
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy Practice, KLR College Of Pharmacy, Paloncha, Bhadradri Kothagudem, Telangana, India.
Background: Cardiovascular and endocrine complications during pregnancy remain major contributors to maternal and neonatal morbidity worldwide. Among these conditions, hypertensive disorders of pregnancy and gestational diabetes mellitus represent significant clinical challenges due to their potential impact on maternal cardiovascular health and foetal development. Early identification and appropriate management of these complications are essential to improve pregnancy outcomes. Objective: The present study aimed to evaluate the prevalence of cardiac and endocrine complications among pregnant women and to investigate the association between gestational diabetes mellitus and hypertensive disorders of pregnancy, along with their effects on maternal and neonatal outcomes. Methods: A hospital-based observational study was conducted among 303 pregnant women attending antenatal care at a tertiary care hospital. Demographic characteristics, clinical parameters, and pregnancy-related complications were systematically recorded. The prevalence of cardiovascular complications, endocrine disorders, and obstetric outcomes were analyzed using descriptive statistics. Associations between gestational diabetes mellitus and hypertensive disorders were assessed using chi-square analysis, while multivariable logistic regression was performed to identify predictors of hypertensive complications. Results: Hypertensive disorders were the most common cardiovascular complication, affecting 41.9% of the study population, with gestational hypertension being the predominant subtype. Among endocrine disorders, thyroid dysfunction (41.9%) and gestational diabetes mellitus (32.3%) were the most frequently observed conditions. Hypertensive pregnancies demonstrated a higher incidence of preterm birth (21.5%) compared with normotensive pregnancies. Significant associations were observed between gestational diabetes and adverse outcomes including preterm birth (p = 0.030) and foetal macrosomia (p = 0.043). Furthermore, logistic regression analysis revealed that gestational diabetes mellitus significantly increased the risk of hypertensive disorders (OR = 3.45; 95% CI: 1.62–7.34; p = 0.001). Conclusion: The study highlights the substantial burden of hypertensive and endocrine complications during pregnancy, particularly gestational diabetes and thyroid disorders. The strong association between gestational diabetes mellitus and hypertensive disorders underscores the importance of early metabolic screening and integrated antenatal management strategies. Multidisciplinary care, including optimized pharmacotherapy and continuous monitoring, may play a critical role in improving maternal and neonatal outcomes.
Pregnancy is a complex physiological state characterized by significant anatomical, cardiovascular, metabolic, and endocrine adaptations that support foetal development and maternal well-being. These physiological changes include increased cardiac output, expanded plasma volume, and alterations in hormonal regulation that influence glucose metabolism and thyroid function. Although such changes are essential for maintaining pregnancy, they may unmask previously undiagnosed conditions or exacerbate pre-existing disorders, particularly those affecting the cardiovascular and endocrine systems [1].
Cardiovascular disorders are increasingly recognized as a leading indirect cause of maternal morbidity and mortality worldwide. Pregnancy imposes substantial hemodynamic stress on the cardiovascular system, including a 30–50% increase in cardiac output and blood volume, which can precipitate complications such as hypertensive disorders, arrhythmias, and peripartum cardiomyopathy in susceptible women. These conditions contribute significantly to adverse maternal outcomes, including heart failure, stroke, and increased hospitalization rates during pregnancy [2]. Hypertensive disorders of pregnancy, including gestational hypertension and preeclampsia, remain among the most common cardiovascular complications and are strongly associated with maternal organ dysfunction and adverse foetal outcomes such as intrauterine growth restriction and preterm birth [3].
Endocrine disorders represent another major category of medical complications during pregnancy. Gestational diabetes mellitus (GDM) is one of the most common endocrine disorders and is defined as glucose intolerance first recognized during pregnancy. The global prevalence of GDM varies widely, ranging from approximately 1% to 28% depending on population characteristics, screening criteria, and ethnic variations [4]. In South Asian populations, the burden of GDM is particularly high due to genetic susceptibility, lifestyle factors, and increasing maternal age. Uncontrolled gestational diabetes is associated with significant maternal and neonatal complications, including macrosomia, neonatal hypoglycemia, cesarean delivery, and long-term metabolic disorders in both mother and child [5].
Thyroid dysfunction is another frequently encountered endocrine disturbance during pregnancy. Epidemiological studies indicate that thyroid disorders affect a considerable proportion of pregnant women, with overt hypothyroidism occurring in approximately 2–3% of pregnancies and subclinical hypothyroidism occurring in up to 15% depending on diagnostic criteria [6]. In India, recent hospital-based studies estimate that nearly 10–13% of pregnant women experience thyroid dysfunction during gestation, highlighting the substantial burden of endocrine abnormalities in this population [7]. Untreated thyroid dysfunction has been associated with adverse maternal and foetal outcomes, including preeclampsia, miscarriage, preterm delivery, and impaired foetal neurodevelopment [8].
The interaction between cardiovascular and endocrine disorders during pregnancy further complicates maternal health outcomes. For instance, endocrine abnormalities such as thyroid dysfunction and gestational diabetes have been shown to increase the risk of cardiovascular complications during pregnancy through mechanisms involving insulin resistance, systemic inflammation, and endothelial dysfunction. Emerging evidence suggests that women with gestational diabetes are at increased risk of thyroid abnormalities and long-term cardiovascular disease, emphasizing the importance of integrated screening and management strategies [9].
Despite advancements in maternal healthcare and antenatal screening programs, the prevalence of pregnancy-related medical complications remains substantial in many low- and middle-income countries. In India, although institutional deliveries and antenatal care coverage have improved significantly, high-risk pregnancies associated with metabolic and cardiovascular disorders continue to pose serious challenges to maternal and neonatal health outcomes. Early identification of these conditions through systematic screening and multidisciplinary management is therefore critical for reducing maternal morbidity and improving perinatal outcomes [10].
Hospital-based observational studies play an important role in understanding the epidemiological patterns and clinical characteristics of pregnancy-related medical disorders in specific populations. Such studies provide valuable insights into disease prevalence, associated risk factors, and clinical outcomes, which are essential for developing targeted prevention strategies and optimizing maternal healthcare services. Therefore, the present study was undertaken to evaluate the prevalence and clinical profile of cardiac and endocrine complications among pregnant women attending a tertiary care hospital in South India, with the aim of contributing to improved clinical management and maternal health outcomes.
MATERIALS AND METHODS
MATERIALS
The present study utilized a range of clinical, laboratory, and diagnostic resources to evaluate cardiac and endocrine complications among pregnant women. Standardized clinical documentation tools and validated diagnostic investigations were used to ensure accurate data collection and reliable assessment of maternal and foetal outcomes.
Study Setting
The study was conducted at Singareni Collieries Company Limited (SCCL) Main Hospital, Kothagudem, a tertiary care referral hospital equipped with specialized departments including obstetrics and gynecology, cardiology, endocrinology, neonatology, and clinical laboratory services. The hospital caters to a diverse population from both rural and semi-urban areas, providing comprehensive antenatal care and high-risk pregnancy management.
Study Population
The study population consisted of pregnant women attending the antenatal clinic (ANC) and obstetric inpatient services of SCCL Main Hospital during the study period. Women diagnosed with or suspected to have cardiovascular or endocrine complications during pregnancy were considered eligible for evaluation.
Clinical Materials and Diagnostic Resources
The following materials and diagnostic tools were used during the study:
Clinical Assessment Tools
Laboratory Investigations
Laboratory investigations were conducted using standard hospital laboratory facilities and included:
Cardiac Diagnostic Investigations
Obstetric Imaging
METHODS
Study Design
This investigation was conducted as a hospital-based prospective observational study. The prospective design enabled continuous monitoring of pregnant women from antenatal enrollment through subsequent follow-up visits, allowing detailed assessment of the development and progression of cardiac and endocrine complications during pregnancy.
Study Duration
The study was carried out over a six-month period, which included patient recruitment, clinical monitoring, data compilation, statistical analysis, and interpretation of results.
Participant Recruitment and Sampling Technique
A consecutive sampling method was used for patient recruitment. All pregnant women attending the antenatal clinic during the study period who satisfied the eligibility criteria were enrolled until the required sample size was achieved.
A minimum of 200 participants were included in the study. The sample size was determined based on the average antenatal clinic attendance at the study hospital and the expected incidence of cardiac and endocrine complications among pregnant women.
Inclusion Criteria
Participants were included in the study if they met the following criteria:
Exclusion Criteria
Participants were excluded from the study under the following conditions:
Data Collection Procedures
Data were collected using standardized case record forms designed for the study. Information obtained included demographic details, obstetric history, clinical findings, laboratory results, and maternal and foetal outcomes.
Clinical Evaluation
All participants underwent comprehensive clinical examination that included:
Laboratory Assessment
Laboratory investigations were conducted according to standard antenatal screening protocols. Thyroid function tests were performed to detect hypo- or hyperthyroidism. Oral glucose tolerance testing and HbA1c measurement were used to identify gestational diabetes mellitus. Routine antenatal laboratory investigations were also performed to evaluate general maternal health status.
Diagnostic Imaging
Electrocardiography and echocardiography were performed when clinically indicated to identify cardiac abnormalities. Doppler ultrasonography was used to assess foetal growth, placental circulation, and amniotic fluid volume.
Statistical Analysis
Collected data were entered into a computerized database and analyzed using appropriate statistical software.
Descriptive Statistics
Descriptive statistical methods were used to summarize demographic and clinical characteristics. Continuous variables were expressed as mean ± standard deviation, while categorical variables were presented as frequencies and percentages.
Inferential Statistics
Associations between maternal risk factors and pregnancy outcomes were analyzed using:
A p-value less than 0.05 was considered statistically significant.
Multivariate Analysis
Multivariate logistic regression analysis was performed to identify independent predictors of cardiac and endocrine complications during pregnancy. Adjusted odds ratios with 95% confidence intervals were calculated for relevant variables including maternal age, body mass index, parity, and comorbid conditions.
Ethical Considerations
The research protocol was reviewed and approved by the Institutional Ethics Committee of SCCL Main Hospital, Kothagudem. All study procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Written informed consent was obtained from all participants after explaining the objectives and procedures of the study. Confidentiality of patient information was maintained throughout the study by anonymizing personal identifiers and restricting access to authorized research personnel only.
Participation in the study was voluntary, and participants were informed of their right to withdraw at any stage without affecting their medical care.
RESULTS AND DISCUSSION
Overview of Study Findings
This study evaluated the prevalence and clinical characteristics of cardiac and endocrine complications among pregnant women receiving antenatal care at a tertiary care hospital in South India. A total of 303 pregnant women were enrolled and systematically evaluated for demographic characteristics, maternal risk factors, clinical manifestations, and maternal–foetal outcomes associated with cardiovascular and endocrine disorders.
The results highlight the significant burden of hypertensive disorders, thyroid dysfunction, and gestational diabetes mellitus among the study population. These complications represent major contributors to maternal morbidity and adverse neonatal outcomes, emphasizing the importance of early screening and multidisciplinary clinical management during pregnancy.
Recent epidemiological studies have similarly reported an increasing prevalence of cardiometabolic disorders in pregnancy, particularly in low- and middle-income countries where antenatal screening programs are still evolving [11]. Such complications can significantly affect placental function, maternal cardiovascular adaptation, and foetal growth, thereby increasing the risk of preterm delivery and neonatal complications [12].
Demographic and Clinical Characteristics of the Study Population
As shown in Table 1, the study included 303 pregnant women whose demographic and clinical characteristics were analyzed. The age distribution indicated that the majority of participants were in the 26–35 years age group (204 participants; 67.33%), followed by 18–25 years (83 participants; 27.39%), while only 16 participants (5.28%) belonged to the 36–45 years age category. This distribution demonstrates that most pregnancies occurred during the typical reproductive age period.
Regarding body mass index (BMI), the findings presented in Table 1 indicate that 296 participants (97.69%) had normal BMI, whereas 4 participants (1.32%) were overweight and 3 participants (0.99%) were obese. The predominance of normal BMI suggests that the majority of women maintained appropriate weight status during pregnancy.
With respect to parity, Table 1 shows that primiparous women represented the largest proportion of the study population (160 participants; 52.81%), followed by nulliparous women (104 participants; 34.32%) and multiparous women (37 participants; 12.21%). This indicates that a substantial proportion of the study participants were experiencing pregnancy for the first time.
Statistical comparison of categorical variables demonstrated a significant predominance of participants in the 26–35 year age group compared with other age categories (p < 0.05). Similarly, the proportion of women with normal BMI was significantly higher than overweight and obese groups (p < 0.05). The distribution of parity also revealed a statistically significant predominance of primiparous women compared with multiparous participants (p < 0.05). These findings suggest that the study cohort primarily consisted of women within the optimal reproductive age range with normal body weight and early parity status.
The demographic characteristics summarized in Table 1 provide important insights into the maternal profile of the study population. The predominance of women within the 26–35 year age group reflects the typical reproductive age distribution observed in hospital-based obstetric studies. Although this age range is generally considered optimal for pregnancy, evidence from epidemiological studies indicates that advancing maternal age within this group may increase susceptibility to metabolic disorders such as gestational diabetes mellitus and hypertensive disorders of pregnancy due to progressive insulin resistance and endothelial dysfunction [13].
The high proportion of participants with normal BMI, as reported in Table 1, suggests that the majority of women maintained a healthy anthropometric profile during pregnancy. Maternal overweight and obesity are well-established risk factors for pregnancy complications including gestational diabetes, preeclampsia, cesarean delivery, and neonatal macrosomia. Excess maternal adiposity can also influence drug pharmacokinetics by altering drug distribution and metabolic clearance, which may impact pharmacotherapeutic management during pregnancy.
Parity distribution presented in Table 1 revealed that primiparous women constituted more than half of the study population. Primigravidity has been widely reported as a significant risk factor for hypertensive disorders of pregnancy, particularly preeclampsia. The pathophysiological mechanisms are believed to involve inadequate maternal immunological tolerance to foetal antigens and impaired placental vascular remodeling, which may lead to endothelial dysfunction and abnormal placental perfusion [14].
From a clinical pharmacy perspective, these demographic variables are important for identifying women at increased risk for pregnancy-related complications and for optimizing medication management during antenatal care. Clinical pharmacists can contribute to improved maternal health outcomes through pharmacotherapy monitoring, medication safety evaluation, and patient education aimed at promoting rational drug use and adherence to treatment during pregnancy.
Table 1: Demographic And Clinical Characteristics Of Study Participants (N = 303)
|
Parameter |
Frequency (n) |
Percentage (%) |
|
Age 18–25 years |
83 |
27.39 |
|
Age 26–35 years |
204 |
67.33 |
|
Age 36–45 years |
16 |
5.28 |
|
Normal BMI |
296 |
97.69 |
|
Overweight |
4 |
1.32 |
|
Obese |
3 |
0.99 |
|
Primiparous |
160 |
52.81 |
|
Nulliparous |
104 |
34.32 |
|
Multiparous |
37 |
12.21 |
Prevalence of Cardiac Complications in the Study Population
The prevalence of cardiovascular complications observed among the study participants is summarized in Table 2. Among the 303 pregnant women included in the study, hypertensive disorders represented the most common cardiac complication, affecting 127 participants (41.91%). In contrast, arrhythmias were identified in 19 women (6.27%), while heart failure was reported in only 2 cases (0.66%). No cases of peripartum cardiomyopathy or thromboembolic disorders were recorded during the study period.
These findings indicate that hypertensive disorders constitute the dominant cardiovascular condition complicating pregnancy in the studied population. The distribution of cardiac disorders is further illustrated in Figure 1, where hypertensive disorders represent the largest proportion of cardiovascular complications compared with other cardiac conditions.
Descriptive statistical analysis demonstrated that hypertensive disorders accounted for the highest proportion of cardiovascular complications (41.91%), significantly exceeding the prevalence of other cardiac conditions observed in the study population. Chi-square comparison of the categorical variables revealed that the occurrence of hypertensive disorders was significantly higher than arrhythmias and heart failure (p < 0.05). These findings suggest a clear predominance of hypertensive disorders as the major cardiovascular complication during pregnancy within this cohort.
Cardiovascular complications remain a major contributor to maternal morbidity and mortality during pregnancy. The present study demonstrated that hypertensive disorders were the most prevalent cardiac complication, affecting nearly two-fifths of the study population. This observation is consistent with epidemiological reports indicating that hypertensive disorders of pregnancy, including gestational hypertension and preeclampsia, represent one of the leading causes of adverse maternal outcomes worldwide.
The high prevalence of hypertensive disorders observed in this study may be attributed to complex pathophysiological mechanisms associated with abnormal placental development and maternal vascular maladaptation. Impaired trophoblastic invasion of uterine spiral arteries leads to inadequate placental perfusion, which triggers systemic endothelial dysfunction, oxidative stress, and inflammatory responses. These changes increase maternal vascular resistance and contribute to the development of hypertension and related cardiovascular complications during pregnancy [15].
Although arrhythmias were observed in a smaller proportion of participants (6.27%), pregnancy is known to predispose women to rhythm disturbances due to physiological cardiovascular adaptations, including increased blood volume, elevated cardiac output, and hormonal influences on myocardial excitability. Most pregnancy-associated arrhythmias are benign; however, careful monitoring is necessary because persistent arrhythmias may compromise maternal hemodynamic stability and foetal oxygenation.
The very low occurrence of heart failure (0.66%) and the absence of peripartum cardiomyopathy and thromboembolic disorders in the present study may reflect the relatively young age distribution and generally favourable baseline health status of the study population. Nevertheless, these conditions remain clinically significant in obstetric practice due to their potential for severe maternal morbidity.
From a clinical pharmacy perspective, early identification and appropriate pharmacotherapeutic management of cardiovascular complications during pregnancy are essential to reduce maternal and foetal risks. Clinical pharmacists play an important role in optimizing antihypertensive therapy, evaluating drug safety profiles during pregnancy, monitoring potential drug-related adverse effects, and supporting multidisciplinary antenatal care. Evidence-based pharmacological interventions, combined with regular maternal monitoring, can significantly improve clinical outcomes in pregnant women with cardiovascular disorders.
Overall, the findings of this study emphasize the predominance of hypertensive disorders as the major cardiovascular complication during pregnancy, highlighting the importance of early screening, risk assessment, and multidisciplinary management strategies to prevent adverse maternal and foetal outcomes.
Table 2: Prevalence of cardiac complications among pregnant women included in the study population (N = 303).
|
Cardiac Disorder |
Number of Cases |
Percentage (%) |
|
Hypertensive Disorders |
127 |
41.91 |
|
Arrhythmias |
19 |
6.27 |
|
Heart Failure |
2 |
0.66 |
|
Peripartum Cardiomyopathy |
0 |
0 |
|
Thromboembolic Disorders |
0 |
0 |
Hypertensive Disorders in Pregnancy
The incidence and distribution of hypertensive disorders identified among the study participants are presented in Table 3. The analysis demonstrated that gestational hypertension was the most frequently observed condition (125 cases), followed by preeclampsia (58 cases) and eclampsia (8 cases). This distribution indicates that mild to moderate hypertensive conditions occurred more commonly than severe complications within the study population. The predominance of gestational hypertension is consistent with epidemiological patterns reported in obstetric surveillance studies, where gestational hypertension typically represents the earliest and most prevalent manifestation of hypertensive disorders during pregnancy [16].
The variation in blood pressure levels among the different hypertensive disorders is illustrated in Figure 2. The graphical representation demonstrates a progressive increase in both systolic and diastolic blood pressure values across the clinical spectrum, beginning with gestational hypertension and advancing toward preeclampsia and eclampsia. Women diagnosed with eclampsia exhibited the highest blood pressure measurements, reflecting severe vascular dysfunction and advanced disease progression. These findings align with established clinical observations that hypertensive disorders represent a continuum of disease severity characterized by increasing hemodynamic instability and systemic endothelial injury [16].
Comparative analysis of blood pressure measurements across the hypertensive categories revealed a gradual escalation in mean systolic and diastolic blood pressure from gestational hypertension to eclampsia, suggesting progressive cardiovascular strain associated with worsening disease severity. The observed differences between the hypertensive disorder categories were statistically significant (p < 0.05), indicating that blood pressure levels increased systematically with the severity of the condition. Elevated blood pressure during pregnancy is primarily driven by abnormal placental implantation and impaired remodelling of uterine spiral arteries, which results in placental hypoperfusion, oxidative stress, and systemic endothelial dysfunction. These pathophysiological mechanisms ultimately contribute to increased vascular resistance and widespread maternal organ involvement.
Hypertensive disorders of pregnancy represent a major global health concern and remain among the leading causes of maternal morbidity and mortality worldwide. Clinical evidence suggests that uncontrolled hypertension during pregnancy may lead to severe maternal complications, including placental abruption, renal impairment, hepatic dysfunction, cerebrovascular accidents, and progression to eclampsia. In addition to maternal complications, hypertensive disorders also significantly affect foetal outcomes by impairing uteroplacental circulation, which may result in intrauterine growth restriction, preterm birth, and perinatal mortality [16].
From a clinical pharmacotherapy perspective, the early identification and appropriate management of hypertensive disorders during pregnancy are essential to prevent disease progression and reduce adverse outcomes. Pharmacological management often involves the careful use of antihypertensive agents such as labetalol, nifedipine, and methyldopa, which are considered relatively safe during pregnancy when used under appropriate clinical supervision. Clinical pharmacists play an important role in optimizing antihypertensive therapy, monitoring drug safety, preventing medication-related complications, and ensuring adherence to evidence-based treatment guidelines.
Overall, the findings of the present study highlight the predominance of gestational hypertension and demonstrate a clear progression of blood pressure severity across hypertensive disorders of pregnancy. These results emphasize the importance of routine antenatal blood pressure monitoring, early risk stratification, and multidisciplinary management to minimize maternal and foetal complications associated with hypertensive pregnancy disorders.
Table 3. Incidence of Different Hypertensive Disorders
|
Disorder |
Cases |
|
Gestational Hypertension |
125 |
|
Preeclampsia |
58 |
|
Eclampsia |
8 |
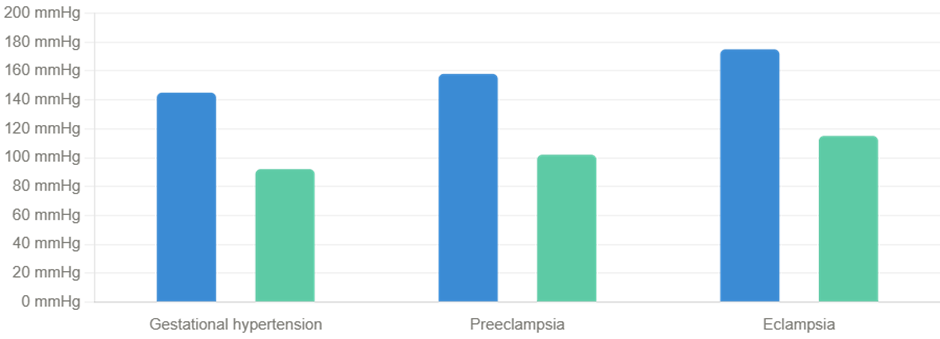
Figure 1. Blood Pressure Trends in Hypertensive Pregnancy Disorders
(Bar graph illustrating progressive elevation in systolic and diastolic blood pressure from gestational hypertension to preeclampsia and eclampsia.)
Maternal and Neonatal Outcomes in Hypertensive Pregnancies
The maternal and neonatal outcomes associated with hypertensive disorders of pregnancy are summarized in Table 4. The analysis revealed that preterm birth occurred considerably more frequently among hypertensive pregnancies (21.5%) compared with non-hypertensive pregnancies (5.4%). This finding indicates a strong association between maternal hypertension and premature delivery. In contrast, the occurrence of foetal growth restriction showed relatively similar proportions between hypertensive (5.2%) and non-hypertensive pregnancies (5.4%), suggesting that additional maternal or placental factors may influence foetal growth patterns in this cohort. The incidence of stillbirth was slightly lower among hypertensive pregnancies (6.3%) compared with non-hypertensive pregnancies (10.7%), whereas maternal stroke was reported in a small proportion of both groups, reflecting the relatively low frequency of severe neurological complications within the study population.
The comparative distribution of these maternal and neonatal outcomes is illustrated in Figure 3, which demonstrates the higher frequency of preterm birth among pregnancies complicated by hypertension.
Statistical comparison of maternal and neonatal outcomes revealed that preterm birth was significantly more common among hypertensive pregnancies (p < 0.05). Hypertensive disorders of pregnancy are characterized by impaired uteroplacental perfusion resulting from endothelial dysfunction and increased vascular resistance, which compromises oxygen and nutrient delivery to the foetus. As a result, clinicians may need to initiate early delivery to prevent maternal and foetal deterioration, thereby increasing the incidence of preterm birth. Although other outcomes such as foetal growth restriction and stroke did not demonstrate strong statistical differences between the groups in this study, hypertensive disorders remain important contributors to adverse obstetric outcomes.
Hypertensive disorders of pregnancy are widely recognized as one of the major causes of maternal and neonatal morbidity worldwide. The increased prevalence of preterm birth observed in this study is consistent with previous research indicating that hypertension during pregnancy often leads to placental insufficiency and foetal compromise, necessitating medically indicated preterm delivery. Large cohort studies have reported that women with hypertensive disorders are at significantly higher risk of delivering prematurely compared with normotensive pregnancies [17].
The pathophysiological mechanisms underlying these complications involve abnormal placental implantation and defective remodelling of uterine spiral arteries, which results in reduced placental perfusion and increased oxidative stress. These alterations contribute to placental ischemia and inflammatory responses, ultimately affecting foetal growth and increasing the likelihood of preterm birth and other neonatal complications [16].
Although foetal growth restriction was not markedly elevated in this study, previous investigations have shown that chronic uteroplacental insufficiency associated with hypertensive disorders may impair foetal nutrient supply, thereby increasing the risk of intrauterine growth restriction and low birth weight [18]. Furthermore, severe hypertensive complications such as eclampsia may predispose pregnant women to rare but life-threatening events including cerebrovascular accidents and organ dysfunction.
From a clinical pharmacy perspective, effective management of hypertensive disorders during pregnancy requires careful selection and monitoring of antihypertensive therapy to balance maternal cardiovascular stability with foetal safety. Medications such as labetalol, nifedipine, and methyldopa are commonly recommended as first-line agents due to their favorable safety profiles in pregnancy. Clinical pharmacists play an important role in monitoring therapeutic response, preventing drug-related adverse effects, and supporting multidisciplinary care strategies aimed at improving maternal and neonatal outcomes.
Overall, the findings of the present study highlight the significant association between hypertensive disorders and adverse obstetric outcomes, particularly preterm birth. These results emphasize the importance of early antenatal screening, regular blood pressure monitoring, and evidence-based pharmacological management to reduce the burden of hypertensive complications during pregnancy.
Table 4. Maternal and Neonatal Outcomes in Hypertensive Disorders
|
Outcome |
Hypertensive Pregnancies (%) |
Non-Hypertensive Pregnancies (%) |
|
Preterm Birth |
21.5 |
5.4 |
|
Foetal Growth Restriction |
5.2 |
5.4 |
|
Stillbirth |
6.3 |
10.7 |
|
Stroke |
1.0 |
0.9 |
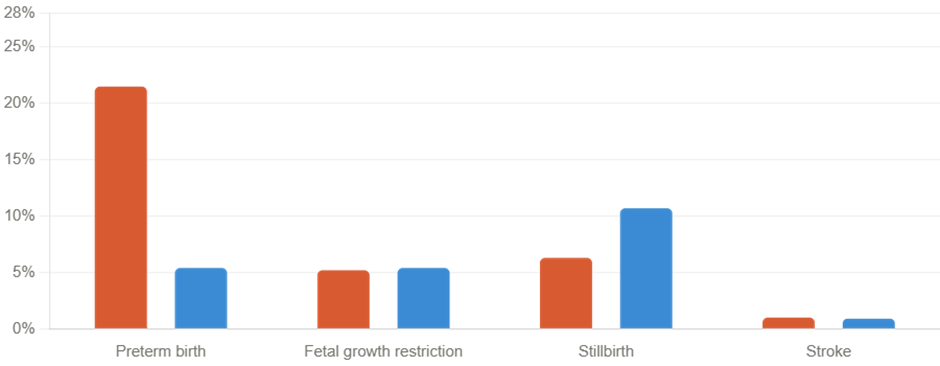
Figure 3. Comparison of Maternal and Neonatal Outcomes in Hypertensive and Non-Hypertensive Pregnancies
(Bar chart comparing the frequency of maternal and neonatal outcomes between hypertensive and normotensive pregnancies.)
Endocrine Complications in Pregnancy
The prevalence of endocrine disorders observed among the study participants is summarized in Table 5. Among the endocrine abnormalities identified, thyroid disorders were the most frequently reported condition, affecting 127 women (41.9%), followed by gestational diabetes mellitus (98 cases; 32.3%), while adrenal dysfunction was rare, with only 2 cases (0.7%) reported during the study period. These findings indicate that thyroid-related abnormalities represent the predominant endocrine complication affecting pregnant women in the present cohort.
The distribution of endocrine disorders is illustrated in Figure 4, which demonstrates the relative proportion of thyroid dysfunction, gestational diabetes mellitus, and adrenal disorders within the study population. The graphical representation clearly highlights thyroid disorders as the leading endocrine disturbance observed during pregnancy.
Descriptive statistical analysis revealed that thyroid disorders accounted for the largest proportion of endocrine complications in the study population. The prevalence of thyroid dysfunction was substantially higher than that of gestational diabetes mellitus and adrenal disorders. Although adrenal dysfunction occurred infrequently, its presence remains clinically important due to its potential impact on maternal hemodynamic stability and foetal development.
Endocrine disorders during pregnancy represent an important clinical concern because hormonal imbalances can significantly influence both maternal physiology and foetal development. In the present study, thyroid disorders were identified as the most prevalent endocrine complication, accounting for nearly two-fifths of the study population. Thyroid hormones are essential for regulating maternal metabolism, maintaining normal placental function, and supporting foetal brain development, particularly during early gestation when the foetus relies entirely on maternal thyroid hormone supply.
Abnormalities in thyroid function during pregnancy, including hypothyroidism, hyperthyroidism, and subclinical thyroid disorders, have been associated with several adverse obstetric outcomes such as miscarriage, preterm birth, gestational hypertension, and impaired neurocognitive development in offspring. These complications occur primarily due to alterations in maternal metabolic regulation and placental hormone interactions that influence foetal growth and development.
The relatively high prevalence of gestational diabetes mellitus (32.3%) observed in this study further highlights the metabolic challenges associated with pregnancy. Gestational diabetes results from pregnancy-induced insulin resistance combined with inadequate pancreatic β-cell compensation, leading to maternal hyperglycaemia. Uncontrolled maternal glucose levels can contribute to complications such as macrosomia, neonatal hypoglycaemia, and increased risk of future type 2 diabetes in both mother and child.
The very low occurrence of adrenal dysfunction (0.7%) in this cohort is consistent with clinical observations that adrenal disorders during pregnancy are relatively rare compared with thyroid and glucose metabolism abnormalities. However, conditions such as Cushing’s syndrome or adrenal insufficiency, although uncommon, can significantly affect maternal cardiovascular stability and pregnancy outcomes if not diagnosed and managed appropriately.
These findings are consistent with international epidemiological studies indicating that thyroid dysfunction is one of the most prevalent endocrine disorders affecting pregnant women globally. Global health reports have emphasized the importance of routine screening for thyroid abnormalities during pregnancy, particularly in regions where iodine deficiency or autoimmune thyroid disease is common [18].
From a clinical pharmacy and pharmacotherapeutic perspective, early detection and appropriate management of endocrine disorders are critical for optimizing maternal and foetal outcomes. Clinical pharmacists play a key role in monitoring pharmacotherapy for thyroid disorders and gestational diabetes, evaluating drug safety during pregnancy, adjusting medication dosages when necessary, and educating patients about adherence and lifestyle modifications. Integrating pharmaceutical care into antenatal services can enhance medication safety and improve therapeutic outcomes for pregnant women experiencing endocrine complications.
Overall, the findings of the present study emphasize the predominance of thyroid disorders and gestational diabetes among endocrine complications during pregnancy. These results underscore the importance of routine antenatal endocrine screening, multidisciplinary management strategies, and evidence-based pharmacotherapy to reduce maternal and neonatal risks associated with endocrine abnormalities.
Table 5. Prevalence of Endocrine Disorders in Pregnancy
|
Disorder |
Number of Cases |
Percentage (%) |
|
Thyroid Disorders |
127 |
41.9 |
|
Gestational Diabetes Mellitus |
98 |
32.3 |
|
Adrenal Dysfunction |
2 |
0.7 |
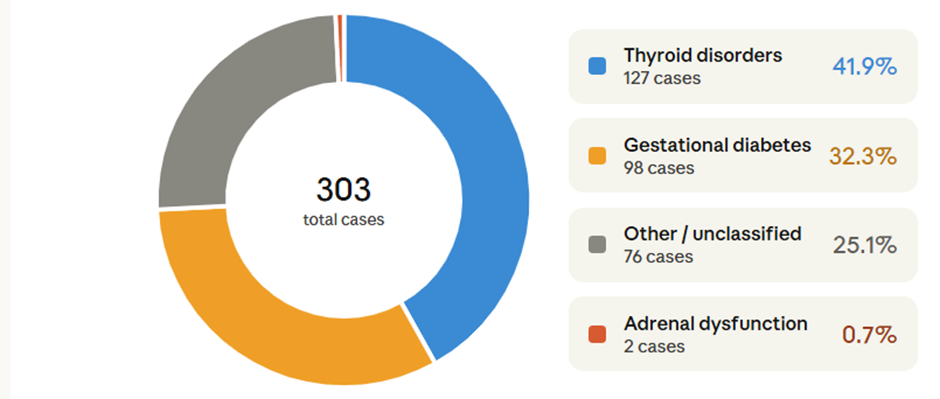
Figure 4. Distribution of Endocrine Disorders in Pregnancy
(Pie chart illustrating the proportion of thyroid disorders, gestational diabetes mellitus, and adrenal dysfunction among pregnant women.)
Maternal and Neonatal Outcomes in Gestational Diabetes Mellitus
The maternal and neonatal outcomes associated with gestational diabetes mellitus (GDM) are presented in Table 6. Comparative analysis between women diagnosed with GDM and those without GDM demonstrated notable differences in several obstetric and neonatal outcomes. The occurrence of preterm birth was higher among women with GDM (7 cases) compared with those without GDM (34 cases), and this difference was statistically significant (p = 0.030). Similarly, foetal macrosomia was more frequently observed among pregnancies complicated by GDM (7 cases) compared with non-GDM pregnancies (4 cases), with the association reaching statistical significance (p = 0.043).
In contrast, neonatal hypoglycaemia occurred in relatively few cases, with 2 cases reported in the GDM group and 4 cases in the non-GDM group, and the difference between the groups was not statistically significant (p = 1.000). A particularly notable finding was the markedly higher incidence of postpartum diabetes among women previously diagnosed with GDM (62 cases) compared with the non-GDM group (9 cases). This association demonstrated strong statistical significance (p < 0.001), indicating a substantial long-term metabolic risk among women who develop gestational diabetes during pregnancy.
The statistical analysis indicates that gestational diabetes mellitus is significantly associated with adverse pregnancy outcomes, particularly preterm birth and foetal macrosomia. Maternal hyperglycaemia results in increased transfer of glucose across the placenta, which stimulates excess insulin secretion in the foetus. This condition, known as foetal hyperinsulinemia, promotes accelerated foetal growth and contributes to the development of macrosomia. Additionally, metabolic disturbances associated with maternal hyperglycaemia may trigger obstetric complications that increase the likelihood of preterm delivery.
Gestational diabetes mellitus is one of the most common metabolic disorders encountered during pregnancy and has been associated with both short-term obstetric complications and long-term metabolic consequences for the mother and offspring. The findings of the present study demonstrate a significant association between GDM and adverse pregnancy outcomes, particularly preterm birth and foetal macrosomia. These results are consistent with previous investigations that have identified maternal hyperglycaemia as a major determinant of abnormal foetal growth patterns and pregnancy complications.
The mechanism underlying macrosomia in pregnancies complicated by GDM involves excessive maternal glucose availability, which freely crosses the placenta and leads to increased foetal insulin secretion. Insulin acts as a potent foetal growth factor, stimulating adipose tissue deposition and overall foetal growth. As a result, infants born to mothers with GDM are at increased risk of macrosomia, birth trauma, and metabolic disturbances in the neonatal period [19].
Preterm birth is another important complication associated with gestational diabetes. Maternal hyperglycaemia and metabolic dysregulation can contribute to placental dysfunction and inflammatory responses, which may precipitate premature labor or necessitate early delivery due to maternal or foetal complications. Large epidemiological studies have reported a higher prevalence of preterm birth among pregnancies affected by GDM compared with normoglycaemic pregnancies [20].
One of the most clinically significant findings in the present study is the strong association between GDM and postpartum diabetes mellitus. Women who develop gestational diabetes have been shown to possess underlying insulin resistance and β-cell dysfunction, which persist after pregnancy and substantially increase the risk of developing type 2 diabetes mellitus later in life. Long-term follow-up studies have demonstrated that up to 50% of women with a history of GDM may develop type 2 diabetes within 10 years of pregnancy, emphasizing the importance of postpartum metabolic monitoring and preventive interventions [21].
From a clinical pharmacy perspective, effective management of gestational diabetes requires careful monitoring of glycaemic control and appropriate pharmacotherapeutic interventions. Lifestyle modification, including dietary counselling and physical activity, represents the first-line management strategy. However, pharmacological therapy such as insulin or selected oral hypoglycaemic agents may be required when lifestyle interventions are insufficient to maintain adequate glycaemic control. Clinical pharmacists play an essential role in optimizing antidiabetic therapy, monitoring medication safety during pregnancy, and providing patient education regarding adherence and lifestyle management.
Overall, the findings of this study emphasize the importance of early screening for gestational diabetes, strict glycaemic control during pregnancy, and continued metabolic monitoring after delivery. These strategies are crucial for reducing adverse maternal and neonatal outcomes and for preventing the long-term progression to type 2 diabetes mellitus among women affected by gestational diabetes.
Table 6. Outcomes Associated with Gestational Diabetes Mellitus
|
Outcome |
GDM |
Non-GDM |
p-value |
|
Preterm Birth |
7 |
34 |
0.030 |
|
Macrosomia |
7 |
4 |
0.043 |
|
Neonatal Hypoglycaemia |
2 |
4 |
1.000 |
|
Postpartum Diabetes |
62 |
9 |
<0.001 |
Association Between Gestational Diabetes Mellitus and Hypertensive Disorders
The association between gestational diabetes mellitus (GDM) and hypertensive disorders of pregnancy is presented in Table 7. The analysis revealed that gestational hypertension occurred more frequently among women diagnosed with GDM (40 cases) compared with women without GDM (15 cases). Similarly, preeclampsia was more commonly observed in the GDM group (19 cases) than in the non-GDM group (8 cases). The observed differences between the groups were statistically significant (p < 0.05), indicating a meaningful relationship between gestational diabetes and hypertensive conditions during pregnancy.
These findings suggest that women with gestational diabetes are at an increased risk of developing hypertensive complications compared with normoglycaemic pregnant women. The coexistence of these two conditions reflects shared metabolic and vascular disturbances that influence maternal cardiovascular function during pregnancy.
Statistical analysis demonstrated a significant association between GDM and both gestational hypertension and preeclampsia (p < 0.05). The increased prevalence of hypertensive disorders among women with GDM suggests that metabolic abnormalities occurring during pregnancy may contribute to vascular dysfunction and impaired placental circulation. This relationship highlights the importance of comprehensive metabolic monitoring during antenatal care.
To further evaluate the predictors of hypertensive disorders during pregnancy, a multivariable logistic regression analysis was performed, and the results are presented in Table 8. The regression model demonstrated that gestational diabetes mellitus was a significant predictor of hypertensive disorders, with an odds ratio (OR) of 3.45 (95% CI: 1.62–7.34; p = 0.001). This finding indicates that women diagnosed with gestational diabetes were approximately 3.45 times more likely to develop hypertensive complications during pregnancy compared with women without GDM.
In contrast, maternal obesity did not show a statistically significant association with hypertensive disorders in this study population (p > 0.05). Although obesity is widely recognized as a risk factor for both metabolic and cardiovascular complications, its influence may vary depending on the demographic characteristics and baseline health status of the study population.
The logistic regression model highlights gestational diabetes mellitus as an independent predictor of hypertensive disorders of pregnancy, emphasizing the close relationship between metabolic and cardiovascular complications during gestation. The confidence interval (95% CI: 1.62–7.34) indicates a robust and clinically meaningful association between GDM and hypertensive disorders.
The present study demonstrated a significant association between gestational diabetes mellitus and hypertensive disorders of pregnancy, including gestational hypertension and preeclampsia. These findings support previous epidemiological studies that have reported a strong relationship between metabolic dysregulation and vascular complications during pregnancy.
The pathophysiological link between gestational diabetes and hypertensive disorders is largely attributed to insulin resistance, endothelial dysfunction, and chronic low-grade inflammation. Pregnancy is characterized by progressive insulin resistance, and in women with GDM this metabolic disturbance becomes more pronounced, leading to hyperglycaemia and increased oxidative stress. These metabolic alterations contribute to vascular endothelial injury, impaired nitric oxide production, and increased systemic vascular resistance, which may predispose affected women to hypertensive disorders [22].
Furthermore, insulin resistance and hyperglycaemia may disrupt normal placental development and function, resulting in abnormal trophoblastic invasion and reduced uteroplacental perfusion. These alterations can trigger inflammatory responses and endothelial activation, which are key mechanisms involved in the development of preeclampsia [23]. Consequently, women with gestational diabetes often exhibit overlapping metabolic and cardiovascular risk profiles that increase their susceptibility to hypertensive complications.
The findings of the logistic regression analysis further support this relationship by demonstrating that gestational diabetes significantly increases the likelihood of developing hypertensive disorders during pregnancy. Similar results have been reported in large cohort studies, which have shown that women with GDM have a substantially higher risk of developing pregnancy-induced hypertension and preeclampsia compared with normoglycaemic women [24].
From a clinical pharmacy and maternal health perspective, these findings highlight the importance of integrated metabolic and cardiovascular monitoring during pregnancy. Early screening for gestational diabetes and timely management of hyperglycaemia can help reduce the risk of hypertensive complications. Clinical pharmacists can contribute to improved maternal outcomes by optimizing pharmacotherapy for glycaemic control, monitoring medication safety during pregnancy, and providing patient counselling on lifestyle modifications and adherence to treatment regimens.
Overall, the observed association between gestational diabetes and hypertensive disorders underscores the need for comprehensive antenatal risk assessment and multidisciplinary management strategies aimed at reducing the burden of metabolic and cardiovascular complications during pregnancy.
Table 7. Association Between Gestational Diabetes Mellitus and Hypertensive Conditions
|
Condition |
GDM Present |
GDM Absent |
p-value |
|
Gestational Hypertension |
40 |
15 |
<0.05 |
|
Preeclampsia |
19 |
8 |
<0.05 |
Table 8. Predictors of Hypertensive Disorders (Logistic Regression Analysis)
|
Predictor |
Odds Ratio |
95% CI |
p-value |
|
Gestational Diabetes Mellitus |
3.45 |
1.62–7.34 |
0.001 |
|
Obesity |
Not significant |
— |
>0.05 |
The present study evaluated the prevalence of cardiovascular and endocrine complications during pregnancy, with particular emphasis on hypertensive disorders and gestational diabetes mellitus. The findings demonstrate that hypertensive disorders and thyroid dysfunction were among the most frequently observed complications, while gestational diabetes also contributed significantly to adverse maternal and neonatal outcomes. These observations highlight the complex interaction between metabolic, endocrine, and cardiovascular pathways that influence pregnancy outcomes.
Hypertensive disorders of pregnancy remain one of the leading causes of maternal morbidity and mortality globally. In the current study, gestational hypertension and preeclampsia accounted for the majority of cardiovascular complications, with a progressive increase in blood pressure levels observed across disease severity. These findings are consistent with previous reports indicating that abnormal placental development and systemic endothelial dysfunction are central mechanisms in the pathogenesis of hypertensive disorders during pregnancy [25]. Impaired placental perfusion leads to increased vascular resistance, inflammatory activation, and oxidative stress, ultimately contributing to maternal cardiovascular complications.
The study also demonstrated a significant association between hypertensive disorders and adverse pregnancy outcomes, particularly preterm birth. Hypertension during pregnancy can compromise uteroplacental circulation, resulting in reduced oxygen and nutrient supply to the foetus. Consequently, obstetric interventions such as medically indicated preterm delivery may be required to prevent further maternal or foetal complications. Similar associations have been reported in large population-based studies, which identify hypertensive disorders as a major determinant of preterm birth and perinatal morbidity [26].
Endocrine disturbances were also common among the study population. Thyroid disorders represented the most prevalent endocrine abnormality, consistent with international studies reporting that thyroid dysfunction affects a substantial proportion of pregnant women worldwide. Adequate thyroid hormone levels are essential for foetal neurological development, particularly during early gestation when foetal thyroid function is not fully established. Maternal thyroid dysfunction has been associated with adverse outcomes including miscarriage, preterm delivery, and impaired neurocognitive development in offspring [27].
Gestational diabetes mellitus was another significant metabolic complication identified in this study. The results demonstrated strong associations between GDM and both preterm birth and foetal macrosomia, reflecting the metabolic consequences of maternal hyperglycemia. Excess maternal glucose readily crosses the placenta and stimulates foetal insulin secretion, which acts as a growth-promoting hormone and leads to excessive foetal growth. This mechanism has been widely documented in clinical studies examining the impact of maternal glycaemic control on foetal development [28].
An important finding of the present study was the significant association between gestational diabetes mellitus and hypertensive disorders, as well as the identification of GDM as an independent predictor of hypertensive complications in logistic regression analysis. These findings suggest that metabolic disturbances such as insulin resistance and systemic inflammation may contribute to vascular dysfunction during pregnancy. Previous studies have reported similar relationships between GDM and hypertensive disorders, indicating shared pathophysiological pathways that increase maternal cardiovascular risk [29].
Overall, the results emphasize the importance of comprehensive antenatal screening for metabolic and cardiovascular complications. Early identification and multidisciplinary management of these conditions are essential for improving maternal and neonatal outcomes.
CLINICAL IMPLICATIONS
The findings of this study have several important implications for clinical practice, particularly in the context of maternal health management. First, routine screening for hypertensive disorders and gestational diabetes should be considered an essential component of antenatal care. Early detection allows timely intervention and may reduce the risk of severe maternal and neonatal complications.
Second, the study highlights the need for integrated management strategies that address both metabolic and cardiovascular risk factors during pregnancy. Multidisciplinary collaboration involving obstetricians, endocrinologists, and clinical pharmacists can enhance patient care through individualized treatment plans and careful monitoring of pharmacotherapy.
Clinical pharmacists play a crucial role in improving maternal outcomes through medication therapy management, pharmacovigilance, and patient education. Monitoring drug safety during pregnancy, optimizing antihypertensive and antidiabetic therapy, and promoting adherence to lifestyle modifications can significantly reduce treatment-related risks and improve therapeutic effectiveness.
Additionally, the identification of gestational diabetes as a predictor of hypertensive disorders underscores the importance of postpartum metabolic follow-up, as women with a history of GDM are at increased risk of developing type 2 diabetes mellitus later in life.
LIMITATIONS
Despite the important findings, several limitations should be considered when interpreting the results of this study. First, the study was conducted in a single tertiary care center, which may limit the generalizability of the findings to broader populations. Differences in demographic characteristics, healthcare access, and regional health practices may influence the prevalence of pregnancy-related complications.
Second, the sample size, although adequate for descriptive analysis, may not fully capture the variability of rare complications such as peripartum cardiomyopathy or adrenal disorders. Larger multicenter studies may provide a more comprehensive understanding of these conditions.
Third, the observational design of the study restricts the ability to establish causal relationships between metabolic and cardiovascular complications during pregnancy. Longitudinal studies with extended follow-up periods would be valuable in assessing long-term maternal and neonatal outcomes.
CONCLUSION
In conclusion, the present study highlights the significant burden of cardiovascular and endocrine complications during pregnancy, particularly hypertensive disorders, thyroid dysfunction, and gestational diabetes mellitus. The findings demonstrate that gestational diabetes is strongly associated with hypertensive disorders and adverse pregnancy outcomes, including preterm birth and foetal macrosomia.
The identification of gestational diabetes as an independent predictor of hypertensive complications underscores the importance of early metabolic screening and integrated antenatal management strategies. Routine monitoring of blood pressure, thyroid function, and glucose levels during pregnancy can facilitate early diagnosis and timely intervention.
Effective multidisciplinary care, including the involvement of clinical pharmacists in medication management and patient counselling , may improve maternal and neonatal outcomes by ensuring safe and evidence-based pharmacotherapy.
FUTURE RESEARCH DIRECTIONS
Future research should focus on large multicenter studies to better understand the epidemiology and risk factors associated with metabolic and cardiovascular complications during pregnancy. Such studies would help establish more robust evidence for preventive strategies and clinical management guidelines.
Longitudinal investigations are also needed to evaluate the long-term metabolic and cardiovascular outcomes among women with gestational diabetes and hypertensive disorders. Understanding these long-term health risks may facilitate the development of targeted postpartum screening programs and preventive interventions.
In addition, future research should explore the role of clinical pharmacy interventions in optimizing medication safety and therapeutic outcomes during pregnancy. Pharmacist-led programs focusing on medication adherence, pharmacovigilance, and patient education may contribute significantly to improving maternal healthcare quality.
Finally, advances in precision medicine and biomarker research may provide new insights into the early detection and prediction of pregnancy-related complications, enabling personalized approaches to maternal healthcare.
ACKNOWLEDGMENT
The authors gratefully acknowledge the administrative authorities and healthcare professionals of SCCL Main Hospital, Kothagudem, for their valuable support and cooperation during the conduct of this study. Their assistance in facilitating access to patient records and clinical information was essential for successful data collection and analysis.
The authors also extend their sincere appreciation to the Department of Pharmacy Practice, KLR College of Pharmacy, Paloncha, for providing academic mentorship, research guidance, and the necessary institutional support throughout the study period. Special thanks are conveyed to the clinical pharmacists, nursing staff, and obstetric care team whose collaboration and professional insights contributed significantly to the completion of this research and to improving the quality of patient-centered clinical care.
CONFLICT OF INTEREST
The authors affirm that there are no financial, professional, or personal relationships that could have influenced the design, conduct, analysis, or reporting of this research. This study was performed independently, and the results presented are based solely on the data collected and interpreted according to established scientific and ethical standards.
REFERENCES






G. Jithendra, K. Sreya, Ch. Keerthi Priya, S. Sravani, M. Sowjanya, V Ramya Sri, K. Shireesha, Rajani G, Prevalence and Clinical Profile of Cardiac and Endocrine Complications in Pregnancy: A Hospital-Based Observational Study from a Tertiary Care Center in South India , Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 582-604. https://doi.org/10.5281/zenodo.19410575
 10.5281/zenodo.19410575
10.5281/zenodo.19410575