
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Kaumarbhritya Balroga, Banaras Hindu University
Nipah virus infection is a highly lethal emerging zoonotic disease characterised by acute febrile illness, encephalitis, respiratory failure, and high case fatality rates. Recurrent outbreaks in South and Southeast Asia, including India and Bangladesh, highlight ongoing risks related to ecological spillover, healthcare transmission, and limited therapeutic options. Currently, no licensed antiviral therapy or vaccine is available, and management relies primarily on early diagnosis, strict infection control, and intensive supportive care. Ayurveda conceptualises communicable and epidemic diseases under Aupasargika Roga, Agantuja Vyadhi, and Janapadodhwamsa, while severe systemic febrile illness corresponds to Sannipata Jwara. To comprehensively review the epidemiology, pathogenesis, clinical spectrum, diagnosis, and modern management of Nipah virus infection and to critically correlate these findings with classical Ayurvedic concepts, therapeutic principles, and preventive strategies for integrative application. A narrative review was conducted using peer-reviewed biomedical databases and classical Ayurvedic texts. Contemporary literature on Nipah virus epidemiology, virology, clinical manifestations, diagnostics, and management was synthesised alongside references from Charaka Samhita, Sushruta Samhita, Ashtanga Hridaya, and authoritative Nighantu texts. Pharmacological evidence for selected medicinal plants and formulations traditionally indicated in febrile and infectious conditions was critically appraised. Nipah virus exhibits endothelial and neurotropic pathogenicity leading to encephalitis, respiratory compromise, and multisystem involvement, with mortality frequently exceeding 40–70%. Ayurvedic analysis correlates this condition with Agantuja Sannipata Jwara within the framework of Aupasargika Roga and Janapadodhwamsa. Samprapti mapping demonstrated involvement of Tridosha (Vata dominance in advanced stages), Rasa, Rakta, Majja, and Ojas, with impairment of Pranavaha and Majjavaha srotas. Classical management principles, including nidana parivarjana, langhana, pachana, jwara shamana, and rasayana, are aligned with modern supportive care goals. Selected medicinal plants demonstrated supportive immunomodulatory, anti-inflammatory, neuroprotective, and respiratory benefits. Ayurveda provides a coherent theoretical framework and supportive strategies that complement modern biomedical management when applied ethically under medical supervision, potentially enhancing recovery support and preventive preparedness without replacing evidence-based care.
Nipah virus (NiV) is a dangerous zoonotic RNA virus belonging to the Henipavirus genus within the Paramyxoviridae family. It was first identified in 1998 and 1999. Nipah virus is known for its high death rate, its ability to spread between people, and the lack of approved antiviral treatments or vaccines. The infection usually starts with a sudden fever and can quickly cause brain inflammation, breathing problems, and multiple organ failure.(Ang BSP et al. Clin Infect Dis.) Outbreak death rates have ranged from 40% to over 75%, depending on healthcare resources and response. (WHO. Nipah virus Fact Sheet. Chua KB, et al. Science. The virus was first discovered during a major outbreak of brain inflammation among pig farmers in Malaysia and Singapore. More than 260 people were infected and over 100 died, leading to significant economic losses from culling livestock (Chua et al., 2000). Later research confirmed it was a new paramyxovirus, different from the Hendra virus. (Goh KJ et al. N Engl J Med.) Since then, NiV has caused repeated outbreaks in Bangladesh and India, with increasing evidence of person-to-person and hospital-based transmission (Luby et al., 2009; Arunkumar et al., 2019). India has experienced several Nipah outbreaks in West Bengal (2001, 2007) and Kerala (since 2018). The return of suspected and confirmed cases in West Bengal in January 2026 indicates that eastern India remains at risk due to its dense population, the presence of bats, cross-border travel, and healthcare exposure. From a public health perspective, NiV is an example of a new zoonotic threat linked to environmental changes, global movement, and climate change (Plowright et al., 2015). Ayurveda, India’s traditional medical system, explains epidemics and contagious diseases with concepts such as Agantuja Vyadhi, Aupasargika Roga, and Janapadodhwamsa. Severe fevers are called Sannipata Jwara. (Charaka Samhita, Susruta Samhita). These ideas help explain how diseases spread, their causes, and who is most at risk. Combining these traditional views with modern medicine may improve prevention, care, and recovery, provided evidence-based practices are used

FIGURE 1: The detailed Overview of the Nipah virus and Ayurvedic correlation
2. MODERN LITERATURE REVIEW REGARDING NIPAH VIRUS
Aetiology and Virology
Nipah virus is an enveloped, single-stranded, negative-sense RNA virus with a genome approximately 18.2 kb in length. (Wong KT et al. Am J Pathol.) Its genome codes for six structural proteins: nucleocapsid (N), phosphoprotein (P), matrix protein (M), fusion protein (F), attachment glycoprotein (G), and large polymerase protein (L). These proteins help the virus attach to cells, fuse with membranes, replicate, assemble, and avoid the immune system (Broder et al., 2013). The virus targets endothelial cells, neurons, smooth muscle cells, and respiratory epithelium. This explains why the central nervous system, lungs, and blood vessels are often affected in clinical disease (Negrete et al., 2005). After entering the cell, the F protein helps the virus fuse with the cell membrane, allowing the viral complexes to enter the cytoplasm and start replication. (Tan CT et al.Ann Neurol.)
Pathogenesis and Host Response
NiV infection directly harms cells and strongly activates the immune system. As the virus multiplies in blood vessel cells, it causes inflammation, blood clots, and small areas of tissue death in organs, especially the brain and lungs. This can lead to brain swelling and nerve damage. In severe cases, the immune response can become uncontrolled, similar to cytokine storms seen in other viral brain infections (Wong et al., 2002). Fruit bats from the Pteropus genus are the main natural hosts of NiV. Studies have found the virus and antibodies in bat populations across South and Southeast Asia (Epstein et al., 2006). Bats can spread the virus without symptoms through their urine, saliva, and leftover fruit, contaminating the environment and infecting people. Domestic animals, especially pigs, can spread the virus. In the Malaysian outbreak, pigs became infected by eating fruit contaminated with bat droppings, and then passed the virus to farmers and slaughterhouse workers (Chua et al., 2000). Other animals, such as horses, goats, and cats, can also be infected in some cases.
Onset and Incubation Period
The time from infection to symptoms for the Nipah virus is usually 4 to 14 days, but in rare cases, it can be up to 45 days (WHO, 2023; Tan et al., 1999). This range depends on the amount of virus, how it enters the body, the person’s immunity, and the virus strain.
Prodromal Phase
The illness commonly begins with nonspecific symptoms, including high-grade fever, headache, myalgia, generalised body aches, fatigue and malaise, sore throat, and nausea or vomiting. These symptoms are very similar to those of other viral illnesses, such as flu, dengue, or viral meningitis, which can delay diagnosis. Within 1 to 3 days after the fever begins, some patients develop nervous system symptoms such as dizziness, sleepiness, confusion, or changes in awareness. Others may have a cough, trouble breathing, or low oxygen levels if the lungs are affected. Severe Nipah infection can worsen quickly, so early transfer to advanced hospitals is important.
Incidence and Epidemiology
Since 1998, Nipah virus outbreaks have been documented primarily in Malaysia and Singapore (1998–1999), Bangladesh (2001–present), and India (West Bengal, Kerala). So far, ongoing transmission has not been seen outside South and Southeast Asia. However, evidence of henipavirus exposure in other regions raises concerns that the virus could spread further.
Bangladesh has reported nearly annual outbreaks since 2001, often during the winter months. Epidemiological investigations consistently implicated consumption of raw date palm sap contaminated by bat secretions as a primary route of transmission (Luby et al., 2009). Person-to-person transmission has been more frequent in Bangladesh than in Malaysia, contributing to higher fatality rates.
India experienced: Siliguri outbreak (2001), where Hospital-based transmission involved multiple healthcare workers. Nadia district outbreak (2007), where a rural cluster with a high fatality rate, and in Kerala outbreaks (2018 onward), multiple sporadic events with improved surveillance and containment. Improved disease monitoring and quick-response teams have helped detect cases earlier in recent years, but environmental risks remain. (Chadha MS et al. Emerg Infect Dis. Arunkumar G et al. J Infect Dis.)
Environmental and Ecological factors
Deforestation and habitat fragmentation, Urban expansion into bat habitats, Climate variability affecting bat migration and fruiting patterns, Intensification of agriculture and livestock farming and increased human mobility and healthcare exposure. All these factors increase the chances of people coming into contact with bats and new diseases emerging (Plowright et al., 2015).
Recent Nipah outbreak in West Bengal (January 2026)
In early January 2026, suspected and laboratory-confirmed Nipah virus infections were reported in the North 24 Parganas and Kolkata districts of West Bengal. Two healthcare workers were identified with severe febrile illness and neurological symptoms. Initial screening samples tested positive at a regional VRDL laboratory, and confirmation was obtained from the National Institute of Virology (NIV), Pune. Public health authorities initiated immediate isolation of cases, contact tracing of healthcare workers and household contacts, quarantine measures, and reinforcement of infection control protocols in hospitals. Rapid response teams were deployed to assess epidemiological links, including travel history, hospital exposure, and potential zoonotic contacts. Preliminary reports suggested possible healthcare-associated transmission; however, full outbreak investigation and genomic sequencing were ongoing at the time of reporting. This event shows that densely populated eastern India remains vulnerable and highlights the need for hospital preparedness, early detection, and strong disease monitoring systems. (NIV Pune Bulletin 2026).
Transmission (WHO. Nipah Virus Fact Sheet)
In Animal-to-Human Transmission, Pigs act as amplification hosts. Occupational exposure among farmers, veterinarians, and slaughterhouse workers. In Human-to-Human Transmission, Close physical contact, Exposure to respiratory droplets and body fluids, Healthcare-associated transmission during patient care and Poor infection control practices. Nosocomial transmission has been documented in multiple outbreaks, underscoring the importance of strict adherence to infection prevention protocols.
Clinical Features
Nipah virus infection exhibits a broad clinical spectrum ranging from asymptomatic or mild febrile illness to rapidly progressive encephalitis, severe respiratory failure, and death. Clinical manifestations vary depending on viral strain, inoculum dose, route of exposure, host immune response, and timeliness of medical intervention. (Ang BSP et al. Clin Infect Dis. WHO. Nipah virus Fact Sheet. Chua KB, et al. Science.)
Early (Prodromal) Phase
The prodromal phase usually begins abruptly after the incubation period and is characterised by nonspecific systemic symptoms that mimic common viral illnesses. Common early manifestations include: High-grade fever – persistent and often poorly responsive to routine antipyretics, Headache – diffuse or frontal, Myalgia and arthralgia – generalised body ache, Malaise and weakness – fatigue, anorexia, Sore throat and cough – mild respiratory symptoms, Nausea and vomiting – gastrointestinal upset. These features have been consistently reported in Malaysian, Bangladeshi, and Indian outbreaks and are responsible for delayed clinical suspicion because they resemble influenza, dengue, or viral meningitis. (Wong KT et al. Am J Pathol. Tan CT, et al. Ann Neurol.)
Neurological Manifestations include Drowsiness and altered sensorium, Disorientation and confusion, Seizures (focal or generalised), Rapid progression to coma, Focal neurological deficits and Autonomic instability. Neuroimaging frequently demonstrates multifocal cortical and subcortical lesions, microinfarctions, and brainstem involvement consistent with vasculitis and viral neurotropism. Neuropathological studies demonstrate endothelial infection, syncytial formation, and necrotizing vasculitis. (Luby SP, et al. Emerg Infect Dis. Chadha MS, et al. Emerg Infect Dis.)
Respiratory Manifestations include Cough and dyspnea; tachypnea and hypoxemia; pneumonia; And Acute respiratory distress syndrome (ARDS). Higher viral loads in respiratory secretions increase transmissibility during coughing and aerosol-generating procedures. In Bangladesh and India, respiratory symptoms correlate with increased secondary transmission. (Wong KT et al. Arunkumar G et al. J Infect Dis.)
Cardiovascular and systemic manifestations include hypotension and shock resulting from systemic inflammatory response, Arrhythmias secondary to autonomic dysfunction and electrolyte imbalance, and Multi-organ dysfunction involving the liver, kidneys, and coagulation systems. Systemic endothelial injury contributes to capillary leak syndrome and hemodynamic instability. (Chua KB, et al. Science. Luby SP, et al. Emerg Infect Dis.)
Children may initially present with nonspecific fever and lethargy but deteriorate rapidly. Elderly patients and individuals with comorbidities demonstrate higher mortality and prolonged neurological sequelae. (Hsu VP, et al. Emerg Infect Dis.)
Acute Neurological Complications: Severe encephalitis with cerebral oedema, Status epilepticus, raised intracranial pressure and Brainstem dysfunction and cranial nerve palsy. Mortality is strongly correlated with the severity of encephalitis and delayed intensive care admission. (Luby SP, et al. Emerg Infect Dis.Chadha MS, et al. Emerg Infect Dis.
Respiratory Complications like Acute respiratory distress syndrome (ARDS), Secondary bacterial pneumonia and Ventilator-associated complications. Respiratory failure contributes significantly to mortality and to the risk of nosocomial transmission. (Wong KT et al. Am J Pathol. Arunkumar G, et al. J Infect Dis.
Systemic Complications include Septic shock-like syndrome, Acute kidney injury, Hepatic dysfunction, Electrolyte Imbalance and Coagulopathy. These complications reflect widespread endothelial damage and cytokine-mediated inflammation. (Chua KB, et al. Science.).
Long-Term Sequelae: Survivors may develop Cognitive impairment, Memory loss, Personality changes, Motor deficits, and chronic fatigue And Relapse encephalitis months or years later. Relapse encephalitis is a unique feature reported in Nipah survivors and indicates viral persistence or immune-mediated mechanisms. (Luby SP, et al. Emerg Infect Dis. Goh KJ, et al. N Engl J Med.)
Diagnosis
Case Suspicion: Suspected Nipah virus infection should be considered in patients presenting with: Acute febrile illness with neurological or respiratory symptoms, or Exposure to the outbreak area or a confirmed case or Healthcare or animal exposure or Consumption of potentially contaminated food products.
Laboratory Confirmation: Definitive diagnostic tests include Real-time RT-PCR, with specimens from throat swabs, nasopharyngeal swabs, blood, urine, and CSF. Most sensitive during acute illness. Serological assays (IgM/IgG ELISA), which are useful during later or convalescent stages, and Virus isolation. Laboratory testing must follow biosafety protocols due to the high infectivity of the agent. (Epstein JH, et al. Curr Infect Dis Rep.).
Preliminary Investigations: CBC, liver and renal function tests, Electrolytes, ABG, Chest imaging, MRI brain, and EEG.
Differential diagnoses are Japanese encephalitis, Herpes encephalitis, Dengue, Leptospirosis, Scrub typhus, Bacterial meningitis, Influenza or COVID-19
Modern Medical Management:
There are currently no guidelines on definitive antiviral therapy or a vaccine for Nipah virus infection. (Plowright RK et al. Proc Biol Sci.)
Infection Control and Public Health Measures: Immediate isolation, PPE use, Dedicated isolation wards, Contact tracing and quarantine, Environmental disinfection and Community risk communication. Strict infection control significantly reduces secondary transmission.(WHO. Nipah virus Fact Sheet.)Wong KT, et al. Am J Pathol.)
Supportive Clinical Management
Respiratory Support by Oxygen therapy, HFNC / NIV or Mechanical ventilation.
Neurological Care by Antiepileptic therapy, ICP control and Sedation.
Hemodynamic support with IV fluids and vasopressors.
Renal Support includes Renal replacement therapy and Nutritional support after the acute phase. Supportive intensive care remains the cornerstone of survival. (Chua KB, et al. Science. Plowright RK, et al. Proc Biol Sci.
Experimental Therapies: Ribavirin – limited and inconsistent benefit; Monoclonal antibodies – under investigation; Vaccine phases – preclinical/early trials. No therapy is currently approved for routine clinical use.(Plowright RK et al. Proc Biol Sci. Negrete OA, et al. PNAS.)
Prognosis: Mortality remains high (40–75%). Early diagnosis, strict isolation, and aggressive supportive care improve outcomes. (WHO. Nipah virus Fact Sheet.Chua KB, et al. Science.Wong KT, et al. Am J Pathol.)
3. AYURVEDIC OVERVIEW OF NIPAH VIRUS INFECTION:
Although viral pathogens were unknown in classical Ayurveda, infectious and epidemic diseases were systematically conceptualised under well-defined frameworks. Nipah virus infection, characterised by rapid onset of fever, systemic toxicity, neurological dysfunction, respiratory compromise, and high transmissibility, can be comprehensively correlated with the classical concepts of Agantuja Vyadhi, Aupasargika Roga, Janapadodhwamsa, and Sannipata Jwara.
Agantuja Vyadhi (Externally Acquired Diseases): Acharya Charaka Samhita describes diseases caused by external factors such as trauma, poisons, microorganisms, environmental contamination, and unseen agents under the category of Agantuja Vyadhi. These disorders initially arise from external factors but later involve an internal doshic imbalance once the pathogenic influence penetrates the body tissues (Charaka Samhita, Nidana Sthana 1). Nipah virus represents a classic example of an Agantuja Hetu, in which viral entry via the respiratory or oral routes initiates systemic pathology. The early febrile phase corresponds to the initial antigenic insult, while later neurological and respiratory manifestations reflect doshic propagation.
“Agantava? ?ar?ram ?padyam?n? do??n prakopayanti” (Charaka Samhita, Nidana Sthana 1/11)
This indicates that external factors ultimately disrupt the endogenous doshas.
Aupasargika Roga (Contagious Diseases): Acharya Sushruta elaborates the concept of communicable diseases under Upasarga, describing disease transmission through physical contact, shared utensils, respiration, clothing, and close proximity (Sushruta Samhita, Nidana Sthana 5/33–34). This classical description remarkably parallels modern concepts of droplet, contact, and fomite transmission.
“prasangat G?tra sa?spar??t ni?v?s?t saha-bhojan?t
saha-?ayy?san?t vastra-m?ly?nulepan?t ca roga? sa?kr?mati”
(Sushruta Samhita, Nidana Sthana 5/33–34)
Nipah virus demonstrates efficient transmission in healthcare and household settings, which correlates precisely with the Aupasargika Roga hypothesis.
Janapadodhwamsa (Epidemic and Pandemic Disorders): Acharya Charaka describes large-scale population destruction caused by simultaneous illness in individuals of different constitutions due to vitiation of Vayu (air), Jala (water), Desha (land), and Kala (season) under the doctrine of Janapadodhwamsa (Charaka Samhita, Vimana Sthana 3/6–7).
“V?yu-jala-de?a-k?l?n?? du??atv?t janapada? vina?yati” (Charaka Samhita, Vimana Sthana 3/6–7)
This concept aligns closely with modern outbreak epidemiology, in which environmental contamination, ecological disruption, population density, and seasonal patterns contribute to epidemic spread. Repeated outbreaks of Nipah virus in specific geographical clusters (Bangladesh, Kerala, West Bengal) reflect localised Janapada Dushti due to bat habitat overlap, agricultural practices, food contamination, and healthcare exposure.
Sannipata Jwara (Acute Fever with complications): Acharya Charaka categorises severe, rapidly progressive febrile illnesses involving all three doshas as Sannipata Jwara, Tridoshaja in Prakrti, often associated with poor prognosis, delirium, organ dysfunction, and mortality (Charaka Samhita, Chikitsa Sthana 3).
“Sarva-do?a-prakop?t sannip?ta? jvara?” (Charaka Samhita, Chikitsa Sthana 3/1)
The multisystem inflammatory response, encephalopathy, respiratory failure, and shock observed in severe Nipah infection closely align with those observed in Sannipata Jwara.
4. Material and method:
A comprehensive literature search was conducted using electronic databases, including PubMed, Scopus, Web of Science, Google Scholar, and ResearchGate, for modern medical literature, and authenticated Ayurvedic textbooks such as Samhitas and Nighantus were also consulted. The search strategy included the following keywords: “ Nipah virus correlation in Ayurveda”, “Aupasargik Roga”, “ Janapadodhansha”, “Jwara chikitsa”, “Sannipatika Jwara”, “Agantuja Vyadhi”. Peer-reviewed original research articles, review articles, case reports, published articles, and outbreak reports are included in this search engine.
Nidana (Causative Factors): The probable etiopathogeneses of the Nipah virus are described in Table 1.
Table 1: Etiopathogenesis of Nipah virus in Ayurveda
|
Modern Factor |
Ayurvedic Correlation |
|
Viral exposure from bats/humans |
Agantu Hetu |
|
Environmental contamination |
Janapada Dushti |
|
Crowded healthcare exposure |
Aupasarga |
|
Low immunity |
Ojas Kshaya |
|
Metabolic stress |
Mandagni |
Srotas (vessels and lymphatics) involvement in Nipah virus, as per the Ayurvedic view, is described in TABLE 2 and TABLE 3
TABLE 2: Involvement of Srotas and manifestation of feature
|
Srotas |
Manifestation |
|
Pranavaha |
Dyspnea, hypoxia |
|
Majjavaha |
Seizures, coma |
|
Rasavaha |
Fever |
|
Manovaha |
Delirium |
Table 3: Samprapti Ghataka (Involvement of all pathogenic factors) in developing Nipah virus
|
Factor |
Status |
|
Dosha |
Tridosha (Vata dominant state) |
|
Dushya |
Rasa, Rakta, Majja, Ojas |
|
Agni |
Mandagni |
|
Ama |
Present |
|
Srotas |
Pranavaha, Majjavaha |
|
Rogamarga |
Madhyama |
|
Adhisthana |
Hridaya, Mastishka, Ura |
Dosha (factors for homeostasis of the body). Involvement in Nipah virus is-
Progression leads to Tridoshaja Sannipata dominance. The clinical progress of the Nipah virus is compared with Ayurvedic symptomatology in TABLE 4.
TABLE 4: Lakshana (Clinical Feature) Correlation with modern overview
|
Modern Clinical Feature |
Ayurvedic Lakshana |
|
High fever |
Jwara |
|
Myalgia |
Angamarda |
|
Headache |
Shirahshoola |
|
Cough |
Kasa |
|
Breathlessness |
Shwasa |
|
Altered sensorium |
Bhrama |
|
Seizures |
Apasmara |
|
Coma |
Murchha |
|
Hypotension |
Ojakshaya |
|
Fatigue |
Daurbalya |
Prognosis (Sadhya-asadhyatwa): Acharya Charaka identifies poor prognostic signs in Sannipata Jwara, such as persistent delirium, severe dyspnea, loss of consciousness, and Ojas depletion (Charaka Samhita, Indriya Sthana). These correlate clinically with severe encephalitis, ARDS, shock, and multi-organ failure in Nipah infection.
TABLE 5: Epidemiological angle in correlation to Janapadodhwamsa
|
Classical Parameter |
Modern relevance |
|
Vayu Dushti |
Aerosol spread |
|
Jala Dushti |
Food contamination |
|
Desha Dushti |
Habitat encroachment |
|
Kala Dushti |
Seasonal outbreaks |
Chikitsa Siddhanta (Principles of Management in Ayurveda): The management of externally acquired, contagious, epidemic febrile disorders in Ayurveda follows a structured hierarchy of principles aimed at eliminating causative factors, correcting metabolic derangements, pacifying aggravated doshas, protecting vital tissues, and restoring immunity. Nipah virus infection, which is correlated with Agantuja Sannipata Jwara, demands a cautious, stage-appropriate application of these principles as adjunctive supportive care.
Nidana Parivarjana (Elimination of Cause): Emphasis on avoidance of causative factors as the first and most important step in disease management.
“Hetu-vipar?ta sev? eva chikits?” (Charaka Samhita, Sutra Sthana 1/24)
In infectious diseases, this correlates with patient isolation, exposure avoidance, hygiene, and environmental sanitation.
Langhana (Therapeutic Fasting): Langhana is the primary intervention in Sama Jwara, where Ama blocks Srotas and impairs metabolism.
“Sama-jvare langhanam agreyam” (Ashtanga Hridaya, Chikitsa Sthana 1/1–2)
Gentle langhana includes a light diet, warm fluids, and digestive rest — carefully applied to avoid dehydration or weakness in critically ill patients.
Pachana and Deepana (Ama Digestion and Agni Stimulation): When ama predominates, pachana herbs facilitate detoxification and improve metabolic clearance.
“?ma-do?a-n??anam pachanam” (Charaka Samhita, Sutra Sthana 28)
Jwara Shamana (Fever Pacification)
Classical jwaraghna therapy aims to normalise dosha imbalance and reduce systemic inflammation. (Charaka Samhita, Chikitsa Sthana 3)
Rasayana (Restoration of immunity and Immunomodulation): Rasayana therapy restores tissue vitality and immunity, supporting recovery.
“Ras?yana? n?ma vayah-sth?panam” (Charaka Samhita, Chikitsa Sthana 1/8)
Integrative Ayurvedic Management
Acute Febrile Toxic Phase (Sama Sannipata avastha): Reduce fever and inflammation; digest ama; maintain hydration; and prevent further progression. Approach: Langhana (light diet, warm water), Pachana herbs and Shadangapaniya (drink made of Musta, Ushira, Parpatak, Udichya, Nagar and Chandan)
Respiratory Dominant Phase: Protect the Pranavaha srotas, reduce cough and bronchospasm, and facilitate expectoration. Approach: Vasa-based formulations, Talisadi churna and Sitopaladi churna.
Neurological Dominant Phase: Stabilise Prana and Majja, reduce neuroinflammation and Support cognitive recovery. Approach: Medhya Rasayana after initial stabilisation.
Immunocompromised Phase: Restore strength and Oja (essence of all Dhatu); prevent relapse; support rehabilitation. Approach: Rasayana therapy, Dietary modification and Mental rehabilitation.
Different herbs and their actions relevant to disease-controlling efficacy:
1. Guduchi (Tinospora cordifolia)
“Gud?c? tikta-ka??y? u??? ras?yan? jvar?pah?” (Bhavaprakasha Nighantu, Guduchyadi Varga, Verse 21)
Doshakarmata: Jwaraghna, Ama pachana, Rasayana, Tridosha shamaka.
Research Evidence: It enhances macrophage function, Modulates IL-6 and TNF-α and has Antioxidant and immunostimulant properties (Sharma et al., J Ethnopharmacol; Upadhyay et al., Int Immunopharmacol)
Clinical rationale: Supports immune resilience and fever modulation.
2. Amalaki (Phyllanthus emblica)
“?malak? sarva-do?aghni ras?yan? balya”(Bhavaprakasha Nighantu, Haritakyadi Varga, Verse 38)
Doshakarmata: Rasayana, Pittashamaka, Dhatu poshana.
Research evidence: It is a potent antioxidant, Endothelial protection and Vitamin C enriched (Krishnaveni et al., Phytother Res)
3. Musta (Cyperus rotundus)
Charaka Samhita described in Lekhaniya Mahakashaya
Doshakarmata: Pachana, Grahi, Kapha-Pitta shamaka.
Research activity: Anti-inflammatory, Antipyretic and Gastroprotective (Sivapalan, J Ethnopharmacol)
4. Kiratatikta (Swertia chirayita)
In the Charaka Samhita, it is explained in Tikta Skandha
Doshakarmata: Jwaraghna, Ama pachana.
Research evidence: Anti-inflammatory, Hepatoprotective and Antimicrobial activity. (Wang et al., Phytomedicine)
5. Vasa (Adhatoda vasica)
“V?s? ?v?sahara k?saghni raktapittahara”(Bhavaprakasha Nighantu, Guduchyadi Varga, Verse 88–89)
Doshakarmata: Kasa-shwasa hara, Kapha shamaka.
Research evidence: Bronchodilator, Expectorant and Anti-inflammatory potential (Dhuley, J Ethnopharmacol)
6. Brahmi (Bacopa monnieri)
“Brahm? medhy? ras?yan?” (Bhavaprakasha Nighantu, Guduchyadi Varga, Verse 279)
Doshakarmata: Medhya rasayana is neuroprotective.
Research evidence: Cognitive enhancement in different RCTs and Neuroprotection. (Stough et al., Psychopharmacology)
7. Shankhapushpi (Convolvulus pluricaulis)
In Bhavaprakasha Nighantu, it is mentioned in Guduchyadi Varga
Doshakarmata: Medhya, nidrajanana.
Research evidence: Neuroprotective and Anxiolytic (Sethiya, Ayu)
8. Ashwagandha (Withania somnifera)
In Bhaisajya Ratnabali, it is mentioned in Rasayan prakarana
Doshakarmata: Balya, Rasayana.
Research evidence: Stress reduction and Immunomodulation (Lopresti et al., Medicine)
Panchakarma is contraindicated in acute infection. Only mild therapies are used in recovery.
Preventive Strategies: Ayurvedic and Public Health Integration
Janapadodhwamsa Chikitsa (Population-Level Prevention): Charaka describes community-wide disease prevention under Janapadodhwamsa Chikitsa, emphasizing correction of environmental vitiation, ethical conduct, hygiene, dietary regulation, and strengthening of population immunity (Charaka Samhita, Vimana Sthana 3/6–12).
“Tatra satvavajaya? d?n?di ca janapadoddhvamsa-n??anam.” (Charaka Samhita, Vimana Sthana 3)
Classical preventive domains include:
These align with modern public health strategies, including sanitation, food safety, ventilation, vector control, and community awareness.
Dhoopana Karma (Herbal Fumigation): Ayurveda prescribes Dhoopana for environmental sterilization and reduction of microbial load, particularly in epidemic settings (Sushruta Samhita, Kalpa Sthana; Kashyapa Samhita).
“Dhoopanena bhavanti rak?a?a? krimi-n??anam”(Sushruta Samhita)
Classical drugs used include: Guggulu, Nimba, Vacha, Haridra, Sarshapa and Agaru. Modern studies demonstrate antimicrobial and air-purifying effects of fumigation herbs, supporting translational relevance.
Diet, Lifestyle, and Immunoprotection: Lightly digestible diet during outbreaks; avoidance of contaminated fruits and raw drinks or juices; Rasayana intake for immune resilience, with Adequate sleep and stress reduction. The overview of preventive strategies and their Ayurvedic correlations is presented in TABLE 6.
TABLE 6: Prevention in Ayurveda integration with Public Health
|
Ayurveda |
Modern Equivalent |
|
Janapadodhwamsa |
Epidemic surveillance |
|
Dhoopana |
Environmental disinfection |
|
Pathya Ahara |
Food safety |
|
Rasayana |
Immunoprophylaxis |
|
Satvavajaya |
Mental health |
Safety and Ethical Considerations: Ayurvedic therapy never delays emergency care and is the best preventive measure for infectious diseases, helping protect against complications. Informed consent is required; avoid unverified claims and follow national treatment protocols. Panchakarma during acute infection is prohibited. Metallic preparations (Rasa Ausadhi) without monitoring of liver and kidney function and emaciating therapies (Apakarshan) should not be given in this condition, where immunity is already compromised.
4. DISCUSSION
Nipah virus (NiV) infection represents one of the most serious emerging zoonotic threats globally due to its high case fatality rate, potential for human-to-human transmission, and lack of licensed antiviral therapy or vaccines. Recurrent outbreaks in Bangladesh, Kerala, and West Bengal highlight persistent ecological and healthcare vulnerabilities associated with bat–human interfaces, food contamination, occupational exposure, and nosocomial transmission. (Ang BSP et al, Arunkumar G et al, WHO. Nipah Virus Fact Sheet.) .The suspected outbreak in West Bengal in January 2026 further underscores the need for strengthened surveillance, early clinical suspicion, and rapid infection-control preparedness in densely populated healthcare settings. (NIV Pune Bulletin 2026, West Bengal Health Dept Report 2026.) From a biomedical perspective, Nipah virus demonstrates marked endothelial and neuronal tropism mediated by ephrin-B2 and ephrin-B3 receptors, leading to systemic vasculitis, microthrombosis, blood–brain barrier disruption, and encephalitis. (Negrete OA et al., Goh KJ et al., Tan CT et al.)
These mechanisms explain the rapid clinical deterioration from nonspecific febrile illness to coma, seizures, respiratory failure, and multi-organ dysfunction reported across outbreaks. (Wong KT et al.,Goh KJ et al.). Mortality remains high despite improved intensive care support, particularly in resource-limited settings and in patients with delayed diagnosis. (Ang BSP et al, Wong KT et al, Hsu VP et al.). Although monoclonal antibodies and antiviral candidates have demonstrated promising preclinical efficacy, none are currently approved for routine clinical use. (Mire CE et al., Broder CC et al.)
Ayurveda offers a parallel conceptual framework for epidemic infectious diseases through the doctrines of Agantuja Vyadhi, Aupasargika Roga, and Janapadodhwamsa described in classical texts. Charaka explains mass illness resulting from the vitiation of air, water, land, and seasonal factors, a concept that aligns closely with modern ecological and environmental determinants of zoonotic spillover. (Charaka Samhita, Vimana Sthana 3). Sushruta’s description of Sansargaja Roga, i.e., transmission through contact, respiration, shared bedding, clothing, and utensils, closely resembles modern droplet and fomite transmission pathways. (Sushruta Samhita, Nidana Sthana 5). These correlations demonstrate that ancient epidemiological observations possess strong translational relevance to contemporary infectious disease science.
Clinically severe Nipah infection correlates well with Sannipata Jwara, characterised by Tridoshic imbalance, rapid systemic deterioration, delirium, respiratory distress, and high fatality. (Charaka Samhita, Chikitsa Sthana 3). The Ayurvedic concept of Oja kshaya provides a theoretical model for immune exhaustion, shock, and organ failure observed in critical viral illness. Mapping modern manifestations such as fever, encephalopathy, seizures, dyspnea, and hypotension with Ayurvedic Lakshanas, including Jwara, Bhrama, Apasmara, Shwasa, and Ojakshaya, allows meaningful integrative interpretation without compromising biomedical safety standards. The probable mode of etiopathogenesis is depicted in FIGURE 2.
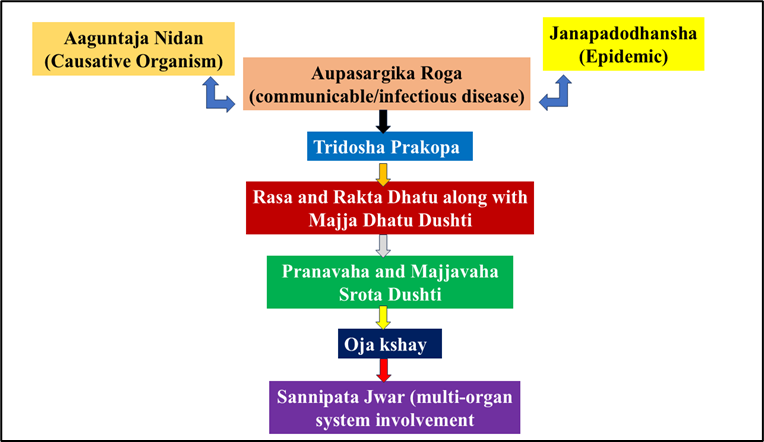
FIGURE 2: Samprapti(pathogenesis) of Nipah virus from the Ayurvedic point of view
The therapeutic role of Ayurveda in Nipah infection must be positioned strictly as adjunctive supportive care, not curative treatment. Classical principles such as Nidana parivarjana, Langhana, Pachana, Jwara Shamana, and Rasayana emphasise metabolic regulation, toxin clearance, tissue protection, and recovery enhancement. (Ashtanga Hridaya, Chikitsa Sthana 1). These principles parallel modern supportive strategies, including controlled nutrition, hydration, inflammation modulation, rehabilitation, and immune recovery. Herbal agents discussed in this review, including Guduchi, Amalaki, Musta, Kiratatikta, Vasa, Brahmi, Shankhapushpi, and Ashwagandha, demonstrate experimentally supported immunomodulatory, antioxidant, anti-inflammatory, neuroprotective, and respiratory-supportive properties. (Sharma U et al., Upadhyay AK et al., Krishnaveni M et al., Sivapalan SR, Wang P et al., Dhuley JN, Stough C et al., Sethiya NK, Lopresti AL et al.). The detailed line of management is explained in FIGURE 3.
Although none have demonstrated direct antiviral efficacy against Nipah virus in human trials, these biological activities support cautious, supportive use during the recovery and rehabilitation phases under medical supervision. The integration of classical verse citations with modern pharmacological data enhances academic value and translational credibility. Preventive strategies derived from Janapadodhwamsa Chikitsa, including environmental sanitation, dietary discipline, behavioural regulation, and Rasayana usage, closely parallel modern public health interventions such as hygiene promotion, ventilation, food safety regulation, and community education. (Charaka Samhita, Vimana Sthana 3, WHO Outbreak Preparedness Manual.) The traditional practice of Dhoopana (herbal fumigation) has demonstrated antimicrobial and air-purifying potential in experimental studies, suggesting relevance for environmental infection control in low-resource settings, although standardisation and safety validation remain essential. (Sushruta Samhita Kalpa Sthana, Experimental fumigation studies – AYUSH publications, Environmental microbiology fumigation studies).
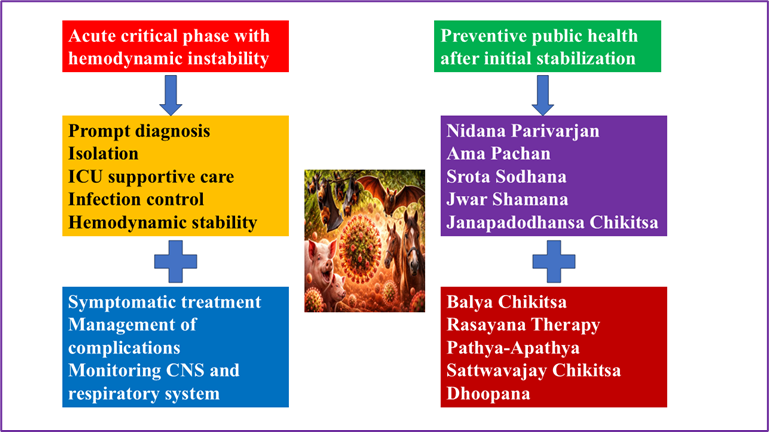
FIGURE 3: Treatment modality of Nipah virus in Ayurveda and modern system of medicine
Several limitations must be acknowledged. Clinical trials evaluating Ayurvedic interventions specifically for Nipah infection are lacking due to the sporadic nature and high biosafety risk of outbreaks. Most evidence supporting herbal interventions originates from experimental models or surrogate inflammatory conditions rather than direct viral disease trials. The various herbal and mineral preparations used in the ayurvedic treatment of infectious diseases are summarised in TABLE 7. Ethical principles require that integrative interventions must never delay isolation, intensive care, or public health response. Potential herb–drug interactions and quality-control issues require institutional oversight and pharmacovigilance (Izzo AA et al.; Williamson EM et al.).
Future research should prioritise multicentric observational studies during outbreak recovery phases, validation of standardised supportive protocols, evaluation of environmental disinfection strategies such as Dhoopana, and interdisciplinary collaboration between infectious disease specialists, public health experts, and Ayurveda researchers. (Integrative medicine research frameworks – WHO / NCCIH.) Such integrative research may enhance resilience, rehabilitation outcomes, and preparedness while maintaining scientific standards and patient safety. In summary, this review demonstrates that Ayurveda provides a coherent conceptual framework and supportive evidence that complement modern biomedical understanding of Nipah virus infection. Responsible integration may enhance recovery, preventive preparedness, and holistic care when practised within evidence-based clinical governance and public health ethics.
TABLE 7: Classical Ayurvedic formulation with its relevance regarding research activity and utility in infectious diseases
|
Formulation |
Classical Reference |
Key Ingredients |
Classical Indication |
Modern Evidence |
Type of Study |
Research study reference |
|
Sudarshan Churna |
Bhaishajya Ratnavali – Jwara Prakarana |
Kiratatikta, Musta, Guduchi, Triphala, Katuki |
Sarva Jwara, Vishama Jwara, yakrt- pleeha roga, gulma |
Antipyretic, immune-modulatory effects demonstrated inexperimental models |
Animal + in-vitro study |
Patgiri B et al, Sharma PV, et al |
|
Amritarishta |
Bhaishajya Ratnavali – Jwara |
Guduchi, Dashamoola, ativisha, trikatu |
Jwara |
Hepatoprotective immunostimulant activity |
Animal study |
Kapil A et al |
|
Mahasudarshan Kwatha |
Sharangadhara Samhita |
triphala, chirayata, kalmegh,musta, usira, parpati |
Jwar, ajirna, kasa, pandu, kamla, dourvalya |
Anti-inflammatory and antioxidant effects reported |
Experimental study |
Tripathi YB, et al. |
|
Tribhuvan Kirti Rasa |
Rasatarangini |
Vatsanabha, Trikatu, hingula, tankan, tulsi, dhatura |
Jwar, Vedanahara |
Clinical symptomatic fever reduction reported |
Observational study |
Kulkarni RR et al. |
|
Guduchi Ghana Vati |
AFI |
Guduchi extract |
Rasayani, balya, swas, kasa hara, agni deepana |
Enhanced macrophage activation and cytokine modulation |
In-vitro + human study |
Sharma U et al, Upadhyay AK et al. |
|
Sitopaladi Churna |
Bhaishajya Ratnavali – Kasa rogadhikara |
Pippali, Vanshlochan,Sitopal, pippali, ela, twak |
Swas, kasa, mandagni, jwar, parsva sula |
bronchodilator and expectorant effect demonstrated |
Clinical study |
Bhatt N, et al. |
|
Dashamoola Kwatha |
Charaka Samhita |
Laghu and Brihat Panchamoola |
Jwar, swas, kasa, parsva sula, bala- varna-agni vardhan |
Anti-inflammatory and analgesic activity |
Animal study |
Gupta MB et al. |
5. CONCLUSION
Nipah virus continues to pose a severe public health challenge due to its high mortality, epidemic potential, and absence of definitive therapy. Modern management relies on early diagnosis, isolation, infection control, and intensive supportive care. Ayurveda provides a robust conceptual framework for understanding epidemic diseases and offers supportive strategies for symptom modulation, recovery enhancement, and population-level prevention when responsibly integrated. Future collaborative research is required to validate integrative models and optimise preparedness.
6. RESEARCH GAPS AND FUTURE DIRECTIONS:
No clinical trials in Nipah. It needs integrative observational studies. And the standardization of dosage and safety.
7. DECLARATIONS
Conflict of interest: nil
Funding sources: nil
Acknowledgement: nil
Author contribution: S.S; Conceptualization and study design; literature search and data acquisition; analysis and interpretation of biomedical and Ayurvedic literature; development of integrative framework, figures, and tables; manuscript drafting and critical revision; final approval of the manuscript.
Informed consent: not applicable
REFERENCES

Subhabrata Sarkar, Nipah Virus Outbreak as an Aupasargik Roga (Infectious Disease):-Emerging Epidemiology, Clinical Spectrum and Integrative Management with Ayurvedic Insights, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4142-4159. https://doi.org/10.5281/zenodo.18776576
 10.5281/zenodo.18776576
10.5281/zenodo.18776576