
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Samarth Educational Trust ., Arvind Gavali College Of Pharmacy Jaitapur, Satara-415004. Maharastra India.
Transdermal drug delivery was presented to overcome the difficulties of drug delivery especially oral route. Drug delivery through the skin a drug to achieve a systemic of drug is known as transdermal patches. Transdermal patches are widely used as cosmetic, topical, transdermal drug delivery system. Transdermal patch is medicated adhesive patch that is placed on the Skin to deliver a specific dose of medication through the skin and into the bloodstream. Topical administration of therapeutic agent’s offers many advantages over conventional oral and invasive methods of drug delivery. Several important advantages of transdermal drug delivery are limitation of hepatic first pass metabolism, enhancement of therapeutic efficiency and maintenance of steady plasma level of drug. The basic components of transdermal patch consists of polymer matrix\drug reservoir, active ingredient (Drug), permeation enhancer, pressure sensitive adhesive, backing laminates, release liner, other excipients like plasticizer and solvent. There are many methods of preparation of transdermal patches like circular Teflon mould method, assymetric tpx membrane method, mercury substrate methods, IPM membrane methods, EVAC membrane method, free film method. Cellulose derivative, zein, gelatin, polyvinyl alcohol, polyvinyl chloride, polyethylene, polypropylene this are the polymers used in the preparation of transdermal patches. Also, there are many evaluations parameter of transdermal patches like thickness, uniformity of weight, drug content determination, moisture content, moisture uptake, flatness, microscopic studies, adhesive studies, peel adhesion, tack properties, quick stick (peel tack method) test . This review article provides an overview of transdermal drug delivery system, its advantages over conventional dosage forms, drug delivery routes across human skin, permeation enhancer, and various preparation methods.
A transdermal patch or skin patch is a medicated adhesive patch that is placed on the skin to deliver a specific dose of medication through the skin and into the blood stream [1]. Transdermal drug delivery system has been in existence for a long time. In past commonly applied systems were topically applied creams and ointments for dermatologically disorders. The occurrence of systemic side effects with some of these formulations is indicative of absorption through the skin. A number of drugs have been applied to the skin for the systemic treatment.
Various types of patches along with various methods of applications have been discovered to deliver the drug from the transdermal patch.[2] Because of its great advantage, it has become one of the highly researched fields among the various drug delivery system. Here a general view over the transdermal patch has been discussed along with its advantages, disadvantages methods of applying, care taken while applying, types and applications of transdermal patch and recent advances and marketed product.[3][4].
Advantages:
• Hepatic first pass metabolism, salivary metabolism and intestinal metabolism are avoided.
• The ease of usage makes it possible for patients to self-administer these systems.
• In case of an emergency, removing the patch at any point of time during therapy can instantly stop drug input.
• Since the composition of skin structurally and biologically is the same in almost all the humans, there is minimal inter and intra patient variation.
• Drugs showing gastrointestinal irritation and absorption can be suitably administered through the skin.
• Continuous, non-invasive infusion can be achieved for drugs with short biological halflives, which would otherwise require frequent dosing.[23]
Disadvantages:
• There is possibility of skin irritation due to the one or many of the formulation components.
• Binding of drug to skin may result in dose dumping.
• Lag time is variable and can vary from several hours to days for different drug candidates.
• Cutaneous metabolism will affect therapeutic performance of the system
• Transdermal therapy is feasible for certain potent drugs only.
• Transdermal therapy is not feasible for ionic drugs.
• It cannot deliver drug in pulsatile fashion..[23]
Skin’s Anatomical Structure:
The skin is broadly divided into the stratum corneum (SC), epidermis, dermis, and hypodermis. The outermost SC consists of corneocytes embedded in a lipid matrix, forming a strong barrier that prevents moisture loss and protects against UV radiation and pathogens. Beneath it, the epidermis contains keratinocytes, Merkel cells, and Langerhans cells. The dermis, rich in capillaries, plays a key role in drug absorption by connecting to systemic circulation. The hypodermis is composed of adipose and loose connective tissue. Drugs penetrate the skin mainly through transepidermal and transappendageal routes. In the transepidermal pathway, drugs pass either through the intercellular lipid matrix or through corneocytes (transcellular route). The intercellular lipid matrix acts as the primary barrier, especially limiting the entry of large hydrophilic molecules. The transappendageal route involves passage through hair follicles and sebaceous glands, bypassing the lipid barrier, though it contributes minimally due to limited surface area. .[5][6][7]
Skin appendages cover only a small fraction of the skin surface and vary across individuals, making drug absorption unpredictable. To enhance drug permeation, various techniques are used. Chemical enhancers such as fatty acids, surfactants, and solvents improve drug solubility and penetration. Physical methods like heat, ultrasound, electrical fields, and micro needles increase skin permeability. Biological approaches, including peptides, also aid in improving transdermal drug delivery. [8][9]
Anatomical structure of Skin:
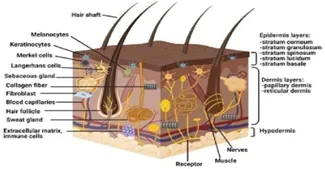
Fig No: 1
Epidermis layer: The thickness of epidermis,which is the skin’s outermost layer varies measuring around 0.8 mm on the palms of hands and the soles of feet. The viable epidermis is sometimes referred to as the epidermal layers underneath the stratum corneum and is composed of multi- layered areas of epithelial cells[10][11]. Approximately 95% of the cells of the epidermis are keratinocytes, melanocytes, Langerhans cells and merkel cells make up the remaining cells in the epidermal layers. The outermost layer of the epidermis is called the stratum corneum [12][13][14]. It has direct touch with the outside world and its extremely high density (1.4g/cm3) may contribute to some of its barrier qualities in the arid condition and its minimal 15%–20% hydration. The majority of the cells of the stratum corneum are made up of 20% lipid and 70% insoluble keratins. keratin in the corneocytes is linked to water in the stratum corneum..[15][16]
Dermis Layer: The dermis is a critical layer of the skin situated beneath the epidermis and plays a vital role in providing strength and flexibility. Typically measuring around 2-3 mm in thickness, the dermis is primarily composed of collagenous and elastin fibers which make up approximately70% of its structure. These fibers are essential for maintaining the skin’s resilience and elasticity, allowing it to withstand various forms of stress while remaining pliable.[17] This vascular network is crucial for sustaining the health of the skin facilitating not only nutrient delivery but also waste removal. Furthermore, the dermis houses lymphatic vessels, which play a significant role in immune function and fluid balance..[13]
Hypodermis layer:
The innermost layer of the skin known as the hypodermis or subcutaneous layer is made up of a network of fat cells. It serves as the layer of contact between the skin and the body’s deeper tissues including the bones and muscles. Thus, the primary roles of the hypodermis are defence from physical shock, heat insulation, skin conductivity and support for vascular and neurological signals. About half of the body’s fat is made up of cells that dwell in the hypodermis; the other main hypodermis cells are made up of macrophages and fibroblasts..[18][19]
Drug Penetration Pathways:
The fundamental prerequisite for the therapeutic response in the formulation used for transdermal medication delivery is drug permeability. The drug molecules involved in formulation must pass through multiple layers of the skin and eventually enter the systemic circulation to produce a therapeutic response It can reach systemic circulation in several ways.[20][21][22].
They are as follows:
A. Transepidermal Routes
• Intracellular (molecular intersection through the cells) routes
• Intercellular (molecular intersection between the cells) routes.
B. Trans-appendageal (shunt routes) routes [24][25][26][27].
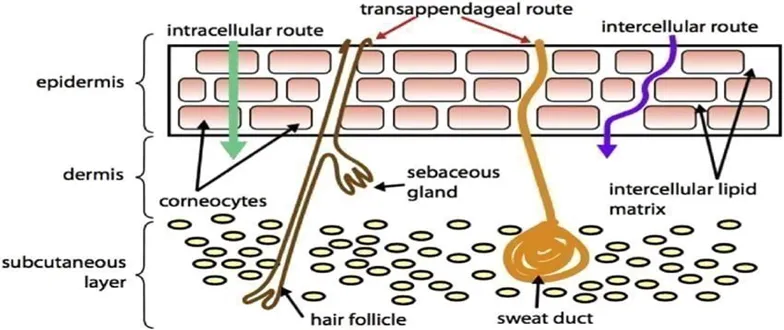
Fig No: 2
Aim:-Formulation and evaluation of transdermal patch containing Azadiracta indica and Allium sativum.
Objectives:- To design and formulate transdermal patches for controlled and sustained drug delivery through the skin.To select suitable polymers and excipients (film-forming agents, plasticizers, permeation enhancers, and backing membrane) for patch formulation.To optimize the composition and ratios of polymers and plasticizers for achieving uniformity, flexibility, and stability of the patch. To evaluate physicochemical compatibility of the drug with formulation excipients using techniques such as FTIR. To standardize the method of preparation (solvent evaporation, melting, or casting method) for reproducible patch characteristics
MATERIALS AND METHODS
Azadiracta indicaPowder and Allium sativum L. Powder
HPMC: Pharmaceutical grade E15 Thermo fisher scientific
Propylene glycol: IP grade Thermo fisher scientific
Gelatin: Pharmaceutical grade, Type B Thermo fisher scientific
Glycerin: IP grade Thermo fisher scientific
Ethanol: 95% v/v IP Thermo fisher scientific
2.1. Determination of calibration curve:
From the standard stock solution (1000 ug/ml), 10 ml solution was diluted to 100 ml using the solvent (100 ug/ml ). From this 0.2 ml, 0.4 ml, 0.6 ml, 0.8 ml, 1ml of solutions were taken into different volumetric flask and made upon 10 ml with solvent so as to get the concentration of 2 ug, 4 ug, 6 ug, 8 ug and 10 ug respectively. The absorbances of these solutions were measured at 243 nm.[33][37]
2.2. The process of making transdermal patch:
The solvent casting method is a common technique used to prepare transdermal patches by dissolving drug and excipients in a solvent and forming a thin film after evaporation. In this method, polymers such as Hydroxypropyl methylcellulose, Methyl cellulose, and Gelatin are dissolved in a suitable solvent like Ethanol. The drug (for example herbal extracts like neem or garlic) is added and mixed thoroughly to obtain a uniform solution. Plasticizers such as Glycerin are added to improve flexibility and prevent brittleness of the film. A permeation enhancer like Propylene glycol is incorporated to enhance drug penetration through the skin. The resulting mixture is stirred properly and allowed to stand or sonicated to remove air bubbles. The solution is then poured onto a flat surface such as a glass plate or petri dish and spread uniformly. The solvent is allowed to evaporate slowly at room temperature or under controlled conditions, forming a thin and uniform film. After complete drying, the film is carefully peeled off and cut into patches of required size. These patches are then evaluated for thickness, weight variation, drug content, folding endurance, and drug release. [38].
|
Batch |
Azadiracta indica |
Allium sativum |
HPMC |
MC |
Propylene glycol |
Gelatin |
Glycerin |
Ethanol |
|
F1 |
450mg |
250mg |
150mg |
50mg |
0.5ml |
5ml |
2ml |
10ml |
|
F2 |
450mg |
250mg |
200mg |
100mg |
0.5ml |
5ml |
2ml |
10ml |
|
F3 |
450mg |
250mg |
250mg |
150mg |
0.5ml |
5ml |
2ml |
10ml |
3. Evaluation of transdermal patches
3.1 Physical appearance:
Color, clarity, flexibility and smoothness were all visually assessed for all of the prepared patches.
3.2 Patch thickness:
A digital micrometer was used to measure the drug loaded patch's diameter at various points and the average width and variation were calculated to ensure the patch's thickness.[39][40][41]
3.3 Weight uniformity:
In order to assess weight variance, the individual weight of 10 randomly chosen patches were obtained, followed by the average weight. The individuals weight and the average weight shouldn't vary significantly.[42]
3.4 Flatness:
A transdermal patch needs to have a smooth surface and shouldn't shrink over time. The study of patch used to demonstrate this. To establish how flat a patch is three strip are cut from it two from each side and one from the middle. The length variance is calculated using the % constriction method after measuring the length of each strip. [44]
Flatness is equivalent to a limitation of 0%.
% Constriction = (L1 L2) / L1 × 100 L1 = Initial length of each strip
L2 =Final length of each strip.
3.5 Folding endurance:
Two by two centimeters of strip were cut, folded in the same place repeatedly and broken. The folding endurance number was derived by figuring out how many times a film could be twisted in the same direction before rupturing.[45]
3.6 Drug content determination:
It can be determined by completely dissolving patches of 2 by 2 cm in a solvent that is appropriate, stirring them for up to 24 hours, then placing them in a sonicator, filtering them and then conducting a spectroscopic investigation on the filtrate, it was possible to estimate how much drug was there.[43]
3.7 pH determination
About 1 g of each powder was weighed separately and mixed with 100 mL of distilled water to prepare a 1% w/v solution. The mixture was stirred and allowed to stand for 30–60 minutes to extract soluble components. It was then filtered to obtain a clear solution. The pH meter was calibrated using standard buffer solutions. The electrode was immersed in the filtrate and pH was recorded once stable readings were obtained. Measurements were taken in triplicate and the average value was noted.[46]
3.8 In vitro drug release :
The patch was placed and fixed between donor and receptor compartments. The receptor compartment was filled with phosphate buffer of pH 7.4 and maintained at 37˚C with continuous stirring. Since the herbal drug have low solubility, a small amount of ethanol was added to maintain proper drug release. At fixed time intervals, 5ml was taken and replaced with fresh buffer. The sample was analyzed using a UV spectrophotometer at 254 nm.
3.9 Determination of concentration for diffused drug(ug/ml) :
using calibration curve: Y = mX + c.
Where, Y= Absorbance, m= slope, X= conc. , c = intercept.
i. Cumulative amount of drug diffused (CADD) :
[Concentration (ug/mg) x Volume of diffusion medium x dilution factor]/1000
ii. Surface area (A) of onion membrane (cm2):
A=𝜋𝑟2
a. Cumulative amount of drug diffused per unit area (CADD):
CADD/cm2 = CADD/Area of membrane.
b. Percent cumulative drug released:
Amount of drug released x 100/ strength of patch
4. RESULT AND DISCUSSION
4.0 Preformulation Studies
4.1. Organoleptic evaluation:-
• Azadiracta indica:-
Color: Greenish to dull green (leaf powder) Odour: Strong pungent and bitter
Taste: Intensely bitter and astringent
Texture: Fine to coarse powder, slightly fibrous
• Allium sativum:-Color: Off-white to pale yellow
Odour: Strong, characteristic garlic aroma
Taste: Pungent, spicy and less sharp than fresh garlic Texture: Fine, dry, free-flowing powder
4.2.Melting point
Azadiracta indica was found to be between 158 to 162°C Allium sativum was found to be between 164 to 168°C.
4.3.Solubility
Azadiracta indica and Allium sativum are methanol and ethanol but in water and mild acids.
4.4.FTIR Spectroscopy
i. IR of Azadiracta indica-
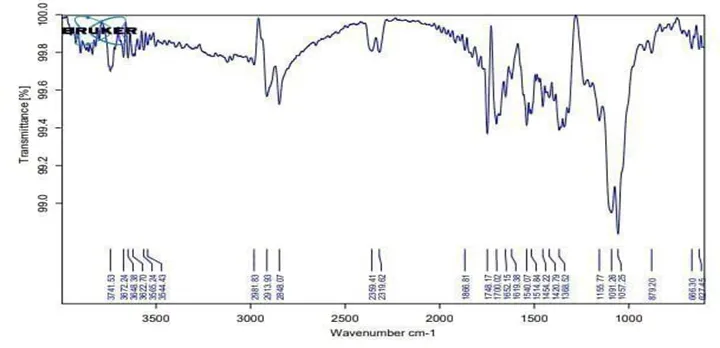
Fig no.3
The FTIR spectrum shows a broad peak in the range 3741–3544 cm⁻¹, indicating O–H stretching of alcohols or phenols. Peaks at 2981, 2913, and 2848 cm⁻¹ correspond to aliphatic C–H stretching.
Strong absorption at 1748 and 1700 cm⁻¹ suggests the presence of carbonyl (C=O) groups such as esters or ketones. The peak around 1652 cm⁻¹ indicates C=C stretching of alkenes or conjugated systems. Bands at 1596 and 1540 cm⁻¹ confirm aromatic ring structures. Peaks in the region 1514–1398 cm⁻¹ are due to C–H bending vibrations. The bands at 1155, 1091, and 1057 cm⁻¹ indicate C–O stretching of alcohols or ethers. Peaks at 879, 666, and 627 cm⁻¹ correspond to aromatic C–H bending. Overall, the spectrum confirms the presence of hydroxyl, carbonyl, and aromatic functional groups.
ii. IR of Allium sativum-
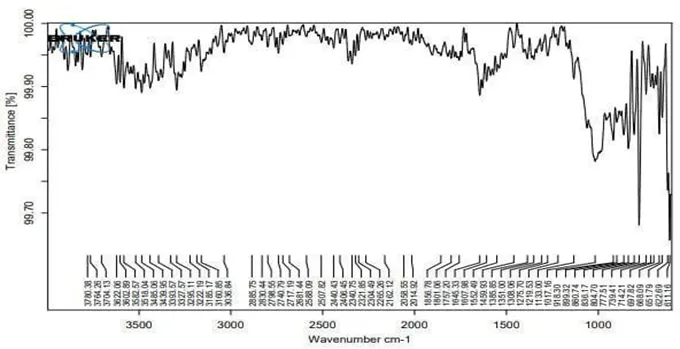
Fig.no: 4
The FTIR spectrum shows a broad absorption band in the region 3700–3200 cm⁻¹, indicating O–H stretching of alcohols or phenolic compounds. Peaks around 2915–2850 cm⁻¹ correspond to aliphatic C–H stretching, confirming the presence of hydrocarbons. Weak bands near 2350 cm⁻¹ may be due to atmospheric CO₂ interference. The peak observed around 1700–1600 cm⁻¹ suggests C=O stretching or C=C stretching of conjugated systems. Absorption bands near
1500–1400 cm⁻¹ indicate aromatic ring vibrations and C–H bending. Strong peaks in the region 1250–1000 cm⁻¹ correspond to C–O stretching, indicating alcohols, ethers, or esters. The peaks below 900 cm⁻¹ represent out-of-plane C–H bending, confirming substituted aromatic structures.Overall, the spectrum indicates the presence of hydroxyl, carbonyl, aliphatic, and aromatic functional groups, and suggesting phytoconstituents in the sample.
iii. IR of mixture of Azadiracta indica and Allium sativum
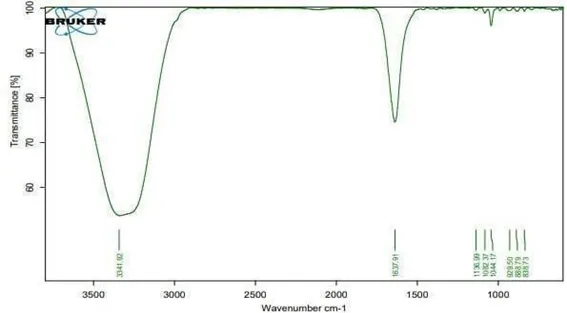
Fig.no: 5
The FTIR spectrum shows a broad and strong peak at 3341 cm⁻¹, indicating O–H stretching of alcohols or phenolic compounds. A sharp peak at 1637 cm⁻¹ corresponds to C=C stretching or may indicate amide (N–H bending) vibrations. The absence of strong peaks near 2900 cm⁻¹ suggests minimal aliphatic C–H stretching. Peaks observed at 1138, 1083, and 1044 cm⁻¹ are due to C–O stretching, indicating alcohols, ethers, or glycosidic linkages. The bands at 929, 888, and 858 cm⁻¹ represent out-of-plane C–H bending, suggesting substituted aromatic rings or alkenes. Overall, the spectrum confirms the presence of hydroxyl, unsaturated (C=C), and ether functional groups, indicating phytochemical constituents in the sample.
4.5. Lambda Max mixure of Azadiracta indica and Allium sativum
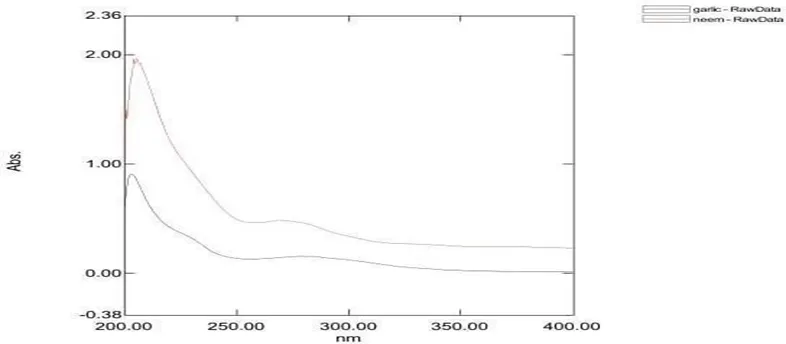
Fig. no.6
4.6 Calibration curve of Azadiracta indica and Allium sativum
|
Sr. No |
Concentration (ug/ml) |
Absorbance |
|
1. |
02 |
0.13 |
|
2. |
04 |
0.31 |
|
3. |
06 |
0.5 |
|
4. |
08 |
0.7 |
|
5. |
10 |
0.85 |
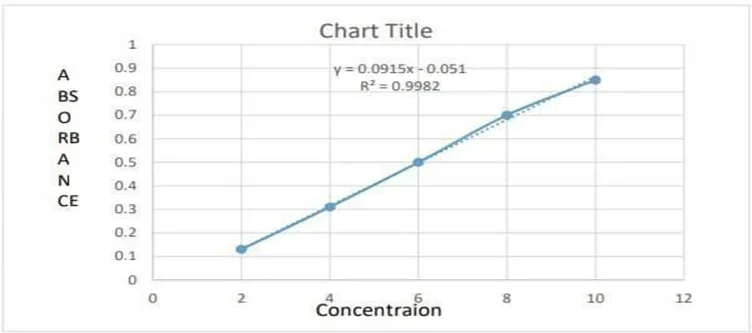
Fig no: 7
5. Evaluation of transdermal patches
5.1. Physical appearance
All of the patches are found to be opaque, non-sticky, homogenous. The presence of plasticizers may explain the flexibility, smoothness opaqueness and non-stickiness of the material.
Fig no: 8
5.2.Thickness
The thickness of each produced patch varied from 0.24 to 0.28 mm . Low standard deviation values in measures of film thickness kept patches uniform, demonstrating the dependability of the patch preparation process
5.3.Weight uniformity
Individually weighing 10 randomly selected patches was used to investigate weight variation. For each formulation , this determination was made. The weight ranged from 284.50 to 291.07 milligrams.
5.4. Flatness
The flatness evaluation indicated that all formulations were completely flat, as there was no change in the strip length before and after cutting. The absence of constriction confirmed that the patches possessed a smooth and uniform surface. This suggests that the patches would maintain their shape and remain properly adhered when applied to the skin.
5.5.Folding endurance
The tested patches demonstrated remarkable mechanical resilience, effectively maintaining their structural integrity and original form when subjected to skin-like folding. The folding endurance values, ranging from
28.64±0.08 to 36.55±0.06, confirm that these formulations are flexible and resistant to rupture during typical application on the skin.
5.6. Percentage drug content
The evaluation of drug content across all formulations revealed high uniformity among the patches. Measured values spanned from 76.56% (±0.25) to 83.67% (±0.18). These results confirm that the manufacturing process used in this study is effective at producing patches with stable medicinal concentrations and minimal deviation.
5.7. pH
The pH for Azadiracta indica was found to be 5.8 to 6.2 and for Allium sativum pH was found to be
5.4 to 6.0 .
Fig. no: 9
5.8. In vitro Cumulative Percentage Drug Release
|
Sr. no |
Time |
F1(%) |
F2(%) |
F3(%) |
|
1 |
0 |
0 |
0 |
0 |
|
2 |
1 |
10.48 |
11.42 |
8.22 |
|
3 |
2 |
12.46 |
12.84 |
10.6 |
|
4 |
3 |
25.08 |
14.64 |
11.75 |
|
5 |
4 |
24.39 |
15.14 |
13.04 |
|
6 |
5 |
27.54 |
18.64 |
16.2 |
|
7 |
6 |
28.52 |
21.1 |
22.1 |
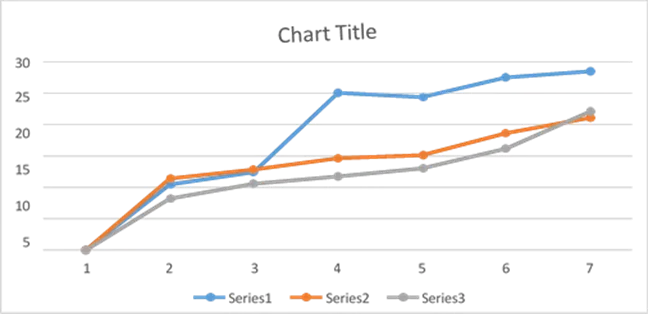
Fig. no.10
The prepared patches were smooth, flexible and uniform. Totally three formulations were formulated Using HPMC and methyl cellulose in different ratios. The result of invitro drug release through onion from different formulation as shown in table. The corresponding value of cumulative percentage drug release from the formulation F1, F2 and F3 in 6 hours were 28.52%, 21.1% and 22.1% respectively. From the invitro permeation study it was confirmed that release of drug from formulation F1 in 6 hours was found to be higher than F2 and F3 formulation so the formulation F1 is optimized.
CONCLUSION
A transdermal patch or skin patch is a medicated adhesive patch that is placed on the skin to deliver a specific dose of medication through the skin and into the blood stream Transdermal drug delivery represents one of the most rapidly advancing areas of novel drug delivery. Due to recent advances in technology and the ability to deliver the drug systemically without rupturing the skin membrane, transdermal route is becoming a widely accepted route of drug administration. TDDS are designed for controlled release of drug through the skin into systemic circulation maintaining consistent efficacy. It offers the delivery of drug at lowered dose that can save the recipient from the harm of large doses with improved bioavailability. In TDDS, there are many methods of preparation of transdermal patches like circular Teflon mould method, assymetric tpx membrane method, mercury substrate methods, IPM membrane methods, EVAC membrane method, aluminium backed adhesive film method, Proliposome/ Proniosome based method, free film method. Cellulose derivative, zein, gelatin, polyvinyl alcohol, polyvinyl chloride, polyethylene, polypropylene this are the polymers used in the preparation of transdermal patches. This may be achieved by by-passing the hepatic first metabolism. Almost all major and minor pharmaceutical companies are developing TDDS.
REFERENCES
Akhter M, Alam MM. Physical pharmacy and instrumental methods of analysis. Springer; 2023. p. 55–77, 123–156.



Shelke A. P, Jadhav S. S, Vijay Balu Patait, Formulation and evaluation of Transdermal Patch containing Azadiracta and Allium sativum, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 3501-2513, https://doi.org/10.5281/zenodo.21412790
 10.5281/zenodo.21412790
10.5281/zenodo.21412790