Diabetic neuropathy is a common and dangerous consequence of diabetes. It arises as a result of chronic and uncontrolled hyperglycemia, which causes structural and functional damage to peripheral nerves. Diabetic neuropathy affects a substantial percentage of people with long-term diabetes and has a severe influence on their quality of life. Persistently elevated blood glucose levels generate a combination of metabolic and vascular alterations, resulting in oxidative stress, microvascular damage, and gradual nerve fiber degeneration. Diabetic neuropathy is clinically defined by a range of symptoms, including numbness, tingling sensations, scorching pain, stabbing pain, and loss of sensation, primarily in the feet and lower limbs .These symptoms may gradually progress and can lead to impaired sensation and reduced motor function. In advanced stages, the loss of protective sensation increases the risk of foot injuries, ulcers, infections, and in severe cases may lead to amputation. The development of diabetic neuropathy is influenced by several risk factors such as poor glycemic control, long duration of diabetes, obesity, hypertension, and dyslipidemia.This article provides an overview of the pathophysiology, clinical manifestations, diagnosis, and current therapeutic approaches for diabetic neuropathy, highlighting the importance of early detection and comprehensive management to improve patient outcomes.
A variety of clinical and subclinical symptoms with varying anatomical distributions, clinical histories, and potentially distinct underlying pathogenetic pathways are together referred to as diabetic neuropathy. Diffuse or focal damage to peripheral somatic or autonomic nerve fibers arising from diabetes mellitus characterizes each, while indistinguishable symptoms may arise idiopathically or in conjunction with other illnesses in people without diabetes [1,3,34].
Distal symmetric sensorimotor neuropathy, often known as diabetic peripheral neuropathy, or DPN, is the most prevalent type and the most common neurological consequence of diabetes mellitus [2,3,34].
Diabetic neuropathy (DN) occurs when certain indications or symptoms suggest neuropathy in people with diabetes mellitus (DM) after other sources of neuronal damage have been ruled out [3].Loss of Schwann cells, myelinated axons, and a population of sensory neurons in the dorsal root ganglia are signs of diabetic neuropathy (DN), which is caused by hyperglycemia-induced damage to the peripheral nervous system [4,41] .Diabetic neuropathy is characterized by persistent albuminuria, elevated blood pressure, decreased glomerular filtration rate (GFR), and a substantial risk of cardiovascular morbidity and mortality [5,6].
Distal symmetric polyneuropathy (DSPN) is the most prevalent type of this long-term diabetic consequence. The prevalence of DSPN rises with age and the length of diabetes, and it is usually diagnosed in patients with poor glycemic control. Autonomic neuropathy frequently coexists with this type of neuropathy. Because of its variable clinical presentation and unique symptoms, DSPN is frequently diagnosed at an advanced stage [7,8].According to a UK study , 22.7% of people with type 1 diabetes have DN, as do 65% of insulin-treated DM patients and 59% of those using oral antidiabetic medications. Other investigations showed that the DN prevalence in patients with type 2 diabetes was 32.1% [8] .By 2045, the global diabetes patient population is predicted to reach 783 million.By 2050, the global diabetes population is expected to be 1.31 billion [9] .The most frequent microvascular complication in people with diabetes mellitus is diabetic neuropathy (DN); after 20 years of disease progression, over 50% of DM patients have this problem, which significantly affects their quality of life given the characteristic persistent discomfort in their lower limbs [10,11,12]. Painful diabetic neuropathy (PDN), which exacerbates impairment, can occur in up to one-third of diabetic patients. Strict glycemic control is therefore the main emphasis of PDN treatment in order to prevent the disease's progression and manage discomfort. Patients with PDN spent US$7066 more per year than those without pain, according to one study, underscoring the substantial financial burden [13,14,15].
In the therapeutic setting, PDN frequently entails polypharmacy, emphasizing the difficulties of achieving pain management with single drugs.Among small problems like retinopathy, nephropathy, and ischemic heart disease, diabetic neuropathy is the most common [16,34,40].The rate of occurrence varies by type of diabetes.Neuropathy is more common in people with type II diabetes mellitus (T2DM) (6.1%) than in those with type I diabetes (T1DM) (2.8%), according to numerous epidemiologic research [16,17]. Due to its high incidence in those with long-term diabetes, diabetic neuropathy is still a serious health concern. A patient's quality of life may be significantly impacted by the increasing damage to peripheral nerves, which could result in serious problems if left untreated. In order to lower associated risks and delay the disease's course, early detection and effective treatments are critical. The therapy of diabetic neuropathy depends critically on quick diagnosis, appropriate glucose control, and successful treatment approaches. To improve patient care, it is crucial to comprehend the underlying mechanisms, clinical symptoms, and accessible therapeutic options. An overview of diabetic neuropathy's pathogenesis, clinical characteristics, diagnosis, and treatment is what this Article seeks to provide.
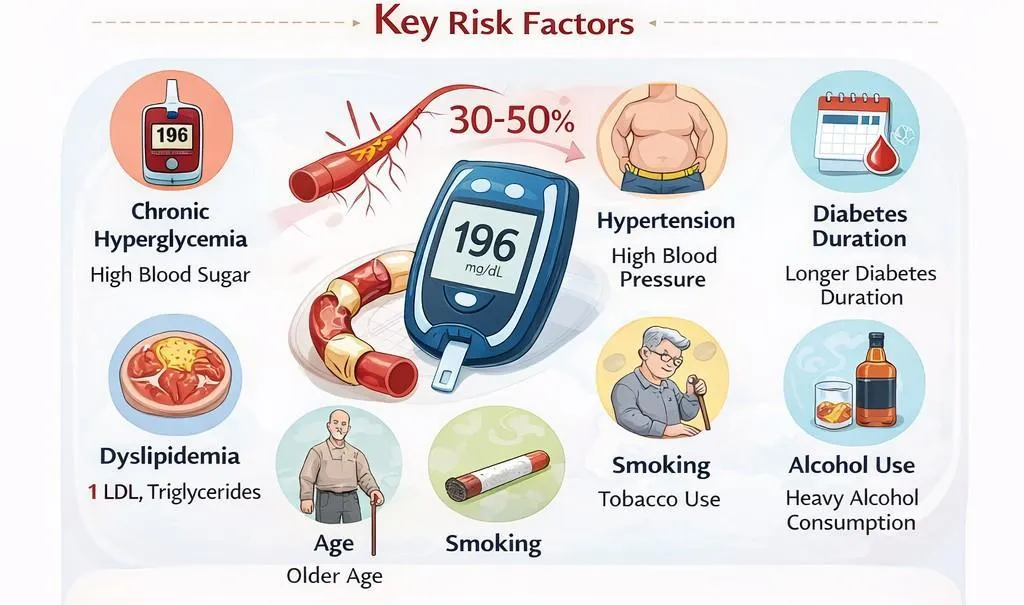
2 . RISK FACTORS FOR DIABETIC NEUROPATHY
Major risk factors contributing to Diabetic Neuropathy [Fig. 1].
Hyperglycemia is considered the primary risk factor for the development of diabetic neuropathy. Improved glycemic control has been shown to delay or prevent the progression of neuropathy, particularly in patients with type 1 diabetes. However, strict glucose control is less effective in preventing distal polyneuropathy in individuals with type 2 diabetes [18]. Several clinical trials have demonstrated that tight regulation of blood glucose levels can slow the progression of diabetic peripheral neuropathy in both type 1 and type 2 diabetic patients [19,41]. Furthermore, observational studies have reported long-term and sustained benefits of intensive glycemic control in patients with type 1 diabetes .
In individuals with both type 1 and type 2 diabetes, height has been shown to be an independent predictor of neuropathy and is regarded as a marker for neuronal length [20].
Since high levels of total cholesterol, triglycerides, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) are linked to an increased risk of neuropathy, dyslipidemia is another risk factor that may contribute to the development of DN. Triglycerides have the biggest impact on the risk of neuropathy out of all the lipid fractions [21].
Despite longer diabetes duration, strict metabolic control over an extended period of time may lower the occurrence of DSPN, particularly in type 1 diabetes (T1D) [22].In a 24-year follow-up of T1D patients, 64% of patients with insufficient control developed verified clinical DSPN, compared to 0% of patients with strict control [23]. The age of onset varies widely; some individuals get DSPN after having diabetes for a long time, while others show this consequence as early as the prediabetic stage [24].
In diabetic patients, being overweight is linked to increased insulin resistance, persistent inflammation, and metabolic abnormalities that may exacerbate nerve damage[25].Peripheral neuropathy is more common in obese diabetics than in people with normal body weight, according to studies [26,27,4].
Another significant risk factor linked to diabetic neuropathy is hypertension. Chronically high blood pressure can cause ischemia damage and gradual nerve dysfunction by reducing blood supply to peripheral nerves and impairing microvascular circulation [28,29,30,31] The risk of having neuropathic consequences is greatly increased when diabetes and hypertension combine [31,32].
The onset and advancement of diabetic neuropathy are also associated with lifestyle choices including drinking alcohol and smoking cigarettes. Neuropathic consequences may worsen as a result of these variables' direct toxic effects on nerve tissues and vascular injury [32,33].
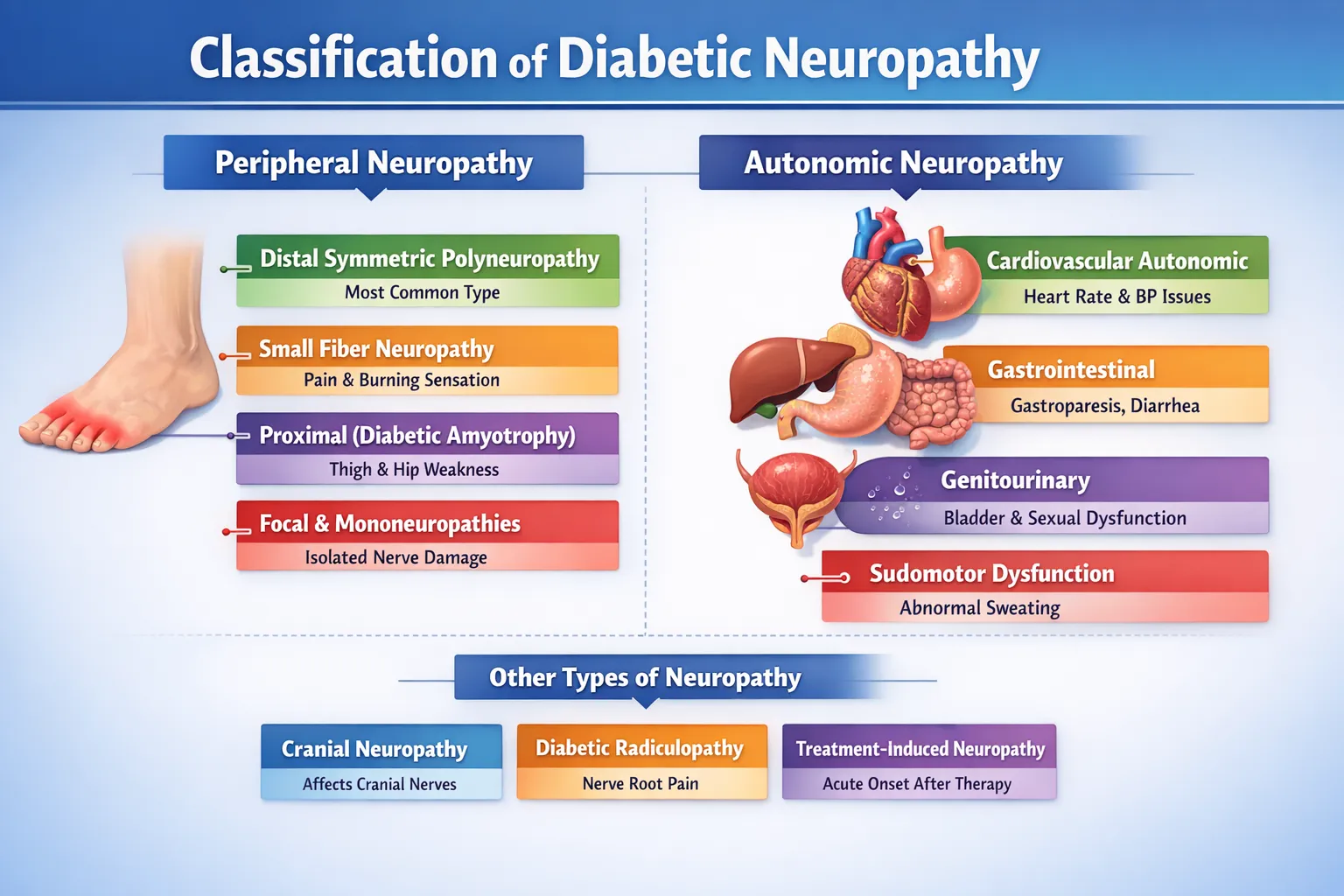
3. CLASSIFICATION OF DIABETIC NEUROPATHY
Diabetic neuropathy can present in various forms depending on the affected nerves and clinical features. It is broadly classified into different types, as summarized in Figure 2.
Classification of diabetic neuropathy to guide diagnosis and management based on affected nerve types and clinical presentation [Fig.2].
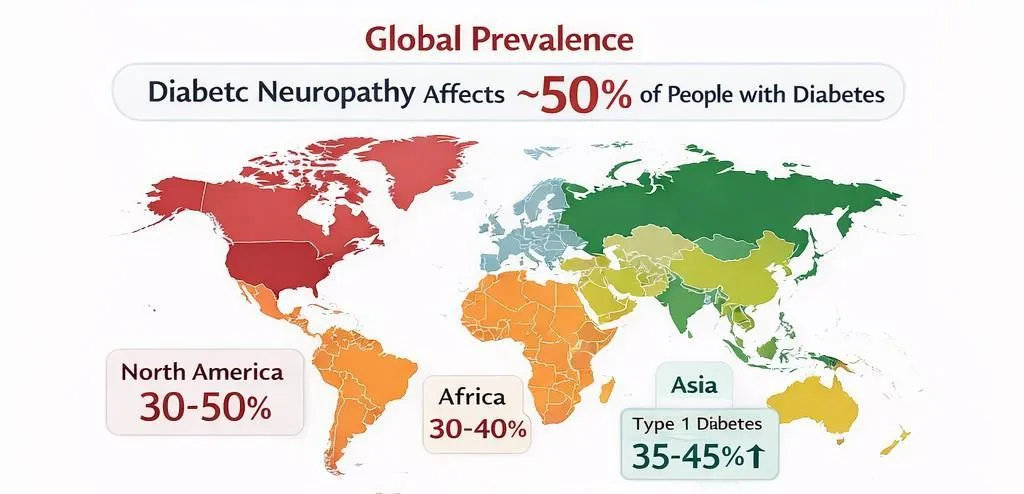
4. EPIDEMIOLOGY OF DIABETIC NEUROPATHY
Diabetic neuropathy is one of the most prevalent chronic consequences of diabetes mellitus and a leading source of morbidity among diabetic people globally [11,12]. It is believed that nearly 50% of diabetics acquire diabetic neuropathy at some point in their lives, making it one of the most commonly reported problems [2,34,40].The disorder typically affects peripheral nerves and is frequently linked to long-term metabolic problems produced by chronic hyperglycemia. The frequency of diabetic peripheral neuropathy varies significantly across populations and studies. According to research undertaken in the United States and Europe, the prevalence varies between 6% and 51%, depending on the diagnostic criteria utilized, study design, and patient demographic characteristics [35].These discrepancies could be brought about by variances in screening techniques, the length of diabetes, glycemic control, and research group demographics.
Diabetic peripheral neuropathy is thought to be the most prevalent type of neuropathy in the world, and it greatly lowers the quality of life and causes impairment in people with diabetes [36]. Patients with type 2 diabetes are more likely than those with type 1 diabetes to develop diabetic peripheral neuropathy due to delayed diagnosis and prolonged exposure to metabolic risk factors[37].Symptoms including numbness, tingling, scorching pain, and lack of sensation are common in patients with this illness, especially in the lower extremities. These symptoms might make it difficult to go about everyday tasks and raise the possibility of problems like infections and foot ulcers.According to systematic reviews and meta-analyses, between 22% and 46% of diabetes people worldwide have diabetic peripheral neuropathy [38]. This high incidence underscores the disease's significant worldwide impact and shows the necessity of early detection and effective care techniques to stop the disease's progression.Additionally, there are notable regional variations in the prevalence of diabetic neuropathy. Prevalence rates, for instance, have been found to be 8.4% in China, 29.2% in India, 48.1% in Sri Lanka, and 71.1% in Nigeria[39].Genetic factors, lifestyle choices, access to healthcare, and population-specific variances in diabetes management techniques may all have an impact on these discrepancies. The onset and course of diabetic neuropathy are known to be influenced by a number of factors. An increased risk of neuropathic consequences is highly correlated with longer duration of diabetes, poor glycemic control, aging, and the presence of other metabolic illnesses [40].
The burden of diabetic neuropathy is predicted to rise along with the global prevalence of diabetes, underscoring the significance of good management and preventive measures.
Epidemiology of diabetic neuropathy: Prevalence varies globally, affecting 22–65% of diabetic patients, influenced by diabetes type, duration, and regional factors [Fig .3].
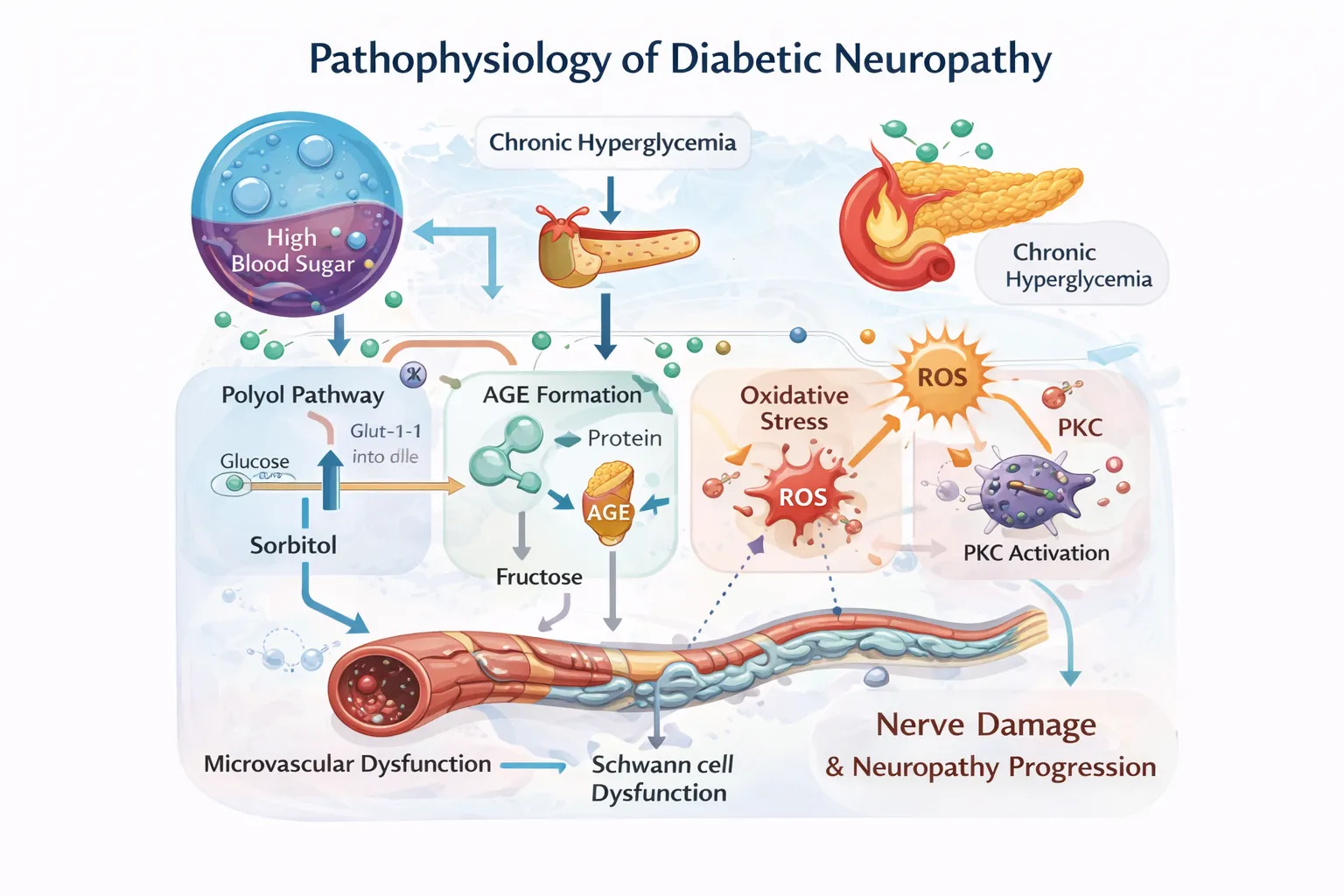
5. PATHOPHYSIOLOGY OF DIABETIC NEUROPATHY
Diabetic neuropathy's etiology is complex, involving several metabolic and vascular pathways that are caused by prolonged hyperglycaemia. Persistent elevations in blood glucose levels cause metabolic changes that harm nerve cells and supporting tissues. These metabolic abnormalities cause anatomical and functional damage to peripheral nerves [41] .
5.1. Chronic hyperglycemia: It is evident that hyperglycemia is a major factor in the onset and development of diabetic neuropathy as well as the other microvascular problems associated with diabetes [41,42].The polyol route, advanced glycation end-products (AGE)-receptor for AGE (RAGE) axis, hexosamine biosynthetic pathway, and protein kinase C (PKC) activation are among the most extensively researched mechanisms involved in hyperglycemia-induced brain injury [42]. In the most severe forms of DN, chronic hyperglycemia damages Schwann cells, resulting in demyelination. Because axons and Schwann cells interact and support one another, damage to the latter would also result in different changes to the axons [43,44].
5.2 . Polyol pathway activation: When intracellular glucose levels grow too high, the polyol pathway provides an alternate route for glucose metabolism. The enzyme aldose reductase converts glucose into sorbitol during hyperglycemia. Activating this route alters the redox balance of NADP⁺ and NADPH, leading to oxidative stress and neuronal damage in diabetic neuropathy [45,46].NADPH is consumed when aldose reductase is activated, which weakens the body's defenses against oxidative stress. After sorbitol is metabolized into fructose by sorbitol dehydrogenase, NAD is changed into NADH [46].
5.3 . Advanced glycation end product (AGE) formation in hyperglycemia : When proteins or lipids come into contact with aldose sugars, they undergo nonenzymatic glycation and oxidation, resulting in changes known as advanced glycation end products (AGEs) [47,48,49].Reduced blood flow to peripheral nerves and microvascular dysfunction are caused by the buildup of advanced glycation end products [50].
5.4 . Protein kinase C activation: In diabetic complications, hyperglycemia raises intracellular levels of diacylglycerol (DAG), which activates protein kinase C and causes vascular damage [51].Diabetic neuropathy is exacerbated by protein kinase C activation, which impairs endothelial function and lowers nerve blood flow [52] .
5.5 . Oxidative stress: In diabetic neuropathy, oxidative stress lowers blood flow to peripheral nerves and exacerbates endothelial dysfunction [53] .Elevated oxidative stress triggers inflammatory pathways and exacerbates neuronal damage [54].Neuronal dysfunction is exacerbated by oxidative stress, which causes lipid peroxidation and protein degradation in nerve cells [55].
In conclusion, persistent hyperglycemia activates multiple interrelated metabolic pathways, including the polyol pathway, AGE production, protein kinase C activation, and oxidative stress. These pathways all contribute to neuronal damage, microvascular dysfunction, and the progression of diabetic neuropathy.
Pathophysiological mechanisms involved in Diabetic Neuropathy [Fig.4]
6. CLINICAL MANIFESTATIONS
Diabetic neuropathy can present with a wide spectrum of sensory, motor, and autonomic disturbances.
Autonomic abnormalities, such as decreased heart rate variability and baroreflex sensitivity, can be a clinical symptom of diabetic neuropathy. These abnormalities were more severe in patients with confirmed neuropathy [56].While motor involvement is rare, diabetic neuropathy typically manifests as a combination of positive sensory symptoms like burning and tingling as well as negative symptoms like numbness and sensory loss [57].Neuropathic pain, which can become chronic and incapacitating, is reported by about 20% of individuals with distal symmetric polyneuropathy and about 25% of individuals with distal symmetric polyneuropathy (DSPN) have painful diabetic neuropathy due to small fiber involvement [58,59].Additionally, diabetic neuropathy may lessen the perception of ischemic discomfort, delaying the detection of myocardial infarction that is quiet or asymptomatic [60] .Autonomic neuropathy can result in reduced exercise tolerance, edema, paradoxical supine or nocturnal hypertension, and heat intolerance due to impaired thermoregulation [61].According to a recent comprehensive study, individuals with painful diabetic neuropathy had significant prevalence of psychiatric comorbidities, with anxiety ranging from 7.8% to 60.4%, depression from 13.6% to 50.6%, and coexistence of both illnesses in 26.4% to 30.6% of patients [62].Proprioceptive loss brought on by impaired peripheral sensory input might increase the risk of falls by causing sensory ataxia and imbalance [63].
7. DIAGNOSIS
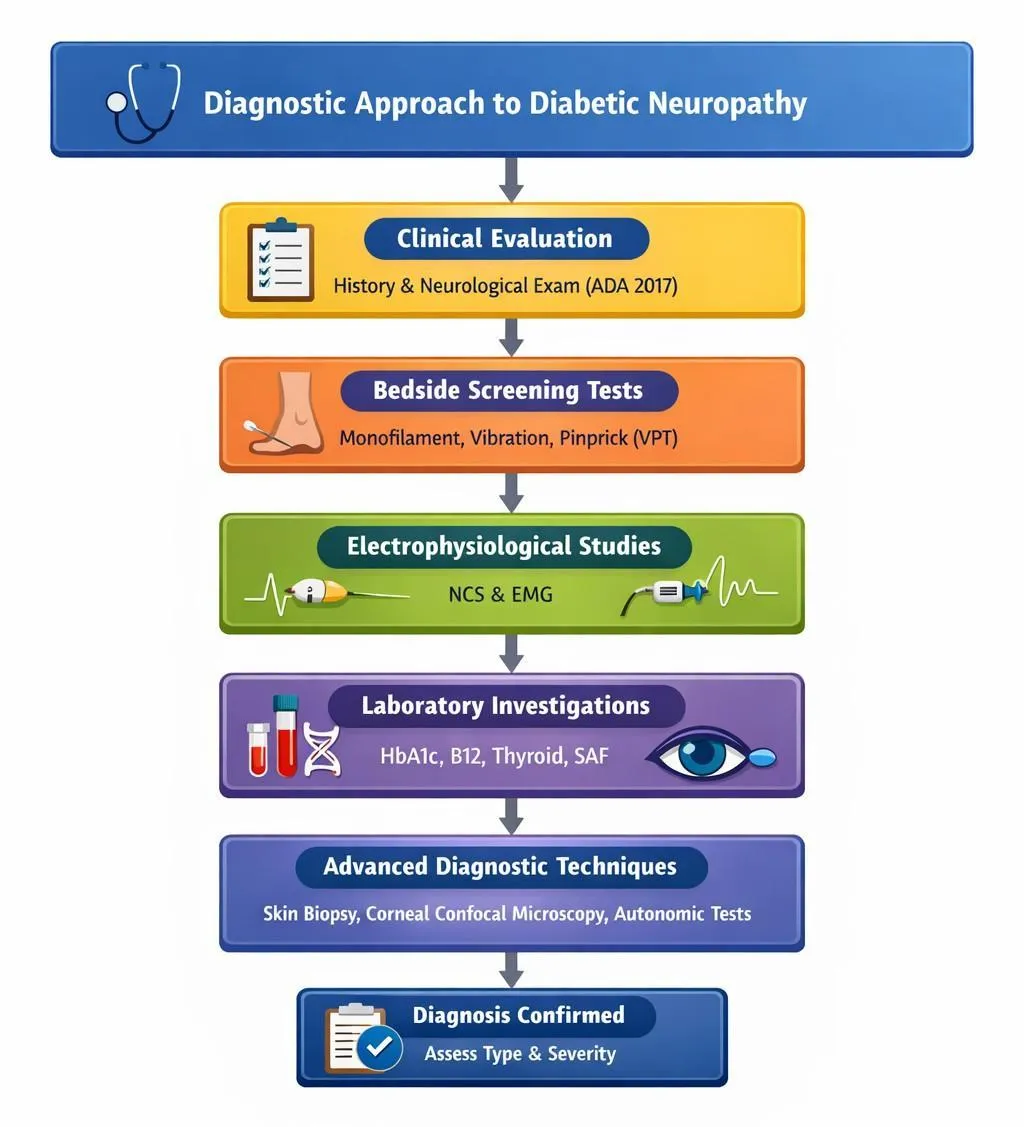
A methodical approach comprising clinical evaluation, bedside screening tests, electrophysiological studies, and laboratory investigations is essential for the accurate diagnosis of diabetic neuropathy. The aim of diagnosis is to confirm the presence of neuropathy, determine its type and severity, and exclude other potential causes.
Clinical Evaluation :
The diagnosis of diabetic neuropathy is mostly based on the patient's medical history and neurological examination including assessment of sensory, motor and automatic functions (ADA,2017) [64].
Bedside screening tests :
Bedside screening procedures,such as 10-g monofilament, large fiber function (vibration perception), and small fiber function (temperature and pinprick sensitivity) are commonly used for early detection.Vibration perception threshold (VPT) is a valuable and effective diagnostic tool for diagnosing diabetic peripheral neuropathy that, when supplemented with clinical examination procedures, increases diagnostic accuracy and is strongly associated with an increased risk of diabetic foot ulceration [65_67] .
Electrophysiological Studies:
The gold standard for verifying diabetic neuropathy is electrophysiological testing, particularly nerve conduction studies (NCS) and electromyography (EMG). In the distal lower limbs, nerve conduction studies (NCS) show reduced sensory nerve action potential amplitudes with a slight decrease of conduction velocities [68] .While big fiber involvement is easier to identify using electromyography (EMG), small fiber neuropathy frequently manifests as pain or dysesthesia but is challenging to identify using traditional nerve conduction investigations . Early or mixed-type DPN is often underdiagnosed because of the constraints of using either EMG or symptom assessment [69,70].
Laboratory investigations :
Laboratory tests such as fasting blood glucose, HbA1c, vitamin B12 levels, and thyroid function tests are essential to assess glycemic control and to exclude other metabolic or nutritional causes of neuropathy. Skin autofluorescence (SAF) has emerged as a non-invasive screening tool that reflects long-term metabolic status beyond conventional biomarkers such as HbA1c [71].
Advanced diagnostic techniques :
Skin biopsy is a valuable diagnostic tool used particularly for the evaluation of small fiber neuropathy. It involves a punch biopsy to assess intraepidermal nerve fiber density and helps in cases where routine nerve conduction studies are normal [72,73].A non-invasive method for early identification of diabetic neuropathy is corneal confocal microscopy, which makes tiny nerve fibers visible [74].Autonomic nerve system involvement in diabetic neuropathy is assessed by autonomic function tests, such as blood pressure response and heart rate variability [75].
Routine electrophysiological tests may not detect small fiber neuropathy, however advanced diagnostic techniques like skin biopsy, corneal confocal microscopy, and autonomic function testing help overcome these limitations.
Flowchart illustrating the key steps in diagnosing diabetic neuropathy [Fig.5].
8. TREATMENT / MANAGEMENT OF DIABETIC NEUROPATHY
8.1 . Pathogenesis oriented treatment
Glycemic control : It has been demonstrated that glycaemic management can effectively slow the development of diabetic neuropathy. Tight glycaemic control can delay the start and limit the progression of neuropathy, as determined by clinical examination, autonomic testing, and nerve conduction investigations, according to the diabetes control and complications trial, which included 1441 patients with type 1 diabetes [76,77] .Participants were split into two groups at random: a conventional group and an intensive HbA1c goal group (<6%) [78] .Intensive diabetes treatment decreased the incidence of microalbuminuria by 39% in the Diabetes Control and Complications Trial (DCCT) [79]. Interestingly, seven to eight years after the DCCT ended, patients randomly assigned to stringent glycemic control exhibited a persistent 40% decrease in the probability of developing microalbuminuria and hypertension [80].
Aldose reductase inhibitors : The enzyme that limits the pace of glucose metabolism in the polyol pathway is Aldose reductase. Hyperglycemia stimulates the activity of aldose reductase, resulting in decreased synthesis of the vasodilator nitric oxide and, eventually, ischemic nerve damage. Although aldose reductase inhibitors (ARIs) improved nerve conduction velocity, myelinated nerve fiber density, and regeneration clusters in sural nerve biopsies, they routinely failed in phase III clinical trials [81,82,83].Aldose-reductase inhibitors, however, are not included in the ADA guidelines since a meta-analysis comprising 32 trials showed that the drug is no more beneficial than a placebo in reducing DN symptoms and nerve conduction [84].
a - lipoic acid : α-lipoic acid (ALA) may lower oxidative stress, which is a critical component in the etiopathogenesis of DN [85]. In the "Alpha-Lipoic Acid in Diabetic Neuropathy" (ALADIN) research, individuals with symptomatic DN received intravenous ALA at a dose of 600 or 1,200 mg daily for three weeks; this treatment decreased DN symptoms without causing any notable side effects [86].The study found that α-lipoic acid improved positive neuropathic symptoms by 24.1% compared to placebo, but did not significantly affect the neuropathy impairment score [87].
Benfotiamine : A synthetic version of vitamin B1 that is very soluble in fats is called benfotiamine. Thiamine is recognized as a cofactor of an enzyme called transketolase, which is involved in the pentose-pathway metabolism of fructose-6 phosphate and glyceraldehyde-3 phosphate, converting them to pentose-5 phosphates and other sugars [88].In a phase III placebo-controlled trial involving 165 patients treated with benfotiamine for 6 weeks, the primary outcome measure (Neuropathy Symptom Score) improved in the per-protocol arm compared to placebo, but there was no improvement in the study's intent-to-treat arm [89] .Other studies have demonstrated that benfotiamine, when combined with pyridoxine, not only decreases DN symptoms but also increases the speed of nerve transmission [90].
8.2 . Symptomatic treatment
The goal of symptomatic treatment is to enhance quality of life by considerably reducing self-reported lower limb pain by 30–50% [91].Management primarily involves the use of pharmacological agents targeting neuropathic pain, along with supportive and non-pharmacological interventions.
Antidepressants: Antidepressants are widely regarded as first-line medications for the treatment of diabetic neuropathic pain (DNP). Duloxetine, a serotonin–norepinephrine reuptake inhibitor (SNRI), has shown strong clinical efficacy and holds a Level A recommendation. It is approved in the United States for managing this condition. Furthermore, clinical evidence indicates that duloxetine is also beneficial in treating other chronic pain disorders, including fibromyalgia and chronic musculoskeletal pain [92,93].Based on results from extensive randomized controlled studies, the US Food and medication Administration authorized duloxetine, an SNRI, as the first medication for DPN in 2004.In the first placebo-controlled double-blind experiment, individuals treated with duloxetine at 60 mg and 120 mg experienced considerable improvement in average pain scores that persisted throughout the research [94].
Venlafaxine is another SNRI that has been evaluated in the context of DPN and found to be effective, despite the fact that the FDA has not approved it for this use. Venlafaxine has been observed to be superior to placebo in treating the symptoms of pDPN at doses over 150 mg per day. However, clinically significant ECG alterations were reported in seven patients [95].
Anticonvulsants :The Food and Drug Administration (FDA) approved pregabalin as the first anticonvulsant to treat postherpetic neuralgia, DNP, and neuropathic pain following spinal cord injury [96-98].Pregabalin is a stronger gabapentinoid having a similar mechanism of action to gabapentin [99].The daily dosage is between 150 and 300 mg [100].Positive results with more than 30–50% pain reduction have been observed in numerous investigations [101].This group of agents also includes gabapentin Its therapeutic aim is identical to that of pregabalin [102].Gabapentin, which mimics the activities of the neurotransmitter GABA, is considered to function by inhibiting the α2δ unit of the calcium channel, leading to pain relief. It is currently extensively suggested in guidelines for treating PDN [103].
8.3 . Opioids and atypical opioids
Tapentadol : A centrally acting analgesic that inhibits norepinephrine reuptake and acts as an opioid agonist. It may be considered in refractory situations, although there are concerns of dependence and side effects [104].Based on findings from two clinical trials where patients titrated with an appropriate dose of tapentadol were arbitrarily asked to either continue with that dose or switch to a placebo, the FDA approved prolonged-release tapentadol for painful DSPN [104,105].
Tramadol : Tramadol is primarily a µ receptor agonist that inhibits serotonin and norepinephrine reuptake. In a multicenter, outpatient, double-blind, parallel-group research, Harati et al. randomly assigned 131 patients to receive tramadol or a placebo. They discovered that an average dose of 210 mg/day tramadol provided significant pain alleviation as measured by a Likert scale, as well as enhanced respondents' social and physical functioning. These advantages continued during the open-label extension of the 6-week experiment. Higher tramadol doses, on the other hand, were linked to more common side effects such as nausea (23%), constipation (21%), and headache (17%) [106].
8.4 . Topical therapies
Lidocaine 5% patches (Lidoderm) and capsaicin cream (Zostrix) are common topical therapies for diabetic peripheral neuropathic pain.
Capsaicin cream : Topical capsaicin may be a viable alternative to centrally acting oral neuropathic medicines. Capsaicin is the key chemical in red peppers, and it has antioxidant and antiinflammatory qualities. Capsaicin is currently available in two forms for analgesia: a topical 0.025 to 0.075% cream and an 8% high concentration patch. The United States Food and Drug Administration recently approved the capsaicin dermal patch for the treatment of DPN [107,108].
Lidocaine patches : Neuronal sodium channels are blocked by lidocaine patches [109]. The blockage increases the threshold for peripheral sensory neuron firing and decreases ectopic discharges [110].This medicine has been the subject of minor effectiveness trials. An NNT of 4.4 for a 50% reduction in pain was found in a 2003 RCT. The majority of side effects are dermatological and go away after the patch is removed. The main benefit of topical therapy is that it can be administered at any point to systemic therapy .
CONCLUSION
Diabetic neuropathy is a highly prevalent and disabling complication of diabetes mellitus, associated with significant morbidity and increased healthcare burden. Although diabetic neuropathies differ in clinical course, distribution, fiber involvement, and underlying pathophysiology, the two major forms include painful neuropathy and autonomic neuropathy. The condition arises primarily due to chronic hyperglycemia, leading to complex metabolic and vascular changes that result in progressive nerve damage.
At present, effective pathogenetic treatments remain limited, with strict glycemic control being the primary strategy to delay the onset and progression of diabetic peripheral neuropathy. Current management is largely focused on symptomatic relief using pharmacological therapies aimed at reducing neuropathic pain and improving quality of life.
Early diagnosis, appropriate therapeutic intervention, and continuous monitoring are essential to minimize complications such as foot ulcers, infections, and amputations. Further research is needed to develop targeted therapies addressing the underlying mechanisms of nerve injury, thereby improving long-term outcomes in patients with diabetic neuropathy.
REFERENCES
Chong MS, Hester J. Diabetic painful neuropathy: current and future treatment options. Drugs. 2007;67:569–585.
Pop-Busui R, Boulton AJ, Feldman EL, Bril V, Freeman R, Malik RA, et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017;40:136–154.
Vinik AI, Mitchell BD, Maser RE, Freeman R. Diabetic autonomic neuropathy. Diabetes Care. 2003;26,(5):1553–1579.
Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, et al. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: The Rochester Diabetic Neuropathy Study. Neurology. 1993;43:817–824.
Sun H, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119.
Kaur S, Pandhi P, Dutta P. Painful diabetic neuropathy: An update. Ann Neurosci. 2011;18:168–175.
Abbott CA, Malik RA, van Ross ERE, Kulkarni J, Boulton AJM. Prevalence and characteristics of painful diabetic neuropathy in a large community-based diabetic population in the U.K. Diabetes Care. 2011;34:2220–2224.
Alleman CJM, Westerhout KY, Hensen M, et al. Humanistic and economic burden of painful diabetic peripheral neuropathy in Europe: a review of the literature. Diabetes Res Clin Pract. 2015;109:215–225.
Kiyani M, Yang Z, Charalambous LT, et al. Painful diabetic peripheral neuropathy: health care costs and complications from 2010 to 2015. Neurol Clin Pract. 2020;10:47–57.
Staudt MD, Clark AJ, Gordon AS, et al. Long-term outcomes in the management of central neuropathic pain syndromes: a prospective observational cohort study. Can J Neurol Sci. 2018;45:545–552.
Mai LM, Clark AJ, Gordon AS, et al. Long-term outcomes in the management of painful diabetic neuropathy. Can J Neurol Sci. 2017;44:337–342.
Tesfaye S, Selvarajah D. Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy. Diabetes/Metab Res Rev. 2012;28(S1):8–14.
Pop-Busui R, Lu J, Brooks MM, et al. Impact of glycemic control strategies on the progression of diabetic peripheral neuropathy in the BARI 2D cohort. Diabetes Care. 2013;36:3208–3215.
Callaghan BC, Little AA, Feldman EL, Hughes RAC. Enhanced glucose control for preventing and treating diabetic neuropathy. Cochrane Database Syst Rev. 2012;6:160.
Ang L, Jaiswal M, Martin C, Pop-Busui R. Glucose control and diabetic neuropathy: lessons from recent large clinical trials. Curr Diab Rep. 2014;14:115528.
Adler AI, Boyko EJ, Ahroni JH, Stensel V, Forsberg RC, Smith DG, et al. Body height is an independent predictor of peripheral neuropathy in diabetes. Am J Epidemiol. 2006;164(9):873–880.
Elliott J, Tesfaye S, Chaturvedi N, et al. EURODIAB Prospective Complications Study Group: Large-fiber dysfunction in diabetic peripheral neuropathy is predicted by cardiovascular risk factors. Diabetes Care. 2009;32:1896–1900.
Martin CL, Albers JW, Pop-Busui R; DCCT/EDIC Research Group. Neuropathy and related findings in the DCCT/EDIC study. Diabetes Care. 2014;37:31–38.
Ziegler D, Behler M, Schroers-Teuber M, Roden M. Near-normoglycaemia and development of neuropathy: a 24-year prospective study from diagnosis of type 1 diabetes. BMJ Open. 2015;5:e006559.
Papanas N, Ziegler D. Polyneuropathy in impaired glucose tolerance: is postprandial hyperglycemia the main culprit? Gerontology. 2013;59:193–198.
Callaghan BC, Cheng HT, Stables CL, Smith AL, Feldman EL. The Lancet Neurology. 2012;11:521–534.
Callaghan BC, Xia R, Banerjee M, de Rekeneire N, Harris TB, Feldman EL. Metabolic syndrome components are associated with symptomatic polyneuropathy independent of glycemic status. Diabetes Care. 2016;39:801–807.
Feldman EL, Nave KA, Jensen TS, Bennett DLH. New horizons in diabetic neuropathy: mechanisms, bioenergetics, and pain. Neuron. 2017;93:1296–1313.
Tesfaye S, Boulton AJM, Dyck PJ, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33:2285–2293.
Cameron NE, Cotter MA. Effects of hypertension on peripheral nerve function and structure in experimental diabetes. Diabetes. 1992;41:623–629.
Tesfaye S, Chaturvedi N, Eaton SEM, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med. 2005;352:341–350.
Vinik AI, Casellini CM. Diabetic neuropathy and the impact of comorbid conditions such as hypertension. Endocrinol Metab Clin North Am. 2013;42:747–787.
Tesfaye S, Chaturvedi N, Eaton SEM. N Engl J Med. 2005;352:341–350.
Said G. Diabetic neuropathy—A review. Nat Clin Pract Neurol. 2007;3:331–340.
Boulton AJM, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, et al. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care. 2005;28:956–962.
Callaghan BC, Cheng HT, Stables CL, Smith AL, Feldman EL. Diabetic neuropathy: clinical manifestations and current treatments. Lancet Neurol. 2012;11:521–534.
Tesfaye S, Selvarajah D. The epidemiology of diabetic peripheral neuropathy. Curr Diabetes Rep. 2012;12:423–430.
Ziegler D. Type 2 diabetes as a risk factor for the development and progression of diabetic neuropathy. Diabetes Res Clin Pract. 2009;86:S3–S8.
Iqbal Z, Azmi S, Yadav R, et al. Diabetic peripheral neuropathy: epidemiology, diagnosis, and pharmacotherapy. Clin Ther. 2018;40:828–849.
International Diabetes Federation. IDF Diabetes Atlas, 10th Edition. 2019.
Callaghan BC, Gallagher G, Fridman V, Feldman EL. Diabetic neuropathy: what does the future hold? Diabetologia. 2020;63:891–897.
Edwards JL, Vincent AM, Cheng HT, Feldman EL. Diabetic neuropathy: mechanisms to management. Pharmacol Ther. 2008.
Oshitari T. Advanced glycation end-products and diabetic neuropathy of the retina. Int J Mol Sci. 2023;24:2927.
Gumy LF, Bampton ETW, Tolkovsky AM. Hyperglycaemia inhibits Schwann cell proliferation and migration and restricts regeneration of axons and Schwann cells from adult murine DRG. Mol Cell Neurosci. 2008;37:298–311.
Dunnigan SK, Ebadi H, Breiner A, et al. Conduction slowing in diabetic sensorimotor polyneuropathy. Diabetes Care. 2013;36:3684–3690.
Yan LJ. Redox imbalance stress in diabetes mellitus: role of the polyol pathway. Anim Model Exp Med. 2018;1:7–13.
Hotta N, Kawamura T, et al. Polyol pathway in diabetic neuropathy: NADPH consumption and oxidative stress. Diabetes Metab Res Rev. 2006;22:170–177.
Schmidt AM, Hori O, Brett J, Yan SD, Wautier JL, Stern D. Cellular receptors for advanced glycation end products. Arterioscler Thromb. 1994.
Singh R, Barden A, Mori T, Beilin L. Advanced glycation end-products: a review. Diabetologia. 2001;44:129–146.
Ahmed N. Advanced glycation endproducts—role in pathology of diabetic complications. Diabetes Res Clin Pract. 2005.
Vincent AM, Callaghan BC, Smith AL, Feldman EL. Diabetic neuropathy: cellular mechanisms as therapeutic targets. Nat Rev Neurol. 2011.
Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005;54:1615–1625.
Geraldes P, King GL. Activation of protein kinase C isoforms and its impact on diabetic complications. Circ Res. 2010;106:1319–1331.
Vincent AM, Russell JW, Low P, Feldman EL. Oxidative stress in the pathogenesis of diabetic neuropathy. Endocr Rev. 2004;25:612–628.
Obrosova IG. Diabetes and the peripheral nerve. Biochim Biophys Acta. 2009;1792:931–940.
Giacco F, Brownlee M. Oxidative stress and diabetic complications. Circ Res. 2010;107:1058–1070.
Meerwaldt R, Links TP, Graaff R, Hoogenberg K, et al. Increased accumulation of skin advanced glycation end-products precedes and correlates with clinical manifestation of diabetic neuropathy. Diabetologia. 2005;48:1637–1644.
Razmaria A. Diabetic neuropathy. JAMA. 2009;301:537–547.
Alsaloum M, Estacion M, Almomani R, et al. A gain-of-function sodium channel β2-subunit mutation in painful diabetic neuropathy. Mol Pain. 2019;15:1744806919849802.
Ziegler D. Cardiovascular autonomic neuropathy: clinical manifestations and measurement. Diabetes Rev. 1999;7:342–357.
Stansberry KB, Hill MA, Shapiro SA, et al. Impairment of peripheral blood flow responses in diabetes resembles an enhanced aging effect. Diabetes Care. 1997;20:1711–1716.
Naranjo C, Del Reguero L, Moratalla G, et al. Anxiety, depression and sleep disorders in patients with diabetic neuropathic pain: a systematic review. Expert Rev Neurother. 2019;19:1201–1209.
Boulton AJ, Vinik AI, Arezzo JC, et al. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care. 2005;28:956–962.
American Diabetes Association. Standards of Medical Care in Diabetes—2017. Diabetes Care. 2017;40(Suppl 1):S136–S154.
Boulton AJ, Armstrong DG, Albert SF, Frykberg RG, Hellman R, Kirkman MS, Lavery LA, Lemaster JW, Mills JL Sr, Mueller MJ, Sheehan P, Wukich DKAmerican Diabetes Association, American Association of Clinical Endocrinologists. Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care 2008;31:1679–1685.
Subramani A, Periasamy P, Gunasekaran S. A comparative analysis of diagnostic accuracy: vibration perception threshold vs. diabetic neuropathy examination for diabetic neuropathy. J Pharm Bioallied Sci. 2024;16(Suppl 5):S4536–S4539.
Young MJ, Boulton AJM, MacLeod AF, Williams DRR, Sonksen PH. A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia. 1993;36(2):150–154.
Callaghan BC, Kerber KA, Lisabeth LL et al (2014) Role of neurologists and diagnostic tests on the management of distal symmetric polyneuropathy. JAMA Neurol 71(9):1143–1149.
Chiaramonte R, Romano M, Vecchio M. A systematic review of the diagnostic methods of small fiber neuropathies in rehabilitation. Diagnostics. 2020;10(9):613.
Tai HF, Zhang YL, Yang JY, et al. Clinical and neuroelectrophysiological characteristics of primary peripheral nerve hyperexcitability syndrome. Zhonghua Yi Xue Za Zhi. 2023;103(25):1925–1930.
.Hosseini M.S., Razavi Z., Bahri R.A., Ehsani A.H., Firooz A., Aryanian Z., Ehsani A., Sadeghi Y. Is skin autofluorescence a novel non-invasive marker in diabetes? A systematic review and meta-analysis of case-control studies. J. Res. Med. Sci. 2023;28:68. doi: 10.4103/jrms.jrms_127_23.8
Tavakoli M, Quattrini C, Abbott C, et al. Corneal confocal microscopy: a novel noninvasive test to diagnose and stratify the severity of human diabetic neuropathy. Diabetes Care. 2010;33(8):1792–1797.
Vinik AI, Ziegler D. Diabetic cardiovascular autonomic neuropathy. Circulation. 2007;115(3):387–397.
Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year. Diabetes Res Clin Pract 1995;28:103-17
Diabetes Control and Complications Trial Research Group. The effect of intensive diabetes treatment on the development and progression of neuropathy. Ann Intern Med 1995;122:561-
Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, Davis M, Rand L and Siebert C: The effect of intensive treatment of diabetes on the development and progression of long‑term complications in insulin‑dependent diabetes mellitus. N Engl J Med 329: 977‑986, 1993.
The Diabetes Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 329:977–986, 1993.
Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group: Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Interventions and Complications (EDIC) study. JAMA 290:2159–2167, 2003.
Callaghan BC, Cheng HT, Stables CL, Smith AL, Feldman EL. Diabetic neuropathy: clinical manifestations and current treatments. Lancet Neurol. 2012;11(6):521–534. doi: 10.1016/S1474-4422(12)70065-0.
Tomlinson DR, Moriarty RJ, Mayer JH. Prevention and reversal of defective axonal transport and motor nerve conduction velocity in rats with experimental diabetes by treatment with the aldose reductase inhibitor Sorbinil. Diabetes. 1984;33(5):470–476. doi: 10.2337/diab.33.5.470.
Boulton AJ, Malik RA, Arezzo JC, Sosenko JM. Diabetic Somatic Neuropathies. Diabetes Care. 2004;27(6):1458–1486. doi: 10.2337/diacare.27.6.1458.
Chalk C, Benstead TJ and Moore F: Aldose reductase inhibitors for the treatment of diabetic polyneuropathy. Cochrane Database Syst Rev: CD004572, 2007.
Yamagishi S, Imaizumi T. The role of aldose reductase in glucose toxicity: an overview. Diabetes Metab Res Rev. 2002;18(2):104–112. doi:10.1002/dmrr.237.
Vallianou N, Evangelopoulos A and Koutalas P: Alpha-lipoic acid and diabetic neuropathy. Rev Diabet Stud. 6:230–236. 2009.
Ziegler D, Hanefeld M, Ruhnau KJ, Meissner HP, Lobisch M, Schütte K and Gries FA: Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant alpha-lipoic acid. A 3-week multicentre randomized controlled trial (ALADIN Study). Diabetologia. 38:1425–1433. 1995.
Pácal L, Kuricová K and Kaňková K: Evidence for altered thiamine metabolism in diabetes: Is there a potential to oppose gluco‑ and lipotoxicity by rational supplementation? World J Diabetes 5: 288‑295, 2014.
Stracke H., Gaus W., Achenbach U., Federlin K., Bretzel R. (2008) Benfotiamine in diabetic polyneuropathy (BENDIP): results of a randomised, double blind, placebo-controlled clinical study. Exp Clin Endocrinol Diabetes 116: 600–605.
Nikolić A, Kacar A, Lavrnić D, Basta I and Apostolski S: The effect of benfothiamine in the therapy of diabetic polyneuropathy. Srp Arh Celok Lek. 137:594–600. 2009.
Pop‑Busui R, Boulton AJ, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM and Ziegler D: Diabetic neuropathy: A position statement by the American diabetes association.Diabetes Care 40: 136‑154, 2017.
Attal N, Cruccu G, Baron R, Haanpää M, Hansson P, Jensen TS, Nurmikko T; European Federation of Neurological Societies. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol. 2010;17:1113–1e88. doi: 10.1111/j.1468-1331.2010.02999.x.
Pergolizzi JV, Raffa RB, Taylor R, Rodriguez G, Nalamachu S, Langley P. A review of duloxetine 60 mg once-daily dosing for the management of diabetic peripheral neuropathic pain, fibromyalgia, and chronic musculoskeletal pain due to chronic osteoarthritis pain and low back pain. Pain Pract. 2013;13:239–252. doi: 10.1111/j.1533-2500.2012.00578.x.
Tavakoli M., Mojaddidi M., Fadavi H., Malik R. (2008) Pathophysiology and treatment of painful diabetic neuropathy. Curr Pain Headache Rep 12: 192–197.
Goldstein D., Lu Y., Detke M., Lee T., Iyengar S. (2005) Duloxetine vs. placebo in patients with painful diabetic neuropathy. Pain 116: 109–118.
Rowbotham MC, Goli V, Kunz NR, Lei D. Venlafaxine extended release in the treatment of painful diabetic neuropathy: a double-blind, placebo-controlled study. Pain. 2004;110(3):697–706. doi: 10.1016/j.pain.2004.05.010.
.Verma V, Singh N, Singh Jaggi A. Pregabalin in neuropathic pain: evidence and possible mechanisms. Curr Neuropharmacol. 2014;12:44–56. doi: 10.2174/1570159X1201140117162802.
Blommel ML, Blommel AL. Pregabalin: an antiepileptic agent useful for neuropathic pain. Am J Health Syst Pharm. 2007;64:1475–1482. doi: 10.2146/ajhp060371.
Guy S, Mehta S, Leff L, Teasell R, Loh E. Anticonvulsant medication use for the management of pain following spinal cord injury: systematic review and effectiveness analysis. Spinal Cord. 2014;52:89–96. doi: 10.1038/sc.2013.146.
Lesser H., Sharma U., Lamoreaux L., Poole R. (2004) Pregabalin relieves symptoms of painful diabetic neuropathy: a randomized controlled trial. Neurology 63: 2104–2110.
Cross, A.L.; Sherman, A.L. Pregabalin. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2019.
Freeman, R.; Durso-Decruz, E.; Emir, B. Efficacy, safety, and tolerability of pregabalin treatment for painful diabetic peripheral neuropathy: Findings from seven randomized, controlled trials across a range of doses. Diabetes Care 2008, 31, 1448–1454.
Spallone V. (2012) Management of painful diabetic neuropathy: guideline guidance or jungle? Curr Diab Rep 12: 403–413.
Schwartz, S. et al. Safety and efficacy of tapentadol ER in patients with painful diabetic peripheral neuropathy: results of a randomized-withdrawal, placebo-controlled trial. Curr. Med. Res. Opin. 27, 151–162 (2011).
Vinik, A.I.; Shapiro, D.Y.; Rauschkolb, C.; Lange, B.; Karcher, K.; Pennett, D.; Etropolski, M.S. A randomized withdrawal, placebo-controlled study evaluating the efficacy and tolerability of tapentadol extended release in patients with chronic painful diabetic peripheral neuropathy. Diabetes Care 2014, 37, 2302–2309.
Harati Y, Gooch C, Swenson M, Edelman S, Greene D, Raskin P, Donofrio P, Cornblath D, Sachdeo R, Siu CO, Kamin M. Double-blind randomized trial of tramadol for the treatment of the pain of diabetic neuropathy. Neurology. 1998;50(6):1842–1846. doi: 10.1212/wnl.50.6.1842.
Dludla PV, Nkambule BB, Cirilli I, Marcheggiani F, Mabhida SE, Ziqubu K, Ntamo Y, Jack B, Nyambuya TM, Hanser S, Mazibuko-Mbeje SE. Capsaicin, its clinical significance in patients with painful diabetic neuropathy. Biomed Pharmacother. 2022;153:113439. 10.1016/j.biopha.2022.113439.
Abrams RMC, Pedowitz EJ, Simpson DM. A critical review of the capsaicin 8% patch for the treatment of neuropathic pain associated with diabetic peripheral neuropathy of the feet in adults. Expert Rev Neurother. 2021;21(3):259–66. 10.1080/14737175.2021.1874920.
Barbano RL, Herrmann DN, Hart-Gouleau S, Pennella-Vaughan J, Lode-wick PA, Dworkin RH. Effectiveness, tolerability, and impact on quality of life of the 5% lidocaine patch in diabetic polyneuropathy. Arch Neurol. 2004;61(6):914-918.
Casale R, Mattia C. Building a diagnostic algorithm on localized neuropathic pain (LNP) and targeted topical treatment: focus on 5% lidocaine-medicated plaster. Ther Clin Risk Manag. 2014;10:259–268. doi: 10.2147/TCRM.S58844.
Reference
Chong MS, Hester J. Diabetic painful neuropathy: current and future treatment options. Drugs. 2007;67:569–585.
Pop-Busui R, Boulton AJ, Feldman EL, Bril V, Freeman R, Malik RA, et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017;40:136–154.
Vinik AI, Mitchell BD, Maser RE, Freeman R. Diabetic autonomic neuropathy. Diabetes Care. 2003;26,(5):1553–1579.
Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, et al. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: The Rochester Diabetic Neuropathy Study. Neurology. 1993;43:817–824.
Sun H, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119.
Kaur S, Pandhi P, Dutta P. Painful diabetic neuropathy: An update. Ann Neurosci. 2011;18:168–175.
Abbott CA, Malik RA, van Ross ERE, Kulkarni J, Boulton AJM. Prevalence and characteristics of painful diabetic neuropathy in a large community-based diabetic population in the U.K. Diabetes Care. 2011;34:2220–2224.
Alleman CJM, Westerhout KY, Hensen M, et al. Humanistic and economic burden of painful diabetic peripheral neuropathy in Europe: a review of the literature. Diabetes Res Clin Pract. 2015;109:215–225.
Kiyani M, Yang Z, Charalambous LT, et al. Painful diabetic peripheral neuropathy: health care costs and complications from 2010 to 2015. Neurol Clin Pract. 2020;10:47–57.
Staudt MD, Clark AJ, Gordon AS, et al. Long-term outcomes in the management of central neuropathic pain syndromes: a prospective observational cohort study. Can J Neurol Sci. 2018;45:545–552.
Mai LM, Clark AJ, Gordon AS, et al. Long-term outcomes in the management of painful diabetic neuropathy. Can J Neurol Sci. 2017;44:337–342.
Tesfaye S, Selvarajah D. Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy. Diabetes/Metab Res Rev. 2012;28(S1):8–14.
Pop-Busui R, Lu J, Brooks MM, et al. Impact of glycemic control strategies on the progression of diabetic peripheral neuropathy in the BARI 2D cohort. Diabetes Care. 2013;36:3208–3215.
Callaghan BC, Little AA, Feldman EL, Hughes RAC. Enhanced glucose control for preventing and treating diabetic neuropathy. Cochrane Database Syst Rev. 2012;6:160.
Ang L, Jaiswal M, Martin C, Pop-Busui R. Glucose control and diabetic neuropathy: lessons from recent large clinical trials. Curr Diab Rep. 2014;14:115528.
Adler AI, Boyko EJ, Ahroni JH, Stensel V, Forsberg RC, Smith DG, et al. Body height is an independent predictor of peripheral neuropathy in diabetes. Am J Epidemiol. 2006;164(9):873–880.
Elliott J, Tesfaye S, Chaturvedi N, et al. EURODIAB Prospective Complications Study Group: Large-fiber dysfunction in diabetic peripheral neuropathy is predicted by cardiovascular risk factors. Diabetes Care. 2009;32:1896–1900.
Martin CL, Albers JW, Pop-Busui R; DCCT/EDIC Research Group. Neuropathy and related findings in the DCCT/EDIC study. Diabetes Care. 2014;37:31–38.
Ziegler D, Behler M, Schroers-Teuber M, Roden M. Near-normoglycaemia and development of neuropathy: a 24-year prospective study from diagnosis of type 1 diabetes. BMJ Open. 2015;5:e006559.
Papanas N, Ziegler D. Polyneuropathy in impaired glucose tolerance: is postprandial hyperglycemia the main culprit? Gerontology. 2013;59:193–198.
Callaghan BC, Cheng HT, Stables CL, Smith AL, Feldman EL. The Lancet Neurology. 2012;11:521–534.
Callaghan BC, Xia R, Banerjee M, de Rekeneire N, Harris TB, Feldman EL. Metabolic syndrome components are associated with symptomatic polyneuropathy independent of glycemic status. Diabetes Care. 2016;39:801–807.
Feldman EL, Nave KA, Jensen TS, Bennett DLH. New horizons in diabetic neuropathy: mechanisms, bioenergetics, and pain. Neuron. 2017;93:1296–1313.
Tesfaye S, Boulton AJM, Dyck PJ, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33:2285–2293.
Cameron NE, Cotter MA. Effects of hypertension on peripheral nerve function and structure in experimental diabetes. Diabetes. 1992;41:623–629.
Tesfaye S, Chaturvedi N, Eaton SEM, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med. 2005;352:341–350.
Vinik AI, Casellini CM. Diabetic neuropathy and the impact of comorbid conditions such as hypertension. Endocrinol Metab Clin North Am. 2013;42:747–787.
Tesfaye S, Chaturvedi N, Eaton SEM. N Engl J Med. 2005;352:341–350.
Said G. Diabetic neuropathy—A review. Nat Clin Pract Neurol. 2007;3:331–340.
Boulton AJM, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, et al. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care. 2005;28:956–962.
Callaghan BC, Cheng HT, Stables CL, Smith AL, Feldman EL. Diabetic neuropathy: clinical manifestations and current treatments. Lancet Neurol. 2012;11:521–534.
Tesfaye S, Selvarajah D. The epidemiology of diabetic peripheral neuropathy. Curr Diabetes Rep. 2012;12:423–430.
Ziegler D. Type 2 diabetes as a risk factor for the development and progression of diabetic neuropathy. Diabetes Res Clin Pract. 2009;86:S3–S8.
Iqbal Z, Azmi S, Yadav R, et al. Diabetic peripheral neuropathy: epidemiology, diagnosis, and pharmacotherapy. Clin Ther. 2018;40:828–849.
International Diabetes Federation. IDF Diabetes Atlas, 10th Edition. 2019.
Callaghan BC, Gallagher G, Fridman V, Feldman EL. Diabetic neuropathy: what does the future hold? Diabetologia. 2020;63:891–897.
Edwards JL, Vincent AM, Cheng HT, Feldman EL. Diabetic neuropathy: mechanisms to management. Pharmacol Ther. 2008.
Oshitari T. Advanced glycation end-products and diabetic neuropathy of the retina. Int J Mol Sci. 2023;24:2927.
Gumy LF, Bampton ETW, Tolkovsky AM. Hyperglycaemia inhibits Schwann cell proliferation and migration and restricts regeneration of axons and Schwann cells from adult murine DRG. Mol Cell Neurosci. 2008;37:298–311.
Dunnigan SK, Ebadi H, Breiner A, et al. Conduction slowing in diabetic sensorimotor polyneuropathy. Diabetes Care. 2013;36:3684–3690.
Yan LJ. Redox imbalance stress in diabetes mellitus: role of the polyol pathway. Anim Model Exp Med. 2018;1:7–13.
Hotta N, Kawamura T, et al. Polyol pathway in diabetic neuropathy: NADPH consumption and oxidative stress. Diabetes Metab Res Rev. 2006;22:170–177.
Schmidt AM, Hori O, Brett J, Yan SD, Wautier JL, Stern D. Cellular receptors for advanced glycation end products. Arterioscler Thromb. 1994.
Singh R, Barden A, Mori T, Beilin L. Advanced glycation end-products: a review. Diabetologia. 2001;44:129–146.
Ahmed N. Advanced glycation endproducts—role in pathology of diabetic complications. Diabetes Res Clin Pract. 2005.
Vincent AM, Callaghan BC, Smith AL, Feldman EL. Diabetic neuropathy: cellular mechanisms as therapeutic targets. Nat Rev Neurol. 2011.
Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005;54:1615–1625.
Geraldes P, King GL. Activation of protein kinase C isoforms and its impact on diabetic complications. Circ Res. 2010;106:1319–1331.
Vincent AM, Russell JW, Low P, Feldman EL. Oxidative stress in the pathogenesis of diabetic neuropathy. Endocr Rev. 2004;25:612–628.
Obrosova IG. Diabetes and the peripheral nerve. Biochim Biophys Acta. 2009;1792:931–940.
Giacco F, Brownlee M. Oxidative stress and diabetic complications. Circ Res. 2010;107:1058–1070.
Meerwaldt R, Links TP, Graaff R, Hoogenberg K, et al. Increased accumulation of skin advanced glycation end-products precedes and correlates with clinical manifestation of diabetic neuropathy. Diabetologia. 2005;48:1637–1644.
Razmaria A. Diabetic neuropathy. JAMA. 2009;301:537–547.
Alsaloum M, Estacion M, Almomani R, et al. A gain-of-function sodium channel β2-subunit mutation in painful diabetic neuropathy. Mol Pain. 2019;15:1744806919849802.
Ziegler D. Cardiovascular autonomic neuropathy: clinical manifestations and measurement. Diabetes Rev. 1999;7:342–357.
Stansberry KB, Hill MA, Shapiro SA, et al. Impairment of peripheral blood flow responses in diabetes resembles an enhanced aging effect. Diabetes Care. 1997;20:1711–1716.
Naranjo C, Del Reguero L, Moratalla G, et al. Anxiety, depression and sleep disorders in patients with diabetic neuropathic pain: a systematic review. Expert Rev Neurother. 2019;19:1201–1209.
Boulton AJ, Vinik AI, Arezzo JC, et al. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care. 2005;28:956–962.
American Diabetes Association. Standards of Medical Care in Diabetes—2017. Diabetes Care. 2017;40(Suppl 1):S136–S154.
Boulton?AJ, Armstrong?DG, Albert?SF, Frykberg?RG, Hellman?R, Kirkman?MS, Lavery?LA, Lemaster?JW, Mills?JL?Sr, Mueller?MJ, Sheehan?P, Wukich?DKAmerican Diabetes Association, American Association of Clinical Endocrinologists. Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care?2008;31:1679–1685.
Subramani A, Periasamy P, Gunasekaran S. A comparative analysis of diagnostic accuracy: vibration perception threshold vs. diabetic neuropathy examination for diabetic neuropathy. J Pharm Bioallied Sci. 2024;16(Suppl 5):S4536–S4539.
Young MJ, Boulton AJM, MacLeod AF, Williams DRR, Sonksen PH. A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia. 1993;36(2):150–154.
Callaghan BC, Kerber KA, Lisabeth LL et al (2014) Role of neurologists and diagnostic tests on the management of distal symmetric polyneuropathy. JAMA Neurol 71(9):1143–1149.
Chiaramonte R, Romano M, Vecchio M. A systematic review of the diagnostic methods of small fiber neuropathies in rehabilitation. Diagnostics. 2020;10(9):613.
Tai HF, Zhang YL, Yang JY, et al. Clinical and neuroelectrophysiological characteristics of primary peripheral nerve hyperexcitability syndrome. Zhonghua Yi Xue Za Zhi. 2023;103(25):1925–1930.
.Hosseini M.S., Razavi Z., Bahri R.A., Ehsani A.H., Firooz A., Aryanian Z., Ehsani A., Sadeghi Y. Is skin autofluorescence a novel non-invasive marker in diabetes? A systematic review and meta-analysis of case-control studies. J. Res. Med. Sci. 2023;28:68. doi: 10.4103/jrms.jrms_127_23.8
Tavakoli M, Quattrini C, Abbott C, et al. Corneal confocal microscopy: a novel noninvasive test to diagnose and stratify the severity of human diabetic neuropathy. Diabetes Care. 2010;33(8):1792–1797.
Vinik AI, Ziegler D. Diabetic cardiovascular autonomic neuropathy. Circulation. 2007;115(3):387–397.
Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year. Diabetes Res Clin Pract 1995;28:103-17
Diabetes Control and Complications Trial Research Group. The effect of intensive diabetes treatment on the development and progression of neuropathy. Ann Intern Med 1995;122:561-
Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, Davis M, Rand L and Siebert C: The effect of intensive treatment of diabetes on the development and progression of long?term complications in insulin?dependent diabetes mellitus. N Engl J Med 329: 977?986, 1993.
The Diabetes Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 329:977–986, 1993.
Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group: Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Interventions and Complications (EDIC) study. JAMA 290:2159–2167, 2003.
Callaghan BC, Cheng HT, Stables CL, Smith AL, Feldman EL. Diabetic neuropathy: clinical manifestations and current treatments. Lancet Neurol. 2012;11(6):521–534. doi: 10.1016/S1474-4422(12)70065-0.
Tomlinson DR, Moriarty RJ, Mayer JH. Prevention and reversal of defective axonal transport and motor nerve conduction velocity in rats with experimental diabetes by treatment with the aldose reductase inhibitor Sorbinil. Diabetes. 1984;33(5):470–476. doi: 10.2337/diab.33.5.470.
Boulton AJ, Malik RA, Arezzo JC, Sosenko JM. Diabetic Somatic Neuropathies. Diabetes Care. 2004;27(6):1458–1486. doi: 10.2337/diacare.27.6.1458.
Chalk C, Benstead TJ and Moore F: Aldose reductase inhibitors for the treatment of diabetic polyneuropathy. Cochrane Database Syst Rev: CD004572, 2007.
Yamagishi S, Imaizumi T. The role of aldose reductase in glucose toxicity: an overview. Diabetes Metab Res Rev. 2002;18(2):104–112. doi:10.1002/dmrr.237.
Vallianou N, Evangelopoulos A and Koutalas P: Alpha-lipoic acid and diabetic neuropathy. Rev Diabet Stud. 6:230–236. 2009.
Ziegler D, Hanefeld M, Ruhnau KJ, Meissner HP, Lobisch M, Schütte K and Gries FA: Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant alpha-lipoic acid. A 3-week multicentre randomized controlled trial (ALADIN Study). Diabetologia. 38:1425–1433. 1995.
Pácal L, Kuricová K and Ka?ková K: Evidence for altered thiamine metabolism in diabetes: Is there a potential to oppose gluco? and lipotoxicity by rational supplementation? World J Diabetes 5: 288?295, 2014.
Stracke H., Gaus W., Achenbach U., Federlin K., Bretzel R. (2008) Benfotiamine in diabetic polyneuropathy (BENDIP): results of a randomised, double blind, placebo-controlled clinical study. Exp Clin Endocrinol Diabetes 116: 600–605.
Nikoli? A, Kacar A, Lavrni? D, Basta I and Apostolski S: The effect of benfothiamine in the therapy of diabetic polyneuropathy. Srp Arh Celok Lek. 137:594–600. 2009.
Pop?Busui R, Boulton AJ, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM and Ziegler D: Diabetic neuropathy: A position statement by the American diabetes association.Diabetes Care 40: 136?154, 2017.
Attal N, Cruccu G, Baron R, Haanpää M, Hansson P, Jensen TS, Nurmikko T; European Federation of Neurological Societies. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol. 2010;17:1113–1e88. doi: 10.1111/j.1468-1331.2010.02999.x.
Pergolizzi JV, Raffa RB, Taylor R, Rodriguez G, Nalamachu S, Langley P. A review of duloxetine 60 mg once-daily dosing for the management of diabetic peripheral neuropathic pain, fibromyalgia, and chronic musculoskeletal pain due to chronic osteoarthritis pain and low back pain. Pain Pract. 2013;13:239–252. doi: 10.1111/j.1533-2500.2012.00578.x.
Tavakoli M., Mojaddidi M., Fadavi H., Malik R. (2008) Pathophysiology and treatment of painful diabetic neuropathy. Curr Pain Headache Rep 12: 192–197.
Goldstein D., Lu Y., Detke M., Lee T., Iyengar S. (2005) Duloxetine vs. placebo in patients with painful diabetic neuropathy. Pain 116: 109–118.
Rowbotham MC, Goli V, Kunz NR, Lei D. Venlafaxine extended release in the treatment of painful diabetic neuropathy: a double-blind, placebo-controlled study. Pain. 2004;110(3):697–706. doi: 10.1016/j.pain.2004.05.010.
.Verma V, Singh N, Singh Jaggi A. Pregabalin in neuropathic pain: evidence and possible mechanisms. Curr Neuropharmacol. 2014;12:44–56. doi: 10.2174/1570159X1201140117162802.
Blommel ML, Blommel AL. Pregabalin: an antiepileptic agent useful for neuropathic pain. Am J Health Syst Pharm. 2007;64:1475–1482. doi: 10.2146/ajhp060371.
Guy S, Mehta S, Leff L, Teasell R, Loh E. Anticonvulsant medication use for the management of pain following spinal cord injury: systematic review and effectiveness analysis. Spinal Cord. 2014;52:89–96. doi: 10.1038/sc.2013.146.
Lesser H., Sharma U., Lamoreaux L., Poole R. (2004) Pregabalin relieves symptoms of painful diabetic neuropathy: a randomized controlled trial. Neurology 63: 2104–2110.
Cross, A.L.; Sherman, A.L. Pregabalin. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2019.
Freeman, R.; Durso-Decruz, E.; Emir, B. Efficacy, safety, and tolerability of pregabalin treatment for painful diabetic peripheral neuropathy: Findings from seven randomized, controlled trials across a range of doses. Diabetes Care 2008, 31, 1448–1454.
Spallone V. (2012) Management of painful diabetic neuropathy: guideline guidance or jungle? Curr Diab Rep 12: 403–413.
Schwartz, S. et al. Safety and efficacy of tapentadol ER in patients with painful diabetic peripheral neuropathy: results of a randomized-withdrawal, placebo-controlled trial. Curr. Med. Res. Opin. 27, 151–162 (2011).
Vinik, A.I.; Shapiro, D.Y.; Rauschkolb, C.; Lange, B.; Karcher, K.; Pennett, D.; Etropolski, M.S. A randomized withdrawal, placebo-controlled study evaluating the efficacy and tolerability of tapentadol extended release in patients with chronic painful diabetic peripheral neuropathy. Diabetes Care 2014, 37, 2302–2309.
Harati Y, Gooch C, Swenson M, Edelman S, Greene D, Raskin P, Donofrio P, Cornblath D, Sachdeo R, Siu CO, Kamin M. Double-blind randomized trial of tramadol for the treatment of the pain of diabetic neuropathy. Neurology. 1998;50(6):1842–1846. doi: 10.1212/wnl.50.6.1842.
Dludla PV, Nkambule BB, Cirilli I, Marcheggiani F, Mabhida SE, Ziqubu K, Ntamo Y, Jack B, Nyambuya TM, Hanser S, Mazibuko-Mbeje SE. Capsaicin, its clinical significance in patients with painful diabetic neuropathy. Biomed Pharmacother. 2022;153:113439. 10.1016/j.biopha.2022.113439.
Abrams RMC, Pedowitz EJ, Simpson DM. A critical review of the capsaicin 8% patch for the treatment of neuropathic pain associated with diabetic peripheral neuropathy of the feet in adults. Expert Rev Neurother. 2021;21(3):259–66. 10.1080/14737175.2021.1874920.
Barbano RL, Herrmann DN, Hart-Gouleau S, Pennella-Vaughan J, Lode-wick PA, Dworkin RH. Effectiveness, tolerability, and impact on quality of life of the 5% lidocaine patch in diabetic polyneuropathy. Arch Neurol. 2004;61(6):914-918.
Casale R, Mattia C. Building a diagnostic algorithm on localized neuropathic pain (LNP) and targeted topical treatment: focus on 5% lidocaine-medicated plaster. Ther Clin Risk Manag. 2014;10:259–268. doi: 10.2147/TCRM.S58844.
Irtizah Farooq
Corresponding author
St. Soldier Institute of Pharmacy, Lidhran Campus Behind NIT (R.E.C) Jalandhar- Amritsar bypass, NH-1, Jalandhar- 144011, Punjab, India
Rajesh Kumar
Co-author
Professor, St. Soldier Institute of Pharmacy
Ajeet Pal Singh
Co-author
St. Soldier Institute of Pharmacy, Lidhran Campus Behind NIT (R.E.C) Jalandhar- Amritsar bypass, NH-1, Jalandhar- 144011, Punjab, India
Amar Pal Singh
Co-author
St. Soldier Institute of Pharmacy, Lidhran Campus Behind NIT (R.E.C) Jalandhar- Amritsar bypass, NH-1, Jalandhar- 144011, Punjab, India
Irtizah Farooq, Rajesh Kumar, Diabetic Ajeet Pal Singh, Amar Pal Singh, Neuropathy:Pathophysiology, Clinical Features and Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6947-6963, https://doi.org/10.5281/zenodo.20957820



 10.5281/zenodo.20957820
10.5281/zenodo.20957820