
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 Msc Biotechnology, Dayanand Science College, Latur, India
2 Bsc Nursing, Dr. Rajendra Gode Nursing Institute of Buldhana, India.
Effervescent tablets combining an antacid base with vitamins B12 and B6 represent a rational fixed-dose approach for patients whose acid-related disorders and chronic acid-suppressive therapy place them at elevated risk of micronutrient depletion. This review synthesises current literature on the epidemiology of acid-related gastrointestinal disorders, the pharmacology of antacid agents, the physiological roles and deficiency states of vitamins B12 and B6, and the pharmaceutical science underlying effervescent tablet technology. Formulation strategies, granulation and manufacturing technologies, stability behaviour under humidity stress, Quality by Design (QbD) and regulatory frameworks, standard evaluation parameters, and reported clinical evidence for combined antacid-vitamin regimens are critically appraised. Emerging technologies, including three-dimensional printing, microencapsulation-based taste masking, and nanocarrierassisted vitamin delivery, are discussed as future directions. Persistent challenges include the physicochemical incompatibility of cobalamin and pyridoxine with acidic or alkaline effervescent excipients, moisture-driven degradation during manufacture and storage, and a scarcity of dedicated clinical trials evaluating the combined product rather than its components in isolation. Addressing these gaps through QbD-guided formulation design, protective coating or microencapsulation of the vitamin fraction, and targeted clinical evaluation could support the development of a stable, palatable, and therapeutically meaningful next-generation effervescent antacid-vitamin tablet.
Acid-related gastrointestinal disorders, encompassing gastro-oesophageal reflux disease (GERD) and peptic ulcer disease (PUD), remain among the most common reasons for both self-medication and physician consultation worldwide, and antacids continue to serve as first-line, on-demand symptomatic therapy for millions of patients [1,2]. Long-term acid suppression, whether through chronic antacid use, histamine-2 receptor antagonists, or proton pump inhibitors, has been repeatedly linked in the literature to reduced gastric acidity and consequent impairment of micronutrient release and absorption, most notably of vitamin B12 (cobalamin), which depends on an acidic gastric environment for its liberation from dietary protein [3,4]. Vitamin B6 (pyridoxine) shares overlapping metabolic pathways with cobalamin in one-carbon metabolism and homocysteine regulation, and its co-administration is frequently rationalised on similar grounds of gastrointestinal risk and nutritional support [5,6].
Effervescent tablets, uncoated solid dosage forms that release carbon dioxide upon contact with water to produce a rapidly disintegrating, palatable solution, have long been valued in pharmaceutical practice for their rapid onset of action, ease of swallowing, and superior patient acceptability relative to conventional tablets, particularly among paediatric, geriatric, and dysphagic populations [7,8]. Combining an antacid effervescent base with vitamins B12 and B6 in a single dosage form is therefore an attractive proposition: it offers immediate symptomatic relief while simultaneously addressing a nutritional vulnerability created, at least in part, by the very therapy being administered.
However, the pharmaceutical development of such a combination product is far from trivial. Effervescent systems are inherently moisture-sensitive, and the acid-base reaction central to their function creates a chemically reactive microenvironment that can be hostile to labile actives such as cobalamin and pyridoxine, both of which are known to degrade under conditions of extreme pH, heat, humidity, and light [9,10]. This review integrates the pharmacological rationale for combined antacid-vitamin therapy with the pharmaceutical technology required to translate that rationale into a stable, manufacturable, and clinically meaningful product. It surveys the epidemiology of acidrelated disorders, antacid pharmacology, the physiology of vitamins B12 and B6, effervescent tablet technology, formulation and manufacturing strategies, stability and bioavailability considerations, regulatory frameworks including Quality by Design (QbD), standard evaluation parameters, available clinical evidence, and emerging technologies, before identifying persistent research gaps and future directions.
Acid-Related Disorders
GERD and PUD together constitute a substantial global disease burden. Estimates derived from the Global Burden of Disease (GBD) study indicate that GERD prevalence rose from roughly 441–451 million cases in 1990 to approximately 784–826 million cases by 2019–2021, an increase of nearly 80% over three decades, with age-standardised prevalence, incidence, and years-lived-withdisability rates all trending upward, particularly in middle sociodemographic index regions and in adults aged 25–34 years [11–13]. Historical prevalence estimates have generally been higher in Western populations (approximately 9–28%) than in Asian populations (approximately 2.5–8%), although recent projections suggest this gap is narrowing and that global GERD cases could reach over 527 million among the 15–49 age group alone by 2035 [13,14].
Peptic ulcer disease shows a contrasting long-term trajectory. GBD analyses report that global PUD prevalence was approximately 8.09 million cases in 2019, a 25.8% increase in absolute numbers since 1990, even though the age-standardised prevalence rate actually declined by roughly 143 per 100,000 population over the same period, reflecting population growth and ageing rather than a rising per-capita risk; a modest upward inclination in the age-standardised rate has, however, been observed over the most recent fifteen years, attributed in part to changing risk-factor profiles such as non-steroidal anti-inflammatory drug use [2,15]. Regional estimates place the global point prevalence of peptic ulcer between roughly 0.12% and 1.5%, with considerably higher rates historically reported in some Western cohorts [1].
Both conditions are managed predominantly with acid-neutralising or acid-suppressing pharmacotherapy, and antacids remain a mainstay for rapid, on-demand symptom control even where longer-acting agents such as proton pump inhibitors are used for maintenance therapy [16]. The scale of this disease burden underlines the clinical relevance of formulating antacid products that are not only effective and well-tolerated but also capable of mitigating the nutritional consequences associated with prolonged acid suppression.
Antacid Therapy
Antacids are basic compounds that neutralise gastric hydrochloric acid through direct acid-base reactions, thereby raising intragastric pH and providing rapid, though relatively short-lived, symptomatic relief from heartburn, dyspepsia, and ulcer-related pain [17,18]. The principal active moieties include sodium bicarbonate, calcium carbonate, magnesium hydroxide or carbonate, and aluminium hydroxide, each differing in onset, neutralising capacity, and side-effect profile. Sodium bicarbonate reacts almost instantaneously with gastric acid to liberate carbon dioxide and is highly water-soluble, but its systemic absorption can precipitate metabolic alkalosis with excessive or prolonged use [18,19]. Calcium carbonate is a potent, fast-acting, and widely used neutralising agent; magnesium compounds are effective but tend to cause a laxative effect, whereas aluminium compounds are constipating, and combinations of the two are frequently used to offset these opposing gastrointestinal effects [19].
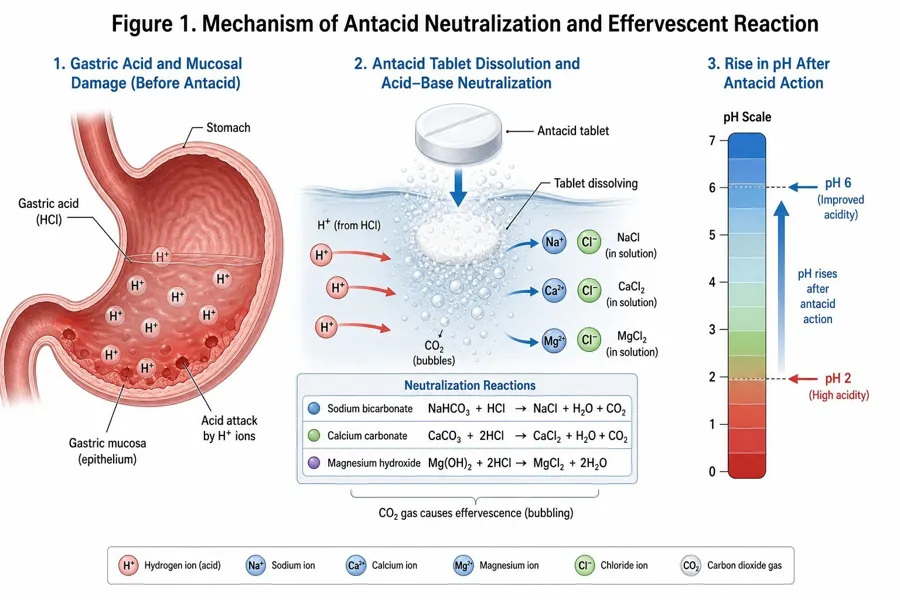
Figure 1. Mechanism of antacid neutralisation and effervescent acid-base reaction (see Section 4).
Mechanistically, all antacid salts are classified as either systemically absorbable (e.g., sodium bicarbonate) or largely non-absorbable (e.g., aluminium and magnesium hydroxides), with the latter preferred for chronic or repeated use owing to a lower risk of acid-base disturbance, although accumulation of aluminium or magnesium can be problematic in renal insufficiency [18]. Because antacids elevate gastric and duodenal pH, they can also alter the absorption of co-administered drugs; well-documented examples include reduced bioavailability of certain antiretroviral and antibiotic agents when co-ingested with aluminium/magnesium-containing antacids, an interaction attributed to cation chelation and pH-dependent solubility changes, and clinically managed by separating dosing times [20].
Of particular relevance to this review, gastric acid is required to cleave dietary cobalamin from its protein matrix so that it can bind haptocorrin and, subsequently, intrinsic factor for ileal absorption [4,21]. Long-term acid-suppressive therapy, most extensively studied for proton pump inhibitors but mechanistically relevant to any strategy that chronically elevates gastric pH, has therefore been proposed as a contributor to vitamin B12 deficiency, although the epidemiological evidence is heterogeneous: several systematic reviews and meta-analyses report a significant association between long-term acid suppression and biochemical markers of B12 deficiency (elevated homocysteine and methylmalonic acid, reduced serum B12) [4,22,23], whereas other wellpowered analyses have found no significant difference in serum B12 or homocysteine between chronic users and non-users [3,24]. This conflicting evidence base, discussed further in Section 13, underscores both the biological plausibility of the antacid-vitamin rationale and the need for caution in overstating its clinical certainty.
Table 1. Comparative composition, neutralising capacity, and safety profile of common antacid agents used in effervescent formulations.
|
Antacid Agent |
Neutralisation Reaction with Gastric HCl |
Approx. Acid Neutralising Capacity |
Onset of Action |
Principal Adverse Effect / Caution |
|
Sodium bicarbonate |
NaHCO₃ + HCl → NaCl + H₂O + CO₂ |
~11.9 mEq/g |
Very rapid (seconds) |
Systemic (metabolic) alkalosis and sodium load with repeated dosing |
|
Calcium carbonate |
CaCO₃ + 2HCl → CaCl₂ + H₂O + CO₂ |
~20 mEq/g |
Rapid |
Constipation; rebound acid hypersecretion with high doses |
|
Magnesium hydroxide |
Mg(OH)₂ + 2HCl → MgCl₂ + 2H₂O |
~32.6 mEq/g |
Rapid |
Osmotic (laxative) diarrhoea; often combined with aluminium salts to offset this effect |
|
Antacid Agent |
Neutralisation Reaction with Gastric HCl |
Approx. Acid Neutralising Capacity |
Onset of Action |
Principal Adverse Effect / Caution |
|
Aluminium hydroxide |
Al(OH)₃ + 3HCl → AlCl₃ + 3H₂O |
Lower relative potency than Mg/Ca salts |
Moderate |
Constipation; aluminium accumulation — caution/ contraindicated in renal insufficiency |
Reaction stoichiometry and neutralising-capacity values compiled from [17–19].
Vitamins B12 and B6
Vitamin B12 (cobalamin) is a water-soluble, cobalt-containing vitamin synthesised exclusively by certain bacteria and archaea and obtained by humans through animal-derived foods or supplementation [25,26]. It is an essential cofactor for methionine synthase, which converts homocysteine to methionine while regenerating tetrahydrofolate for nucleotide synthesis, and for methylmalonyl-CoA mutase, which participates in fatty acid and amino acid catabolism; through these reactions cobalamin underpins DNA synthesis, myelin maintenance, and erythropoiesis [26,27]. Dietary absorption is a multistep process: gastric acid and pepsin liberate protein-bound cobalamin, which is then bound by salivary and gastric haptocorrin; pancreatic proteases degrade the haptocorrin complex in the duodenum, allowing cobalamin to bind intrinsic factor secreted by gastric parietal cells, and the intrinsic factor-cobalamin complex is subsequently absorbed via cubam receptors in the terminal ileum before entering the circulation bound to transcobalamin [21,28]. Disruption at any of these steps, including reduced gastric acidity, intrinsic factor deficiency, or ileal disease, can precipitate deficiency, which manifests clinically as megaloblastic anaemia and a spectrum of neurological disturbances including peripheral neuropathy, cognitive impairment, and gait abnormalities [29,30]. Subclinical deficiency is reported to affect between roughly 2.5% and 26% of the general population depending on the diagnostic threshold applied, with elderly individuals, vegetarians, and vegans at particularly elevated risk owing to reduced dietary intake or age-related declines in intrinsic factor secretion and gastric acidity [26,31].
Vitamin B6 exists in six interconvertible vitamers, with pyridoxal 5'-phosphate (PLP) representing the principal biologically active coenzyme form, supporting more than one hundred and sixty enzymatic reactions involved in amino acid, carbohydrate, lipid, and neurotransmitter metabolism [32,33]. PLP is also required, alongside cobalamin and folate, for homocysteine remethylation and transsulfuration pathways, linking B6 status mechanistically to the same one-carbon metabolic network affected by cobalamin depletion [32]. Clinically manifest B6 deficiency is uncommon in isolation but can present with seborrheic dermatitis, glossitis, microcytic anaemia, peripheral neuropathy, and, in severe or genetically determined cases, intractable seizures responsive to pyridoxine administration [34,35]. Certain drugs, including isoniazid, hydralazine, penicillamine, and levodopa, are recognised to interfere with pyridoxine metabolism or increase its urinary excretion, and prophylactic pyridoxine supplementation is an established clinical practice in patients receiving such agents [36]. Recommended daily intake for adults is generally cited in the range of 1.6–2.0 mg, and oral bioavailability of pyridoxine itself is high owing to efficient gastrointestinal absorption that, unlike cobalamin, is not critically dependent on gastric acidity or intrinsic factor [30,33].
The pairing of B12 and B6 (frequently alongside folate) in combination products reflects both their overlapping role in homocysteine metabolism and the clinical observation that populations at risk of acid-related gastrointestinal disease, particularly older adults on chronic antacid or acidsuppressive therapy, are also disproportionately represented among those with suboptimal Bvitamin status [5,6].
Effervescent Tablet Technology
Effervescent tablets are uncoated dosage forms typically composed of an organic acid (commonly citric acid, tartaric acid, or a combination thereof) and a carbonate or bicarbonate source, which react on contact with water to liberate carbon dioxide gas, producing rapid disintegration and a palatable, carbonated solution [37,38]. This technology dates back to the eighteenth-century development of saline cathartics and has since been extended across a wide range of therapeutic categories, valued for the rapid onset of drug action associated with dissolution prior to ingestion, improved palatability that can mask unpleasant drug tastes, and superior swallowability for paediatric, geriatric, and dysphagic patients who struggle with conventional tablets or capsules [7,39].
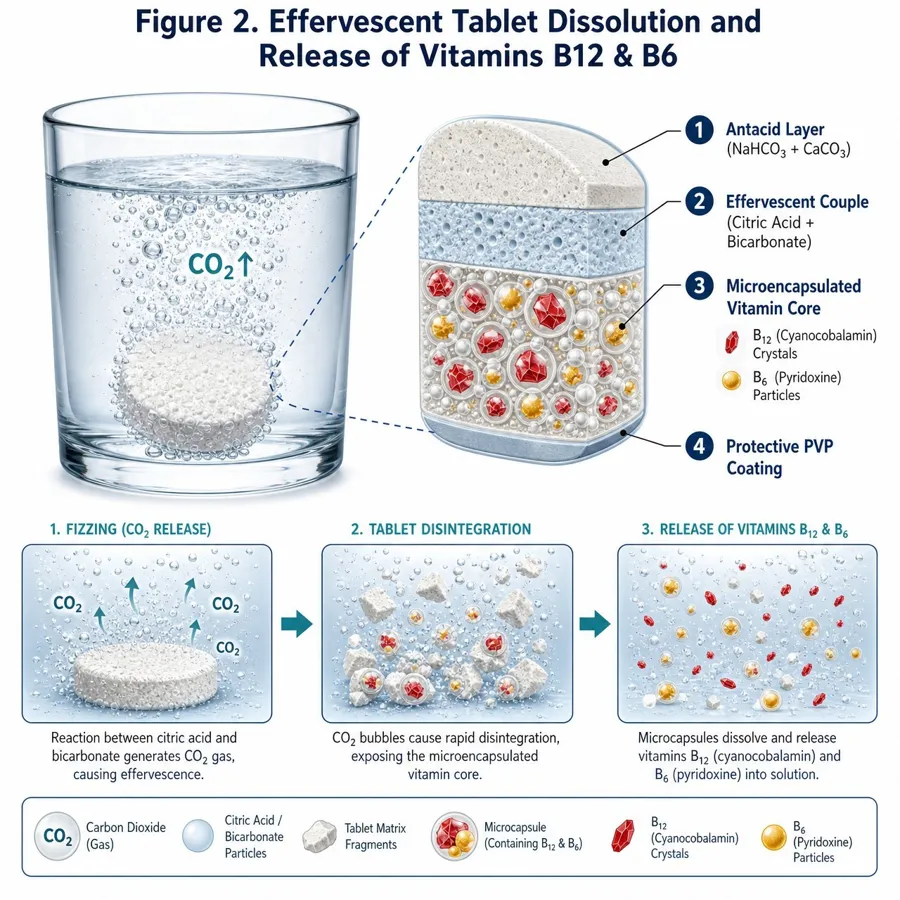
Figure 2. Effervescent tablet dissolution and release of vitamins B12 and B6 (see Section 6).
Because the acid and carbonate components are designed to remain inert until exposed to water, effervescent formulations are exceptionally sensitive to ambient and process-related humidity; premature or partial reaction during manufacture compromises both the physical integrity of the tablet and its in-use performance, making moisture control the single most critical variable across the entire production and packaging chain [40,41]. A comprehensive body of recent review literature has systematically catalogued the excipients, manufacturing routes, and quality parameters relevant to effervescent systems, reflecting sustained pharmaceutical interest in optimising this dosage form for an increasingly broad range of actives, including nutraceuticals, herbal extracts, and, as considered in this review, combination antacid-vitamin products [8,42,43].
Formulation Strategies
The core formulation challenge for an effervescent antacid-vitamin tablet lies in reconciling three functionally distinct components within a single, moisture-sensitive matrix: an antacid neutralising agent (e.g., sodium bicarbonate, calcium carbonate), the effervescent acid-base couple that may overlap with or be distinct from the antacid itself, and the vitamin actives, which are physicochemically labile and prone to interaction with both the acidic and basic microenvironments generated during dissolution and, potentially, during storage [9,44]. Selection of the organic acid is an important formulation variable; citric acid is hygroscopic and can promote caking, whereas fumaric and tartaric acids, or blends thereof, are sometimes preferred for their lower hygroscopicity and more controlled reaction kinetics, and coating individual excipient particles with a thin polyvinylpyrrolidone (PVP) layer has been used to slow premature acid-base interaction during processing [45].
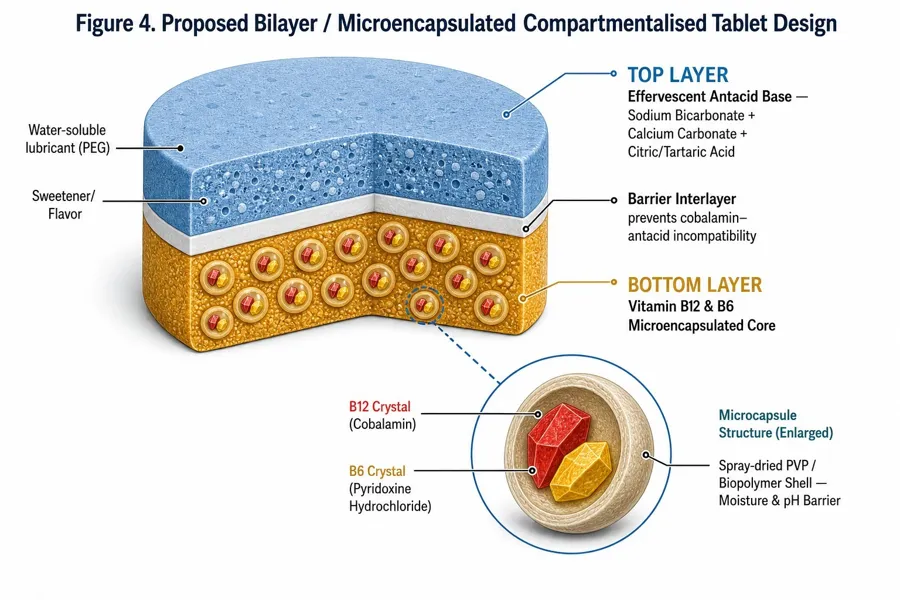
Figure 4. Proposed bilayer / microencapsulated compartmentalised tablet design (see Section 7).
Vitamin B12 stability within multi-component solid formulations is strongly influenced by coformulated ingredients. Comparative stability data indicate that cyanocobalamin retains more than 95% of labelled content after twelve months at room temperature when formulated alone, but degrades to as little as 28–37% of label claim in some multi-ingredient preparations over the same period, with thiamine and, to a lesser extent, riboflavin and pyridoxine implicated as contributing factors depending on the specific matrix and pH [9,46]. Notably, some studies report that pyridoxine co-formulated with cyanocobalamin alone (without thiamine) preserves the majority of B12 potency, whereas the presence of thiamine or combined thiamine-pyridoxine exposure produces substantially greater losses, suggesting that careful selection of co-actives and, where feasible, physical separation of incompatible components (for example through bilayer tableting or microencapsulation) is a rational formulation strategy for the B12/B6 antacid combination [9,47].
Taste masking is a further formulation consideration, since both the antacid salts and vitamin actives, particularly cobalamin, can contribute metallic or bitter notes that compromise palatability; microencapsulation with biopolymer coatings (e.g., spray-dried or spray-chilled particles) has been shown to both protect labile vitamins from environmental degradation and mask undesirable taste, and similar coating and nanocapsule-based approaches developed for other bitter actives illustrate a transferable design principle for this dosage form [48–51]. Sweeteners, flavouring agents, and effervescent-compatible lubricants (typically water-soluble types such as polyethylene glycol or sodium benzoate) complete the excipient profile, balancing mouthfeel, compressibility, and chemical compatibility [39,45].
Stability Studies
Stability testing of effervescent antacid-vitamin tablets must address both the intrinsic reactivity of the effervescent base and the specific degradation pathways of cobalamin and pyridoxine. Internationally, stability protocols are governed by the ICH Q1A(R2) guideline, which specifies long-term storage testing at 25 °C ± 2 °C/60% RH ± 5% RH (or 30 °C ± 2 °C/65% RH ± 5% RH), intermediate testing at 30 °C ± 2 °C/65% RH ± 5% RH, and accelerated testing at 40 °C ± 2 °C/75% RH ± 5% RH, generally over six to twenty-four months, with quality attributes such as appearance, assay, degradation products, dissolution, pH, and moisture content assessed at defined intervals [52–54].
Effervescent systems are considerably more moisture-sensitive than conventional tablets, and manufacturing environments are typically maintained at or below approximately 20–25% relative humidity to prevent premature reaction and to preserve granule flow and compressibility [40,55]. Once manufactured, effervescent tablets require protective packaging, commonly individually wrapped strips, foil-sealed tubes with desiccant, or blister packaging with high-barrier films, since even brief exposure to ambient humidity can initiate localised effervescence, softening, or caking that compromises both mechanical integrity and chemical stability of the moisture-sensitive vitamin fraction [41,56].
Vitamin B12 is recognised as strongly hygroscopic and, while comparatively stable in neutral aqueous solution, undergoes accelerated decomposition at temperatures above approximately 120 °C and at extreme pH values (below 3 or above 8), conditions that can transiently arise within an effervescent tablet matrix during dissolution or under accelerated stability testing [10,57]. Pyridoxine similarly demonstrates reduced stability on heating in neutral-to-basic solution and benefits from photoprotection during storage [46,58]. Empirical single-ingredient versus multi-ingredient comparisons consistently show that co-formulation, rather than temperature or humidity alone, is often the dominant driver of accelerated cobalamin loss, reinforcing the case for stability indicating analytical methods (typically stability-indicating HPLC) capable of resolving cobalamin, pyridoxine, and their respective degradation products within the complex effervescent matrix [9,46].
Bioavailability
For the antacid component, bioavailability is not the primary pharmacological objective, since neutralising agents act locally within the gastric lumen; however, systemic exposure to absorbable cations (notably sodium, calcium, magnesium, and aluminium) remains a relevant safety consideration, particularly with repeated or high-dose use [18,19]. For the vitamin components, oral bioavailability is a central formulation and clinical concern, especially for cobalamin, whose absorption is capacity-limited by intrinsic factor-mediated uptake in the terminal ileum, restricting efficient absorption of a single oral dose to approximately 1–2% of very large doses once the intrinsic factor pathway is saturated, with the remainder relying on a slower, passive diffusion mechanism [59,60].
Despite this apparent inefficiency, a substantial and consistent body of clinical evidence indicates that high-dose oral cobalamin (typically 1,000–2,000 micrograms daily) can normalise serum B12 and reduce homocysteine as effectively as intramuscular injection in patients with confirmed deficiency, including some with malabsorptive conditions, because the passive diffusion component becomes clinically sufficient at pharmacological doses even though fractional absorption is low [59,61,62]. A 2018 Cochrane systematic review of randomised trials comparing oral and intramuscular B12 replacement concluded that high-dose oral therapy achieves comparable short-term haematological and neurological responses to injectable therapy, while offering practical and cost advantages by avoiding the burden of repeated clinical visits [61]. More recent meta-analytic work extends this comparison to sublingual administration, again finding no statistically significant differences in efficacy across oral, sublingual, and intramuscular routes, and further reports that increasing oral dose does not proportionally improve outcomes, suggesting that absorption efficiency of the delivered formulation, rather than raw dosage, is the more important determinant of clinical response [59,63].
This has direct relevance for effervescent tablet design: because the effervescent dosage form delivers the vitamin fraction in aqueous solution rather than as an intact solid, gastric mixing and mucosal contact may be enhanced relative to conventional tablets, potentially improving the practical, if not fractional, bioavailability of the B12/B6 load, although this hypothesis has not yet been rigorously tested for the antacid-vitamin combination specifically and represents an identified research gap (Section 15). Novel oral B12 delivery technologies, including sucrosomial and lipid vesicle-based systems, have demonstrated superior serum B12 elevation compared with conventional oral formulations in head-to-head trials and illustrate a broader trend toward absorption-enhancing formulation strategies that could plausibly be adapted to the effervescent platform [60,64]. Pyridoxine, by contrast, is efficiently absorbed by passive diffusion across the gastrointestinal tract regardless of formulation, such that bioavailability optimisation for the B6 component is of comparatively minor concern relative to its chemical stability within the matrix [30].
Manufacturing Technologies
Effervescent tablets can be manufactured by direct compression, wet granulation, dry (roller) granulation, or melt granulation, each carrying distinct trade-offs relevant to an antacid-vitamin combination product [40,65]. Direct compression is used comparatively rarely for effervescent systems because of the hygroscopicity and poor compressibility of unprocessed effervescent powders and the risk of premature acid-base reaction during blending, and generally requires preprocessed, moisture-protected excipients to be viable [40]. Wet granulation remains the most widely used technique, typically employing a non-aqueous granulating solvent such as ethanol to minimise premature reaction, with the acidic and alkaline components granulated separately before final blending; this approach produces strong, uniform granules with good flow and compressibility but requires solvent-handling infrastructure and rigorous drying to very low residual moisture, often below 0.15% loss-on-drying, before compression [55,66,67].
Dry granulation, most commonly via roller compaction, avoids solvent and associated drying steps entirely, making it attractive for moisture-sensitive combinations, though it typically requires a higher proportion of excipients relative to active ingredient to achieve acceptable granule properties, which can constrain the achievable antacid or vitamin payload per tablet [40,65]. Melt granulation is the least widely adopted route, owing to the need for specialised, temperature controlled equipment and the risk of thermal degradation to heat-labile vitamin actives, but it offers a genuinely water-free alternative for particularly hygroscopic formulations [40].
Across all manufacturing routes, environmental humidity control (generally maintained at or below 20–25% RH), use of sealed or dehumidified processing equipment, and minimisation of hold times between granulation, blending, and compression are considered critical process controls [55,68]. Specialised granulation technologies, such as vacuum-assisted or fluidised-bed spray granulation with controlled drying temperatures, have been developed specifically to reduce the likelihood of uncontrolled effervescent chain reactions during processing while achieving low residual moisture, and are of particular relevance where a heat- and moisture-sensitive active such as cyanocobalamin must be incorporated into the effervescent granule [69,70]. Tablet presses used for effervescent compression are typically adapted with enhanced dust extraction and moisture exclusion relative to standard rotary presses, reflecting the distinct handling requirements of this dosage form [40].
Quality by Design (QbD) & Regulatory Aspects
Quality by Design, as codified in the ICH Q8(R2) guideline, represents a systematic, science- and risk-based approach to pharmaceutical development in which quality is built into the product and process from the outset rather than tested for retrospectively in the finished dosage form [71,72]. The framework begins with definition of the Quality Target Product Profile (QTPP), a prospective summary of the quality characteristics the effervescent antacid-vitamin tablet must possess to ensure its intended safety and efficacy, from which Critical Quality Attributes (CQAs), such as disintegration time, moisture content, assay of each active, and effervescence time, are identified [71,73]. Critical Process Parameters (CPPs), including granulation humidity, drying endpoint, compression force, and blending time, are then linked to these CQAs through risk assessment tools such as failure mode and effects analysis (FMEA) or Ishikawa diagrams, complemented where appropriate by design-of-experiments methodology to establish a multidimensional design space within which the process can be operated with assured quality [73,74].
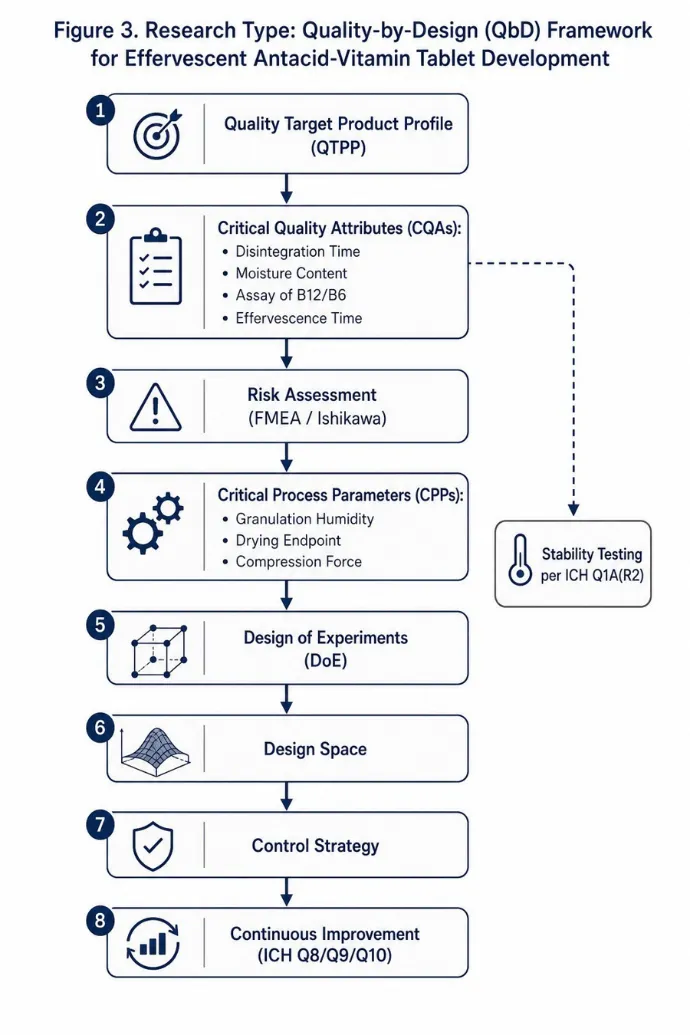
Figure 3. Research-type schematic: Quality-by-Design (QbD) framework for effervescent antacid-vitamin tablet development (see Section 11).
ICH Q9 (Quality Risk Management) and Q10 (Pharmaceutical Quality System) extend this framework across the product lifecycle, formalising risk-prioritisation of CQAs/CPPs and embedding continuous improvement and control-strategy maintenance into ongoing manufacture, while regulatory initiatives such as Process Analytical Technology (PAT) encourage real-time, inprocess monitoring, for example of granule moisture content, as an alternative or complement to end-product testing [74,75]. A systematic review of QbD implementation in regulatory dossiers submitted to European authorities between 2014 and 2019 found that QbD-based development and control-strategy documentation facilitated regulatory acceptance, particularly for complex or modified-release dosage forms, and supported more flexible post-approval change management [75,76].
For an effervescent antacid-vitamin combination product specifically, applying QbD would entail systematically mapping how variations in acid-to-carbonate ratio, granulation method, drying endpoint, and packaging barrier properties affect the CQAs of moisture content, cobalamin/pyridoxine assay, disintegration and effervescence time, and content uniformity, thereby establishing a control strategy robust enough to accommodate the inherent chemical sensitivity of the vitamin fraction within a moisture-reactive effervescent matrix [72,76]. Stability testing under ICH Q1A(R2) conditions, appropriate photostability assessment per ICH Q1B where pyridoxine or cobalamin photolability is a concern, and adherence to relevant compendial monographs (e.g., USP/Ph. Eur. specifications for effervescent tablets) collectively constitute the regulatory backbone against which such a product would be evaluated for marketing authorisation [52,71].
Evaluation Parameters
Pharmacopoeial and literature-standard evaluation of effervescent tablets encompasses a battery of physical and chemical tests broadly analogous to, but distinct in acceptance criteria from, those applied to conventional compressed tablets. Weight variation, thickness, and hardness are assessed using standard tablet-testing equipment, with typical reported hardness values for effervescent tablets in the range of approximately 3–5 kg/cm², generally lower than for conventional immediate-release tablets to permit rapid disintegration [77,78]. Friability, measured using a USPtype friabilator, is subject to a distinct acceptance threshold for effervescent, chewable, and orodispersible tablets, which are permitted to exceed the standard 1% weight-loss limit applied to conventional compressed tablets, reflecting their intentionally softer, more friable structure [78,79].
Disintegration and effervescence time, defined as the interval required for complete tablet breakdown and cessation of gas evolution upon immersion in water (typically at 15–25 °C per compendial methods, or at 37 °C in physiological simulations), constitute the principal functional Critical Quality Attribute for this dosage form, with acceptance criteria commonly specifying complete disintegration within approximately three to five minutes; disintegration time is influenced by formulation variables including effervescent salt composition, particle size distribution, compression force, and tablet porosity, as well as process and storage humidity [77,80,81]. Solution pH after complete dissolution is measured to confirm both palatability and appropriate antacid neutralising behaviour, while carbon dioxide content is quantified gravimetrically or volumetrically as a direct index of the completeness and reproducibility of the effervescent reaction [77,82].
Chemical evaluation includes content uniformity and assay of each active (antacid salt, cobalamin, and pyridoxine) by validated, stability-indicating chromatographic methods (typically HPLC), together with related-substance and degradation-product testing to satisfy ICH Q3A/Q3B impurity thresholds [52,54]. Moisture content, determined by loss-on-drying or Karl Fischer titration, is monitored as both an in-process control during granulation/drying and a finished-product release specification, given its direct mechanistic link to both effervescent reactivity and vitamin stability
[66,83]. Collectively, these evaluation parameters, hardness, friability, disintegration/effervescence time, solution pH, CO2 content, moisture content, and assay/content uniformity of each active, define the quality profile against which formulation optimisation and batch release decisions for the antacid-vitamin effervescent tablet are made [77,80].
Table 2. Standard evaluation parameters, test methods, and typical acceptance criteria for effervescent antacid-vitamin tablets.
|
Evaluation Parameter |
Standard Test Method |
Typical Acceptance Range / Purpose |
|
Hardness |
Tablet hardness tester (breaking-force apparatus) |
Approximately 3–5 kg/cm² — lower than conventional tablets to permit rapid disintegration |
|
Friability |
USP-type friabilator (100 revolutions) |
Effervescent, chewable, and orodispersible tablets are exempted from the standard 1% weight-loss limit applied to conventional compressed tablets |
|
Disintegration / effervescence time |
Immersion in water per USP/Ph. Eur. apparatus or beaker method |
Complete disintegration and cessation of gas evolution typically within 3–5 minutes |
|
Solution pH |
pH meter on the fully dissolved tablet solution |
Confirms palatability and appropriate antacid neutralising behaviour |
|
Carbon dioxide (CO₂) content |
Gravimetric or volumetric determination |
Index of the completeness and batch-to-batch reproducibility of the effervescent reaction |
|
Moisture content |
Loss-on-drying or Karl Fischer titration |
In-process and release specification; directly linked to both effervescent reactivity and vitamin (B12/B6) stability |
|
Content uniformity / assay |
Validated, stability-indicating HPLC |
Quantifies antacid salt, cobalamin, and pyridoxine content per ICH Q3A/Q3B impurity and assay limits |
Compiled from pharmacopeial and formulation-evaluation literature [66,77–83].
Clinical Evidence
Direct clinical trial evidence for a combined effervescent antacid-vitamin B12/B6 product is limited, and the available evidence base is therefore assembled largely from studies of the individual components and of the broader antacid-B12 relationship that motivates the combination. Evidence linking chronic acid-suppressive therapy to vitamin B12 deficiency is genuinely mixed. Several systematic reviews and meta-analyses, together with large cohort studies, report a statistically significant association between long-term acid suppression and biochemical markers of B12 insufficiency; one meta-analysis of pooled data reported an odds ratio of approximately 1.42 (95% CI 1.16–1.73) for B12 deficiency among chronic acid-suppressive drug users, with a cohort study from a tertiary hospital reporting B12 deficiency rates as high as 54% among longterm omeprazole users, and case-control data suggesting the strongest association in younger patients (under 30 years) and in women [3,22,24,84]. Conversely, other rigorously conducted meta-analyses of comparable studies found no statistically significant difference in serum vitamin B12 or homocysteine between chronic users and non-users, and some case-control data in older hospitalised patients likewise found no association [4,23]. This heterogeneity likely reflects differences in the diagnostic biomarkers used (serum cobalamin versus methylmalonic acid or homocysteine), variable definitions of chronic use, and residual confounding by dietary intake and comorbidity, and it means the antacid-vitamin combination rationale should be presented as biologically plausible and clinically prudent rather than as a definitively proven preventive intervention.
Evidence for oral vitamin B12 replacement efficacy is considerably more consistent. Randomised controlled trials and subsequent systematic reviews, including a Cochrane review, have found that high-dose oral cyanocobalamin achieves haematological and neurological normalisation comparable to intramuscular injection in patients with confirmed deficiency [61,62]. A more recent systematic review and meta-analysis extending this comparison to sublingual administration similarly found no significant difference in efficacy across oral, sublingual, and intramuscular routes for restoring serum cobalamin and reducing homocysteine [59]. These findings lend clinical plausibility to the notion that an orally delivered, effervescent B12/B6 formulation could meaningfully support vitamin status in an at-risk population, even though fractional intestinal absorption per dose remains low.
For vitamin B6, clinical trial evidence specific to co-administration with antacids is essentially absent from the published literature, and existing controlled data on pyridoxine supplementation relate predominantly to other indications, such as prevention of isoniazid-induced neuropathy or correction of biochemical B6 deficiency in inflammatory conditions, rather than to gastric acid suppression-related depletion [34,36]. This represents a clear and specific evidence gap: no identified randomised controlled trial has directly evaluated a combined effervescent antacid-B12B6 product against either antacid alone or antacid plus separately administered vitamins for either symptomatic gastrointestinal endpoints or vitamin-status biomarkers, and this absence should be regarded as a priority for future clinical investigation (Section 15).
Emerging Technologies
Additive manufacturing, particularly fused deposition modelling and binder-jet three-dimensional printing, has emerged as a transformative platform for personalised oral dosage forms since the 2015 regulatory approval of the first three-dimensionally printed tablet, enabling on-demand fabrication of orodispersible tablets, multilayer or multicompartment dosage forms that physically separate incompatible actives, and dose-flexible formulations tailored to individual patient needs such as paediatric or geriatric dosing [85–88]. For an antacid-vitamin combination, three dimensional printing offers a conceptually attractive route to physically segregate the vitamin fraction from the reactive effervescent core within discrete printed compartments, potentially mitigating the co-formulation-driven cobalamin degradation described in Section 7, although this application has not yet been reported specifically for effervescent antacid systems and remains a theoretical extension of the technology [86,87].
Orodispersible film technology, a thin, flexible polymeric film designed to dissolve rapidly in the oral cavity, represents an alternative or complementary rapid-delivery platform to the effervescent tablet, with recent reviews highlighting the integration of nanoparticle carriers and three dimensional printing techniques to enable multilayer films that similarly separate incompatible actives while enhancing dissolution and, potentially, mucosal absorption of the vitamin payload [84].
Microencapsulation and nanocarrier-based taste-masking and stabilisation technologies constitute a further area of active development directly relevant to this combination product. Spray-drying and spray-chilling encapsulation of cyanocobalamin within biopolymer or lipid matrices has been shown to improve stability against environmental stressors while simultaneously masking its metallic taste, and comparable coating strategies using pH-responsive or ion-exchange polymers have been used to mask the taste of other bitter actives in fast-disintegrating and effervescent dosage forms [48,49,92,93]. Nanocapsule-based taste-masking systems, for example those employing polyamide shells formed by interfacial polycondensation, illustrate a further extension of this principle that could, in future work, be evaluated for cobalamin protection within an effervescent matrix [50]. Collectively, these emerging technologies point toward a next generation of antacid-vitamin effervescent products in which physical or chemical compartmentalisation of the vitamin fraction, rather than co-formulation within a single homogeneous granule, may offer the most promising route to simultaneously achieving chemical stability, acceptable palatability, and reliable bioavailability.
Challenges and Research Gaps
Several interconnected challenges constrain the development of a robust effervescent antacidvitamin B12/B6 tablet. First, the physicochemical incompatibility between cobalamin and both the acidic and basic components of the effervescent-antacid matrix, compounded by well-documented interactions between cobalamin and co-formulated B-vitamins such as thiamine, creates a narrow formulation window in which sufficient chemical stability can be achieved without resorting to complex and costly compartmentalisation strategies [9,46]. Second, the intrinsic moisture sensitivity of effervescent systems is difficult to reconcile with the additional hygroscopicity of cyanocobalamin, requiring exceptionally stringent manufacturing humidity control and highbarrier packaging that increase production cost and complexity relative to either a plain antacid or a plain vitamin effervescent product manufactured separately [10,55].
Third, as detailed in Section 13, the clinical evidence base directly supporting the combined product is essentially absent: no randomised controlled trial identified in this review has evaluated the combined antacid-B12-B6 effervescent formulation against relevant comparators for either symptomatic or biomarker-based endpoints, and the underlying premise that antacid or acid suppressive use meaningfully depletes vitamin B12 is itself supported by conflicting meta-analytic evidence [3,4,22,23]. This creates uncertainty as to the appropriate target population, optimal vitamin dose, and expected magnitude of clinical benefit, all of which are necessary inputs for rational Quality Target Product Profile definition under a QbD development approach.
Fourth, bioavailability of the vitamin fraction when delivered in effervescent, pre-dissolved form alongside an antacid has not been directly studied; while oral high-dose cobalamin is well established as clinically effective in other formulations, whether co-administration with an antacid solution alters gastric transit, mucosal contact time, or passive-diffusion-mediated absorption remains an open pharmacokinetic question [59,60]. Finally, regulatory and analytical challenges persist around establishing stability-indicating assays capable of simultaneously resolving multiple degradation pathways for two chemically dissimilar vitamins within a reactive, gas-evolving matrix, and around justifying an appropriate shelf life given the accelerated degradation observed in some multi-ingredient B-vitamin preparations [9,52]. Addressing these four gaps, formulation compatibility, moisture/stability management, clinical evidence generation, and bioavailability characterisation, represents the principal research agenda for advancing this dosage form from laboratory concept to a commercially and clinically validated product.
Future Perspectives
Future development of next-generation effervescent antacid-vitamin tablets is likely to proceed along several converging trajectories. Formulation science will probably continue to move toward physical or chemical compartmentalisation of the vitamin fraction, whether through microencapsulation, multilayer or bilayer tableting, or additive-manufacturing-enabled multicompartment dosage forms, as a means of decoupling cobalamin and pyridoxine stability from the reactive effervescent-antacid core without sacrificing the single-dosage-unit convenience that motivates the combination in the first place [86,92]. Continued application of QbD principles, supported by design-of-experiments-based optimisation of granulation method, acid-carbonate ratio, and packaging barrier properties, should progressively narrow the design space needed to guarantee both effervescent performance and vitamin stability across realistic storage conditions [72,76].
On the clinical side, dedicated randomised controlled trials comparing the combined antacid-B12B6 effervescent product against antacid alone, and evaluating both symptomatic gastrointestinal outcomes and objective vitamin-status biomarkers (serum cobalamin, methylmalonic acid, homocysteine, and plasma pyridoxal-5'-phosphate), are needed to resolve the current evidentiary uncertainty and to define the patient populations, such as elderly patients or those on established chronic acid-suppressive therapy, most likely to derive meaningful benefit [3,22,84]. Pharmacokinetic studies specifically characterising oral B12/B6 bioavailability when delivered in effervescent, pre-dissolved solution, potentially benchmarked against emerging absorption enhancing oral B12 technologies such as sucrosomial or lipid-vesicle carriers, would help establish whether the effervescent route offers any practical absorption advantage over conventional tablet based multivitamin supplementation [60,64].
More broadly, the convergence of three-dimensional printing, nanoencapsulation, and real-time process analytical technology is expected to enable increasingly personalised, stable, and palatable multi-active oral dosage forms across pharmaceutical practice, and the effervescent antacid vitamin tablet represents a tractable and clinically motivated test case for translating these broader technological trends into a widely accessible, over-the-counter or pharmacist-recommended product [85,87].
CONCLUSION
Effervescent antacid tablets fortified with vitamins B12 and B6 address a coherent, if not yet definitively proven, clinical rationale: rapid, palatable relief of acid-related gastrointestinal symptoms combined with supplementation of micronutrients whose status may be compromised by the acid-suppressive context in which such products are used. The pharmaceutical science underpinning this dosage form, spanning excipient selection, granulation technology, stability management, and Quality by Design-guided process control, is well developed in the broader effervescent tablet literature, but its specific application to a chemically challenging antacid cobalamin-pyridoxine combination remains comparatively underexplored. Persistent formulation incompatibilities, stringent moisture-control requirements, and, most importantly, a limited and partly conflicting direct clinical evidence base constitute the principal barriers to widespread adoption of this dosage form. Targeted formulation innovation, particularly compartmentalisation strategies for the vitamin fraction, combined with dedicated stability and clinical studies of the combined product, would substantially strengthen the scientific and regulatory foundation for next-generation effervescent antacid-vitamin B12/B6 tablets and support their rational, evidence based use in clinical practice.
REFERENCES

Vaijayanti Kulkarni, Pratiksha Jadhao, Next-Generation Effervescent Antacid Tablets with Vitamins B12 and B6: A Comprehensive Review of Formulation, Clinical Evidence, and Future Directions, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 1940-1958. https://doi.org/10.5281/zenodo.21280762
 10.5281/zenodo.21280762
10.5281/zenodo.21280762