
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
AISSMS College of Pharmacy, Pune, Maharashtra-411001.
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) represents one of the most prevalent chronic liver diseases in the world as well as is closely related to metabolic disorders obesity, type 2 diabetes mellitus, dyslipidemia, hypertension, and insulin resistance. Disease is a result of over accumulation of triglycerides in the hepatocytes that can lead to the progressive stages of hepatic steatosis to other serious diseases such as metabolic dysfunction-associated steatohepatitis (MASH), fibrosis, cirrhosis, and hepatocellular carcinoma. The rising case of MASLD across the globe is directly connected to sedentary living, unhealthy eating, and the escalating metabolic syndrome. MASLD is a complicated pathogenesis that entails several interconnected processes that include insulin insensitivity, enhanced de novo lipogenesis, oxidative stress, inflammation, mitochondrial dysfunction, and gut-liver axis disruptions. The role of genetic susceptibility is also important and the variations in the genes like PNPLA3, TM6SF2 and HSD17B13 affect lipid metabolism and the development of the disease. MASLD can also be asymptomatic at early stages and is often accidentally identified during regular clinical visits or radiographic tests. Diagnosis is usually by means of laboratory tests, imaging methods including ultrasound and MRI and occasionally a liver biopsy to precisely stage the disease. When MASLD is not treated, it may cause severe hepatic and extrahepatic problems such as cardiovascular disease and chronic kidney disease. Thus, it is necessary to identify and manage early diseases with an emphasis on metabolic control, lifestyle change, and treatment methods that would help prevent development of the disease and enhance long-term health outcomes
Steatotic liver disease (MASLD) is a loose clinical term that is employed to describe a continuum of
liver diseases that includes the abnormal build-up of fat in liver cells in connection with metabolic dysfunction. Hepatic steatosis is defined as the process of triglycerides in the hepatocyte, which may be observed with the help of imaging method and confirmed by means of histologic research. MASLD is among the most prevalent chronic liver diseases in the world and is strongly linked with the metabolic diseases including obesity, type 2 diabetes mellitus, dyslipidemia, hypertension and insulin resistance. The disease is covered by a variety of conditions which run a continuum of simple hepatic steatosis to more serious complications of steatohepatitis, fibrosis, cirrhosis and finally hepatocellular carcinoma [1,2]. The growing incidence of MASLD has been one of the consequences of the escalating cases of obesity and metabolic syndrome in the world as well as in both developed and developing nations.
The idea behind the MASLD and its name have developed during a number of decades. Historically, the fatty liver disease was initially identified in the 19th century after pathologists noticed fatty infiltration in the liver of people who consume alcohol excessively. Fatty liver had been divided into alcohol-related liver injury as well as fatty liver over many years. Nevertheless, towards the end of the 20th century, clinicians started diagnosing patients who developed fatty liver changes even though they did not consume alcohol in large amounts or at all. In 1980, Ludwig and others defined a phenomenon called nonalcoholic steatohepatitis (NASH) as the state where hepatic steatosis was accompanied by inflammation and hepatocellular in the non-alcoholic drinkers. This spawned the more comprehensive nonalcoholic fatty liver disease (NAFLD) which encompassed both simple steatosis and nonalcoholic steatohepatitis. The diagnosis of NAFLD was mainly based on the absence of other liver disease causes, particularly, the intake of alcohol in large amounts. In the long run, the shortcomings of this nomenclature came into the limelight since it was deemed scientifically weak and even perplexing to describe a disease in terms of what it is not. Also, the word fatty was thought to be having negative stigma to the patients.
In order to overcome these limitations, some new terminology was suggested by experts, which is more likely to reflect the underlying pathophysiological mechanisms of the disease. In 2020, Eslam and colleagues coined the term of metabolic dysfunction-associated fatty liver disease (MAFLD). This definition focused on the hepatic steatosis presence along with the metabolic risk factors like obesity, type 2 diabetes mellitus, or other metabolic disorders. The MAFLD concept changed the paradigm of excluding alcohol intake to metabolic dysfunction as the main cause of liver disease. Later on, the nomenclature was further improved by an international consensus which included the term metabolic dysfunction–related steatotic liver disease (MASLD). MASLD has been included as one of the subtypes of the broader term steatotic liver disease (SLD), which encompasses a number of conditions that lead to the accumulation of hepatic fats. The new classification offers a more realistic and comprehensive approach to the diagnosis of fatty liver diseases and studying them and indicates the accumulating knowledge about the metabolic processes of hepatic steatosis.
MASLD is the pathological process of the liver that can go through the mildest fat deposition to the most serious liver damage. The most basic one is the isolated hepatic steatosis, whereby the liver cells are filled with fat with minimal inflammation or fibrosis. Although simple steatosis may not cause any further disease over many years, in some people, simple steatosis can develop into a more aggressive disease, called metabolic dysfunction-associated steatohepatitis (MASH). The liver pathology of MASH is a hepatic steatosis and inflammation, hepatocellular injury, and different extents of fibrosis. Prolonged inflammation and fibrotic alteration can eventually result into progressive fibrosis and cirrhosis, characterized by scarring of liver tissue extensively and liver dysfunction. Cirrhosis has a great role in causing hepatocellular carcinoma, the most widespread primary liver cancer. Thus, MASLD is a disease with many stages of development, and it is critical to detect it and manage it early.
MASLD is caused by a number of metabolic and environmental factors. Insulin resistance, which facilitates the deposition of fatty acids in liver is the most significant underlying mechanism. Overconsumption of calories and lack of exercise in people with obesity or possessing a metabolic syndrome result in more adipose tissue lipolysis and increased levels of circulating free fatty acids. These fatty acids are taken to the liver, which transforms to triglycerides and is stored in hepatocytes [3,4]. Also, greater de novo lipogenesis hepatic accumulation and the inability to oxidize fatty acids are additional contributors to lipid build-up. Oxidative stress, mitochondrial dysfunction, and cytokine release play a role in hepatocellular injury and steatohepatitis development of simple steatosis. The genetic predisposition, changes in the gut microbiota, as well as the impact of the diet and hormones, are also important in the development and progression of diseases.
Clinical manifestations of MASLD are subtle or not present especially at the initial stages of the disease. A lot of people do not show any symptoms and are accidentally diagnosed when a routine medical checkup was done or when an imaging procedure was conducted due to other causes. The symptoms are usually nonspecific when they happen and could consist of fatigue, weakness, and feeling of discomfort or fullness in the upper right quadrant of the abdomen. Other patients can have mild hepatomegaly or enlargement of the liver that is felt during the physical examination. With the further development of the disease to the advanced fibrosis or the cirrhosis, more serious symptoms can emerge. These can be jaundice, swelling in the abdomen by ascites, easy bruising, confusion by hepatic encephalopathy and general weakness. Portal hypertension, gastrointestinal bleeding, liver failure are complications that may arise in the progression in the advanced stages.
MASLD diagnosis is made through a complex of the clinical examination, lab tests, radiography, and occasionally liver biopsy. The initial diagnosis requires the detection of the existence of hepatic steatosis, through imaging systems that may include ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI). The most frequently used imaging method as the first one is ultrasound due to its noninvasive nature, universal availability and the fact that it is not a very expensive method. It is able to detect moderate and severe fat in the liver but it could be weak when it comes to the detection of mild steatosis. MRI and some special methods like the proton density fat fraction (MRI-PDFF) are more precise to determine the hepatic fat content and are typically applied in the research sphere or special clinics.
The laboratory tests are also significant in the assessment of MASLD. Detection of slightly higher liver enzymes, especially liver alanine aminotransferase (ALT) and aspartate aminotransferase (AST) may be observed in blood tests. But the normal liver enzyme levels do not rule out the occurrence of MASLD since there are also patients whose liver is not damaged severely but yet they have normal enzyme levels. Further lab tests can consist of lipid profile evaluation, fasting glucose, glycated hemoglobin (HbA1c), and indicators of insulin resistance to assess risk factors of related metabolic disorders. Simple noninvasive scoring systems like the Fibrosis-4 (FIB-4) index and NAFLD fibrosis score can usually be used to estimate the risk of progressive liver fibrosis in relation to the routine clinical parameters.
Imaging techniques that have been shown to measure liver stiffness, including transient elastography (FibroScan), can be used to measure the presence and extent of fibrosis in some scenarios. Those are noninvasive methods of liver biopsy, which gain popularity in clinical practice. Although noninvasive diagnostic methods have advanced, liver biopsy is still considered the gold standard in the confirmation of the diagnosis of steatohepatitis and the stage of liver fibrosis. The important characteristics that can be observed through the histological analysis of liver tissue include macrovesicular steatosis, hepatocellular ballooning, lobular inflammation and fibrotic changes. Nonetheless, liver biopsy is very invasive and may come with complications hence it is usually done on some selected cases when the diagnosis is not clear or when it is necessary to have proper staging of the disease.
Over the past decades, the global burden of MASLD has grown tremendously with the escalating levels of obesity, sedentary lifestyles and the occurrence of metabolic disorders. Epidemiological researches have estimated that MASLD has a prevalence of about a quarter-third of adult population all over the world. Its occurrence is quite high in patients with type 2 diabetes mellitus and obesity, and over 50% of these patients have signs of hepatic steatosis. MASLD is also being identified in children and adolescents, which is partly the role of the increasing prevalence of childhood obesity. The disease does not only cause liver related morbidity and mortality, but also raises chances of cardiovascular disease, which is still the leading cause of death among the victims.
To conclude, steatotic liver disease associated with metabolic dysfunction is a multifactorial and complicated issue in relation to excessive fat deposition in the liver in relation to metabolic dysfunction. The development of previous names like NAFLD into the current MASLD classification is a positive sign of a better comprehension of the metabolic causes behind the disease and attempts to offer a more straightforward and mechanistic model of diagnosis and studies. There is a broad range of pathological stages involved in MASLD with presence of simple steatosis up to hepatocellular carcinoma as a result of fibrosis, steatohepatitis, cirrhosis and steatosis. In spite of the fact that the disease is not accompanied with many symptoms in its initial stages, gradual liver damage may result in severe complications. Clinical evaluation, laboratory tests, and imaging studies should therefore be carried out at an early stage so that the disease can be managed and prevented. Since the number of patients with metabolic disorders has become increasingly high worldwide, MASLD is likely to remain a significant concern of healthcare systems and a significant subject of current medical studies.
CAUSES AND RISK FACTORS:
The picture demonstrates the key risk factors that can take part in the development of Metabolic Dysfunction associated Steatotic Liver Disease (MASLD) and how interplaying metabolic, genetic and environmental factors can result in liver injury. MASLD is a multifaceted metabolic disease that is related to the accumulation of fat in the liver cells which may eventually result in inflammation, fibrosis and severe liver complications without proper management. Genetic predisposition is also one of the key factors in MASLD development. Certain genetic mutations that include PNPLA3, TM6SF2, and HSD17B13 are identified to play a role in determining the intensity of lipid metabolism and fat build-up in the liver. These genes have the capability to modify the hepatic fat storage, lipid transport and inflammatory response and this renders some people more vulnerable to developing MASLD despite having no major lifestyle-related risk factors. Genetic susceptibility thus is very important in influencing the severity and development of the disease in various people. One more significant factor that contributes to the process of MASLD is Type 2 diabetes mellitus that is strongly correlated with insulin resistance and metabolic imbalance. Hyperinsulinemia and long-term hyperglycemia are the factors that make the liver increase hepatic lipid synthesis and decrease lipid oxidation, which leads to excessive fat accumulating in the liver. These metabolic alterations may also stimulate a number of molecular pathways including transforming growth factor beta (TGF- β) and connective tissue growth factor (CTGF), which stimulate liver inflammation and fibrosis. Also, NOX2 and TIMP3 as enzymes mediate oxidative stress and deactivate protective factors like Sirt1 and TIMP3, which worsen liver damage [5,6]. Therefore, patients with Type 2 diabetes are much more exposed to the risk of developing MASLD and developing the disease at a high rate. Another significant risk factor of MASLD is visceral obesity. Abdominal fat in excess is metabolically active and condenses different pro-inflammatory cytokines and adipokines that interfere with the normal metabolism. High concentrations of the inflammatory mediators and hormones like leptin favor insulin resistance and improve lipid buildup in the liver. Simultaneously, changes in adiponectin levels upset the defensive metabolic processes which, as a rule, maintain the metabolism of glucose and lipids. Such an unbalance of pro-inflammatory and protective signals provides a metabolic environment, which supports hepatic steatosis, inflammation, and fibrosis. This means that people having central obesity are highly susceptible to the development of MASLD and associated metabolic issues. The diet and lifestyle are also important factors that contribute to the occurrence of MASLD. Diets characterized by excessive intake of saturated fatty acids (SFAs), processed foods, and alcohol intake are major causes of metabolic imbalances, which influence the condition of the liver. The consumption of high-fat diets may trigger toll-like receptors (TLRs), which cause the rise of inflammatory signals and oxidative stress in the liver. Such dietary habits can also disrupt autophagy, which is a protective mechanism of the cell that gets rid of damaged organelles (and surplus lipid droplets). Decreased autophagy is thus capable of advancing lipid collection and dysfunction of the hepatocytes. Prolonged exposure to these food elements can also elevate the likelihood of tumorigenesis and developed liver diseases. The other crucial aspect that is indicated in the diagram is gut dysbiosis, which is described as an excess of intestinal microbiota. The gut-liver axis is important in ensuring metabolic and immune homeostasis. The disturbance of the gut microbial community may elevate intestinal permeability through which bacterial elements and toxins may enter the bloodstream and reach the liver. It is called bacterial translocation and causes inflammatory reactions and the release of cytokines like interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-A). Also, gut dysbiosis has the potential to disrupt intestinal nuclear receptors like FXR that mediate bile acid metabolism and lipid homeostasis. The combination of these changes leads to inflammation of the liver, metabolic dysfunction and evolution of the disease in the MASLD. In general, the pathogenesis and pathophysiology of MASLD are the combination of a number of factors such as genetic predisposition, metabolic diseases such as Type 2 diabetes, visceral obesity, unhealthy dietary habits, and intestinal microbiome disruptions. All these mechanisms contribute to fat deposition in the liver, inflammation and oxidative stress, and fibrosis eventually leading to the development of serious liver complications [7]. These risk factors are important to understand in order to come up with efficient preventive and therapeutic measures that would help in controlling the abnormalities of their metabolism, lifestyle, and keep the gut healthy. These contributing factors can be identified and managed early and this will go a long way in the prevention of the further development of the disease and this will also be able to enhance the long-term liver health outcomes. The risk factors are presented in Fig. 1.1.
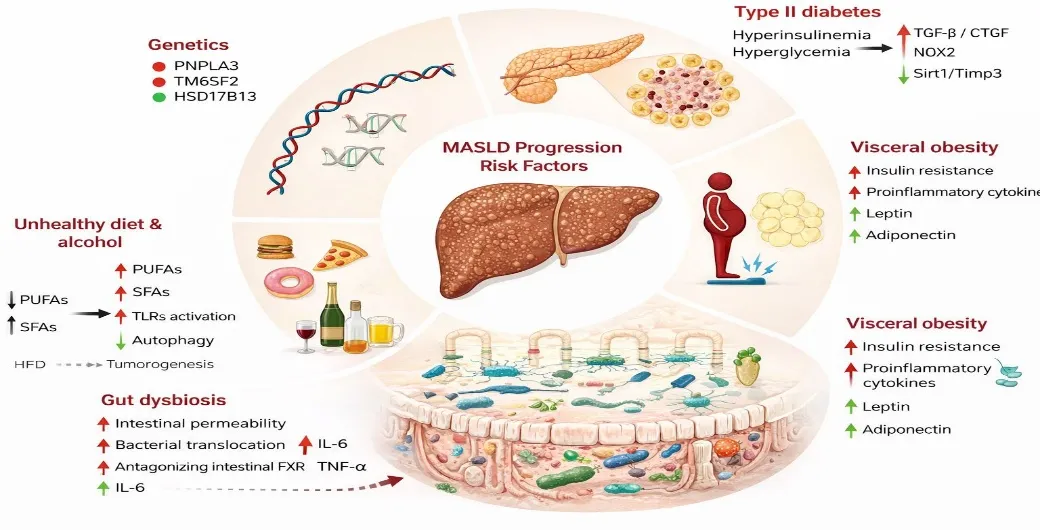
Fig. 1.1- Risk factors of MASLD
COMPLICATIONS:
A new form of steatotic liver disease (MASLD) has become the most prevalent cause of chronic liver disease across the world and is caused by obesity and type 2 diabetes epidemics in the world. The pathophysiology of MALSD consists of hepatic steatosis with metabolic dysfunction, which consists of obesity, type 2 diabetes, dyslipidemia, and hypertension. The disease may develop into metabolic dysfunction-related steatohepatitis (MASH), simple steatosis, more advanced fibrosis, cirrhosis and finally hepatocellular carcinoma. Nevertheless, MASLD has much wider clinical implications than hepatic complications since it is a systemic metabolic disease that has severe cardiovascular and metabolic effects [8,9]. The complications are presented in Fig. 1.2.
Cirrhosis and Hepatic Decompensation-
Cirrhosis is a significantly severe terminal in MASLD pathogenesis, which happens when structural distortion of the liver caused by chronic inflammation and fibrosis is untenable. Cirrhosis related to MASLD is marked by high morbidity and mortality rates and liver fibrosis was determined as the greatest predictors of mortality in patients with this condition. Cirrhosis is an evolutional process whose development is complicated by the presence of insulin resistance, lipotoxicity, chronic inflammation, and mitochondrial dysfunction. The progression of the compensated to the decompensated cirrhosis is marked by hepatic decompensation which is manifested by ascites, variceal bleeding, hepatic encephalopathy, and jaundice [10,11]. A study of MASLD cirrhosis by Veterans Affairs cohort study revealed that lean patients with compensated cirrhosis had a lower risk of hepatic decompensation than non-lean patients, but had a higher all-cause mortality paradoxically compared to non-lean patients.
Hepatocellular Carcinoma-
Hepatocellular carcinoma (HCC) is one of the most detrimental complications of MASLD and that is expected to cause most HCC in the world because of rising comorbidities in metabolism. Remarkably, MASLD-related HCC may also manifest itself without cirrhosis and is, therefore, not to be confused with other causes of chronic liver disease. The pathways that mediate MASLD-associated hepatocarcinogenesis are multifactorial that comprise adipose tissue-mediated inflammation, hormonal alterations, lipotoxicity, oxidative stress, gut dysbiosis, and genetics. Ferroptosis may be caused by lipid peroxidation in MASLD and MASH, which are involved in the development of HCC. A national cohort study established that persistent MASLD has the greatest risk of HCC, incidence and resolved MASLD has a second highest risk, but resolved MASLD still has a residual risk of HCC [12].
Liver failure and transplantation-
The term liver failure and transplantation are also referred to as hepatic insufficiency and transplantation. Liver failure may develop later in advanced MASLD and requires liver transplantation. MASLD is currently the leading predictor of liver transplant in the United States in the case of HCC and in women. The incremental rate of MASLD-associated end-stage liver disease is indicative of the escalating rate of metabolic risk factors as well as the progressive progression of the disease. MASLD-related cirrhosis patients must be monitored closely to observe any signs of hepatic decompensation and undergo any assessment to undergo transplantation as early as possible [13].
Cardiovascular Disease-
Heart disease (CVD) is the most common cause of death among MASLD patients exceeding deaths related to the liver even in advanced liver disease. There is an independent association of MALSD with higher risks of coronary artery disease, stroke, arrhythmias and heart failure. A population-based investigation on coexistence of MASLD and chronic kidney disease has established that persons with both illnesses were at the greatest risk of coronary heart disease (relative risk 1.79) and heart failure (relative risk 2.33). Pathophysiological interrelationships exist between MASLD and CVD include insulin resistance, visceral adiposity, systemic inflammation, oxidative stress and endothelial dysfunction. These common mechanisms contribute to subclinical atherosclerosis and fast-tracked cardiovascular disease. An extensive meta-analysis of 129 articles proved that MASLD is related to 43% more risk of cardiovascular outcomes [14].
Chronic Kidney Disease-
Chronic kidney disease (CKD) is a severe extrahepatic MASLD complication, and the two diseases have two-way effects. MASLD is linked to 38 per cent more risk of getting CKD. MASLD in combination with CKD has a potent increase in mortality risk, especially in the group of people having advanced hepatic fibrosis and CKD. Patients with MASLD and CKD have the incidences of obesity, hypertension, dyslipidemia, and diabetes that are the highest, thus forming a high-risk group. MASLD-CKD axis shows overlapping pathways of metabolic dysfunction, inflammation, and oxidative stress with opportunities of early interventions [15].
Type 2 Diabetes and Metabolic Syndrome-
There is a bidirectional correlation between MASLD and type 2 diabetes, in which each disorder worsens the other. MASLD is linked to a 2.56-fold higher risk of incident diabetes, and the patients with advanced liver disease are at an even higher risk (hazard ratio 3.60). On the other hand, type 2 diabetes increases the speed of MASLD to MASH, fibrosis, and cirrhosis and HCC. Pathogenesis is associated with genetic polymorphisms, the environment, and various metabolic alterations such as insulin resistance, gut dysbiosis, and adipokines signaling. There is a high correlation of MASLD with metabolic syndrome as well, and the difference is 2.57 times higher. Also, MASLD gives a 75 percent risk-enhancement of incident hypertension and a 69 percent risk-enhancement of prediabetes [16].
Clinical Outcomes and Mortality-
Clinical outcomes of MASLD are indicative of the systemic nature as well as the interaction of the hepatic and extrahepatic complications. Although MASLD may develop in cirrhosis and HCC, the majority of non-cirrhotic MASLD patients succumb to non-hepatic diseases, especially cardiovascular disease and non-hepatic cancers. This trend highlights the need to implement both extrahepatic and hepatic risk assessment and management programs. It was shown in a meta-analysis that MASLD is linked to the additional risk of all types of cancer (54% higher risk), which can be considered the effect of the disease as a systemic one with far-reaching implications. The risk of mortality is especially higher in patients with a combination of coexisting chronic conditions, i.e. both patients with MASLD and CKD, who exhibit an adjusted hazard ratio of 3.28 in terms of mortality.
These results underline the fact that the effective management of MASLD should go beyond liver-based therapy and include cardiovascular risk prevention, metabolic optimization, and extrahepatic complications screening.
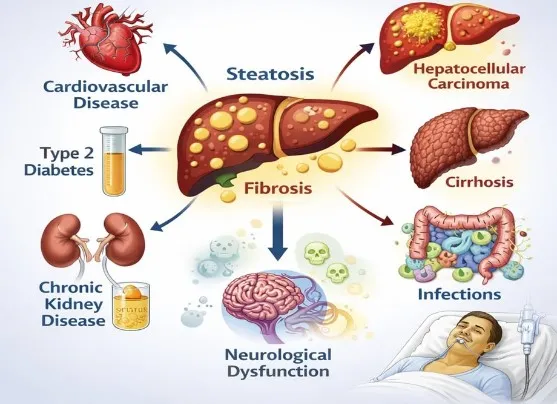
Fig. 1.2- Complications of MASLD
PATHOGENESIS:
MASLD is the manifestation of the dysfunction of the liver metabolism and not only the issue of fat accumulation. It is the result of the interplay between dysfunction of the insulin singling, lipid metabolism, oxidative stress, inflammation, gut homeostasis and genetic susceptibility.
Insulin Resistance
The Primary Driver Insulin resistance is the primary pathophysiological process of MASLD.
Insulin prevents lipolysis in the adipose tissue and regulates the hepatoglucose and lipid metabolism in a normal condition. When resistance occurs, the adipocytes will leech out excess of the free fatty acids (FFAs) into the blood. Approximately 60-percent of hepatic fat is caused by lipolysis in the adipose tissue, and the remaining fraction of it is caused by dietary fats and de novo lipogenesis (DNL) in hepatocytes.
The FFAs are deposited in the liver and overload it which are then converted to triglycerides leading to hepatic steatoses. Meanwhile, hepatic insulin resistance enhances gluconeogenesis and lipogenic pathways and this additional results in a further increase in fat deposition [17,18].
Excessive de novo lipogenesis occurs during the generation of new fat
The intake of excess carbohydrates and specifically the fructose encourages DNL. The transcription factors that activate the activity of the enzymes necessary in the synthesis of fatty acids are called sterol regulatory element-binding protein (SREBP1c) and carbohydrate response element-binding protein (ChREBP). Even though initially the formation of a triglyceride is a protective mechanism to store the excess fat in a harmless location, the lipids become accumulated with the continuous growth in the toxic l intermediates such as diacylglycerols and ceramides thus raising the insulin resistance.
Lipotoxicity/ Oxidative Stress
Lipotoxicity is a condition that arises when the storage level of lipid is exceeded. This affects the b-oxidation of mitochondria leading to excess production of reactive oxygen species (ROS). Oxidative stress damages protein, lipids and DNA of cells. Apoptosis and injury of hepatocytes is also raised by endoplasmic reticulum stress. This is the beginning of nonmalignant necrosis of hepatocytes.
Inflammation and Fibrogenesis
Injured hepatocytes release damage signals to initiate Kupffer cells and inflammatory cells. These immune cells secrete proteins of inflammation such tumor necrosis factor a (TNF a) and transforming growth factor b (TNF b). With prolonged inflammation this initiates special cells in the liver is known as hepatic stellate cells. Progressive accumulation of extracellular matrix proteins by these cells can consequently cause scarring of the tissues, and is, so far, the most significant prognosticator of the disease outcome in the long run.
Gut-Liver Axis Dysfunction
In case of gut dysbiosis and augmented intestinal permeability, dysbiosis in the gut and inflammatory mediators can enter the liver via portal. The altered bile acid signalling and non-functional metabolic regulation also cause disturbed lipid homeostasis and insulin sensitivity worsening hepatic damage.
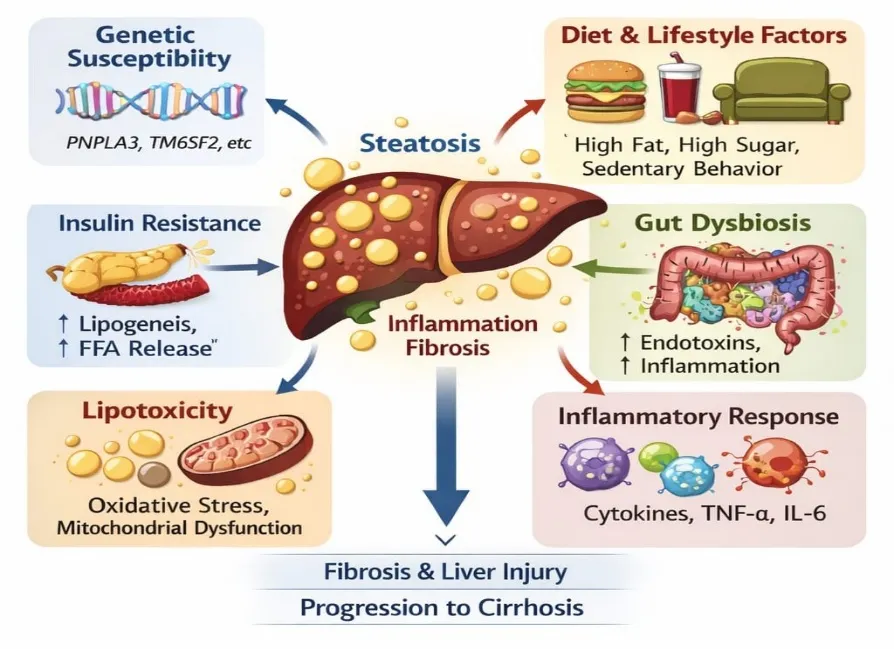
Fig. 1.3- Pathogenesis of MASLD
Genetic Susceptibility
Genetic variation is particularly in lipid metabolic genes which predetermine the sizes of fat and the pathogenesis of fibrosis. These differences are indicative of the fact that some of them progress to steatohepatitis and fibrosis, but others remain quite stable [19].
The Fig. 1.3 shows pathogenesis of MASLD.
ALLOPATHIC REMEDIES:
The allopathic treatment of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) is aimed at alleviating fat on the liver and enhancing metabolic regulation and avoiding complications, including inflammation and fibrosis. As MASLD is tightly connected with such metabolic diseases as obesity, type 2 diabetes, and dyslipidemia, drugs are often aimed at these comorbidities. The use of insulin sensitizers including metformin and pioglitazone aids in increasing the sensitivity of insulin and decreasing fat levels in the liver. Semaglutide and liraglutide are GLP-1 receptor agonists that induce weight reduction and liver reduction of fat, thus enhancing steatohepatitis. SGLT-2 inhibitors such as empagliflozin and dapagliflozin enhance the glycemic control and decrease fat in the liver by augmenting glucose excretion via the kidneys. Lipid-lowering drugs, especially atorvastatin and rosuvastatin statins, can be used to treat dyslipidemia and decrease cardiovascular risks in patients with MASLD. Also, antioxidants have the potential to influence the amount of oxidative stress and liver inflammation. More recent agents like thyroid hormone receptor-2 agonist (resmetirom) and FXR agonists (e.g., obeticholic acid, in trials) are liver metabolism/fibrosis agonists with potential to be used in advanced MASLD [20]. Fig. 1.4 shows classification of drugs used in treatment of MASLD.
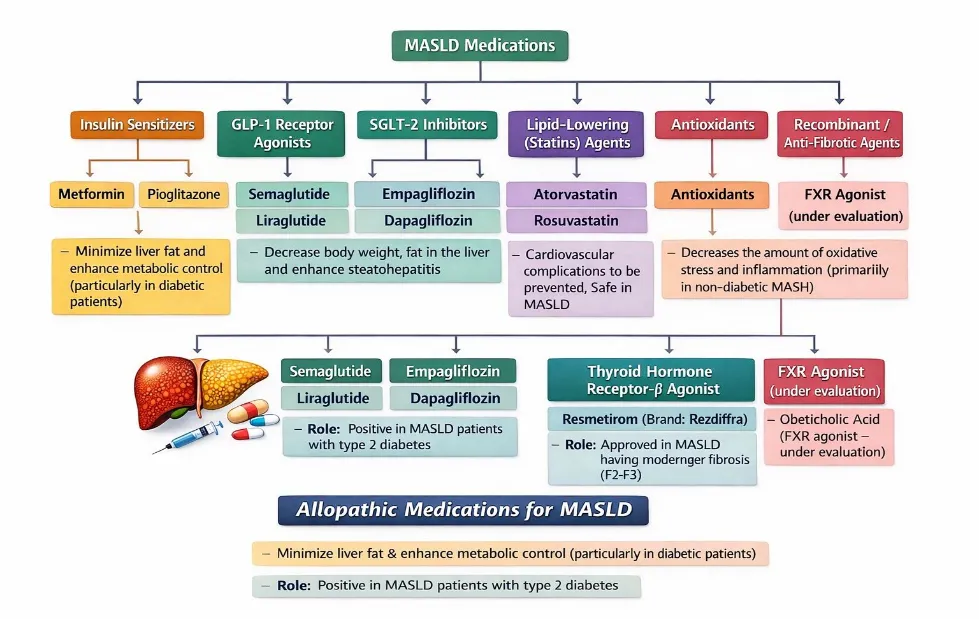
Fig. 1.4- Classification of drugs used in MASLD
AYURVEDIC REMEDIES AND MEDICINAL PLANTS USED IN MASLD:
According to Ayurveda, liver diseases that do resemble steatotic liver disease (MASLD) are in most cases related to the following conditions: Yakrit Roga (liver disorders), Medoroga (disorders related to fat metabolism), and Agnimandya (impaired digestive fire). The liver, according to Ayurvedic theory, is very important in digestion, metabolism and detoxification and imbalance in Pitta dosha, as well as disequilibrium of Kapha and Meda dhatu (fat tissue), may cause the liver to accumulate fat and toxins. Modern MASLD has many similar pathological characteristics with these Ayurvedic ideas such as lipid metabolism, inflammation, and oxidative stress. Hence, Ayurvedic treatment methods aim at restoring the metabolic balance, improving liver functioning, improving digestion and eliminating accumulated toxins in the body. The Ayurvedic care of fatty liver diseases is usually focused on dietary control, lifestyle management, herbal treatment and detoxification therapies (Panchakarma). Traditional medicine uses herbal drugs that have hepatoprotective, antioxidant, anti-inflammatory and lipid-lowering effects to take care of liver health. The herbs are used to prevent the buildup of fat in the liver, aid in bile secretion, increase the digestion, and stimulate detoxification. Ayurveda has many medicinal plants that have undergone scientific studies and have been found to contain bioactive compounds that help to prevent the oxidative damage of the liver cells and inflammation. Phyllanthus niruri, also referred to as Bhumyamalaki is one of the most popular herbs used in treating liver disorders. This plant is the traditional Ayurveda usage in the treatment of jaundice, hepatitis, and liver diseases. It has bioactive substances including lignans, flavonoids, and alkaloids which have hepatoprotective effects, antioxidant effects and anti-inflammatory effects. Research has indicated that this plant extract has the potential to lower hepatic enzyme levels and hepatocyte toxicity. Likewise, Andrographis paniculata (Kalmegh) is another famous Ayurvedic herb having great Hepatoprotective properties. Andrographolide, which is the active compound found in this plant has been said to decrease inflammation, improves liver enzyme levels and prevent oxidative damage to liver cells. The Kutki, Picrorhiza kurroa is another plant of importance medically as used in Ayurvedic preparations targeting liver problems [21-25]. Active constituents of kutki include picroside I and picroside II and both have hepatoprotective and antioxidant properties. It is conventionally applied in management of liver enlargement, fatty liver and gastrointestinal diseases. Kutki assists in the secretion of biles, increased digestion, and decreased the development of lipids in the liver. Yashtimadhu or licorice Glycyrrhiza glabra is also used to treat liver ailment because of its anti-inflammatory and hepatoprotective qualities. The most significant bioactive substance in licorice, glycyrrhizin, has been found to prevent oxidative damage of liver cells and lower the liver disease-related inflammation. Silybum marianum, also known as Milk Thistle is another well-known liver protective plant. It is not a classical Ayurvedic ingredient although it is often used in modern herbal medicine because it has been well-documented to have hepatoprotective effects. Silymarin (form of silymarin that is active) aids in stabilizing liver cell membranes as well as promotes liver regeneration, and oxidative damage. Milk thistle is also popular as an auxiliary medication in multiple liver diseases such as the fatty liver disease. Turmeric or Haridra (Curcuma longa) is also an important component in Ayurvedic treatment of metabolic disorders. The main active constituent of turmeric is curcumin, which is a good antioxidant, anti-inflammatory and lipid-lowering agent. Research studies have shown that curcumin can help decrease hepatic accumulation of fat, increase sensitivity to insulin and decrease inflammatory liver tissue. On the same note, Tinospora cordifolia (Guduchi) has been reported to have immunomodulatory and hepatoprotective effects. Guduchi is useful in enhancing metabolic balance, body detoxification and oxidative stress on the liver. Boerhavia diffusa (Punarnava) is another herb that is helpful and widely used in Ayurvedic medicine to treat liver and kidney problems. Punarnava is diuretic, anti-inflammatory, hepatoprotective and is able to decrease liver swelling and enhance liver function. The herb is commonly used in Ayurvedic preparations that are aimed at liver detoxification and metabolism. Besides single herbs, Ayurveda also prescribes some traditional herbal formulations in treating liver disorders. Arogyavardhini Vati, Liv-52, Punarnavadi Kashayam and Bhumyamalaki Churna are some of the preparations that are commonly used in clinical practice to aid liver functioning [26-29]. These are a combination of herbs which synergize to enhance metabolism, increase the bile release and to decrease the fat deposition in the liver. The lifestyle habits like exercise, healthy eating, and intake of fatty or processed foods should be avoided as other factors of Ayurvedic treatment of MASLD. A summary of the medicinal plants that were typically used to treat fatty liver and other metabolic liver disorders is summarized in the following table 1.1.
Table 1.1 - Medicinal Plants Used in MASLD Management
|
Sr. No. |
Plant Name |
Common Name |
Family |
Part Used |
Major Active Constituents |
Therapeutic Activity |
|
1 |
Phyllanthus niruri |
Bhumyamalaki |
Phyllanthaceae |
Whole plant |
Lignans, flavonoids, alkaloids |
Hepatoprotective, antioxidant |
|
2 |
Andrographis paniculata |
Kalmegh |
Acanthaceae |
Leaves, aerial parts |
Andrographolide |
Anti-inflammatory, hepatoprotective |
|
3 |
Picrorhiza kurroa |
Kutki |
Plantaginaceae |
Rhizome |
Picroside I, Picroside II |
Hepatoprotective, lipid-lowering |
|
4 |
Glycyrrhiza glabra |
Licorice (Yashtimadhu) |
Fabaceae |
Root |
Glycyrrhizin |
Anti-inflammatory, hepatoprotective |
|
5 |
Silybum marianum |
Milk Thistle |
Asteraceae |
Seeds |
Silymarin |
Liver regeneration, antioxidant |
|
6 |
Curcuma longa |
Turmeric (Haridra) |
Zingiberaceae |
Rhizome |
Curcumin |
Anti-inflammatory, antioxidant |
|
7 |
Tinospora cordifolia |
Guduchi |
Menispermaceae |
Stem |
Tinosporin, alkaloids |
Immunomodulatory, hepatoprotective |
|
8 |
Boerhavia diffusa |
Punarnava |
Nyctaginaceae |
Root, whole plant |
Boeravinones |
Diuretic, hepatoprotective |
Ayurvedic medicine provides a number of herbal remedies that could be considered in the treatment of the steatotic liver disease associated with metabolic dysfunction by enhancing liver functionality, mitigating inflammation, and controlling lipid metabolism. Most of these herbs contain bioactive compounds that have been scientifically identified to have hepatoprotective effect. Combinations of traditional herbal therapy and lifestyle change along with the mainstream management of modern medicine can offer an inclusive approach to the prevention and management of MASLD. More clinical studies and controlled trials are however required to determine the effectiveness, safety of these herbal medicines, and the standard dose of these herbs in long-term management of the disease [30]. Fig. 1.5 shows key medicinal plants and ayurvedic formulations used in treatment of MASLD.
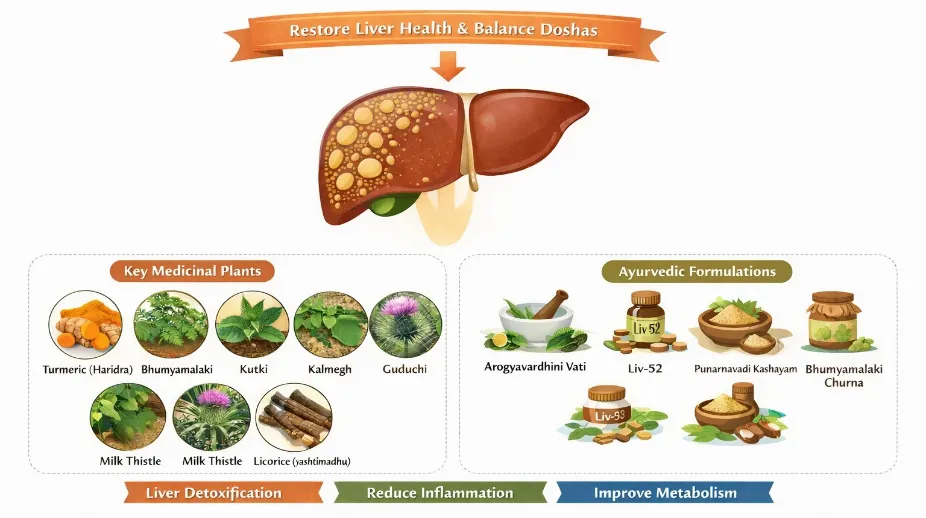
Fig. 1.5 - Ayurvedic remedies for MASLD
Ayurvedic formulations in treatment of MASLD:
The table presents several commonly used Ayurvedic formulations for the management of liver disorders such as MASLD and fatty liver disease. These formulations are produced by well-known Ayurvedic pharmaceutical companies including Himalaya Wellness Company, Baidyanath Ayurved Bhawan, Dabur India Ltd., Arya Vaidya Sala Kottakkal, and Patanjali Ayurved Ltd. Products such as Liv.52 Tablets/Syrup, Liv.52 DS Tablets, and Liv.52 HB Capsules are widely used for improving liver function, managing fatty liver, hepatitis, and protecting the liver from drug-induced toxicity. Other classical Ayurvedic preparations such as Arogyavardhini Vati, Punarnava Mandur, Phalatrikadi Kwath, and Bhumyamalaki Churna are traditionally used for treating liver enlargement, jaundice, digestive disorders, metabolic imbalance, and detoxification of the liver. These formulations help support liver health by improving digestion, enhancing bile secretion, and promoting hepatoprotective activity. The approximate market prices of these products range from ₹120 to ₹594, depending on the formulation, dosage form, and pack size. Overall, these Ayurvedic medicines are commonly used as supportive therapies for maintaining liver health and managing various hepatic disorders [31, 32]. Table 1.2 shows list of ayurvedic formulations in treatment of MASLD.
Table 1.2 - Ayurvedic formulations used in treatment of MASLD
|
Sr. No. |
Name of Product |
Manufactured By |
Used For (Indications) |
Approx. Cost in Market |
|
1 |
Liv.52 Tablets/Syrup |
Himalaya Wellness Company |
Fatty liver, hepatitis, alcohol-induced liver damage, drug-induced hepatotoxicity, cirrhosis (early stage), loss of appetite, improves digestion and liver function |
₹230–₹340 (tablets 60–100), ₹220–₹234 (syrup) |
|
2 |
Liv.52 DS Tablets |
Himalaya Wellness Company |
Fatty liver, liver enlargement, hepatitis, liver detoxification, improves appetite and digestion |
₹230–₹281 for 60 tablets |
|
3 |
Liv.52 HB Capsules |
Himalaya Wellness Company |
Hepatitis B management, liver inflammation, hepatoprotection, improves immune response in liver diseases |
₹211 (10 capsules), ₹594 (30 capsules) |
|
4 |
Arogyavardhini Vati |
Baidyanath Ayurved Bhawan |
Liver disorders, fatty liver, digestive problems, skin diseases, metabolism improvement |
₹150–₹250 (40–80 tablets) |
|
5 |
Punarnava Mandur |
Dabur India Ltd. |
Liver enlargement, anemia, edema, spleen disorders, improves liver function |
₹120–₹200 |
|
6 |
Phalatrikadi Kwath |
Arya Vaidya Sala Kottakkal |
Fatty liver, jaundice, digestive disorders, detoxification, improves metabolism |
₹150–₹300 |
|
7 |
Bhumyamalaki Churna |
Patanjali Ayurved Ltd. |
Hepatitis, fatty liver, jaundice, liver detoxification, improves bile secretion |
₹120–₹180 |
CONCLUSION
Metabolic Dysfunction -Associated Steatotic Liver Disease (MASLD) has become one of the most widespread chronic hepatitis diseases in the world, because of the progressive rise in obesity, unhealthy lifestyles, and metabolic diseases like type 2 diabetes mellitus, dyslipidemia and insulin resistance. The disease is a continuous spectrum of hepatic steatosis to metabolic dysfunction related steatohepatitis (MASH), fibrosis, cirrhosis, and hepatocellular carcinoma. The mechanism behind the complicated pathogenesis of MASLD is multifactorial and interrelated and includes insulin resistance, disturbances in lipid metabolism, oxidative stress, inflammation, genetic vulnerability, gut-liver axis changes. Even though MASLD may go unnoticed at the initial stages of its development, its progressive development may cause serious hepatic and extrahepatic complications, including cardiovascular disease, chronic kidney disease, and metabolic syndrome. Clinical assessment, laboratory studies, and imaging research are vital in the early diagnosis of the disease and prevention of its progression and better patient outcome. Treatment of MASLD is based on a holistic and multidisciplinary approach to treatment that includes lifestyle change, metabolic risk management, medication therapy, and supportive care. Also, non-modern systems like Ayurveda offer promising herbal treatments with hepatoprotective, antioxidant, and anti-inflammatory effects that can be used to supplement the conventional approach to treatment. Thus, earlier diagnosis, raise of awareness and combination of therapeutic strategies are also vital to the successful management of MASLD and its increasing health pandemic.
REFERENCES
Parbat, A. Y.; Malode, G. P.; Shaikh, A. R.; Panchale, W. A.; Manwar, J. V.; Bakal, R. L. Ethnopharmacological review of traditional medicinal plants as immunomodulator. World J Biol Pharm Health Sci 2021, 6 (2), 043–055



Mitali Gandhi, Gautam Gundecha, Naziya InamdarHerbal Therapeutic Approaches for Metabolic Dysfunction-Associated Steatotic Liver Disease, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2092-2108, https://doi.org/10.5281/zenodo.21294366
 10.5281/zenodo.21294366
10.5281/zenodo.21294366