
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
K. M. Kundnani College of Pharmacy.
Medical treatment is based on the traditional “one fits all” approach, but treatment can vary with patients' genetic makeup. The treatment which is adventitious for one may not be useful for others to resolve this problem the new approach invented is personalized medicine. Personalized medicine (PM) or the right medicine for the right patient has long been considered the next step and the highest safety margin to ensure better and effective patient care hence is a great approach because it focuses on the enhancement of treatment outcomes, and curing, detecting disease in less time and avoids patients suffering from adverse drug reactions. Pharmacogenetics and Pharmacogenomics are the main tools utilized in personalized medicine which detect the drug response with the help of biomarker testing. The main objectives of this review are to discuss the recent developments in personalized drugs, their roles and their challenges, and customized technologies like bio-electronic medicine and 3D printing.
Personalized medicine is not a novel or latest innovation, but it is a continuous process of research efforts made to tailor treatments as required for individual patient characteristics. Examine as much as idiosyncratic effects or adverse drug reactions link with the authorized drugs in benefits, the ‘genetic factors of a person are responsible [1]. Out of the approved drugs, 16 are associated with adverse drug reactions (ADRs) due to poor metabolism (i.e., genetic variation). The patient’s unexpected responses, such as any ADRs or mysterious idiosyncratic effects, or hypersensitivity to any drug in normal dose or the drug itself, maybe because of the patient’s non-genetic factors (phenotype) and genetic factors (genotype) [2-4]. Genetic dissimilarities in drug-metabolizing enzymes, drug transporters and drug receptors have been linked with individual inconsistency in the effectiveness and toxicity of the drug. Single nucleotide polymorphism (SNP) profiles and multigene analysis are included in clinical use for new drug development [5]. An allele is a term that is defined as a genetic variation that arises when there is an alteration in the deoxyribonucleic acid (DNA) sequence and it could be SNP which may or may not create changes in protein regulation [6]. There is a 1% or higher chance of occurrence of SNP mutation and in human DNA 90% of the variation is due to SNPs which can take place in every 100–300 base pair.
Few mutations affect the protein mechanism which leads to affecting the metabolic pathway. These affect the individual's capability to metabolize some drugs [7].
Precision Medicine is another name for personalized medicine and is defined as “the right patient treated with the right medicine with the correct dose at the right time [8]. The aim of personalized medicine is to give the correct treatments to the patients at the right time by studying their genetics. Testing the genetic variation of patients helps to treat with effective medication and avoid harmful adverse effects because different genetic makeup in the same family members gives different responses to the same drug to treat inherited diseases for example Cystic fibrosis [9]. Institute for Systems Biology and Dr. Hood, personalized medicine is included in specified P4 due to its four elements Personalized, Predictive, Preventive, and Participatory. The main goals of personalized medicine are:
a.To recognize the personalized treatment for each patient by using genetic information.
b.To reduce side effects by identification of biomarkers to perform a correct diagnosis for targeted therapy.
c.To evaluate therapy responses and regulate long-term outcomes by considering patient safety and identifying disease at its early stage which reduces disease detection and treatment time and also reduces treatment cost, considering disease-related and patient-related elements to perform accurate diagnosis and its etiology in an individual patient.
d.To initiate the prognosis by using prognostic scores and by considering further individual patient-related variables to increase benefits from given treatment by observing strategies in an individual patient.
Personalized medicine is getting eye-catching because of its advantages like, it is cost-effective due to early detection of disease to prevent disease and reduce adverse effects and improve patient compliance, it selects targeted therapy by improving the ability to know the mechanism of action of the drug by studying genetic makeup, the lower number of patients to be tested in clinical trials and drug development cost also reduced, it avoids trial-error complex and thus targeted drugs prescribed by the physician. Some marketed personalized medicines are mentioned in table 1 with their mechanism, trade name, generic name and targeted site of action. Although PM is effective but also has limitations are costly biomarker testing, time-consuming in case of collection of the data of an individual patient, the responsibility of collecting huge complex data and storing individual genetic information (Ethical responsibility).
Table 1: Marketed personalized drugs.
|
Class of drug |
Trade name |
Generic name of the drug |
Target site |
Approved year |
Reference |
|
Tyrosine kinase inhibitor |
Tarceva |
erlotinib |
Epidermal growth factor receptor |
14 May 2013 |
10 |
|
Iressa |
gefitinib |
13 July2015 |
11 |
||
|
Tagrisso |
osimertinib |
Nov 2015 |
12 |
||
|
Monoclonal Antibody |
Portrazza |
necitumumab |
Epidermal growth factor receptor |
24 November 2015 |
13 |
|
A monoclonal antibody, Antineoplastic |
Keytruda |
pembrolizumab |
Programmed cell death-1 (PD-1) receptor |
23 May 2017 |
14 |
|
Cyclin-dependent kinases (CDK)4/6inhibitors |
Ibrance |
palbociclib |
Human epidermal growth factor receptor 2- negative (HER2-) |
2015 |
15 |
The main aspects of personalized medicine
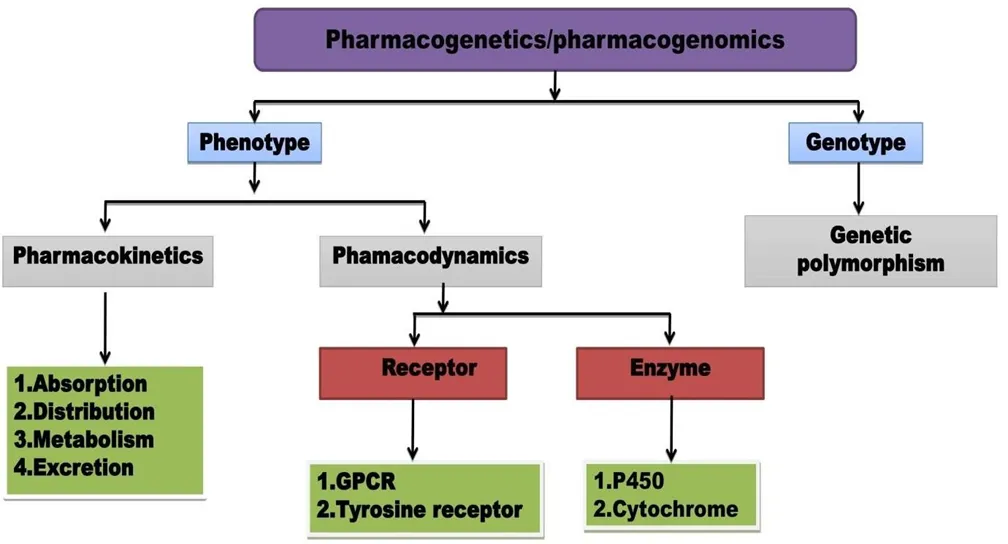
Figure 1: Classification of Pharmacogenetics/Pharmacogenomics
Pharmacogenetics
Pharmacogenetics is defined as a study of a single gene. Till 1957 physicians were not able to recognize the variation in the responses to the drug. However, after 2 years pharmacogenetics term was introduced and this is based on the study of genes of individual patients. The term was first used in the detection of drug response to phenotypic variations, it is a term used for some drugs by the end of the 1950s and heredity is the reason for the variation in drug response. This study gives the direction of how genetic variation affects the drug metabolism pathways, or how the individuals respond to it based on their genetics [16]. Pharmacogenetics
in clinical trials for the development of new drugs are divided into four phases given in table 2 [17,18].
Table 2: Phases of a clinical trial for drug development.
|
Clinical trials |
Pharmacogenetics |
Reference |
|
Phase 1 |
Identification of patients and dose-ranging with their known genotypes. |
19 |
|
Phase 2 |
Refinement of the pharmacogenetics determinants. Phase II studies are divided into Phase IIA (How much quantity will be required for response)and Phase IIB (How the drug is doing in the body at the prescribed dose) |
20 |
|
Phase 3 (Pivotal trial) |
Reduction of studies or phase 1 and 2 re-evaluations confirm the efficacy and identify the incidence of common adverse reactions |
21 |
|
Phase 4 |
The Drug is licensed it is post-marketing surveillance (PMS) |
22 |
Pharmacogenomics
The term pharmacogenomics is the advanced term of pharmacogenetics that was started for use in 1997. The study of the whole human genome is called Pharmacogenomics [23].
Pharmacogenomics is defined as the study of how genes influence the response of an individual to drugs. Pharmacogenomics is a relatively novel method that combines pharmacology (study of drug) and genomics (Study of Genes and their functions) thus the right drug is prescribed for effective treatment [24,25] .
Biomarker testing
A biomarker is defined as according to the National Cancer Institute, “it is a biological molecule which is present in tissues, blood or any other body fluid which indicate regular or irregular processes into the body. Biomarkers detection via biofluid testing (blood, plasma, serum, urine) is a measurement of lung function, blood pressure or electroencephalography and molecular (DNA, protein, metabolite) measures [26]. The different detection techniques used to detect the biomarkers in in different type of cancers are shown in table 3 for example in women's breast tumors there is a 30% chance of overexpression of the HER2/neu gene receptor on the cell membrane due to amplification of the HER2/neu gene. Trastuzumab drug is a choice of treatment for women with HER-2-POSITIVE TUMOR breast cancer [27].
Table 3: Type of cancer and their biomarker with a detection technique
|
Cancer type |
Biomarkers |
Detection technique |
Reference |
|
Breast cancer |
Human Epidermal Growth Factor Receptor (HER2/neu) |
Quantum dots (QD) and optofluidic ring resonator sensor |
28 |
|
Cellular myelocytomatosis oncogene (C-MYC) |
Fluorescence in Situ hybridization (FISH ) |
||
|
Cancer antigen15-3 (CA 153),Carcinoembryonic antigen (CEA), HER2/neu |
Immunohistochemistry |
||
|
Breast cancer susceptibility genes 1 and 2 (BRCA1, BRCA2) |
Western blotting and Protein truncation test (PTT) |
||
|
Carcinoembryonic antigen (CEA) |
Quantum dots (QD) and Gold nanoparticle-based techniques |
||
|
Prostate cancer |
Prostate-specific antigen(PSA) |
Quantum dots (QD) and Gold nanoparticle-based techniques |
29 |
|
Prostatic acid phosphatase (PAP), urinary calgranulin B/MRP-14 |
Matrix-assisted laser desorption ionization-time of flight mass spectrometry ( MALDI-TOF-MS) |
||
|
Lymphoma |
Lactate dehydrogenase (LDH), β2-microglobulin |
Immunohistochemistry |
30 |
|
Ovarian cancer |
Cancer antigen-125 (CA-125) |
Surface-enhanced laser desorption /ionization-time-of-flight mass spectrometry (SELDI-TOF-MS) |
31 |
|
Pancreatic cancer |
Carbohydrate antigen19-9 (CA19-9),carbohydrate antigen 72-4(CA 72-4), MUC1 |
Immunohistochemistry (IHC) |
32 |
|
Lung cancer |
CYFRA 21-1 |
Immunohistochemistry (IHC) |
33 |
The selection of drugs is based on the patient’s phenotypic and genotypic characteristics are mentioned in table 4
Table 4: Example of drug with their gene, clinical uses and phenotype
|
Drugs |
Gene |
Clinical uses |
Phenotype |
|
Mercaptopurine |
Thaiopurine S- |
Pediatric acute lymphoblastic leukemia |
Myelosuppression |
|
Methyltransferace (TPMT) |
|||
|
Trastuzumab |
Human epidermal growth factor receptor (HER2/neu)) |
Breast Cancer |
Resistance to therapy |
|
Phenyton Carbamazepine |
CYP2C8, |
Epileptic seizers |
Reduced dose required |
|
CYP2C19 |
|||
|
Warfarin |
Vitamin K epoxide reductase complex subunit 1 (VKORC1) |
Thrombosis |
Reduced dose required |
|
Codeine |
CYP2D6 |
Analgesic |
Decrease in opioid potency |
|
Tamoxifen |
CYP2D6 |
Homone receptor positive breast cancer |
Tamoxifen metabolism progression -free and overall survival |
|
Ivacaftor |
Cystic fibrosis transmembrane |
Cystic fibrosis (CF) |
Open the gate for longer periods in case of mutation |
Thiopurines
Thiopurines (azathioprine, mercaptopurine) are commonly used to treat childhood acute lymphoblastic leukemia. Thiopurine S-methyltransferase (TPMT) causes the inactivation of thiopurines. Polymorphism of the TPMT gene depends on the TPMT enzyme activity level. TPMT*2, TPMT*3A, and TPMT*3C are common variant alleles of the TPMT gene present in 80-90% of individuals causing too much drug converts to 6-thioguanine nucleotides (6-TGNs) and reduce (80-95%) TPMT activity level. Because of low TPMT levels, a patient’s prescribed (5 – 10%) of the standard dose to avoid toxicity, and if the TPMT level is high then higher than standard doses of a thiopurine drug are prescribed [34]. In a case study, a 7-year-old Latrice was diagnosed with leukemia, which is a type of bone marrow and blood cell cancer. purinethol is a drug used for chemotherapy for over 30 years but it has severe side effects. TPMT (thiopurine S-methyltransferase) enzyme is responsible for purinethol drug metabolism. 80%children are capable to metabolized purinethol but 11% have TPMT variations and thus suffer from toxic effects. The doctor tested his DNA, and he found that there is a partial TPMT variation hence purinethol level should be reduced.
Oral anticoagulants
Blood clotting is prevented by S-warfarin antagonized vitamin K. CYP2C9 is the enzyme that causes the metabolism of S-warfarin. If there are any changes in a drug-metabolizing enzyme (CYP2C9) and vitamin K-activated enzyme, vitamin K epoxide reductase complex subunit 1 (VKORC1) then the warfarin drug administration is difficult. The sensitivity of warfarin is affected by the occurrence of CYP2C9 polymorphisms (CYP2C9*2 and *3 variants) causing S-warfarin to become more active which leads to an increase in the plasma level of warfarin [35]. When a conventional dose is taken in presence of these polymorphs’ patients experience bleeding events due to over-anticoagulation thus reduction of the dose is required. Warfarin inhibits the enzyme vitamin K epoxide reductase (VKOR) leading to coagulation factors hemorrhagic (II, VII, IX, X) and antithrombotic (protein C and protein S) formation prevented [36].
Codeine
Codeine is a prodrug use for analgesic effect. For analgesic activity codeine should be metabolized into morphine after administration [37]. The copy of the Cytochrome P450 CYP2D6 gene is missing in 7% of Caucasians so the metabolism of codeine into morphine is not possible due to the absence of the metabolizing enzyme cytochrome p450 CYP2D6[38]. Thus, codeine administration is not effective in such type of situation.
Phenytoin
Antiepileptic drugs such as phenytoin have a narrow therapeutic index. CYP2C9 metabolized phenytoin in the liver and CYP2C19 metabolized Phenytoin to a smaller extent. Then the drug is transferred to the blood-brain barrier and binds to its therapeutic target. A recent case report found that patients have variants CYP2C9*3 or CYP2C9*2 and when a patient takes a conventional dose, he/she experiences severe phenytoin toxicity [39].
Ivacaftor
In cystic fibrosis (CF) there are severe variations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene exhibiting extremely specific indications. To regulate the transport of salts in and out of cells a 'gate-like' arrangement in the CFTR gene's programmed protein can open and close. If the CFTR gene is dysfunctional the gate is shut, which leads to the building up of mucus and other waste in the lungs. Different types of dysfunctions are caused by mutations in the CFTR gene. Because of other mutations, the gate mechanism gets ineffective. Certain mutation causes get to shut, Ivacaftor is used in a small number of CF patients having a mutation that causes gating problems by the opening gate for a longer period [40]. For the development of effective personalized medicine, the approach can be the use of medical devices to improve patient drug response outcomes.
Customized technologies
Bioelectronic medicine
Rheumatoid arthritis (RA) is an autoimmune inflammatory disorder caused by painful swelling in joints which leads to damage to joints and loss of mobility. Tumor Necrosis Factor (TNF), is a cytokine responsible for rheumatoid arthritis [41,42].
Medications for rheumatoid arthritis are glucocorticoids, methotrexate, and monoclonal antibodies. The vagus nerve is stimulated by a bioelectronic device then the signals go through the vagus nerve into the spleen and splenic nerve triggering depletion in the activation of T cells and macrophages and decreasing the presence of cytokines and tumor necrosis factor (TNF) thus joint pain and inflammation in rheumatoid arthritis patient’s get reduced [43].
3Dprinting
3D printing is defined as formulating 3D object medications for each patient with approved excipients by a coating of materials like metal, liquid, and powder in layers [44,45]. A substrate is layered by the material for making a 3D object with aided programming and drafting technology. The 3D procedure is also stated to as additive manufacturing (AM), and rapid prototyping (RP). Advantages of 3D printing include [46,47]. being an important tool for the development of drugs that reduce time as well as costs, less waste produced, are not complex, have fewer steps than the conventional making tablet process, are accurate, and production of the drug in small quantities. Recently different types of drug delivery systems have been developed using 3D printing for example in transdermal drug delivery to develop microneedles, oral control released systems, sustained release, polypills, implants and rapidly dissolving tablets [48].
Table 5: Roles and challenges of personalized medicine [49-52].
|
Role of personalized medicine |
Challenges of personalized medicine |
|
In the new Drug Discovery and Development: developing more effective drug therapies and evaluating how the cell will respond to the new drug. |
Disease classification: In Precision medicine classification of diseases is based on an old pattern. |
|
Lack of awareness: Personalized medicine is a new field for people so they are not aware of genetic makeup and biomarker testing. |
Legal Challenges: The information stored in the biobank needs high security to protect the data. |
|
In Clinical trial Research studies: Select individuals who participate in a clinical trial based on their genetic susceptibility to react to some type of treatment which results in speedy, inexpensive, productive, and safe clinical trial studies. |
Acceptance of new diagnostic techniques: It is a new term that makes it difficult to replace the older technique which is known to patients and also challenging in overloading the information. |
|
In targeted drug therapy: Personalized Medicine provides more targeted drug therapy. |
Large population size: Common diseases like colds, malaria, and diarrhea, cancer have a large number of rare genes. |
|
In Health Care: The disease is diagnosed at an early stage thus the patient will not suffer from the toxic effects, No switching of drugs. |
Factors affecting drug response: Factors such as diet and lifestyle can influence genetic response to drugs. |
CONCLUSION
In the traditional method, one treatment fits all approach causes mixed results of drug response because of not considering that each patient is unique and different genetic makeup than the other. Today’s medicine is not for individual patients according to their genetic variation so to resolve this problem a personalized medicine approach is used for diagnosis and to treat the disease with an accurate dose of the right medicine. This approach is cost-effective and detects disease at an early stage which reduces the time of treatment and also it avoids switching drugs thus patients will not suffer from adverse effects. Although this approach has some challenges biomarker testing is expensive, people are not aware of it, there is a lack of genetic knowledge and detecting tools this field getting popularity in growing countries because of its uniqueness and FDA-approved so many personalized drugs based on their novelty. In the future, if we strategies challenges regarding personalized medicine this field gain much more importance in improving health care through a targeted therapy approach.
REFERENCES


Madhuri Dhure, Prerana Bambale, Rajratan Thorat, Personalized Medicine: A Novel Approach in Healthcare, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 3255-3265, https://doi.org/10.5281/zenodo.21393687
 10.5281/zenodo.21393687
10.5281/zenodo.21393687