
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Mathematics, M.G.C.G.V Chirakoot, Satna, Madhya Pradesh, India
Blood exhibits distinct non-Newtonian characteristics when flowing through narrow-diameter vessels at low shear rates, where red blood cells (RBCs) form aggregate structures called Rouleaux formations. During viral infections like Dengue, severe physiological changes occur—such as plasma leakage through microscopic vascular holes—which causes critical spikes in blood hematocrit (HCT) and abrupt shifts in blood pressure. This paper develops a mathematical model treating blood as a two-phase fluid consisting of a plasma layer and an RBC-rich core . The flow is governed by a power-law constitutive equation transformed into cylindrical coordinates to match renal artery dimensions (radius R = 0.00375 m), length of renal artery0.05 m, and flow flux (Q = 660 mL/min) . The Newton-Raphson numerical method is utilized to optimize and calculate the absolute value of the power-law index (n = 1.81702329). Using 7 days of longitudinal clinical data from a Dengue patient, a mathematical correlation between blood pressure drop and hematocrit was established as:?P=40.2327 H+764.25.The model successfully computes the Modulated Blood Pressure Drop (MBPD) and compares it with the Real Clinical Blood Pressure Drop (RBPD) alongside tracking radial profiles for velocity, shear stress, and strain rates across the vessel walls.
RENAL BLOOD VESSEL [1,2,3,4]
Renal Vascular Anatomy
Terminal End-Arteries: The intrarenal arterial system consists of end-arteries characterized by a complete absence of parenchymal anastomoses. Consequently, occlusion of any branch inevitably leads to localized tissue infarction. Dual Capillary Beds: The renal vasculature features a distinct portal-like architecture consisting of two sequentially arranged capillary networks: Glomerular Capillaries: A high-pressure network optimized exclusively for ultrafiltration. Peritubular Capillaries: A low-pressure network optimized for solute reabsorption and gas exchange around the tubular segments. Filtration Hemodynamics: The high-pressure state within the glomerular capillaries is precisely regulated by the structural resistance of both the afferent and efferent arterioles, which serve as the primary pre- and post-capillary control gates for the Glomerular Filtration Rate (GFR).
Renal Blood Flow (RBF) Dynamics
Perfusion Volume: The kidneys receive a disproportionately large share of the cardiac output (20–25%, equivalent to ~1000 mL/min or 400 mL/100g/min).
Intrarenal Perfusion Gradient:
Cortex: Receives 95% of total RBF to maximize filtration capacity. Medulla: Receives a restrictive 5% of total RBF. This low-velocity perfusion is a physiological necessity to prevent the washout of the hypertonic medullary urea gradient, thereby preserving the countercurrent mechanism required for urine concentration. Metabolic Paradox: The massive blood supply to the kidneys is driven by functional filtration demands rather than metabolic consumption. Consequently, the renal fractional oxygen extraction is exceptionally low (10–15%, consuming roughly 4 mL/100g/min).
Oxygen Dissociation Stability: Renal oxygen extraction remains remarkably constant despite fluctuations in RBF. This is because renal metabolic oxygen expenditure is directly proportional to GFR and the subsequent energetic workload of tubular sodium reabsorption. [Alex Yartsev 2020]
Macro-Anatomy of the Main Renal Trunk[5,6,7,8]
Aortic Origin and Dimensions: Each kidney is perfused by a primary renal artery, a major large-bore muscular branch arising directly from the abdominal aorta. Morphologically, these vessels typically span 4–5 cm in length and 5–10 mm in diameter, frequently demonstrating a slight physiological asymmetry in caliber between the left and right sides. Pre-Parenchymal Bifurcation: Immediately prior to penetrating the renal parenchyma, the main trunk bifurcates into distinct anterior and posterior main branches. These primary divisions subsequently branch into segmental arteries before entering the dense tissue of the organ.
Micro-Anatomy & Intrarenal Perfusion Architecture
Absolute End-Artery Architecture: Beyond the segmental transition, the intrarenal arterial tree maintains a strict end-artery configuration characterized by an absolute absence of collateral vascular networks or intra-parenchymal anastomoses (Bertram, 2000). Territorial Vulnerability to Ischemia: Because there are no secondary back-up connections between adjacent arterial segments, the occlusion or hypoperfusion of any single segmental branch leads directly to isolated, regional ischemia confined strictly to its specific anatomical territory of distribution.
The normal Peak Systolic Velocity (PSV) for a healthy main renal artery is between 60 and 150 cm/s. The End-Diastolic Velocity (EDV), which measures blood speed at the end of a heartbeat, normally ranges from 20 to 50 cm/s. The Renal-Aortic Ratio (RAR) is the renal artery velocity divided by the abdominal aorta velocity, with a normal value under 3.5. The Resistive Index (RI), indicating resistance within kidney tissue, typically falls between 0.50 and 0.70. Acceleration Time (AT), the time for blood to reach peak flow, should be less than 70 milliseconds. Abnormal diagnostic criteria -PSV exceeding 180 to 200 cm/s, suggesting kidney artery narrowing. RAR of 3.5 or more, indicating severe renal artery stenosis (>60% blockage).RI above 0.70, which implies intrinsic kidney damage or medical renal disease rather than artery blockage.AT delayed beyond 70 to 80 milliseconds, showing upstream blood flow restriction before reaching the kidney[12].
2. DENGUE DISEASE[13]
Dengue Fever (DF):This is the classic form of dengue where blood vessels remain stable. Hematocrit (Hct): Normal or slightly elevated. Any minor rise is due to mild dehydration from high fever. Blood Pressure (BP): Normal. The circulatory system functions perfectly fine, keeping readings near 120/80 mmHg.
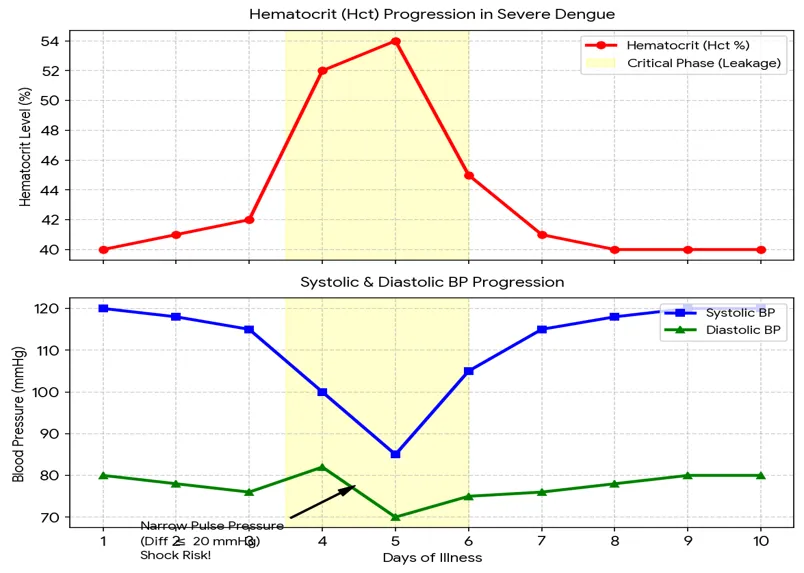
Dengue Hemorrhagic Fever (DHF)Microscopic holes develop in blood vessels, causing the liquid part of blood (plasma) to leak out. Hematocrit (Hct): Rises significantly ( 20% increase). As plasma leaks, the blood becomes severely thick. A baseline Hct of 40% will spike to 48% or higher. Blood Pressure (BP): Systolic drops and Diastolic rises. The top number drops from fluid loss. The bottom number rises as blood vessels squeeze to compensate. This creates a narrow reading like 100/80 mmHg.
Dengue Shock Syndrome (DSS):This is a medical emergency where the circulatory system crashes completely. Hematocrit (Hct): Either spikes critically or drops catastrophically. It peaks very high from extreme plasma loss, but it will suddenly crash to very low levels if severe internal bleeding occurs. Blood Pressure (BP): Severe Hypotension. The blood pressure drops completely. The gap between the top and bottom numbers narrows to 20 mmHg or less (e.g., 80/65 mmHg). In deep shock, it becomes unrecordable.
Febrile Phase (Days 1 to 3)Hematocrit: Remains baseline flat near 40%.Blood Pressure: Stable and wide apart (e.g., 120/80 mmHg), indicating a strong and healthy circulatory volume. Critical Phase & Shock Risk (Days 4 to 6)Hematocrit Spikes: Plasma leaks out of the vessels, causing the hematocrit curve to shoot upward sharply above 50%.BP Line Convergence: The top (systolic) line plummets due to severe volume loss, while the bottom (diastolic) line temporarily rises or stays firm due to vascular constriction. The gap between them constricts to 20 mmHg or less, signaling Dengue Shock Syndrome. Convalescence/ Recovery Phase (Days 7 to 10) Hematocrit Normalizes: The body naturally reabsorbs fluids, causing the blood thickness to dilute back down to a safe 40%. BP Stabilizes: The systolic and diastolic lines pull apart to a healthy, wide gap, normalizing blood circulation.
3. TWO PHASES OF BLOOD [14]
Blood exhibits remarkable non-Newtonian character when Several researchers studied the blood flow characteristics in the presence of stenoses in the lumen of the arteries (Ikbal et al., 2009; Sankar, 2010; Ismail et al., 2008). Blood behaves like a Newtonian fluid when it flows in larger diameter arteries at high shear rates. Many studies were carried out to analyze the steady and unsteady flow of blood in larger diameter arteries, treating it as Newtonian fluid (Liu et al., 2004; Chakravarty and Mandal, 2004; Sud and Sekhon, 1985). Blood exhibits remarkable non-Newtonian character when it flows through narrow diameter arteries at low shear rates and blood flow in narrow arteries is highly pulsatile, particularly in diseased state.
Low Shear Rate (< 100 s⁻¹) — Pure Non-Newtonian Behavior
This occurs when blood flows very slowly, such as in tiny capillaries, branching microvessels, or during the resting phase of the heart (diastole). At this low force, Red Blood Cells (RBCs) begin to aggregate and stick together, stacking like a pile of coins. This physical structure is called a Rouleaux formation. This crowding makes the blood highly viscous (thick). Because its viscosity changes with force, blood exhibits a specific Non-Newtonian trait known as Shear-Thinning (Pseudoplastic) behavior.
High Shear Rate (100 s⁻¹ to 200 s⁻¹) — Newtonian Transition
This occurs when blood moves at a high velocity through large blood vessels, such as the aorta or major arteries. The high fluid forces completely break apart the Rouleaux cell clusters. The individual red blood cells stretch out and align perfectly parallel to the direction of the flow. Once the shear rate crosses 100 to 200 s⁻¹, the viscosity levels off and becomes virtually constant (asymptotic). At this point, blood behaves mathematically as a standard Newtonian fluid. Since here the strain rate of renal artery is 12 to 37.5 so blood is showing a non-Newtonian behavior[15].
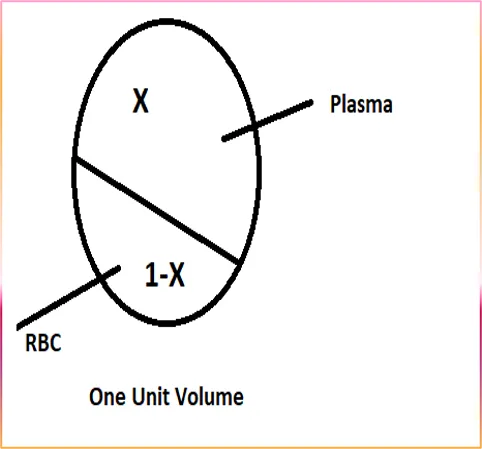
In this case blood divided into two phase by unit volume fluid.
4. REAL MODEL
4.1Parametrization
The blood's velocity


The coordinates





Flow pattern of two phase blood flow in artery vessel [16,17]
In our two phases of blood assumption
Let one unit volume of whole blood and
X= volume fraction of plasma
Y= 1-X
volume fraction of RBCthe mass ratio of RBC to plasma is m

where

we define density of blood mixture ρm
as follows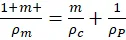
And viscosity of blood mixture ηm as follows

4.2 Boundary conditions.
1. The velocity of blood flow on the axis of blood vessels at r = 0 will be maximum and finite, say v0= maximum velocity.
2. The velocity of blood flow on the wall of blood vessels at r = R, where, R is the radius of blood vessels, will be zero. This condition is well known as no slip condition.
4.3 Equation of Continuity
continuity equation for three phases

Where, vi is the common velocity of two phase blood cells and plasma. Again Xρcvi,i

is co-variant derivative of (Xρcvi)

with respect to Xi.
Equation of motion for blood flow with the three phases using the principle of force conservation (or momentum conservation) in hepatic arteries and assuming that the consistency coefficient (or viscosity coefficient) of RBC cells is ηc.
Yρc∂vi∂t+Yρcviv,ji-YP,jgij+Yηcgjkvi,k,j

Similarly, taking the viscosity coefficient of plasma to be the equation of motion for plasma will be as follows-
XρP∂vi∂t+XρPviv,ji-XP,jgij+XηPgjkvi,k,j

then equation of motion for blood flow with the all three phases will be as follows-
ρm∂vi∂t+ρmvj vi,j =-P,jgij+ηmgjkvi,k,j

Whenever percentage of blood is reduces the blood has been supposed Newtonian but in case of increasing the hematocrit, the effective viscosity of blood flowing through arteries remote from the heart depends on the strain rate.
For this reason,the blood will flow as non Newtonian fluid. When strain rate is in between 5 to 200 per second, the power law
τ'=ηmen

where 0.68≤𝑛 ≤0.80 Describes the flow of blood very well. The constitutive equation of blood is as follow
Blood's constitutive equation is as follows:
τij=-pgij+ηm(eij)n=-pgij+τ,ij

Where τij


4.4 Mathematical formulation
The equation of continuity for power law flow will be as follows:
1g(gvi),i=0

Again the equation in tensorial form is as follows:
ρm∂vi∂t+ρmvjvi,j=τij,j

Since the blood vessels are cylindrical, the above governing equation have to transformed into cylindrical co-ordinates.
Let x1=r, x2=θ, x3=z

Matrix of corresponding metric tensor in cylindrical form is as follow:
gij=1000r20001

So Matrix of conjugate metric tensor is
gij=10001r20001

Where as Christoffel’s symbols of 2nd kind are as follows:
122=-r, 221= 212= 1r

Contravarient and physical components of velocity of blood flow will be related as
g11v1=vr=> vr=v1

g22v2=vθ=> vθ= rv2,

g22v3=vz=> vz= v3

Further the physical component of -p,jgij are-giip,jgij

The matrix of physical component of shearing stress – tensor
τ,ij =ηm(eij)n=ηm(gikv,ki+gjkv,kj)n

will be as follows :
00ηm(dvdz)n000ηm(dvdr)n00
The covariant derivative of τ,ij

τ,j,ij= 1g∂∂xjgτ,ij+ijkτ,kj

Keeping in view the above facts the governing tensorial equation can be transformed into cylindrical form which are as follows :
The Equation of continuity –
∂v∂z=0

The Equation of motion –
r

-∂p∂r=0

θ

0=0

Z-Component
0=-∂p∂z+ηmr ∂∂rrdvdrn
These are the r


Further the fact has been considered that axial flow in artery is symmetric, so that vθ=0 and vr , vz and p


∂p∂t=∂vr∂t=∂vθ∂t=∂vz∂t=0

On integrating equation,we get vz=vr


The integration of equation of motion, we get p=pz


Now, with the help of equation, the equation of motion converts in the following form:
0=-dpdz+ηmr ddrrdvdrn

The pressure gradient -(dpdz)=P

ddrrdvdrn=- Prηm

On integrating equation (9), we get
rdvdrn=-Pr22ηm+A

We know that the velocity of blood flow on the axis of the cylindrical arteries is maximum and constant. So that the apply the boundary condition at r=0, v = V0(

-dvdr=Pr2ηm1n

Integrating equation once again, we get
v=-P2ηm1n r1n+1(n+1)n+B

To determine the arbitrary constant B, we apply the no –slip condition n the inner wall of the arteries : at r=R, V=0,

B=P2ηm1n nR1n+1n+1

Hence the equation takes the following form:
v=P2ηm1n nn+1R1n+1-r1n+1

Which determines the velocity of blood flow in the arteries remote from the liver where P is gradient of blood pressure and ηm

Shear stress
τ=Q1+3nπnnrηmR3n+1

Strain rate
dvdr=∆Pr2∆z ηm1n

The total flow- flux of blood through the transverse section of the arteries is
Q=0Rv.2πr dr=0RP2ηm1n.1n+1R1n+1-r1n+12πr dr

=P2ηm1n.2πnn+1R1n+1.r22-n.r1n+33n+10R
=P2ηm1n.2πnn+1.n+1R1n+323n+1

Q= P2ηm1n.πnR1n+33n+1 , where P= -dpdz

Q=Pi-Pf2ηm(zi-zf)1n.πnR1n+33n+1

5. RESULT & DISCUSSION
Table (a): Pathological Data of Dengue Patient
|
DAY |
Hgb |
HCT |
B.P (mmHg) |
Pressure drop (∆p) 
|
|
1 |
13.40 |
40.2 |
113/66 |
23.5 |
|
2 |
13.82 |
41.46 |
110/67 |
21.5 |
|
3 |
14.01 |
42.03 |
109/69 |
20 |
|
4 |
14.03 |
42.09 |
106/71 |
17.5 |
|
5 |
14.25 |
42.75 |
105/72 |
16.5 |
|
6 |
14.40 |
43.2 |
103/73 |
15 |
|
7 |
14.16 |
42.48 |
103/73 |
15 |
Equation of viscosity
ηm=Yηc+XηP

0.0045=ηc42.03100+0.00141-0.4203

ηc=0.0087756840

Let,H = 42.03
ΔP=Pi-Pf=2457.08 pascal

According to Glenn Elert (2010)
ηm =

According to Gustafson, Daniel R. (1980)
ηp=

ηm=Y×ηc+XηP

where Y=H100

ηm=H100×ηc+(1-H100)ηP

ηm=0.0087756840H100+0.00141-H100

ηm=7.37×10-5 H+0.0014

Q=660[18]mlmin=1.1×10-5 m3/sec

radius R=0.00375 meter

length of renal artery Δz=0.05 meter

Q=Pi-Pf2ηmzi-zf1n.πn R1n+33n+1

By Newton-Raphson method find value of n
def get_newton_raphson(x):
fx = log(x) - log(1+(3*x)) + (4.311238036/x) - 1.822421518
fx_prime= (1/x)-3/(1+(3*x))-(4.311238036/x**2)
delta = fx/fx_prime
x_new = x - delta
return x_new, delta
def get_optimized_value(x_init, n_iteration, eps):
for i in range(n_iteration):
try:
x_new, delta = get_newton_raphson(x_init)
print(x_new)
temp = x_new
if abs(delta)<=eps:
n_iteration = i+1
break
x_init = x_new
except:
x_new = x_init
n_interation = i
print(f"wrong initial guess: getting x_new = {temp} at {n_interation} iteration")
break
abs_per_error = abs((x_new-x_init)/x_new)
return x_new, n_iteration, abs_per_error
if __name__=="__main__":
x_init = 1
n_interation = 2000
eps = 0.00000000001
1.464576690641444
1.759308823795298
1.8173835235248155
1.817008976812434
1.8170238619375374
1.817023273466403
1.8170232967359778
1.8170232958158503
1.8170232958522339
1.8170232958507955
x: 1.8170232958507955, n: 10, abs_per_error: 7.916271376316284e-13
here we will take absolute value
n=1.81702329

Further find a mathematical relation between pressure drop and hematocrit
∆P=40.2327 H+764.25

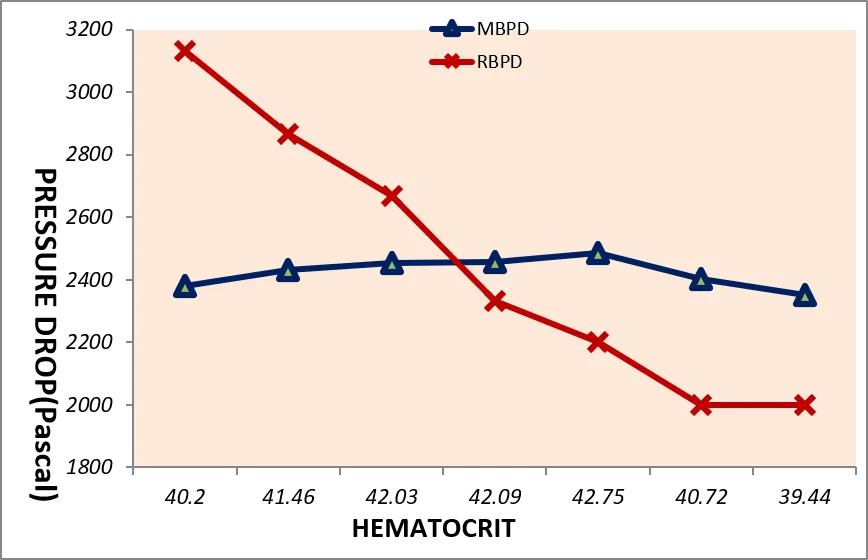
Table (B): Modulated Blood Pressure Drop
|
DAY |
HCT |
Modulated BPD (pascal) |
Real Clinical BPD (pascal) |
|
1 |
40.2 |
2381.57 |
3133.25 |
|
2 |
41.46 |
2432.26 |
2866.59 |
|
3 |
42.03 |
2455.20 |
2666.6 |
|
4 |
42.09 |
2457.61 |
2333.27 |
|
5 |
42.75 |
2484.16 |
2199.94 |
|
6 |
40.72 |
2402.52 |
1999.95 |
|
7 |
39.44 |
2351.02 |
1999.95 |



TABLE (c) r/R v/s shear stress
|
r/R |
STRESS |
|
0 |
0 |
|
0.1 |
0.0672 |
|
0.2 |
0.1744 |
|
0.3 |
0.3027 |
|
0.4 |
0.4564 |
|
0.5 |
0.3914 |
|
0.6 |
0.8542 |
|
0.7 |
1.105 |
|
0.8 |
1.402 |
|
0.9 |
1.733 |
|
1 |
2.102 |

Table (d) radius v/s velocity
|
RADIUS |
VELOCITY |
|
0 |
0.7569 |
|
0.005 |
0.7318 |
|
0.001 |
0.6834 |
|
0.0015 |
0.619 |
|
0.002 |
0.5416 |
|
0.0025 |
0.4526 |
|
0.003 |
0.3532 |
|
0.0035 |
0.2442 |
|
0.004 |
0.1263 |
|
0.0045 |
0 |

Table (e) radius v/s strain rate
|
Radius |
Strain Rate |
|
0.0025 |
188.7 |
|
0.0027 |
196.87 |
|
0.0029 |
204.76 |
|
0.0031 |
212.42 |
|
0.0033 |
219.86 |
|
0.0035 |
227.09 |
|
0.0037 |
234.14 |
|
0.0039 |
241.03 |

Table (f) p-value table
|
Variable |
Mean |
SD |
P-value |
|
Modulated BPD |
2423.48 |
47.22 |
0.847 |
|
Real clinical BPD |
2457.08 |
441.25 |
0.847 |
|
HCT |
41.24 |
1.17 |
- |
Statistical Interpretation:
The paired t-test showed a p-value = 0.847.Since p > 0.05, there is no statistically significant difference between Modulated BPD and Real Clinical BPD values.
6. CONCLUSION
The comprehensive hemodynamic investigation presented in this study yields several key findings: Because the calculated strain rate of the renal artery falls within limit (<100 per sec ) blood deviates from Newtonian properties and operates strictly under non-Newtonian power-law behavior. Applying the Newton-Raphson algorithm accurately identifies the characteristic fluid flow behavior index as n=1.81702329 under the prescribed physiological constraints. The progression of Dengue directly elevates blood hematocrit over the course of the illness, peaking around day 5 to 6. This spike thickens the blood mixture, alters effective fluid viscosity, and causes significant deviations between modulated and real clinical pressure drops. Fluid velocity peaks perfectly along the center axis (r=0) and terminates at zero on the arterial wall due to the no-slip boundary condition. Conversely, shear stress exhibits an inverse relationship, rising to its maximum profile of (2.102) at the vessel wall interface (r/R = 1).here value of hct is rising to till 5 days so in these days we will decrease the drug dose and after we will increase the drug dose rapidly. Overall, this mathematical approach provides a quantitative tool for clinicians to evaluate internal organ perfusion drops and circulatory risks using simple, routine blood test markers like hematocrit.
REFERENCES

Bhaskar Pandey, V. Upadhyay, Mathematical Modeling of Two-Phase Non-Newtonian Blood Flow by Power Law in the Renal Artery with Hemodynamic Analysis of Dengue Patient, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2854-2866. https://doi.org/10.5281/zenodo.20636279
 10.5281/zenodo.20636279
10.5281/zenodo.20636279