumulation in the alveoli and bronchi.
Wheezing (Cardiac Asthma):
Due to bronchial edema and airway narrowing from pulmonary congestion. Mimics asthma but related to heart failure rather than reactive airway disease.
Pulmonary Edema:
Severe form of pulmonary congestion.
Manifests as rapid, labored breathing with pink, frothy sputum. Associated with hypoxia and respiratory distress.
Crackles (Rales) on Auscultation:
Fine crackling sounds heard at lung bases, progressing upward with worsening pulmonary edema. Indicative of fluid in the alveolar spaces.
2. Symptoms of Systemic Congestion:
These occur due to elevated right ventricular pressures leading to venous congestion.
Peripheral Edema:
Swelling in the lower extremities (ankles, legs), sacrum (in bedridden patients), and sometimes abdominal wall.
Pitting edema is commonly seen.
Jugular Venous Distension (JVD):
Elevated jugular venous pressure due to increased right atrial pressure. Best observed at a 45-degree angle with visible neck vein distension.
Hepatomegaly and Hepatojugular Reflux:
Enlarged, tender liver due to hepatic venous congestion.
Positive hepatojugular reflux indicates increased central venous pressure.
Ascites:
Accumulation of fluid in the peritoneal cavity due to chronic venous congestion and elevated hepatic pressure.
Weight Gain:
Rapid weight increase due to fluid retention and edema.
3. Symptoms of Low Cardiac Output and Hypoperfusion:
Result from inadequate cardiac output to maintain sufficient tissue perfusion.
Fatigue and Weakness:
Reduced muscle perfusion and decreased oxygen delivery. Exacerbated by low cardiac output and neurohormonal activation.[23]
Cool Extremities:
Peripheral vasoconstriction as a compensatory response to maintain blood pressure and vital organ perfusion.
Mental Status Changes:
Confusion, dizziness, or decreased alertness due to cerebral hypoperfusion. Often seen in severe low output states or cardiogenic shock
Oliguria:
Decreased urine output (<400 mL/day) due to renal hypoperfusion and activation of the renin-angiotensin-aldosterone system (RAAS).
May progress to acute kidney injury.
Hypotension:
Reduced stroke volume and impaired cardiac output leading to low blood pressure. Indicative of severe left ventricular dysfunction or cardiogenic shock.
4. General Symptoms and Non-Specific Findings:
Tachycardia:
Compensatory increase in heart rate to maintain cardiac output.
May be due to sympathetic nervous system activation or underlying arrhythmias.
Tachypnea:
Rapid breathing due to pulmonary congestion and hypoxia. Often seen in pulmonary edema.
Anxiety and Restlessness:
Caused by hypoxia, dyspnea, and sympathetic nervous system activation.
Pallor or Cyanosis:
Pale or bluish skin due to poor tissue perfusion and hypoxia.
Cyanosis is more prominent in severe pulmonary congestion or low output states.
Palpitations:
Perception of rapid or irregular heartbeats due to arrhythmias or compensatory tachycardia.
Clinical Classifications Based on Symptoms:
Warm and Wet:
Adequate perfusion (warm extremities) with volume overload (pulmonary or systemic congestion).Most common presentation of ADHF.
Cold and Wet:
Hypoperfusion (cold extremities) with volume overload. Indicates severe left ventricular dysfunction or cardiogenic shock.
Warm and Dry:
Adequate perfusion with no significant congestion. Typically seen in stable heart failure, not ADHF.
Cold and Dry:
Hypoperfusion without congestion.
Seen in low-output states with depleted intravascular volume.
ADHF presents with a combination of pulmonary congestion, systemic congestion, and symptoms of low cardiac output. Clinical manifestations vary depending on the severity of volume overload, pulmonary congestion, and impaired tissue perfusion.
CAUSES:
Causes of Acute Decompensated Heart Failure (ADHF):
1. Cardiac-Related Causes:
Ischemic Heart Disease:
Acute myocardial infarction (heart attack) or worsening myocardial ischemia reduces myocardial contractility and impairs cardiac output. This leads to increased ventricular filling pressures and pulmonary congestion.
Ischemic events also contribute to arrhythmias, which further compromise effective cardiac output.
Arrhythmias:
Atrial fibrillation, atrial flutter, or ventricular tachycardia can cause rapid or irregular heart rates, leading to reduced diastolic filling time and decreased stroke volume.
Loss of atrial contraction in atrial fibrillation reduces ventricular preload, particularly in patients with diastolic dysfunction, leading to decreased cardiac output.
Valvular Heart Disease:
Acute mitral or aortic regurgitation increases volume load on the ventricles, leading to elevated end-diastolic pressures and pulmonary congestion.
Acute aortic stenosis increases afterload, significantly reducing stroke volume and causing hypotension and pulmonary edema.
Hypertensive Crisis:
A sudden and severe increase in blood pressure elevates afterload, impairing left ventricular ejection. This leads to decreased cardiac output and increased pulmonary capillary pressures, resulting in pulmonary edema. Myocarditis or Cardiomyopathy:
Inflammatory conditions (e.g., viral myocarditis) or structural abnormalities (e.g., dilated cardiomyopathy) impair myocardial contractility and relaxation.
This reduces stroke volume and cardiac output, leading to elevated filling pressures and congestion.
2. Dietary Volume Overload and Fluid Retention:
Indiscretion:
Excessive salt or fluid intake increases extracellular volume, exacerbating fluid overload.
This raises preload and ventricular filling pressures, leading to pulmonary and systemic congestion.
Nonadherence to Diuretics:
Skipping or discontinuing diuretic medications leads to sodium and fluid retention, worsening volume overload. Increased venous return to the heart elevates ventricular filling pressures, contributing to dyspnea Renal Dysfunction:
Acute or chronic kidney disease impairs sodium and water excretion, leading to volume overload.
Reduced renal perfusion in heart failure further activates the renin-angiotensin-aldosterone system (RAAS),
promoting fluid retention and worsening congestion.
3. Medication-Related Causes:
Negative Inotropes:
Certain medications (e.g., calcium channel blockers, antiarrhythmics) reduce myocardial contractility, decreasing cardiac output.
This leads to elevated ventricular filling pressures and fluid congestion.
NSAIDs or Steroids:
Nonsteroidal anti-inflammatory drugs (NSAIDs) inhibit renal prostaglandins, reducing renal perfusion and causing sodium and fluid retention.
Corticosteroids increase sodium retention and volume overload, worsening heart failure symptoms.
Discontinuation of Heart Failure Medications:
Abrupt withdrawal of medications such as beta-blockers or ACE inhibitors can destabilize heart failure management. This leads to neurohormonal activation, increased afterload, and fluid retention, precipitating ADHF.
4. Infections and Systemic Factors:
Respiratory Infections (e.g., Pneumonia):
Infections increase metabolic demand and pulmonary vascular resistance, exacerbating pulmonary congestion.
Fever and inflammation raise heart rate and myocardial oxygen demand, potentially triggering decompensation.
Sepsis or Systemic Inflammatory Response:
Sepsis causes systemic vasodilation and increased capillary permeability, leading to hypotension and hypoperfusion.
This can result in myocardial depression, reduced cardiac output, and worsening heart failure.
5. Other Contributing Factors:
Pulmonary Embolism:
Obstruction of pulmonary arteries increases right ventricular afterload, leading to right ventricular failure. Reduced left ventricular filling results in decreased cardiac output and systemic hypotension.
Anemia or Thyrotoxicosis:
Anemia reduces oxygen-carrying capacity, increasing cardiac output demand to maintain oxygen delivery.
Thyrotoxicosis increases heart rate and contractility, raising myocardial oxygen demand and precipitating heart failure in vulnerable patients.
Physical or Emotional Stress:
Acute stress activates the sympathetic nervous system and RAAS, increasing heart rate, blood pressure, and myocardial oxygen demand.
This neurohormonal surge can precipitate ADHF, especially in patients with underlying cardiac dysfunction. These factors may act individually or in combination, overwhelming the compensatory mechanisms of the heart and leading to acute decompensation.
RISK FACTORS
Risk factors for ADHF may include:
Acute coronary syndrome, which are conditions that cause a sudden, reduced blood flow to the heart High blood pressure
Diabetes
Ischemic heart disease
Chronic obstructive pulmonary disease
A history of stroke or transient ischemic attack Chronic kidney disease Being of older age
A history of heart attack, heart bypass surgery, or infections.
PATHOPHYSIOLOGY
The pathophysiology of acute decompensated heart failure (ADHF) involves multiple interrelated mechanisms that contribute to the progression of the condition:
1. Hemodynamic Alterations:
Elevated Cardiac Filling Pressures: In ADHF, there is an increase in left ventricular end- diastolic pressure due to impaired ventricular relaxation or increased ventricular stiffness. This leads to elevated pulmonary venous pressures, causing pulmonary congestion and dyspnea. The increased pressure is transmitted backward into the pulmonary circulation, resulting in fluid leakage into the alveolar spaces and subsequent pulmonary edema.[24]
Reduced Cardiac Output: Diminished myocardial contractility, often due to ischemic heart disease, cardiomyopathy, or other underlying cardiac conditions, leads to decreased cardiac output. This reduction impairs tissue perfusion and oxygen delivery, affecting vital organs such as the kidneys, brain, and skeletal muscles. Consequently, patients may experience symptoms like fatigue, confusion, and renal dysfunction.
2. Neurohormonal Activation:
Sympathetic Nervous System (SNS): In response to decreased cardiac output, the body activates the SNS to maintain blood pressure and perfusion. This leads to increased heart rate and peripheral vasoconstriction. While initially compensatory, prolonged SNS activation becomes detrimental as it heightens myocardial oxygen demand, promotes arrhythmias, and contributes to adverse cardiac remodeling.
Renin-Angiotensin-Aldosterone System (RAAS): Reduced renal perfusion activates the RAAS, leading to the release of renin, which converts angiotensinogen to angiotensin I. Subsequently, angiotensin I is converted to angiotensin II, a potent vasoconstrictor that increases afterload and blood pressure. Angiotensin II also stimulates aldosterone secretion, promoting sodium and water retention. This exacerbates fluid overload, increases preload and afterload, and further impairs cardiac function.
3. Vascular Dysfunction:
Endothelial Dysfunction: In ADHF, impaired endothelial function leads to reduced nitric oxide(NO) availability, a critical vasodilator. The resulting imbalance between vasodilators and vasoconstrictors causes increased systemic vascular resistance, elevating cardiac workload. Additionally, endothelial dysfunction promotes inflammation and thrombogenesis, contributing to disease progression.
4. Inflammatory and Oxidative Stress:
Cytokine Release: Elevated levels of pro-inflammatory cytokines such as tumor necrosis factor- alpha (TNF-α) and interleukins contribute to myocardial dysfunction and adverse cardiac remodeling. These cytokines induce myocyte apoptosis, fibrosis, and changes in extracellular matrix composition, impairing cardiac contractility and relaxation.
Oxidative Stress: Increased production of reactive oxygen species (ROS) in the failing myocardium leads to oxidative damage of cellular components, including lipids, proteins, and DNA. This oxidative stress impairs myocardial contractility, reduces NO bioavailability, and exacerbates endothelial dysfunction, further worsening cardiac performance.
5. Cardiorenal Interactions:
Worsening Renal Function: In ADHF, decreased renal perfusion due to low cardiac output activates neurohormonal systems, leading to sodium and water retention. Elevated venous pressures impair renal function, creating a detrimental feedback loop known as cardiorenal syndrome.[25] This exacerbates fluid overload, increases venous congestion, and perpetuates heart failure symptoms. Additionally, impaired renal clearance of neurohormones and inflammatory mediators contributes to disease progression.
DIAGNOSIS
Diagnosing Acute Decompensated Heart Failure (ADHF) involves a systematic approach that includes a thorough clinical evaluation, laboratory tests, imaging studies, and, in some cases, invasive hemodynamic monitoring. The goal is to confirm heart failure, assess its severity, identify precipitating factors, and differentiate it from other conditions that mimic heart failure symptoms.
1. Clinical Evaluation:
History and Symptom Assessment:
A detailed patient history is crucial for the diagnosis of ADHF[26] . Key aspects include:
Dyspnea:
Exertional Dyspnea: Shortness of breath on exertion.
Orthopnea: Difficulty breathing when lying flat, relieved by sitting up.
Paroxysmal Nocturnal Dyspnea: Sudden shortness of breath at night, causing the patient to wake up gasping for air.
Fatigue and Weakness: Due to decreased cardiac output and reduced oxygen delivery to tissues.
Peripheral Edema: Swelling in the legs, ankles, or abdomen due to fluid retention.
Weight Gain: Rapid weight increase due to fluid accumulation. Cough and Wheezing: Resulting from pulmonary congestion. Abdominal Discomfort: Due to hepatic congestion and ascites.
Decreased Exercise Tolerance: Marked reduction in physical activity capacity. Chest Pain or Pressure: May indicate ischemic heart disease as a precipitant Precipitating Factors:
Identifying triggers is essential for tailored management. Common precipitants include:
Cardiac Causes:
Acute Myocardial Infarction (AMI)
Arrhythmias: Atrial fibrillation, ventricular tachycardia. Hypertensive Crisis Valvular Heart Disease
Non-Cardiac Causes:
Infections: Pneumonia, sepsis.
Renal Dysfunction: Leading to fluid overload.
Non-Adherence: To medications or dietary restrictions. Pulmonary Embolism
Medications: NSAIDs, corticosteroids, or negative inotropes.
2. Physical Examination: General Appearance:
Respiratory Distress: Increased work of breathing, use of accessory muscles.
Cyanosis or Pallor: Due to hypoxemia or poor perfusion.
Vital Signs:
Blood Pressure:
Hypertension: Can precipitate ADHF.
Hypotension: Suggests low cardiac output and poor perfusion.
Heart Rate:
Tachycardia: From sympathetic stimulation or arrhythmias.
Bradycardia: In cases of conduction disturbances or medication effects.
Respiratory Rate:
Tachypnea due to pulmonary congestion and hypoxemia.
Jugular Venous Pressure (JVP):
Elevated JVP indicates increased right atrial pressure and systemic venous congestion.[27]
Pulmonary Examination:
Pulmonary Rales or Crackles: Due to alveolar fluid accumulation.
Wheezing (Cardiac Asthma): From bronchial congestion. Pleural Effusion: Reduced breath sounds at lung bases.
Cardiac Examination:
S3 Gallop: Indicative of increased left ventricular filling pressure.
S4 Heart Sound: Due to reduced ventricular compliance (diastolic dysfunction).
Murmurs: From valvular disease (e.g., mitral regurgitation).
Displaced Apical Impulse: Suggestive of left ventricular hypertrophy.
Peripheral Examination:
Peripheral Edema: Pitting edema in lower extremities. Hepatojugular Reflux: Exaggerated JVP with abdominal compression. Ascites: Fluid accumulation in the abdomen due to hepatic congestion.
3. Laboratory Tests:
B-type Natriuretic Peptide (BNP) or NT-proBNP:
BNP and NT-proBNP are released from ventricular myocardium in response to stretch and increased wall tension.[28]
BNP > 100 pg/mL or NT-proBNP > 300 pg/mL suggests heart failure. Higher levels indicate more severe heart failure and worse prognosis. Low levels (<100 pg/mL) make ADHF unlikely.
Factors influencing levels:
Elevated in renal dysfunction, sepsis, and pulmonary hypertension. Lower in obesity.
Cardiac Biomarkers:
Troponin I or T:
Elevated levels indicate myocardial injury or ischemia.
Can be elevated in ADHF due to myocardial stress, even without acute coronary syndrome. Complete Blood Count (CBC):
To evaluate for anemia or infection that can exacerbate heart failure.[29]
Serum Electrolytes and Renal Function:
Sodium (Hyponatremia): Indicates severe heart failure and poor prognosis.
Potassium: Monitor for hypo/hyperkalemia due to diuretics or RAAS inhibitors.
Creatinine and BUN: Assess renal function, which can worsen due to reduced perfusion or diuretics.
Liver Function Tests:
Elevated liver enzymes (AST, ALT, bilirubin) suggest hepatic congestion.
Thyroid Function Tests:
Hyperthyroidism or hypothyroidism can precipitate heart failure.
4. Imaging Studies: Chest X-Ray:
Cardiomegaly: Enlarged cardiac silhouette.
Pulmonary Congestion: Perihilar haze, Kerley B lines.
Alveolar Edema: "Bat wing" pattern of opacities.
Pleural Effusion: Often bilateral.
Echocardiography:
Assessment of Cardiac Structure and Function:
Left Ventricular Ejection Fraction (LVEF): To differentiate:
Heart Failure with Reduced Ejection Fraction (HFrEF): LVEF < 40% Heart Failure with Preserved Ejection Fraction (HFpEF): LVEF ≥ 50% Diastolic Dysfunction: Assess ventricular compliance.
Valvular Abnormalities: Mitral or aortic regurgitation.
Pulmonary Artery Pressure: Estimation of pulmonary hypertension. Wall Motion Abnormalities: Indicating ischemic heart disease.
Electrocardiogram (ECG):
To detect:
Ischemia or Infarction: ST-segment changes, T-wave inversions.
Arrhythmias: Atrial fibrillation, ventricular tachycardia.
Conduction Abnormalities: Left bundle branch block, AV block.[30]
Left Ventricular Hypertrophy (LVH).
4. Advanced Diagnostic Tools:
Cardiac Magnetic Resonance Imaging (MRI):
Detailed evaluation of ventricular function, structure, and fibrosis. Useful in cardiomyopathies and myocarditis.
Computed Tomography (CT) Scan:
To evaluate for pulmonary embolism or aortic dissection.
Nuclear Imaging:
SPECT or PET: To assess myocardial perfusion and viability.
5. Invasive Hemodynamic Monitoring:
Right Heart Catheterization (Swan-Ganz Catheter):
Indications:
Unclear diagnosis.
Severe or refractory heart failure. Evaluation of pulmonary hypertension.
Measurements:
Pulmonary Capillary Wedge Pressure (PCWP): >18 mmHg in left heart failure. Cardiac Output and Cardiac Index.Systemic and Pulmonary Vascular Resistance.
6. Differential Diagnosis:
Chronic Obstructive Pulmonary Disease (COPD) Exacerbation Pneumonia or Acute Respiratory Distress Syndrome (ARDS)
Pulmonary Embolism, Acute Coronary Syndrome, Renal Failure with Fluid Overload
TREATMENT IN ACUTE PHASE OF HEART FAILURE
The primary goals of acute-phase treatment for ADHF are to stabilize the patient, relieve symptoms, optimize hemodynamics, and address any underlying causes or precipitating factors. The approach is typically individualized, based on the patient's clinical presentation and hemodynamic status.
1. Initial Assessment and Stabilization:
Airway and Breathing:
Ensure airway patency and provide supplemental oxygen to maintain oxygen saturation >90%. For severe respiratory distress or hypoxemia, consider non-invasive positive pressure ventilation (NIPPV) like CPAP or BiPAP.
In cases of respiratory failure, invasive mechanical ventilation may be necessary.
Circulation and Hemodynamics:
Monitor vital signs continuously, including blood pressure, heart rate, oxygen saturation, and urine output. Cardiac telemetry is recommended to detect arrhythmias.
2. Pharmacologic therapy:
a. Diuretics
Purpose:
Reduce fluid overload, relieve symptoms of congestion (e.g., dyspnea, edema), and decrease preload on the heart.[31]
Types and Mechanism of Action:
Loop Diuretics: Inhibit the Na-K-2Cl cotransporter in the ascending loop of Henle, increasing sodium, chloride, and water excretion.
Examples: Furosemide, Bumetanide, Torsemide.
Thiazide Diuretics: Inhibit sodium reabsorption in the distal convoluted tubule. They are often used in combination with loop diuretics for diuretic resistance.
Example: Metolazone.
Administration and Dosing:
Intravenous Administration: Preferred for rapid onset. Typically given as a bolus or continuous infusion.
Dosing Strategy: Initial dose is usually 1-2.5 times the patient's chronic oral dose.
Monitoring and Adjustment:
Urine Output: A target urine output of >500 mL within the first 2 hours is desired. Electrolytes and Renal Function: Monitor potassium, magnesium, and serum creatinine. Adjustments: If diuresis is inadequate:
Increase the dose.
Use a continuous infusion for sustained effect. Combine with thiazide diuretics for a synergistic effect.
Electrolyte imbalances (hypokalemia, hypomagnesemia). Hypotension. Worsening renal function.[32]
Ototoxicity (with high doses of loop diuretics).
b. Vasodilators Purpose:
Reduce preload and afterload, improve cardiac output, and decrease pulmonary congestion. Used primarily in patients with adequate blood pressure (SBP >90 mmHg).[33]
Common Agents and Mechanism of Action:
Nitroglycerin:
Primarily a vasodilator, reducing preload.
At higher doses, it also dilates arterioles, reducing afterload. Rapid onset and short half-life allow easy titration.
Nitroprusside:
Balanced vasodilator (arterial and venous), decreasing both preload and afterload. Used in hypertensive crises or severe mitral regurgitation.
Requires continuous blood pressure monitoring.
Nesiritide:
Recombinant B-type natriuretic peptide that induces vasodilation and natriuresis. Limited use due to hypotension risk and uncertain benefit on outcomes
Administration and Dosing:
Intravenous Infusion: Start at a low dose and titrate based on blood pressure and symptom relief.
Nitroglycerin: Start at 10-20 mcg/min, increase by 10 mcg/min every 5-10 minutes as needed.
Nitroprusside: Start at 0.1-0.2 mcg/kg/min, titrate to effect.[34]
Monitoring and Adjustment:
Hemodynamic Monitoring: Continuous blood pressure monitoring is essential. Renal Function: Nitroprusside is metabolized to cyanide; caution in renal impairment. Potential Adverse Effects: Hypotension.
Reflex tachycardia. Headache and flushing.
Cyanide toxicity (with prolonged Nitroprusside use).
c. Inotropic Agents
Purpose: Enhance myocardial contractility and improve cardiac output.
Primarily used in patients with low cardiac output and evidence of hypoperfusion[35] (e.g., cold extremities, low urine output).
Common Agents and Mechanism of Action:
Dobutamine:
β1-adrenergic agonist with inotropic and mild vasodilatory effects. Increases heart rate and contractility, improving cardiac output.
Milrinone:
Phosphodiesterase-3 inhibitor leading to increased cAMP, enhancing contractility and vasodilation. Useful in patients on beta-blockers as it acts independently of β-receptors.
Longer half-life compared to Dobutamine.
Administration and Dosing:
Dobutamine: Start at 2-5 mcg/kg/min, titrate up to 20 mcg/kg/min based on response.
Milrinone: Loading dose (optional) of 25-50 mcg/kg over 10 minutes, followed by a continuous infusion of 0.375-0.75 mcg/kg/min.
Monitoring and Adjustment:
Hemodynamic Monitoring: Continuous monitoring for blood pressure and cardiac rhythm.
Renal Function: Adjust Milrinone dose in renal impairment.
Potential Adverse Effects:
Arrhythmias (especially ventricular).
Hypotension (due to vasodilatory effect of Milrinone). Tachycardia (more common with Dobutamine).[36]
d. Vasopressors
Purpose:
Maintain adequate perfusion in patients with cardiogenic shock or hypotension unresponsive to inotropes. Used as a temporary measure while addressing the underlying cause.
Common Agents and Mechanism of Action:
Norepinephrine:
Potent α1-adrenergic agonist causing vasoconstriction and increased systemic vascular resistance. Mild β1-adrenergic effect increases heart rate and contractility.
Dopamine:
Dose-dependent effects:
Low dose: Renal vasodilation (no proven benefit in heart failure).
Moderate dose: β1-adrenergic effect increasing contractility.
High dose: α1-adrenergic vasoconstriction.
Administration and Dosing:
Norepinephrine: Start at 0.05-0.5 mcg/kg/min and titrate to maintain mean arterial pressure (MAP) >65 mmHg.
Dopamine: Start at 3-5 mcg/kg/min for inotropic support or higher for vasopressor effects.
Monitoring and Adjustment:
Hemodynamic Monitoring: Continuous blood pressure monitoring required.
Perfusion Status: Monitor urine output and peripheral perfusion.
Potential Adverse Effects:
Arrhythmias (particularly with Dopamine). Increased myocardial oxygen demand. Digital or limb ischemia (with high-dose vasopressors).
3. Non-Pharmacologic Interventions:
a. Ventilatory Support:
Non-Invasive Positive Pressure Ventilation (NIPPV):
Indicated for patients with respiratory distress or severe pulmonary edema. Improves oxygenation and reduces work of breathing.
Mechanical Ventilation:
Consider in cases of severe respiratory failure or altered mental status.
b. Ultrafiltration:
Purpose: To remove excess fluid in cases of diuretic resistance or severe fluid overload. Indications: Diuretic resistance or inadequate diuresis despite high-dose loop diuretics. Renal dysfunction limiting the use of diuretics.
Procedure: Requires central venous access and specialized equipment.
4. Management of Underlying Causes and Precipitating Factors:
Identify and Treat Triggers:
Common precipitating factors include:
Acute Coronary Syndrome: Treat with antiplatelet therapy, anticoagulation, and revascularization
as indicated.
Arrhythmias: Manage with rate control or rhythm correction (e.g., atrial fibrillation).
Hypertensive Emergency: Use intravenous antihypertensives to control blood pressure.
Infections: Prompt initiation of antibiotics for pneumonia or sepsis.
TREATMENT DURING HOSPITALIZATION AND TITRATION UPTO DISCHARGE
A. ARNI[Angiotensin Receptor-Neprilysin Inhibitor]:
ARNI (Angiotensin Receptor-Neprilysin Inhibitor), particularly sacubitril/valsartan (brand name Entresto), has revolutionized the management of Heart Failure (HF),[37] including its role in Acute Decompensated Heart Failure (ADHF). Here’s a detailed overview:
Mechanism of Action:
Sacubitril: Inhibits neprilysin, an enzyme that degrades natriuretic peptides. This leads to: Increased levels of natriuretic peptides (BNP, ANP), enhancing natriuresis (sodium excretion) and diuresis.
Vasodilation, reducing blood pressure and afterload. Inhibition of fibrosis and cardiac remodeling.
Valsartan: An ARB that:
Blocks the angiotensin II receptor, reducing vasoconstriction, aldosterone release, and sympathetic activation. Provides renal protection by decreasing glomerular hypertension.
Clinical Evidence and Indications:
1. PARADIGM-HF Trial(2014):
Demonstrated that sacubitril/valsartan significantly reduced cardiovascular death and HF hospitalizations compared to enalapril (an ACE inhibitor) in chronic heart failure with reduced ejection fraction (HFrEF). Findings:
20% reduction in cardiovascular mortality. 21% decrease in HF hospitalizations. Improved quality of life and symptoms.
Implication: Established ARNI as superior to ACE inhibitors in chronic HFrEF.
2. PIONEER-HF Trial(2019):
Focused on ADHF and showed that initiating sacubitril/valsartan in stabilized patients.
Findings:
Greater reduction in NT-proBNP levels compared to enalapril.
No significant increase in adverse events (e.g., hypotension, renal dysfunction).
Implication: Validated early initiation post-stabilization in ADHF.[38]
3. TRANSITION Trial (2019):
Evaluated the timing of ARNI initiation (pre-discharge vs. post-discharge) in ADHF.
Findings:
Both strategies were well tolerated, with similar safety outcomes. Pre-discharge initiation resulted in faster uptitration to target doses.
Implication: Supports starting ARNI before discharge once hemodynamic stability is achieved.
Titration of ARNI (Sacubitril/Valsartan) in ADHF:
1. General Principles:
Titration should be gradual and individualized based on blood pressure tolerance, renal function, and potassium levels.
The goal is to reach the target dose of 97/103 mg twice daily, as this dose demonstrated the best outcomes in clinical trials.Monitor blood pressure, renal function (eGFR), and electrolytes (especially potassium) closely during titration.[39]
Initial Dosing:
24/26 mg twice daily if:
ACEi/ARB-naive.
Low baseline systolic blood pressure (100-110 mmHg). Moderate renal impairment (eGFR 30-60 mL/min/1.73 m²). Age > 75 years or in patients at risk of hypotension.
49/51 mg twice daily if:
Previously on moderate-to-high doses of ACEi or ARB. Hemodynamically stable with SBP > 110 mmHg. 36-hour washout period is mandatory if transitioning from an ACE inhibitor to avoid the risk of angioedema. No washout is needed if switching from an ARB.
Titration Schedule:
After 2-4 weeks, double the dose if well tolerated:
From 24/26 mg to 49/51 mg twice daily.
From 49/51 mg to 97/103 mg twice daily (target dose).
Dose Adjustments:
If symptomatic hypotension occurs:
Lower the dose or temporarily withhold ARNI.
Optimize diuretic therapy and reduce other vasodilators if possible.
If hyperkalemia (>5.5 mEq/L):
Review dietary potassium intake.
Consider reducing the dose or discontinuing potassium supplements/other medications causing hyperkalemia.
If worsening renal function:
Temporarily reduce or hold ARNI, reassess volume status, and adjust diuretics accordingly.
Monitoring:
Blood pressure: Watch for hypotension, especially in patients with low baseline BP.
Renal function: Monitor serum creatinine and electrolytes, particularly potassium.
NT-proBNP rather than BNP for HF monitoring, as BNP levels may be elevated due to neprilysin inhibition.
Contraindications and Precautions:
Contraindications:
History of angioedema associated with ACE inhibitors or ARBs. Severe renal impairment (eGFR < 30 mL/min/1.73 m²).
Hyperkalemia (K+ > 5.5 mEq/L). Pregnancy and lactation.
Drug Interactions:
Avoid concomitant use with ACE inhibitors (36-hour washout needed).
Caution with potassium-sparing diuretics and NSAIDs, which may exacerbate hyperkalemia.
Advantages in ADHF:
Hemodynamic Benefits: Enhanced natriuresis, reduced preload and afterload, improved cardiac output without increasing heart rate.
Symptomatic Relief: Rapid improvement in dyspnea and congestion symptoms.
Prognostic Impact: Reduced mortality and rehospitalization rates due to the dual neurohormonal blockade.
Practical Considerations:
Transition from ACEi/ARB:
Ensure the 36-hour washout if transitioning from ACE inhibitors to minimize angioedema risk. Can switch directly from an ARB without a washout period.
Special Populations:
Elderly: Initiate at the lower dose to minimize hypotension risk.
Renal Impairment: Dose adjustment required; contraindicated in severe renal dysfunction.
Side Effects of ARNI (Sacubitril/Valsartan):
Common Side Effects:
Hypotension (18-20%):
Most common adverse effect due to vasodilation.
Risk is higher in elderly, low baseline blood pressure, or those on high-dose diuretics.
Management:
Lower the dose or titrate more slowly.
Adjust diuretic or other antihypertensive therapies.
Hyperkalemia (12-16%):
Due to RAAS blockade, especially in patients with CKD, diabetes, or those on potassium-sparing diuretics.
Management:
Monitor potassium levels regularly. Dietary potassium restriction. Adjust dose or discontinue if persistent.
Renal Dysfunction (10-15%):
Can occur due to reduced glomerular filtration pressure.
More common in patients with pre-existing CKD or volume depletion.
Management:
Monitor serum creatinine and eGFR.
Adjust diuretic dosing to optimize volume status.
Dose reduction or temporary discontinuation if significant worsening occurs.
Less Common Side Effects:
Cough: Less common than with ACE inhibitors but may occur due to increased bradykinin levels.
Dizziness and Fatigue: Often related to hypotension; dose adjustment may help.
Gastrointestinal Symptoms: Nausea and diarrhea are rare but possible.
Serious Adverse Effects:
Angioedema (<1%):
Rare but potentially life-threatening, especially in patients with a history of angioedema with ACE inhibitors. More common in African American patients.
Management:
Discontinue ARNI immediately and provide supportive care.
Contraindicated in patients with a history of angioedema related to ACE inhibitors or ARBs. Hypersensitivity Reactions: Including rash and pruritus, though rare.
B. ARB(Angiotensin receptor blockers):
ARBs block the effects of angiotensin II at the AT1 receptor, leading to:
Vasodilation: Reduces afterload and systemic vascular resistance.
Reduced aldosterone secretion: Decreases sodium and water retention, lowering preload.
Anti-fibrotic effects: Prevents cardiac remodeling and improves ventricular compliance.
Reduced sympathetic activation: Lowers heart rate and blood pressure, decreasing myocardial workload.[40]
Commonly used ARBs in heart failure include:
1. Valsartan: Initial Dose:
40 mg twice daily in naive patients or those with low blood pressure.
Target Dose:
160 mg twice daily.
Clinical Evidence:
VALIANT Trial: Showed non-inferiority to captopril in reducing mortality post-myocardial infarction with heart failure.
2. Candesartan:
Initial Dose:
4-8 mg once daily.
Target Dose:
32 mg once daily.
Clinical Evidence:
CHARM Program: Demonstrated a reduction in cardiovascular death and heart failure hospitalizations.
3. Losartan:
Initial Dose:25-50 mg once daily.
Target Dose: 150 mg once daily.
Clinical Evidence:
OPTIMAAL Trial: Showed efficacy but was less effective than captopril in reducing mortality post- MI.
Initiation and Titration Guidelines:
General Principles:
Start at the lowest dose and titrate gradually every 1-2 weeks to target dose. Monitor closely for blood pressure, renal function, and potassium levels.[41]
Titration should be slower in elderly patients and those with renal impairment.
Titration Schedule:
Start Low:
Valsartan 40 mg BID or Candesartan 4 mg QD. Double Dose Every 1-2 Weeks if tolerated: Valsartan 40 → 80 → 160 mg BID.
Candesartan 4 → 8 → 16 → 32 mg QD.
Target Dose:
Valsartan 160 mg BID or Candesartan 32 mg QD.
Monitoring Parameters:
Blood Pressure: Risk of hypotension, especially in volume-depleted patients.
Renal Function: Monitor serum creatinine and eGFR. Electrolytes: Potassium levels for hyperkalemia risk. Contraindications:
History of angioedema with ARBs. Bilateral renal artery stenosis.
Severe hyperkalemia (>5.5 mEq/L). Pregnancy and breastfeeding.
Drug Interactions:
Potassium-sparing diuretics and supplements: Increases risk of hyperkalemia.
NSAIDs: May worsen renal function and increase hyperkalemia risk.
Lithium: Risk of lithium toxicity due to reduced clearance.
Practical Considerations:
Transition from ACE Inhibitors:
No washout required but closely monitor for hypotension and hyperkalemia.
Combination Therapy:
Safe with beta-blockers, diuretics, and MRAs (Mineralocorticoid Receptor Antagonists).
Avoid combination with:
ACE inhibitors (increased risk of hyperkalemia and renal dysfunction). Direct Renin Inhibitors (e.g., Aliskiren) due to renal risk.
Special Populations:
Elderly: Start at the lower dose due to increased hypotension risk.
Renal Impairment: Use cautiously in moderate renal dysfunction (eGFR 30-60 mL/min/1.73 m²). Avoid in severe renal impairment.
Side Effects of ARBs:
Common Side Effects:
Hypotension (10-15%):
Due to vasodilation and reduced preload/afterload.
More common in volume-depleted patients or those on high-dose diuretics.
Management:
Hold diuretics temporarily if needed. Reduce ARB dose and retitrate gradually.
Hyperkalemia (5-10%):
Due to reduced aldosterone secretion leading to potassium retention. Risk increases with: Renal impairment.
Concurrent use of potassium-sparing diuretics, MRAs (e.g., spironolactone), or potassium supplements.
Management:
Monitor serum potassium frequently, especially during initiation and dose escalation. Reduce dietary potassium intake if needed.
Dose reduction or discontinuation if severe (>5.5 mEq/L).
Renal Dysfunction (2-5%):
Can worsen renal function, especially in patients with: Pre-existing renal disease.
Severe heart failure with reduced renal perfusion. Concurrent use of NSAIDs or diuretics.
Management:
Monitor serum creatinine and eGFR before and after initiation.
Temporary discontinuation if serum creatinine rises >30% from baseline.[42] Adjust dose based on renal function.
Less Common Side Effects:
Dizziness and Headache:
Related to blood pressure changes. Generally transient and dose-dependent.
Fatigue:
Possibly due to reduced blood pressure and improved cardiac output.
Angioedema (Rare but serious):
Less frequent than with ACE inhibitors.
Presents with facial swelling, lip/tongue edema, and difficulty breathing.
Management:
Discontinue ARB immediately.
Treat with antihistamines, corticosteroids, and epinephrine if needed. Contraindicated for re-challenge in patients with angioedema history.
Rare Adverse Effects:
Rash and Pruritus:
Hypersensitivity reactions are rare but possible.
Gastrointestinal Disturbances:
Nausea, diarrhea, or abdominal pain.
Hepatic Dysfunction:
Rarely, elevated liver enzymes have been reported.
C. ANGIOTENSIN-CONVERTING ENZYME(ACE) INHIBITORS:
Angiotensin-Converting Enzyme (ACE) Inhibitors are a cornerstone of heart failure therapy, including in the context of ADHF.
They work by blocking the conversion of angiotensin I to angiotensin II, leading to: Vasodilation (reduced afterload)
Reduced aldosterone secretion (decreased sodium and water retention) Lower sympathetic activity
This results in reduced preload and afterload, improved cardiac output, and decreased morbidity and mortality.[43]
Mechanism of Action:
Angiotensin-Converting Enzyme (ACE) Inhibitors block the conversion of angiotensin I to angiotensin II, resulting in:
Vasodilation: Reduced systemic vascular resistance, lowering afterload.
Decreased Aldosterone Secretion: Reduced sodium and water retention, decreasing preload.
Inhibition of Sympathetic Nervous System Activation: Lowered heart rate and contractility demands. Reduced Cardiac Remodeling: By inhibiting angiotensin II and aldosterone, they decrease myocardial fibrosis and hypertrophy.
Commonly used ACE inhibitors in ADHF include:
Enalapril: Initial dose: 2.5 mg BID, Target dose: 10-20 mg BID
Captopril: Initial dose: 6.25 mg TID, Target dose: 50 mg TID
Ramipril: Initial dose: 1.25-2.5 mg once daily, Target dose: 10 mg once daily Lisinopril: Initial dose: 2.5-5 mg once daily, Target dose: 20-40 mg once daily. Titration Strategy:
Start Low, Go Slow:
Begin with the lowest dose to reduce the risk of hypotension and renal dysfunction. Titrate every 1-2 weeks as tolerated, aiming for the target dose.
Monitoring Requirements:
Blood Pressure: Monitor for hypotension.
Renal Function: Serum creatinine and eGFR.
Electrolytes: Monitor potassium levels to avoid hyperkalemia.
Clinical Trials:
CONSENSUS Trial:
Demonstrated significant mortality reduction with enalapril in severe heart failure.
SOLVD Trial:
Showed improved survival and reduced hospitalizations with enalapril in symptomatic heart failure.
SAVE Trial:
Highlighted the benefit of captopril in reducing mortality after myocardial infarction with left ventricular dysfunction.
ATLAS Trial:
Compared high-dose vs. low-dose lisinopril showing better outcomes with high doses.
Contraindications:
Absolute Contraindications:
History of angioedema associated with ACE inhibitors. Bilateral renal artery stenosis. Pregnancy.
Relative Contraindications:
Hypotension (SBP < 90 mmHg) Hyperkalemia (> 5.5 mEq/L) Acute Kidney Injury (AKI)
Practical Considerations:
Monitor Closely During Initiation:
Blood pressure, renal function, and electrolytes.
Avoid Abrupt Discontinuation:
May lead to rebound hypertension or worsening heart failure.
Patient Education:
Importance of adherence, monitoring for side effects (e.g., cough, dizziness, swelling).
Side Effects:
Hypotension (10-20%):
Especially in volume-depleted patients or those on high-dose diuretics.
Management:
Hold diuretics temporarily if needed.
Reduce ACE inhibitor dose or retitrate gradually.
Renal Dysfunction (5-15%):
Can cause a rise in serum creatinine due to reduced intraglomerular pressure.
Management:
Monitor renal function closely after initiation and dose increases.
Temporary discontinuation if serum creatinine increases >30% from baseline.
Hyperkalemia (5-10%):
Due to reduced aldosterone secretion leading to potassium retention.
Management:
Monitor potassium levels.
Adjust or discontinue potassium supplements or potassium-sparing diuretics if necessary.
Cough (5-20%):
Due to increased bradykinin levels.
Management:
Switch to an ARB if cough is persistent and intolerable.
Angioedema (Rare but serious):
Presents as facial swelling, lip/tongue edema, and difficulty breathing.
Management:
Discontinue ACE inhibitor immediately. Avoid re-challenge.[44]
Treat with antihistamines, corticosteroids, and epinephrine if necessary.
D. BETA BLOCKERS
Beta blockers are cornerstone therapies in chronic heart failure with reduced ejection fraction (HFrEF) due to their long-term benefits in reducing mortality and hospitalizations.[45] However, their role in acute decompensated heart failure (ADHF) is more nuanced due to their negative inotropic effects, which can potentially worsen symptoms if not used judiciously.
Role and Rationale
Chronic Use: Beta blockers reduce sympathetic overactivity, prevent ventricular remodeling, and decrease the risk of arrhythmias.
In ADHF: The decision to continue, reduce, or temporarily discontinue beta blockers depends on the patient's hemodynamic status. Abrupt withdrawal can lead to rebound tachycardia and worsening heart failure, but continuation in unstable patients may exacerbate hypotension or low cardiac output.
Role and Rationale
Chronic Use: Beta blockers reduce sympathetic overactivity, prevent ventricular remodeling, and decrease the risk of arrhythmias.
In ADHF: The decision to continue, reduce, or temporarily discontinue beta blockers depends on the patient's hemodynamic status. Abrupt withdrawal can lead to rebound tachycardia and worsening heart failure, but continuation in unstable patients may exacerbate hypotension or low cardiac output.
Mechanism of Action in ADHF
Beta-1 Receptor Blockade:
Decreases heart rate and contractility, reducing myocardial oxygen demand.
Lowers renin release, decreasing angiotensin II and aldosterone, thus reducing fluid retention and afterload.
Anti-Arrhythmic Effects:
Stabilizes myocardial electrical activity, reducing the risk of ventricular arrhythmias.
Anti-Remodeling Effects:
By reducing sympathetic stimulation, beta blockers decrease ventricular hypertrophy and fibrosis, promoting reverse remodeling.
Choice of Beta Blocker
Only beta blockers with proven benefits in heart failure should be used:
Carvedilol: Non-selective beta blocker with alpha-1 blocking properties, reducing afterload and providing additional vasodilation.
Metoprolol Succinate: Beta-1 selective, preferred for patients with COPD or asthma.
Bisoprolol: Beta-1 selective, with good tolerability and once-daily dosing. Avoid Beta Blockers Without Proven Benefit:
Atenolol, propranolol, and other non-evidence-based agents should be avoided in heart failure.[46]
Titration Strategy
General Principles:
Start Low and Go Slow: Begin at the lowest possible dose and titrate gradually to minimize adverse effects. Titrate Based on Tolerance and Hemodynamics: Adjust doses every 2-4 weeks based on blood pressure, heart rate, and symptom stability.[47]
Goal Doses: Target the maximum tolerated dose or the dose shown to provide mortality benefits in clinical trials.
Starting and Target Doses
Carvedilol (Non-selective beta blocker with alpha-1 blocking properties) Starting Dose:
3.125 mg twice daily for patients with NYHA Class III-IV symptoms.
6.25 mg twice daily for milder symptoms (NYHA Class II).
Target Dose:
25 mg twice daily for patients < 85 kg. 50 mg twice daily for patients > 85 kg.
Titration: Double the dose every 2 weeks if tolerated.
Metoprolol Succinate (Beta-1 selective) Starting Dose:
12.5 mg once daily for NYHA Class III-IV symptoms. 25 mg once daily for milder symptoms (NYHA Class II). Target Dose: 200 mg once daily.
Titration: Double the dose every 2-4 weeks as tolerated. Bisoprolol (Beta-1 selective) Starting Dose: 1.25 mg once daily. Target Dose: 10 mg once daily.
Titration: Double the dose every 2 weeks as tolerated.
Monitoring and Safety
Blood Pressure and Heart Rate:
Monitor at baseline and regularly during titration (every 1-2 weeks). Maintain SBP > 90 mmHg and HR > 50 bpm.
Fluid Status and Weight:
Monitor daily weight and watch for signs of fluid overload. Adjust diuretics as needed to maintain euvolemia.
Renal Function and Electrolytes:
Check renal function and electrolytes periodically, especially in patients on ACE inhibitors or diuretics.
ECG Monitoring:
Especially in patients at risk for bradyarrhythmias or those with baseline conduction abnormalities.
Key Clinical Trials:
1. CIBIS-II (Cardiac Insufficiency Bisoprolol Study II) Beta Blocker Studied: Bisoprolol (Beta-1 selective) Population:
2,647 patients with chronic heart failure (NYHA Class III-IV) and left ventricular ejection fraction (LVEF) ≤ 35%.
Study Design:
Randomized, placebo-controlled, double-blind.
Dose Titration:
Started at 1.25 mg once daily, titrated up to 10 mg once daily.
Key Findings:
34% reduction in all-cause mortality (11.8% vs. 17.3% in placebo). 20% reduction in hospitalizations for worsening heart failure.
Conclusion:
Bisoprolol significantly reduces mortality and hospitalizations in stable chronic HFrEF.
1. MERIT-HF (Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure) Beta Blocker Studied: Metoprolol Succinate (CR/XL) (Beta-1 selective)
Population:
3,991 patients with chronic heart failure (NYHA Class II-IV) and LVEF ≤ 40%.
Study Design:
Randomized, placebo-controlled, double-blind.
Dose Titration:
Started at 12.5 mg or 25 mg once daily, titrated up to 200 mg once daily.
Key Findings:
34% reduction in all-cause mortality (7.2% vs. 11.0% in placebo). 19% reduction in hospitalizations for worsening heart failure.
Conclusion:
Metoprolol Succinate reduces mortality and hospitalizations, supporting its use in stable chronic HFrEF.
2. COPERNICUS (Carvedilol Prospective Randomized Cumulative Survival) Beta Blocker Studied: Carvedilol (Non-selective with alpha-1 blockade) Population: 2,289 patients with severe chronic heart failure (NYHA Class III-IV) and LVEF < 25%. Study Design:
Randomized, placebo-controlled, double-blind.
Dose Titration:
Started at 3.125 mg twice daily, titrated up to 25 mg twice daily.
Key Findings:
35% reduction in all-cause mortality (11.4% vs. 18.5% in placebo). 24% reduction in hospitalization for worsening heart failure.
Conclusion:
Carvedilol reduces mortality and hospitalizations even in severe chronic heart failure.
Notably, patients were required to be clinically stable for at least 2 weeks before enrollment, thus excluding acute decompensation.
3. COMET (Carvedilol or Metoprolol European Trial) Comparison: Carvedilol vs. Metoprolol Tartrate
Population: 3,029 patients with chronic heart failure (NYHA Class II-IV) and LVEF ≤ 35%.
Study Design:
Randomized, double-blind, head-to-head comparison.
Dose Titration:
Carvedilol: 25 mg twice daily. Metoprolol Tartrate: 50 mg twice daily. Key Findings:
17% reduction in all-cause mortality with Carvedilol compared to Metoprolol Tartrate (34% vs. 40%). No significant difference in hospitalization rates between the two groups.
Conclusion:
Carvedilol showed superior mortality benefit compared to Metoprolol Tartrate.
The dose of Metoprolol Tartrate used was lower than the equivalent beta-blocking dose of Carvedilol, which may partly explain the difference in outcomes.
4. SENIORS (Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with Heart Failure)
Beta Blocker Studied: Nebivolol (Beta-1 selective with nitric oxide-mediated vasodilation) Population: 2,128 elderly patients (≥ 70 years) with heart failure (reduced or preserved EF). Study Design:
Randomized, placebo-controlled, double-blind.
Dose Titration:
Started at 1.25 mg once daily, titrated up to 10 mg once daily.
Key Findings:
14% reduction in composite endpoint of all-cause mortality or cardiovascular hospitalizations. No significant difference in all-cause mortality alone.
Conclusion:
Nebivolol was beneficial in reducing hospitalizations in elderly heart failure patients, including those with preserved EF.
5. US Carvedilol Trials
Beta Blocker Studied: Carvedilol
Population: 1,094 patients with mild-to-moderate heart failure (NYHA Class II-III).
Study Design:
Combined analysis of four randomized, placebo-controlled trials.
Key Findings:
65% reduction in all-cause mortality.
27% reduction in hospitalizations for heart failure.
Conclusion: Established carvedilol as one of the most effective beta blockers in reducing mortality in heart failure.
6. Meta-Analysis and Guidelines Overview Meta-Analysis Findings:
Beta blockers significantly reduce mortality (by ~30-35%) and hospitalizations in chronic HFrEF. Benefits observed consistently across different agents (carvedilol, metoprolol succinate, bisoprolol). Adverse Effects and Management
1. Hypotension Mechanism:
Caused by decreased cardiac output and vasodilation (especially with carvedilol due to alpha-1 blockade).
Signs and Symptoms:
Dizziness, lightheadedness, syncope, fatigue.
Management:
Reduce dose or titrate more slowly.
Consider switching to a more beta-1 selective agent like metoprolol succinate or bisoprolol. Adjust concomitant vasodilators (e.g., ACE inhibitors, ARBs) to minimize hypotensive effects. Ensure adequate fluid status but avoid volume overload.
2. Bradycardia and Heart Block Mechanism:
Beta-1 blockade decreases heart rate and can prolong AV node conduction.
Signs and Symptoms:
HR < 50 bpm, fatigue, dizziness, syncope.
Management:
Reduce the dose or increase dosing interval.
Avoid combining with other negative chronotropes (e.g., non-dihydropyridine calcium channel blockers like verapamil or diltiazem).
If severe or symptomatic, hold the medication and consider atropine or temporary pacing if necessary. Rule out other causes of bradycardia (e.g., electrolyte disturbances).
3. Worsening Heart Failure or Fluid Retention Mechanism:
Negative inotropic effect may acutely reduce cardiac output, leading to fluid retention.
Signs and Symptoms:
Increased dyspnea, peripheral edema, weight gain, fatigue.
Management:
Increase diuretic dose to manage fluid overload.
Reduce the beta blocker dose or hold temporarily if symptoms are severe. Ensure the patient is euvolemic before titrating the dose upward.
Avoid rapid dose escalation to prevent decompensation.
4. Fatigue and Weakness Mechanism: Due to decreased cardiac output and reduced exercise tolerance
Management:
Educate patients that fatigue often improves after 1-2 weeks as the body adjusts. Reduce the dose if symptoms are severe or persistent.
Rule out other causes, including anemia or electrolyte imbalances.
5. Bronchospasm (rare with cardioselective beta blockers) Mechanism:
Non-selective beta blockers (like carvedilol) may exacerbate bronchospasm in patients with reactive airway disease.
Management:
Switch to a more beta-1 selective agent (e.g., metoprolol succinate or bisoprolol). Avoid carvedilol in patients with severe asthma or uncontrolled COPD.
6. Depression and Sleep Disturbances Mechanism:
Exact mechanism unclear but may be related to CNS penetration.
Management:
Consider dose reduction or switching to an agent with less CNS penetration. Provide supportive care and monitor mental health.[48]
E. MINERALOCORTICOID RECEPTOR ANTAGONISTS(MRAs)
Mineralocorticoid Receptor Antagonists (MRAs), including Spironolactone and Eplerenone, are critical in managing chronic heart failure with reduced ejection fraction (HFrEF).[49] They inhibit aldosterone's effects, reducing sodium retention, myocardial fibrosis, and ventricular remodeling. However, their role in ADHF is nuanced, as they can affect electrolyte balance and renal function.
Mechanism of Action in ADHF
Block Aldosterone Receptors: In the distal convoluted tubules and collecting ducts, reducing sodium reabsorption and increasing potassium retention.
Decreased Fluid Retention: By promoting natriuresis, MRAs reduce preload and pulmonary congestion. Anti-fibrotic and Anti-remodeling Effects: Long-term use attenuates myocardial fibrosis and remodeling, improving ventricular function.
Neurohormonal Modulation: Inhibits aldosterone's harmful effects, such as sympathetic activation and endothelial dysfunction.[50]
Clinical Use in ADHF
General Principles:
Continuation in Chronic Users: Continue in ADHF patients already on MRAs unless contraindicated by hyperkalemia or worsening renal function.
Initiation During ADHF: Can be initiated if the patient is hemodynamically stable and not hyperkalemic.
Avoid initiation in patients with acute kidney injury, hyperkalemia (K+ > 5.0 mmol/L), or significant hypotension.[51]
Target Population:
ADHF patients with chronic HFrEF (LVEF ≤ 35%) who are euvolemic or mildly congested. Post-acute MI with LV dysfunction and symptoms of heart failure.
Starting and Target Doses
Spironolactone
Starting Dose: 12.5 mg to 25 mg once daily.
Target Dose: 25-50 mg once daily.
Adjustment: Titrate based on serum potassium and renal function.
Eplerenone (more selective with fewer anti-androgenic side effects) Starting Dose: 25 mg once daily.
Target Dose: 50 mg once daily.
Adjustment: Similar titration strategy as Spironolactone.
Titration Strategy
General Principles of Titration
Start Low and Go Slow: Begin with the lowest recommended dose and titrate gradually based on tolerance, serum potassium, and renal function.
Monitoring is Critical: Regular monitoring of serum potassium and renal function is essential, especially during dose adjustments.
Avoid Rapid Titration: To minimize the risk of hyperkalemia and renal impairment, dose adjustments should be made no more frequently than every 4 weeks.
Titration Schedule for Spironolactone Initial Dose
12.5 mg to 25 mg once daily depending on baseline renal function and potassium levels.
Titration and Target Dose
After 4 weeks: If well tolerated and potassium < 5.0 mmol/L:
Increase to 25 mg once daily (if started at 12.5 mg). Increase to 50 mg once daily (if started at 25 mg).
Maximum Target Dose: 50 mg once daily.
Special Considerations
In elderly patients or those with borderline renal function, consider maintaining at 25 mg once daily to minimize the risk of hyperkalemia.
If hyperkalemia (K+ 5.0-5.5 mmol/L) occurs:
Reduce the dose or increase monitoring frequency.
If K+ > 5.5 mmol/L, withhold the dose and re-evaluate.
Titration Schedule for Eplerenone Initial Dose
25 mg once daily.
Titration and Target Dose
After 4 weeks: If well tolerated and potassium < 5.0 mmol/L:
Increase to 50 mg once daily.
Maximum Target Dose: 50 mg once daily.
Special Considerations
Eplerenone is preferred in patients at risk of hormonal side effects (e.g., gynecomastia).
More selective than Spironolactone, but similar monitoring is required for potassium and renal function.[52]
Key Clinical Trials
1. RALES (Randomized Aldactone Evaluation Study) MRA Studied: Spironolactone
Population:
1,663 patients with severe chronic HFrEF (NYHA Class III-IV, LVEF ≤ 35%).
Study Design:
Randomized, placebo-controlled, double-blind.
Key Findings:
30% reduction in all-cause mortality (35% vs. 46% in placebo). 35% reduction in heart failure hospitalizations.
Conclusion:
Spironolactone improves survival and reduces hospitalizations in severe chronic HFrEF.
2. EPHESUS (Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study)
MRA Studied: Eplerenone
Population:
6,632 patients with acute MI and LV dysfunction (LVEF ≤ 40%) with heart failure symptoms.
Study Design:
Randomized, placebo-controlled, double-blind.
Key Findings:
15% reduction in all-cause mortality (14.4% vs. 16.7% in placebo). 13% reduction in sudden cardiac death.
Conclusion:
Eplerenone reduces mortality and sudden cardiac death post-MI in patients with LV dysfunction and heart failure symptoms.
3. EMPHASIS-HF (Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure) MRA Studied: Eplerenone
Population: 2,737 patients with mild chronic HFrEF (NYHA Class II, LVEF ≤ 35%).
Study Design:
Randomized, placebo-controlled, double-blind.
Key Findings:
37% reduction in cardiovascular death or heart failure hospitalization. 24% reduction in all-cause mortality.
Conclusion: Eplerenone is beneficial even in mild HFrEF, reducing mortality and hospitalizations.
4. EMPHASIS-HF (Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure) MRA Studied: Eplerenone
Population:
2,737 patients with mild chronic HFrEF (NYHA Class II, LVEF ≤ 35%).
Study Design:
Randomized, placebo-controlled, double-blind.
Key Findings:
37% reduction in cardiovascular death or heart failure hospitalization. 24% reduction in all-cause mortality.
Conclusion:
Eplerenone is beneficial even in mild HFrEF, reducing mortality and hospitalizations.
Practical Considerations in ADHF
Continue MRAs if the patient is stable and without significant hyperkalemia or worsening renal function.
Initiate MRAs in hospitalized ADHF patients if:
They have chronic HFrEF (LVEF ≤ 35%). Potassium is < 5.0 mmol/L and eGFR > 30 mL/min. Hemodynamically stable (SBP > 90 mmHg, no cardiogenic shock).
Avoid or Temporarily Discontinue MRAs if:
Hyperkalemia (K+ > 5.0 mmol/L).
Acute kidney injury or worsening renal function. Hypotension or hemodynamic instability.
Adverse Effects and Management
1. Hyperkalemia Mechanism:
Reduced potassium excretion due to aldosterone blockade.
Increased risk with concomitant ACE inhibitors, ARBs, or renal dysfunction.
Monitoring:
Serum Potassium and Renal Function:
Baseline: Check before initiation.
Follow-up: 3 days, 1 week, and monthly for the first 3 months, then every 3-6 months.
Management:
Mild Elevation (K+ 5.0 - 5.5 mmol/L): Reduce dose or increase monitoring frequency.
Moderate to Severe (K+ > 5.5 mmol/L): Withhold MRA and consider potassium binders if necessary. Avoid Potassium Supplements and reduce dietary potassium intake.
2. Worsening Renal Function Mechanism:
Decreased effective circulating volume can reduce glomerular filtration rate (GFR).
Monitoring:
Serum Creatinine and eGFR:
Monitor along with potassium levels at similar intervals.
Management:
Mild Deterioration (eGFR > 30 mL/min): Monitor closely and adjust diuretics to maintain euvolemia. Moderate to Severe (eGFR < 30 mL/min): Consider dose reduction or temporary discontinuation.
3. Gynecomastia and Hormonal Effects (specific to Spironolactone) Mechanism: Anti-androgenic effects leading to gynecomastia, impotence, or menstrual irregularities. Management:
Switch to Eplerenone, which is more selective and has fewer hormonal side effects.
F. SGLT-2 Inhibitors in Acute Decompensated Heart Failure (ADHF)
Sodium-glucose co-transporter-2 inhibitors (SGLT-2i) were initially developed for glycemic control in type 2 diabetes but have demonstrated substantial cardiovascular and renal benefits. Their role in heart failure, including Acute Decompensated Heart Failure (ADHF), is increasingly recognized, influencing current heart failure management guidelines.[53]
Mechanism of Action in ADHF
SGLT-2 inhibitors work through multiple mechanisms that benefit patients with heart failure:
a. Osmotic Diuresis and Natriuresis
Osmotic Diuresis: Inhibiting SGLT-2 in the proximal renal tubules increases urinary glucose excretion, leading to water loss. This reduces plasma volume and decreases preload.
Natriuresis: Increased sodium excretion helps reduce extracellular fluid volume, alleviating congestion without significant activation of the renin-angiotensin-aldosterone system (RAAS).
Preservation of Intravascular Volume: Unlike loop diuretics, SGLT-2i maintain intravascular volume, reducing the risk of hypotension and worsening renal function.
b. Cardio-Renal Benefits
Reduced Cardiac Preload and Afterload: By decreasing plasma volume and arterial stiffness. Improved Renal Hemodynamics: Enhances renal perfusion and reduces glomerular hyperfiltration, protecting against acute kidney injury.
Reduction in Albuminuria: Protects against diabetic nephropathy progression.
c. Metabolic Effects
Enhanced Cardiac Energy Efficiency: Increases ketone body production, which serves as an efficient energy substrate for the failing myocardium.
Reduction in Inflammation and Oxidative Stress: Improves endothelial function and reduces cardiac fibrosis.
d. Direct Myocardial Effects
Inhibition of Sodium-Hydrogen Exchanger (NHE-1): Decreases intracellular sodium and calcium overload, reducing myocardial stiffness and arrhythmogenic potential.
Improved Ventricular Remodeling: Reduces left ventricular mass and improves diastolic function.
Indications and Usage in ADHF
Heart Failure with Reduced Ejection Fraction (HFrEF): Strong evidence supports SGLT-2i use in HFrEF to reduce cardiovascular death and heart failure hospitalization.
Heart Failure with Preserved Ejection Fraction (HFpEF): Recent trials demonstrate benefits in reducing heart failure hospitalization in HFpEF patients.
Type 2 Diabetes with Heart Failure: Effective in reducing cardiovascular events and protecting renal function.
Initiation in ADHF: Safe to initiate in stabilized ADHF patients once they are euvolemic and hemodynamically stable.
Key Clinical Trials
a. DAPA-HF Trial Drug: Dapagliflozin
Population: HFrEF (NYHA class II-IV) with or without diabetes.
Findings:
26% reduction in cardiovascular death or worsening heart failure. 30% reduction in heart failure hospitalizations.
Improved symptoms and quality of life.
Conclusion: Dapagliflozin is beneficial across a broad spectrum of HFrEF patients, irrespective of diabetes status.
b. EMPEROR-Reduced Trial Drug: Empagliflozin Population: HFrEF (NYHA class II-IV) with or without diabetes. Findings:
25% reduction in the combined risk of cardiovascular death and heart failure hospitalization. Slowed progression of renal disease.
Conclusion: Confirms the class effect of SGLT-2i in reducing heart failure events and preserving renal function in HFrEF.
c. EMPEROR-Preserved Trial Drug: Empagliflozin
Population: HFpEF (LVEF > 40%) with or without diabetes.
Findings:
21% reduction in heart failure hospitalization.
Consistent benefit across different EF ranges, including borderline and mildly reduced EF. Conclusion: First trial showing significant benefit in HFpEF, establishing a new therapeutic option for this population.
d. SOLOIST-WHF Trial
Drug: Sotagliflozin (Dual SGLT-1 and SGLT-2 inhibitor)
Population: Patients recently hospitalized for worsening heart failure with diabetes.
Findings:
33% reduction in cardiovascular death and hospitalizations.
Early initiation (within 3 days of discharge) showed significant benefits.
Conclusion: Supports early initiation of SGLT-2i in ADHF to prevent rehospitalization.[54]
Initiation and Titration in ADHF
Timing
During Hospitalization: Initiate once euvolemic and hemodynamically stable (no inotropes or IV diuretics).[55]
Post-Discharge: Safe to start shortly after discharge to reduce readmission risk.
Dosage
Dapagliflozin: 10 mg once daily.
Empagliflozin: 10 mg once daily.
Sotagliflozin: Start at 200 mg once daily, titrate to 400 mg if tolerated.
Monitoring
Renal Function: eGFR before initiation and periodically thereafter.
Electrolytes: Monitor sodium and potassium levels.
Volume Status: Watch for dehydration, especially in combination with loop diuretics.
Blood Pressure: Monitor for hypotension.
Drug Interactions and Contraindications
Caution with Diuretics: Risk of volume depletion and hypotension. Avoid in Type 1 Diabetes: Due to the increased risk of ketoacidosis. Renal Impairment: Avoid initiation if eGFR < 20-30 mL/min/1.73 m².
Practical Considerations
No Need for Dose Titration: Fixed dosing (10 mg once daily) simplifies initiation.
Combination Therapy: Compatible with ACE inhibitors, ARBs, ARNis, beta-blockers, MRAs, and diuretics.
Patient Education: Inform about signs of dehydration, genital infections, and DKA symptoms.
SIDE EFFECTS
Common Side Effects
a. Genitourinary Infections
Increased risk of urinary tract infections (UTIs) and genital mycotic infections (e.g., vulvovaginal candidiasis and balanitis) due to glycosuria.
Incidence: More common in women and uncircumcised men.
Prevention/Management: Good genital hygiene and prompt antifungal or antibiotic treatment if symptoms occur.
b. Volume Depletion and Hypotension
Mechanism: Osmotic diuresis and natriuresis can lead to volume depletion.
Symptoms: Dizziness, orthostatic hypotension, fatigue.
Risk Factors: Elderly, patients on high-dose diuretics, RAAS inhibitors, or with low systolic blood pressure (< 100 mmHg).
Management: Monitor blood pressure, adjust diuretics or antihypertensives as needed, and encourage adequate hydration.
c. Electrolyte Imbalances Hyponatremia: Due to osmotic diuresis.
Hyperkalemia: Rare but possible in patients with renal impairment or those on potassium-sparing diuretics.
Monitoring: Regular monitoring of serum electrolytes, especially in patients with impaired renal function.
d. Acute Kidney Injury (AKI)
Transient decrease in eGFR due to volume contraction, particularly in patients with pre-existing renal impairment or those on diuretics and RAAS inhibitors.
Management:
Monitor renal function before and after initiation.
Hold SGLT-2i temporarily if significant volume depletion or AKI occurs. Typically reversible with volume repletion.
e. Hypoglycemia
Occurrence: Rare in non-diabetics but possible in patients with diabetes on insulin or sulfonylureas.
Prevention: Adjust doses of insulin or sulfonylureas when initiating SGLT-2i.
Serious but Rare Side Effects
a. Euglycemic Diabetic Ketoacidosis (euDKA)
DKA with normal or mildly elevated blood glucose levels (< 250 mg/dL).
Mechanism: Increased glucagon levels and reduced insulin requirements lead to ketogenesis.
Risk Factors:
Low carbohydrate intake, prolonged fasting, excessive alcohol consumption. Acute illness, major surgery, or insulin dose reduction.
Type 1 diabetes (contraindicated).
Symptoms: Nausea, vomiting, abdominal pain, dyspnea, and fatigue.
Management:
Discontinue SGLT-2i and initiate insulin and fluids. Monitor blood ketones in at-risk patients. Educate patients on recognizing symptoms and avoiding fasting or very low-carb diets.
b. Fournier’s Gangrene
Rare but life-threatening necrotizing fasciitis of the perineum.
Incidence: Extremely rare, but a higher incidence has been reported in patients on SGLT-2i.
Symptoms: Severe pain, erythema, swelling in the genital or perineal area, fever, and malaise.
Management: Urgent surgical intervention and broad-spectrum antibiotics.
Prevention: Educate patients on genital hygiene and early recognition of symptoms.
c. Bone Fractures and Reduced Bone Density
Mechanism: Possibly related to volume depletion, hypotension, and increased fall risk.
Evidence: Conflicting data; more commonly reported with canagliflozin.
Management: Ensure adequate calcium and vitamin D intake and assess fall risk in elderly patients.
d. Hypersensitivity Reactions
Rare reports of angioedema, urticaria, and anaphylaxis.
Management: Discontinue the drug and provide appropriate supportive care.
G. IVABRADINE
Ivabradine is a unique heart rate-lowering agent that selectively inhibits the If current in the sinoatrial node. Unlike beta-blockers or calcium channel blockers, it reduces heart rate without affecting myocardial contractility, blood pressure, or intracardiac conduction.[56] This makes it particularly useful in patients with heart failure who are intolerant to beta-blockers or have persistent tachycardia despite optimal medical therapy.
Mechanism of Action
Selective If Channel Blockade: Ivabradine specifically inhibits the funny (If) current responsible for spontaneous depolarization in the sinoatrial node, leading to a reduction in heart rate.
No Negative Inotropy: Unlike beta-blockers, ivabradine does not affect myocardial contractility or relaxation, preserving cardiac output.
Coronary Perfusion Improvement: By slowing heart rate, ivabradine increases diastolic filling time, enhancing coronary perfusion and reducing myocardial ischemia, particularly beneficial in patients with ischemic heart disease.
Reduction in Myocardial Oxygen Demand:
The decreased heart rate reduces oxygen consumption, which can be advantageous in preventing ischemia-induced worsening of heart failure.
Indications and Role in ADHF
Primary Indication: Chronic Heart Failure with Reduced Ejection Fraction (HFrEF) in patients: With sinus rhythm and resting heart rate ≥ 70 bpm.
On maximally tolerated beta-blockers or who are intolerant to beta-blockers.
Emerging Role in ADHF:
For patients with ADHF and persistent sinus tachycardia despite beta-blocker therapy. For those intolerant to beta-blockers due to hypotension or bronchospasm.
As an adjunct to standard therapy (e.g., diuretics, vasodilators, inotropes) to optimize heart rate and improve hemodynamics.
Hemodynamic Effects in ADHF
Heart Rate Reduction: Reduces heart rate without reducing blood pressure, making it suitable for patients with low BP.
Increased Stroke Volume and Cardiac Output: By prolonging diastolic filling time, ivabradine enhances stroke volume and overall cardiac output.
Reduced Ventricular Workload: Decreased heart rate lowers myocardial oxygen demand and reduces the risk of ischemia in patients with coronary artery disease.
No Negative Inotropic Effect: Unlike beta-blockers, it does not reduce myocardial contractility, preserving systolic function.[57]
Titration stratergy
General Principles of Titration
Start Low and Go Slow: Begin with a low dose and titrate gradually to minimize the risk of bradycardia and other adverse effects.
Individualized Dosing: Adjust based on heart rate response, clinical symptoms, and tolerability.
Target Heart Rate: Aim for a resting heart rate of 50-60 bpm to optimize cardiac output while reducing myocardial oxygen demand.
Monitoring: Regularly monitor heart rate, blood pressure, and ECG, particularly after dose adjustments.
Initial Dosing and Titration Schedule
Starting Dose:
5 mg twice daily with meals for most patients.
2.5 mg twice daily for:
Elderly patients (≥ 75 years).
Those with moderate hepatic impairment.
Patients with borderline low baseline heart rates (e.g., 60-70 bpm).
Dose Adjustment:
Reassess after 2 weeks to evaluate heart rate response and tolerability. If resting heart rate > 60 bpm: Increase
by 2.5 mg twice daily.
If resting heart rate 50-60 bpm: Maintain the current dose.
If resting heart rate < 50 bpm or bradycardia symptoms (e.g., dizziness, fatigue): Reduce the dose by 2.5 mg twice daily or discontinue if already on the lowest dose.
Maximum Dose:
7.5 mg twice daily for patients who tolerate lower doses without bradycardia or other adverse effects.
Special Considerations
In Elderly Patients (≥ 75 years): Start with 2.5 mg twice daily due to increased sensitivity to heart rate reduction.[58]
Hepatic Impairment:
Mild to Moderate: No dose adjustment needed, but start low and titrate cautiously.
Severe Hepatic Impairment: Contraindicated.
Renal Impairment: No specific dose adjustment required, but monitor closely in severe renal dysfunction (eGFR < 15 mL/min).
Monitoring Parameters
Heart Rate and Blood Pressure: Before initiation, after dose adjustments, and periodically thereafter. ECG Monitoring: To detect bradycardia, QT prolongation, or new-onset atrial fibrillation.
Symptom Assessment: Monitor for signs of bradycardia (e.g., dizziness, fatigue, syncope).
Visual Disturbances: Ask about transient luminous phenomena (phosphenes).
Combination with Other Medications
Beta-Blockers: Ivabradine can be used in combination with beta-blockers if the target heart rate is not achieved, but caution is needed to avoid excessive bradycardia.
Diuretics and Vasodilators: Safe to use together; monitor for hypotension.
Avoid Concomitant Use With:
Potent CYP3A4 inhibitors (e.g., ketoconazole, clarithromycin).
Negative chronotropes (e.g., diltiazem, verapamil) due to increased risk of bradycardia.
Key Clinical Trials
1. SHIFT Trial (2010)
Objective: Evaluated ivabradine’s impact on cardiovascular outcomes in chronic HFrEF.
Study Design: Randomized, double-blind, placebo-controlled trial involving 6,558 patients with HFrEF and heart rate ≥ 70 bpm.
Results:
Reduced hospitalizations for worsening heart failure by 26%. Decreased cardiovascular mortality by 18%. Relevance to ADHF: Patients with recent exacerbations benefited significantly, suggesting potential in acute settings.
2. ETHIC-AHF Trial (2022)
Objective: Assessed the efficacy and safety of ivabradine in hospitalized ADHF patients.
Study Design: Multicenter, randomized controlled trial involving 201 patients with ADHF and sinus tachycardia (≥ 70 bpm).
Results:
Rapid heart rate reduction within 48 hours.
Improved hemodynamics (cardiac index and stroke volume). Enhanced symptom relief (reduced dyspnea and fatigue).
No significant adverse effects or increased risk of hypotension.
Conclusion: Ivabradine is effective and safe for early heart rate control in ADHF
1. ADHF-IVAB Trial (Ongoing)
Objective: Investigating ivabradine’s impact on short-term outcomes in ADHF.
Primary Endpoint: Heart rate reduction and improvement in cardiac index.
Secondary Endpoints: Hospital readmissions, all-cause mortality, and adverse effects. Preliminary Findings: Indicate favorable hemodynamic responses and reduced ICU stay duration. Side effects
Common Side Effects
a. Bradycardia (3-10%)
Excessive heart rate reduction, potentially leading to dizziness, fatigue, hypotension, or syncope.
Risk Factors: Higher doses, low baseline heart rate, concomitant beta-blocker use.
Management: Dose reduction or temporary discontinuation if heart rate < 50 bpm or symptomatic.
b. Visual Disturbances (Phosphenes) (1-5%)
Brief, enhanced brightness in vision, typically triggered by sudden light changes. Due to If inhibition in retinal photoreceptors.
Onset and Duration: Often occurs within the first 2 months and usually resolves with continued therapy or dose adjustment.
Management: Inform patients of the benign nature; dose adjustment rarely needed.
a. Headache (2-5%)
Mild to moderate headaches, typically transient.
Management: Supportive care with analgesics if necessary.
b. Dizziness and Fatigue (1-3%)
Due to bradycardia or hypotension.
Management: Monitor blood pressure and heart rate; dose adjustment if symptomatic.
Less Common Side Effects
a. Atrial Fibrillation (1-4%)
Increased risk of new-onset atrial fibrillation, possibly due to slowed sinus rhythm and enhanced ectopic activity.
Monitoring: Regular ECG monitoring is recommended, especially in patients with a history of atrial fibrillation.
Management: Discontinue ivabradine if atrial fibrillation occurs.
b. Hypotension (<1%)
Rare but may occur in patients on multiple antihypertensive agents.
Management: Monitor blood pressure regularly; adjust other antihypertensives if needed.
c. QT Prolongation (Rare)
No significant QT prolongation noted at therapeutic doses, but caution in patients with congenital long QT syndrome.
Management: Monitor ECG in high-risk patients.
Rare and Serious Adverse Effects
a. Severe Bradycardia and Heart Block
Rare cases of second-degree or third-degree AV block reported, particularly in patients with pre-existing conduction abnormalities.
Management: Discontinue ivabradine and provide appropriate cardiac monitoring and support.
b. Angioedema and Hypersensitivity Reactions (Very Rare)
Severe allergic reactions have been reported, although extremely rare.
Management: Immediate discontinuation and appropriate medical intervention.[59]
REVIEW OF LITERATURE
1. Selim r. Krim, Patrick T. Campbell, Sapna Desai, Stacy Mandras, Hamang Patel, element Eiswirth and Hector O. Ventura; Management of patients admitted with acute decompensated heart failure. circulation. Ochsner journalSeptember2015,15(3)284- 289; The article on the management of patients admitted with acute decompensated heart failure emphasizes the critical aspects of inpatient therapy. It underscores the importance of decongestion, symptom improvement, addressing precipitating events, and updating medical therapy for these patients. Furthermore, educating patients on lifestyle modifications such as salt and fluid restriction, weight monitoring, and exercise programs is highlighted as essential for long-term management. This comprehensive approach aims to improve patient outcomes and quality of life.
2. John R Teerlink, Khalid Alburikan, Marco Metra, and Jo E Rodgers, Acute decompensated heart failure update, CurrCardiolRev.2015feb;11(1):53-62.; This article provides a comprehensive review of the evaluation and management of acute decompensated heart failure (ADHF), a condition that is increasing in prevalence and is associated with substantial mortality and morbidity. The article discusses the clinical presentation, risk stratification, and decision to admit patients with ADHF. It also covers the general approach to treatment, including the optimization of volume status to relieve congestion. The article highlights the importance of identifying precipitating factors for ADHF and optimizing chronic oral therapies prior to discharge. The article also discusses recent trials and the use of intravenous diuretics, vasodilators, and inotropes in the management of ADHF. Overall, this article provides a valuable resource for clinicians seeking to improve their understanding and management of ADHF.
3. Susan M. Joseph, MD, Ari M. Cedars, MD, Gregory A. Ewald, MD, Edward M.Geltman,MD,andDouglasL.Mann,MD;.Acutedecompensatedheartfailure;TexHeart Inst J. 2009;36(6):510-520.This article provides a comprehensive review of the management of acute decompensated heart failure (ADHF), a condition that is increasingly prevalent in the United States. The authors offer a thorough overview of the definition, characteristics, and precipitants of ADHF, as well as the clinical classification and treatment options. One of the strengths of the article is its evidence-based approach, with numerous studies cited to support the authors' recommendations. The article is also well- organized and easy to follow, making it accessible to a wide range of readers. However, the article's length and technical language may deter some readers, and the discussion of novel therapies is, and the emerging role of ultra filtration and novel therapies such as vasopressin receptor antagonists and relaxin. Overall, this article is a useful resource for clinicians seeking to improve their understanding and management of ADHF.
4. G. Michael Felker, M.D., M.H.S., Kerry L. Lee, Ph.D., David A. Bull, M.D., MargaretM. Redfield, M.D., Lynne W. Stevenson, M.D., Steven R. Goldsmith, M.D., Martin M. LeWinter, M.D., Anita Deswal, M.D., M.P.H., Jean L. Rouleau, M.D. Givertz, M.D. and Christopher M. O'Connor, M.D., for the NHLBI Heart Failure Clinical Research Network; diuretic stratergies in patients with acute decompensated heart failure; New England journal of medicine .This article presents the results of the Diuretic Optimization Strategies Evaluation (DOSE) trial, a randomized, double-blind, controlled study that investigated diuretic strategies in patients with acute decompensated heart failure. The study found no significant differences in patient-reported symptoms or changes in renal function between patients receiving intravenous furosemide via bolus or continuous infusion, or
between those receiving low-dose or high-dose strategies. While high-dose furosemide was associated with greater relief of dyspnea and fluid loss, it also led to more frequent worsening of renal function, although this did not translate to worse clinical outcomes at 60days. Overall, the study suggests that diuretic strategies may not sign if it can impact short- term outcomes in patients with acute decompensated heart failure.
5. Joyce N. Njoroge and John R. Teerlink, MD, Section of cardiology111C, San Francisco Veterans Affairs Medical Center Cardiology,4150 Clement St, San Francisco, CA 94121; Pathophysiology and therapeutic approaches to acute decompensated heart failure; This article provides a comprehensive review of acute decompensated heart failure (ADHF), a leading admission diagnosis worldwide with high in-hospital morbidity and mortality, and frequent rehospitalizations. Despite the availability of agents for chronic heart failure management, there has been no new therapy approved for ADHF in decades. The article discusses the current limited understanding of ADHF pathophysiology, possible therapeutic targets, and current limitations in expanding available therapies in light of the unmet need among these high-risk patients. The review also highlights the importance of effective decongestion and cardiac function optimization, frequent reevaluation of clinical trajectory, comprehensive evaluation of comorbid contributions, and safe discharge preparation and follow-up in the management of patients with ADHF.
6. Sean M. Hickey, MD, Chad Meyers, MD; Acute decompensated heart failure;2019; This article provides a comprehensive overview of acute decompensated heart failure (ADHF), a condition affecting6.5 million Americans with a5-yearmortalityrateof50-55%. The authors discuss the pathophysiology, diagnosis, and management of ADHF, including the use of point- of-care ultrasound, biomarkers, and electrocardiogram. They also highlight controversies in management, such as the optimal timing of diuresis and the use of opiates. The article emphasizes the importance of prompt diagnosis and aggressive management to improve outcomes.
7. .Joyce N. Njoroge and John R. Teerlink, MD, Section of cardiology 111C, San Francisco Veterans Affairs Medical Center Cardiology,4150 Clement St, San Francisco, CA 94121; Pathophysiology and therapeutic approaches to acute decompensated heart failure; This article provides a comprehensive
review of acute decompensated heart failure (ADHF), a leading admission diagnosis worldwide with high in-hospital morbidity and mortality, and frequent rehospitalizations. Despite the availability of agents for chronic heart failure management, there has been no new therapy approved for ADHF in decades. The article discusses the current limited understanding of ADHF pathophysiology, possible therapeutic targets, and current limitations in expanding available therapies in light of the unmet need among these high-risk patients. The review also highlights the importance of effective decongestion and cardiac function optimization, frequent reevaluation of clinical trajectory, comprehensive evaluation of comorbid contributions, and safe discharge preparation and follow-up in the management of patients with ADHF.
8. Steffen HJ, Abel N, Lau F, Schmitt A, Reinhardt M, Akin M, Bertsch T, Rusnak J, Weidner K, Behnes M, Akin I, Schupp T. Timing of acute decompensated heart failure in patients with heart failure and mildly reduced ejection fraction. 2025 Jan 22.The article highlights that patients developing ADHF during hospitalization for other conditions face worse outcomes, including higher mortality and longer stays. This group often has complex medical histories and delayed heart failure management, as their primary admission diagnosis is unrelated to ADHF. The study emphasizes early recognition and intervention to improve prognosis. These findings stress the need for proactive heart failure care in all hospitalized patients.
9. Lala A, Hamo CE, Bozkurt B, Fiuzat M, Blumer V, Bukhoff D, Butler J, Costanzo MR, Felker GM, Filippatos G, Konstam MA, McMurray JJV, Mentz RJ, Metra M, Psotka MA, Solomon SD, Teerlink J, Abraham WT, O’Connor CM, HF-ARC (Heart Failure Collaboratory and Academic Research Consortium). Standardized Definitions for Evaluation of Acute Decompensated Heart Failure Therapies: HF-ARC Expert Panel Paper. J Am Coll Cardiol HF. 2024 Jan;12(1):1-15. The article provides standardized definitions and criteria for evaluating acute decompensated heart failure (ADHF), aiming to enhance consistency in diagnosis and treatment. It emphasizes the importance of uniform terminology to improve clinical decision-making and patient care.
10. Kyriakopoulos CP, Sideris K, Taleb I, Maneta E, Hamouche R, Tseliou E, Zhang C, Presson AP, Dranow E, Shah KS, Jones TL, Fang JC, Stehlik J, Selzman CH, Goodwin ML, Tonna JE, Hanff TC, Drakos SG. Clinical Characteristics and Outcomes of Patients Suffering Acute Decompensated Heart Failure Complicated by Cardiogenic Shock. Originally published 2024 Aug29. The article reviews the clinical features and outcomes of patients with cardiogenic shock due to acute decompensated heart failure (ADHF), noting they have lower in-hospital mortality rates compared to those with shock from acute myocardial infarction. It highlights the need for tailored management strategies, as traditional treatments for myocardial infarction may not be as effective for ADHF-related shock. The study emphasizes early identification and specialized care to improve outcomes, calling for more research to optimize treatment protocols for this unique patient population.
11. Greene SJ, Fonarow GC, DeVore AD, Sharma PP, Vaduganathan M, Albert NM, Duffy CI, Hill CL, McCague K, Patterson JH, Spertus JA, Thomas L, Williams FB, Hernandez AF, Butler J. Titration of medical therapy for heart failure with reduced ejection fraction. J Am Coll Cardiol. May 2019. The
article investigates the titration process for medications in heart failure patients with reduced ejection fraction (HFrEF), highlighting the need for careful dose adjustments of ACE inhibitors, beta-blockers, and mineralocorticoid receptor antagonists. It concludes that systematic up-titration is practical and can improve clinical outcomes when managed with close monitoring, emphasizing the importance of achieving optimal therapeutic doses.
12. .Cotter G, Deniau B, Davison B, Edwards C, Adamo M, Arrigo M, et al. Optimization of Evidence-Based Heart Failure Medications After an Acute Heart Failure Admission: A Secondary Analysis of the STRONG-HF Randomized Clinical Trial. JAMA Cardiol. 2024. The study found that patients who were prescribed a higher number of GDMT agents experienced lower rates of readmission and mortality within six months, along with improved quality of life. These findings underscore the critical need for healthcare providers to prioritize the initiation and titration of evidence- based therapies during hospitalization to enhance patient outcomes.Harrington J, Jones WS, Udell JA, Hannan K, Bhatt DL, Anker SD, et al. Acute
13. Decompensated Heart Failure in the Setting of Acute Coronary Syndrome: State-of-the-Art Review. J Am Coll Cardiol HF. 2022; The article highlights that acute decompensated heart failure (ADHF) is more common in patients with a history of heart failure who develop acute coronary syndrome (ACS). It reports that 11% to 13% of patients with newly diagnosed heart failure present with ACS-related heart failure. This underscores the importance of recognizing and managing ACS as a significant contributor to ADHF, especially in vulnerable patient populations.
AIM AND OBJECTIVES
AIM: To analyse the drug prescription patterns, titrations and adverse effects of patients with ADHF
OBJECTIVES
When analyzing drug prescription patterns, titrations, and adverse effects for inpatients admitted with acute decompensated heart failure (ADHF), the following objectives should guide the analysis:
I. ASSESS PRESCRIPTION PATTERNS:
• Identify Commonly Prescribed Medications: Determine which medications (e.g. diuretics, vasodilators, inotropes, beta-blockers, ACE inhibitors, ARBs, ARNIs, aldosterone antagonists) are frequently used.
• Evaluate Alignment with Guidelines: Examine whether these prescriptions adhere to clinical guidelines (e.g., ACC/AHA, ESC) for managing ADHF.
• Review Medication Combinations: Analyze common combinations of drugs and their appropriateness for different patient profiles.
• Analyze Titration Practices: Evaluate Initial Dosing: Review the initial dosages of medications and the rationale behind these decisions.
• Monitor Titration Strategies: Assess how and when medications are titrated, including increments, frequency, and goals.
• Identify Barriers to Titration: Explore any challenges encountered during titration, such as adverse effects or clinical instability.
II. DOCUMENT AND ANALYS ADVERSEEFFECTS:
• Record Adverse Effects: Track the frequency and types of adverse effects experienced by patients, such as hypotension, renal dysfunction, or electrolyte imbalances.
• Analyze Relationship to Medications: Investigate how specific medications and their dosages contribute to adverse effects.
• Identify Risk Factors: Examine patient-specific factors (e.g., age, comorbid conditions) that may increase the risk of adverse effects.
III. EVALUTE TREATMENT EFFICACY:
• Assess Clinical Outcomes: Review clinical outcomes, including symptom relief, hemodynamic improvements, and overall stabilization.
• Monitor Biomarkers: Analyze changes in biomarkers (e.g., BNP, NT-proBNP) to evaluate the effectiveness of treatment.
IV. IMPACTONHOSPITALIZATION:
• Analyze Length of Stay: Examine how different prescription and titration practices affect the length of hospital stay.
• Review Readmission Rates: Investigate whether certain prescribing patterns or titration strategies are associated with higher or lower rates of readmission.
v. EXAMINE DRUG-DRUG INTERACTIONS:
• Identify Potential Interactions: Assess potential interactions between prescribed drugs that may impact efficacy or safety.
• Evaluate Impact of Interactions: Determine how drug interactions affect patient outcomes and the incidence of adverse effects.
• Assess Patient Adherence and Education: Evaluate Adherence During Hospitalization: Monitor patient adherence to prescribed regimens and the effectiveness of any adherence strategies.
VI. DEVELOP RECOMMENDATIONS FOR PRACTICE IMPROVEMENT:
• Identify Gaps and Opportunities: Use the analysis to identify areas for improvement in drug prescription and titration practices.
• Formulate Evidence-Based Guidelines: Develop or refine clinical guidelines and or protocols based on findings to enhance patient care and outcomes.
METHODOLOGY
MATERIAL AND METHODS STUDYSITE:
• This study is conducted in the In-patient department of Cardiology , Krishna institute of medical sciences (KIMS) hospital, Secunderabad.
STUDY DESIGN:
• This study follows a prospective observational design.
STUDYPERIOD:
• This study is conducted for 6 months.
SAMPLESIZE:60 STUDYCRITERIA
Inclusion Criteria:
• Adults>18years-primarywithsignsandsymptomsof ADHF.
Exclusion Criteria:
• Subject not giving consent Pregnant and lactating women
• Pediatrics and young adults<18years.
Source of Data:
• All essential and relevant information will be obtained from inpatient department prescriptions, test results, and patient records.
• Engaging with medical staff.
STASTICAL ANALYSIS
• The study's objectives were achieved by presenting categorical data through frequencies and percentages, while continuous variables were expressed using standard deviation.
ETHICALCONSIDERATIONS
• Ethical committee approval was taken from Krishna institute of medical sciences (KIMS) hospital, Secunderabad. Consent has obtained with the agreement of the institutional ethical committee.
Proposed plan of work: -
• Data duplication and preparation of procedures.
• Seeking approval from the ethics committee.
• After obtaining informed consent, the study will enroll all patients who meet the inclusion criteria.
• Baseline information and data will be recorded during the initial visit for patients who satisfy the study's inclusion and exclusion criteria.
• Essential information will be collected from various sources, including patient demographics, medical history, prescription details, treatment duration, patient confidentiality, and other relevant comorbidities.
• To assess the patient's condition, medication details such as dosage, frequency of administration, and potential drug interactions will be documented.
• The collected data will be analyzed using appropriate statistical methods.
RESULTS AND DISCUSSION
Table no. 1- Frequency and percentage of subjects according to gender
|
Gender |
Frequency |
Percentage |
|
Female |
29 |
48.3 |
|
Male |
31 |
51.7 |
|
Total |
60 |
100 |
The table presents data on the gender distribution of patients with Acute Decompensated Heart Failure (ADHF). Among the total 60 patients, 29 were female, accounting for 48.3%, while 31 were male, representing 51.7%. This indicates a nearly equal distribution between genders, with a slightly higher prevalence of ADHF in males compared to females.
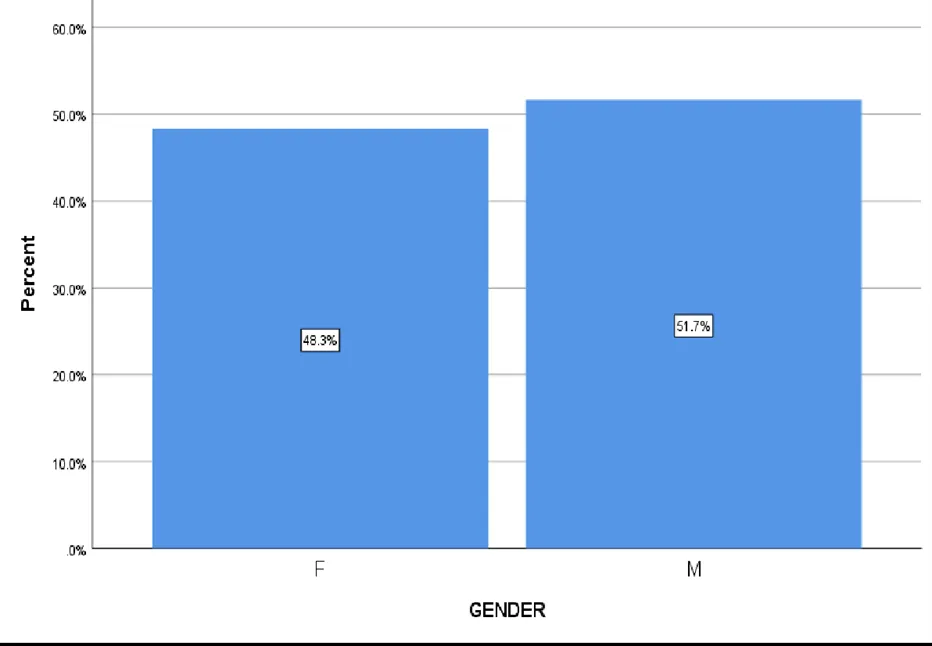
Figure no. 1- Bar diagram representing frequency and percentage of subjects according to gender
The gender distribution within the sample is nearly equal, with 29 females (48.3%) and 31 males (51.7%), indicating that both genders are affected by these clinical conditions in similar proportions.
Table no. 2: Mean and Standard deviation of the subjects according to Age, EF and Other laboratory parameters from minimum to maximum subjects
|
Descriptive Statistics |
||||
|
|
Minimum |
Maximum |
Mean |
Std. Deviation |
|
AGE |
34 |
92 |
66.00 |
12.899 |
|
NT-proBNP |
599 |
30000 |
8285.36 |
9598.803 |
|
TROP-T |
.010 |
4.080 |
.13991 |
.550261 |
|
CPK-MB |
1.10 |
35.94 |
6.4293 |
7.36290 |
|
CREATININE |
.62 |
6.21 |
1.4303 |
.82927 |
|
POTASSIUM |
3.2 |
5.40 |
4.252 |
0.593 |
|
EF |
18.00% |
55.00% |
35.7797% |
8.25471% |
The table provides descriptive statistics for key clinical parameters in patients with Acute Decompensated Heart Failure (ADHF). It summarizes the minimum, maximum, mean, and standard deviation for each variable, offering insights into their distribution.+
Age: The patients range from 34 to 92 years old, with an average age of 66 years. The standard deviation (12.899) suggests moderate variation in age.
NT-proBNP (N-terminal pro-B-type Natriuretic Peptide): Levels range from 599 to 30,000 pg/mL, with a high average of 8,285.36 pg/mL and a large standard deviation (9,598.803), indicating significant differences in heart failure severity among patients.
Troponin-T (TROP-T): Values span from 0.010 to 4.080 ng/mL, with a mean of 0.13991 ng/mL. The high standard deviation (0.550261) suggests that some patients have markedly elevated levels, potentially indicating myocardial injury.
CPK-MB (Creatine Phosphokinase-MB): Ranging from 1.10 to 35.94 ng/mL, this enzyme has an average of 6.4293 ng/mL and a standard deviation of 7.36290, reflecting variability in myocardial damage.
Creatinine: Levels vary between 0.62 and 6.21 mg/dL, with a mean of 1.4303 mg/dL and a standard deviation of 0.82927, suggesting differing degrees of kidney function impairment in these patients.
Potassium: The range is 3.2 to 5.40 mmol/L, with an average of 4.252 mmol/L and a standard deviation of 0.593, highlighting electrolyte imbalances that are common in heart failure.
Ejection Fraction (EF%): EF values span from 18.00% to 55.00%, with a mean of 35.7797% and a standard deviation of 8.25471%, indicating that most patients have reduced ejection fraction (HFrEF).
Table no.3: Frequency and Percentage of subjects according to past history
|
Past history |
Frequency |
Percentage |
|
DM |
39 |
65 |
|
HTN |
36 |
60 |
|
CABG |
6 |
10 |
|
CAD |
12 |
20 |
|
CKD |
8 |
13.3 |
|
Hypothyroidism |
3 |
5 |
|
Others |
14 |
23.3 |
|
Nil |
10 |
16.7 |
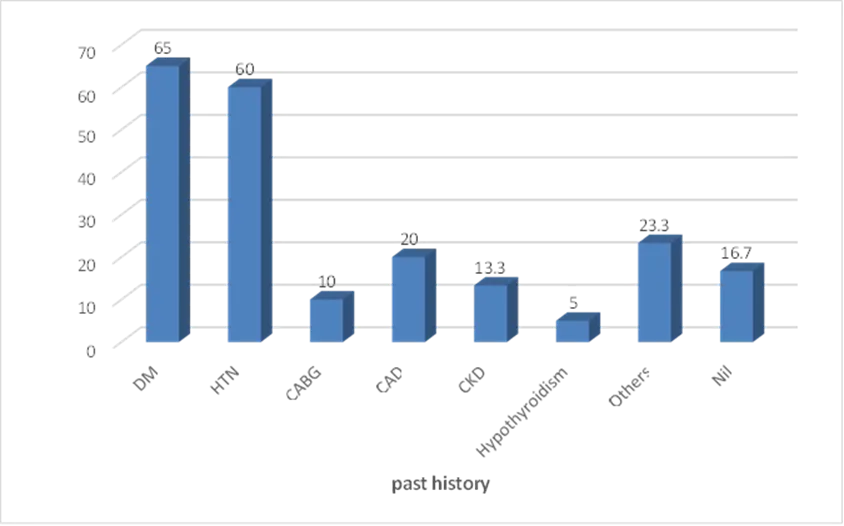
Figure no. 2: Bar diagram representing frequency and Percentage of subjects according to their past history
The bar chart illustrates the percentage distribution of various medical conditions in a given population. Diabetes Mellitus (DM) is the most prevalent condition, affecting 65% of individuals, followed closely by Hypertension (HTN) at 60%. Coronary Artery Disease (CAD) is reported in 20% of the population, while Chronic Kidney Disease (CKD) affects 13.3%. Coronary Artery Bypass Graft (CABG) is observed in 10% of cases, and Hypothyroidism has the lowest prevalence at 5%. Additionally, 23.3% of individuals reported having other medical conditions, and 16.7% had no reported medical history (Nil).
Table no. 4: Frequency and Percentage of subjects according to the diagnosis
|
Diagnosis |
Frequency |
|
Percentage |
|
ADHF |
39 |
|
65 |
|
ADHF FC II |
2 |
|
3.3 |
|
ADHF FC III |
6 |
|
10 |
|
ADHF FC IV |
12 |
|
20 |
|
ADHF intubated |
1 |
|
1.7 |
|
Total |
60 |
|
100 |

Figure no. 3: Bar diagram representing the frequency and Percentage of subjects according to the types of diagnosis
The bar chart illustrates the percentage distribution of Acute Decompensated Heart Failure (ADHF) cases. The majority (65%) are classified as ADHF, while 20% fall under ADHF FC IV, 10% under ADHF FC III, and 3.3% under ADHF FC II. Additionally, 1.7% of patients required intubation. This data highlights the varying severity of ADHF cases.
Table no. 5: Frequency and Percentage of subjects according to 2D echo report
|
2D ECHO |
Frequency |
Percentage |
|
Mild LV Dysfunction |
26 |
43.3 |
|
Moderate LV Dysfunction |
7 |
11.7 |
|
Severe LV Dysfunction |
27 |
45.0 |
|
Total |
60 |
100 |
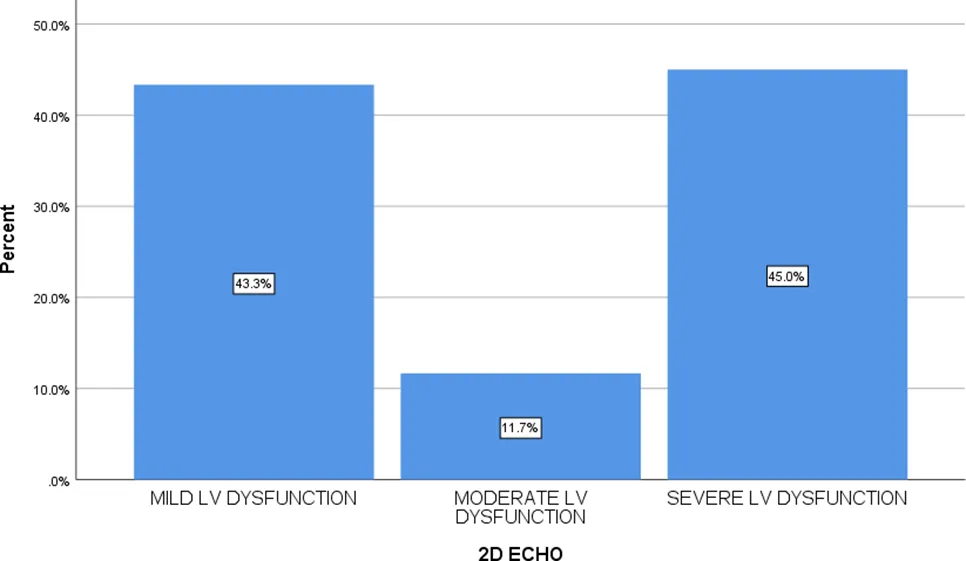
Figure no. 4: Bar diagram representing the Frequency and Percentage of subjects according to 2D echo report
The bar chart illustrates the distribution of LV dysfunction severity in ADHF patients based on 2D ECHO findings. Severe LV dysfunction is the most prevalent, affecting 45% of patients, followed closely by mild LV dysfunction at 43.3%, while moderate LV dysfunction accounts for 11.7%.
Table no. 6: Frequency and Percentage of subjects according to class of drugs prescribed
|
Class of Drug |
Frequency |
Percentage |
|
ARNI/ARB/ACEi |
15 |
25 |
|
Beta blockers |
41 |
68.3 |
|
MRA's |
26 |
43.3 |
|
SGLT-2I |
13 |
21.7 |
|
IVABRADINE/VERCIGUAT |
5 |
8.3 |
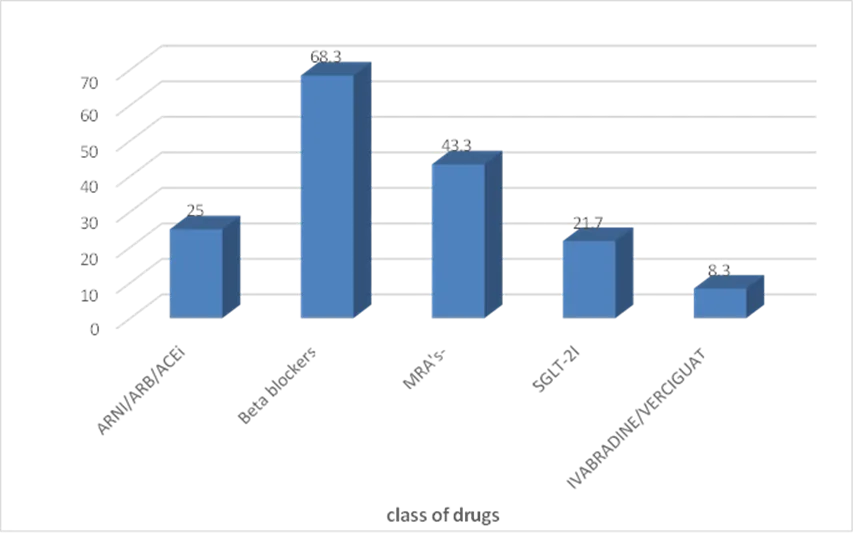
Figure no. 5: Bar diagram representing Frequency and Percentage of ADHF subjects according to class of drugs prescribed
The bar chart represents the percentage of patients receiving different classes of drugs for ADHF. Beta blockers were the most commonly prescribed (68.3%), followed by MRAs (43.3%) and ARNI/ARB/ACEi (25%). SGLT-2 inhibitors were used in 21.7% of cases, while Ivabradine/Vericiguat had the lowest utilization at 8.3%.
Table no. 7: Frequency and Percentage of ADHF subjects according to adverse events due to drugs
|
Drug |
No. of patients |
Frequency of adverse events |
Percentage of adverse events |
|
VALSARTAN |
2 |
1 |
50 |
|
Bisoprolol |
14 |
1 |
16.6 |
|
Carvedilol |
4 |
2 |
50 |
|
Metoprolol succinate |
22 |
6 |
27.3 |
|
Spironolactone |
13 |
1 |
7.7 |
|
Dapagliflozin |
26 |
2 |
7.7 |
|
Ivabradine |
2 |
2 |
100 |
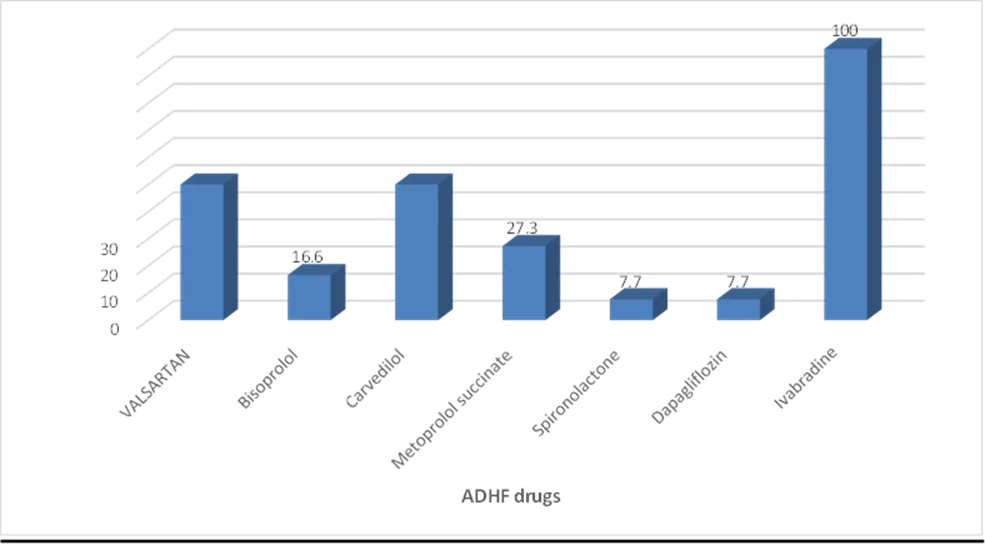
Figure no. 6: Bar diagram representing the Frequency and Percentage of ADHF subjects according to adverse events due to drugs
The bar chart illustrates the percentage of adverse events associated with various drugs used in Acute Decompensated Heart Failure (ADHF). Ivabradine had the highest adverse event rate (100%), followed by Carvedilol and Valsartan (both at 50%). Metoprolol Succinate showed a 27.3% incidence, while Bisoprolol (16.6%), Spironolactone (7.7%), and Dapagliflozin (7.7%) had lower event rates. This data highlights differences in drug tolerability among ADHF patients.
Table no. 8: Frequency and percentage of ADHF subjects according to different types of doses of drugs prescribed
|
Class of Drug |
Dose |
Frequency |
Percentage |
|
ARNI/ARB/ACEi Sacubitril/valsartan Sacubitril/valsartan Sacubitril/valsartan Ramipril Ramipril Valsartan |
25mg 24mg/26mg 50mg 1.25mg 10mg 40mg |
1 3 6 3 1 2 |
1.66 5 10 5 1.66 3.33 |
|
Beta-blockers Metoprolol succinate Metoprolol succinate Metoprolol succinate Metoprolol succinate Bisprolol Bisprolol Bisprolol Bisprolol Bisprolol Carvedilol Carvedilol Carvedilol |
12.5mg 25mg 50mg 150mg 1.25mg 2.5mg 5mg 7.5mg 25mg 3.125mg 5mg 6.25mg |
3 16 2 2 2 9 1 1 1 2 1 2 |
5 26.7 3.33 3.33 3.33 15 1.66 1.66 1.66 1.66 1.66 3.33 |
|
MRA's Spiranolactone Spiranolactone |
25mg 50mg |
10 3 |
10.67 5 |
|
SGLT-2I Dapagliflozin |
10mg |
26 |
43.3 |
|
IVABRADINE/VERCIGUAT IVABRADINE VERCIGUAT VERCIGUAT |
5mg 2.5mg 5mg |
2 2 1 |
3.33 3.33 1.66 |
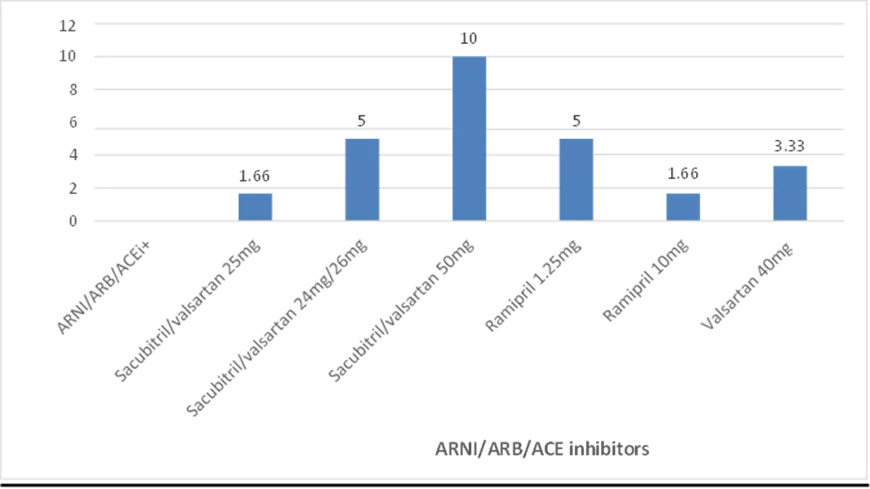
Figure no. 7 : Bar diagram representing the frequency and percentage of ADHF subjects according to different doses of ARNI/ARB/ACEi
The bar graph represents the frequency and percentage of different doses of drugs in same class used in the management of acute decompensated heart failure (ADHF). Among the ARNI/ARB/ACEi group, Sacubitril/Valsartan 50mg is the most frequently prescribed (10%), followed by Sacubitril/Valsartan 24mg/26mg (5%) and Ramipril 10mg (3.33%), while lower doses such as Sacubitril/Valsartan 25mg, Ramipril 1.25mg, and Valsartan 40mg have a lower prescription rate (1.66% each).
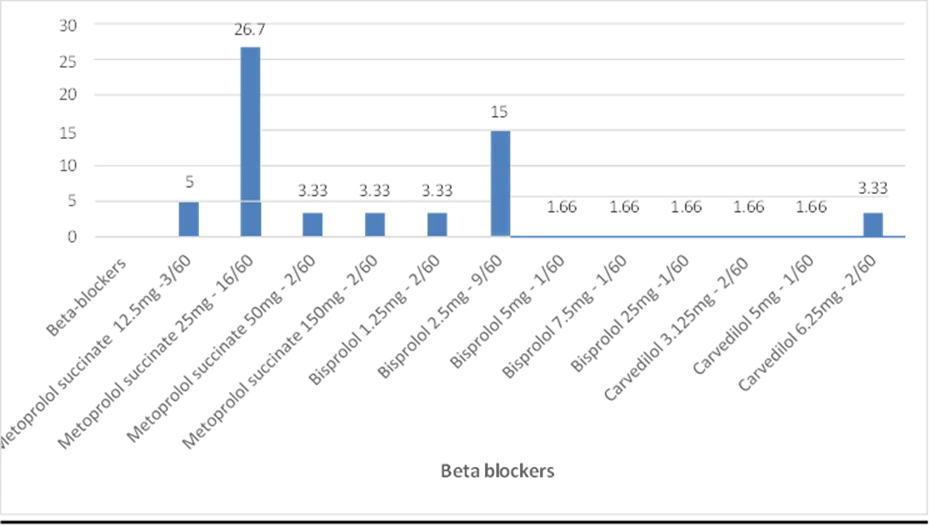
Figure no. 8: Bar diagram representing the frequency and percentage of ADHF subjects according to different doses of betablockers
The bar graph represents the frequency and percentage of different doses of betablockers in the management of acute decompensated heart failure (ADHF). Beta-blockers, which play a crucial role in managing heart failure, are most commonly represented by Metoprolol succinate 25mg (26.7%), followed by Bisoprolol 2.5mg (15%). Other frequently used beta-blockers include Metoprolol succinate 12.5mg (5%), Bisoprolol 1.25mg (3.33%), and Carvedilol 6.25mg (3.33%), while lower doses such as Bisoprolol 5mg, 7.5mg, and 25mg, as well as Carvedilol 3.125mg and 5mg, are prescribed to a smaller percentage (1.66% each).
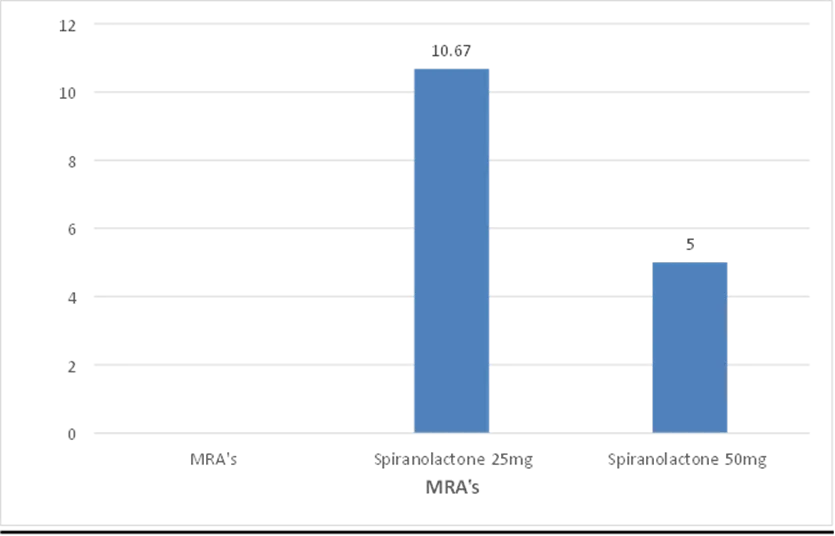
Figure no. 9: Bar diagram representing the frequency and percentage of ADHF subjects according to different types doses of MRA’S
The bar graph represents the frequency and percentage of different doses of mineralocorticoid receptor antagonist (MRA’s) used in the management of acute decompensated heart failure (ADHF). In the MRA (Mineralocorticoid Receptor Antagonists) class, Spironolactone 25mg is prescribed to 10.67% of patients, while Spironolactone 50mg is used less frequently (5%), likely reflecting its role in managing fluid retention.
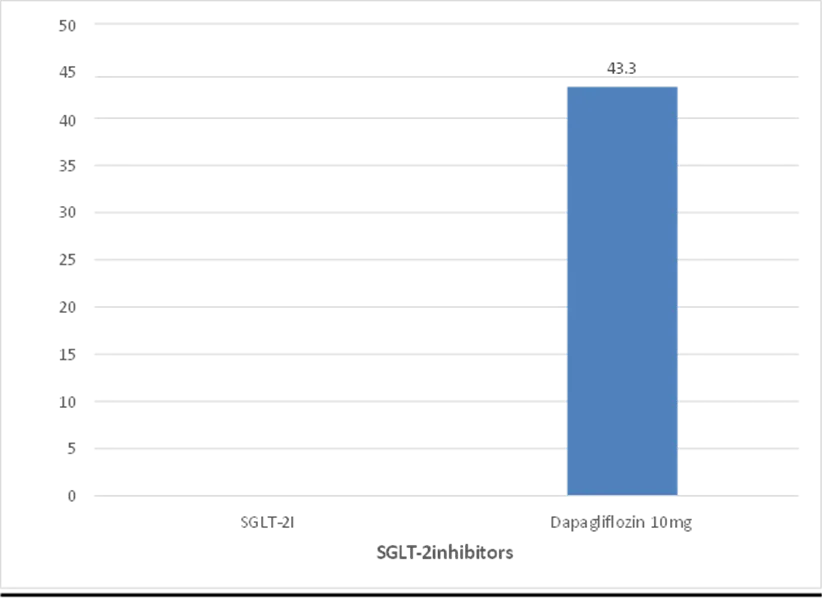
Figure no. 10: Bar diagram representing the frequency and percentage of ADHF subjects according to different doses of SGLT-2 inhibitors
The bar graph represents the frequency and percentage of different doses of SGLT-2 inhibitors used in the management of acute decompensated heart failure (ADHF). SGLT-2 inhibitors, which have gained prominence for their cardioprotective effects, are dominated by Dapagliflozin 10mg, prescribed to 43.3% of patients, making it the most commonly used drug in this dataset.
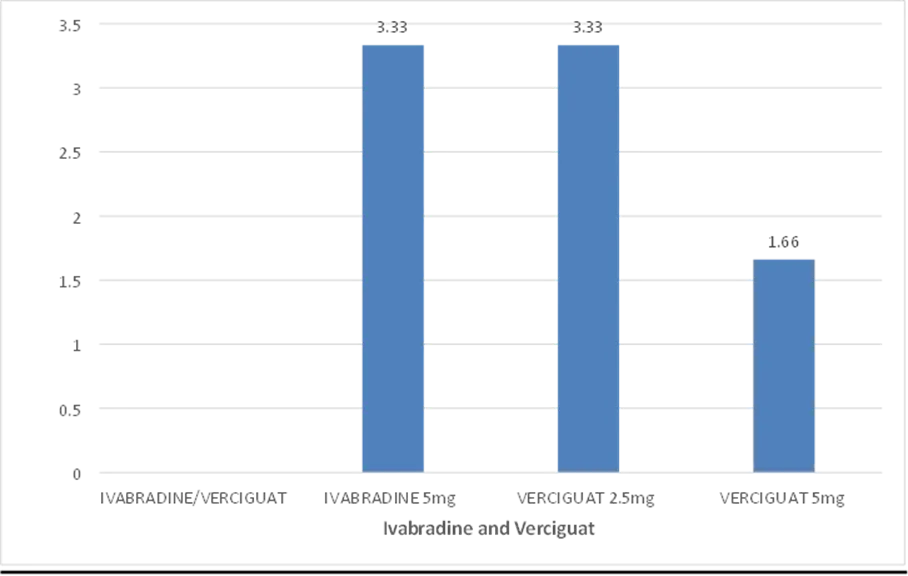
Figure no. 11: Bar diagram representing the frequency and percentage of ADHF subjects according to different doses of Ivabradine and Verciguat
The bar graph represents the frequency and percentage of different doses of Ivabradine and Verciguat used in the management of acute decompensated heart failure (ADHF). In the Ivabradine/Vericiguat category, Ivabradine 5mg and Vericiguat 2.5mg are prescribed to 3.33% of patients each, while Vericiguat 5mg is used in 1.66% of cases, suggesting their selective use in specific heart failure patients.
DISSCUSSION
The analyses of drug prescription patterns, titration strategies, and adverse effects in patients with Acute Decompensated Heart Failure (ADHF) offers valuable insights into real-world clinical management and challenges. The study population consists of 60 patients, with a nearly equal gender distribution (51.7% male, 48.3% female) and an average age of 66 years. The presence of multiple comorbidities is significant, with Diabetes Mellitus (65%) and Hypertension (60%) being the most common, followed by Coronary Artery Disease (20%) and Chronic Kidney Disease (13.3%). The varying severity of ADHF is evident, as 65% of cases fall under the general ADHF category, with a substantial 20% classified as ADHF FC IV, representing the most severe functional class. Additionally, severe left ventricular dysfunction (45%) is the predominant echocardiographic finding, indicating a high prevalence of heart failure with reduced ejection fraction (HFrEF).In terms of pharmacological management, beta-blockers (68.3%) are the most frequently prescribed drug class, underscoring their central role in heart failure treatment. Metoprolol succinate 25mg (26.7%) is the most commonly used dose, followed by Bisoprolol 2.5mg (15%), reflecting a preference for selective beta-blockers with a safer side-effect profile. Mineralocorticoid Receptor Antagonists (MRAs, 43.3%), such as Spironolactone 25mg (10.67%), are widely used for their role in reducing fluid retention and improving heart failure outcomes. ARNI/ARB/ACEi (25%) therapy is increasingly utilized, with Sacubitril/Valsartan 50mg (10%) as the most preferred option, highlighting its growing importance in HFrEF management. Notably, SGLT-2 inhibitors (21.7%) are gaining prominence, with Dapagliflozin 10mg (43.3%) being the most commonly prescribed in this class, demonstrating its cardioprotective benefits. Despite their established efficacy, Ivabradine and Vericiguat (8.3%) are used selectively, suggesting their role in specific patient subgroups where heart rate modulation or additional hemodynamic support is necessary.Titration strategies reflect a cautious and individualized approach, with intermediate doses being more commonly used to balance therapeutic benefits with potential side effects. This approach is particularly evident in ARNI/ARB/ACEi and beta-blocker prescriptions, where higher doses are avoided in some patients, likely due to concerns over hypotension, renal impairment, or worsening heart failure symptoms.An analysis of adverse drug reactions reveals significant differences in tolerability across various heart failure medications. Ivabradine (100%) had the highest adverse event rate, raising concerns about its side effects, such as bradycardia. Similarly, Carvedilol (50%) and Valsartan (50%) exhibited high incidence rates of adverse effects, suggesting the need for close monitoring, especially in patients prone to hypotension. In contrast, Metoprolol (27.3%) and Bisoprolol (16.6%) had moderate event rates, emphasizing the importanceof beta-blocker selection based on patient tolerance. On the other hand, Spironolactone and Dapagliflozin (7.7% each) demonstrated lower adverse event rates, reinforcing their generally favorable safety profiles in ADHF management.These findings emphasize the evolving role of SGLT-2 inhibitors and ARNI/ARB/ACEi as key components of modern ADHF treatment, complementing established therapies like beta-blockers and MRAs. However, the high incidence of adverse effects in certain drugs, such as Ivabradine, Carvedilol, and Valsartan, highlights the need for personalized treatment strategies, careful patient selection, and ongoing monitoring to optimize safety and efficacy.
Overall, the study underscores the complexity of ADHF management, where multiple factors—including disease severity, comorbidities, drug tolerability, and response to therapy—must be carefully considered. Future research should focus on refining dose optimization strategies, minimizing adverse effects, and assessing long-term clinical outcomes to further enhance treatment approaches for patients with ADHF.
CONCLUSION
By summarizing the statistical data of our study, we have observed that the drugs prescribed to subjects of ADHF shows difference in the management. Beta-blockers were the most commonly prescribed class (68.3%), with Metoprolol succinate 25mg being the most frequent dose. Slight titrations were observed, with some patients receiving lower doses such as Metoprolol succinate 12.5mg and Bisoprolol 1.25mg, reflecting cautious up-titration based on patient tolerance. MRAs were used in 43.3% of cases, with Spironolactone 25mg being the preferred dose, while a smaller proportion received 50mg, indicating a gradual titration approach.Among ARNI/ARB/ACEi therapy (25% of patients), Sacubitril/Valsartan 50mg was the most commonly prescribed, but lower doses such as Sacubitril/Valsartan 24/26mg and 25mg were also used, suggesting careful dose adjustments. SGLT-2 inhibitors, particularly Dapagliflozin 10mg, were administered to 21.7% of patients, with no significant titration trends. Ivabradine and Vericiguat were used selectively, with doses ranging from Ivabradine 5mg to Vericiguat 2.5mg and 5mg.Adverse event analysis showed Ivabradine had the highest incidence (100%), followed by Carvedilol and Valsartan (50% each). Metoprolol, Bisoprolol, Spironolactone, and Dapagliflozin had lower rates. The presence of slight titrations in beta-blockers, MRAs, and ARNI therapy highlights the importance of individualized treatment, gradual dose escalation, and monitoring for adverse effects to optimize outcomes in ADHF management.
REFERENCES
Open-Label Extension of the PIONEER-HF Trial. JAMA Cardiol. 2020 Jan 1;5(2):202-207.
E. Angiotensin–Neprilysin Inhibition in Acute Decompensated Heart Failure. N Engl J Med. 2019 Feb 7;380(6):539-548.
49. Mineralocorticoid Receptor Antagonists in Heart Failure: An Update. Circ Heart Fail. 2024;17(12):e011629.
Open-Label Extension of the PIONEER-HF Trial. JAMA Cardiol. 2020 Jan 1;5(2):202-207.
E. Angiotensin–Neprilysin Inhibition in Acute Decompensated Heart Failure. N Engl J Med. 2019 Feb 7;380(6):539-548.
49. Mineralocorticoid Receptor Antagonists in Heart Failure: An Update. Circ Heart Fail. 2024;17(12):e011629.


P. Twila Pushpa, Dr. S. Namratha, R. Glory Therissa, Amanganti Bharat, Accha Harshitha, Ayidalapally ChandraShekar, Drug Prescription Patterns, Titrations and Adverse Effects of In-Patients Admitted with Acute Decompensated Heart Failure, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, https://doi.org/10.5281/zenodo.21412202
 10.5281/zenodo.21412202
10.5281/zenodo.21412202