
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
K. V. N. Naik S. P. Sanstha’s, Institute of Pharmaceutical Education & Research, Canada Corner, Nashik, 422002, Maharashtra, India
Pharmacovigilance plays a critical role in the detection, assessment, and prevention of adverse drug reactions (ADRs). The present study evaluates the role of pharmacovigilance in monitoring ADRs using data obtained from a clinical trial (IN004) conducted in a hospital setting. A total of 20 adverse events were analyzed and categorized based on severity and causality assessment. The findings revealed that 40% of the reported reactions were of moderate severity, with hypertriglyceridemia being one of the commonly observed events. Most reactions showed improvement following appropriate clinical intervention. Causality assessment using established scales, including those developed by the World Health Organization (WHO) and Uppsala Monitoring Centre (UMC), facilitated systematic evaluation of drug-related effects. The study highlights the importance of timely ADR reporting and structured pharmacovigilance practices in improving patient safety and minimizing drug- related risks.
An Adverse Drug Reaction (ADR) is an harmful or unintended or unwanted response of drug taken at normal human dose. Drugs can save our lives. Sometimes they can also cause harm. This happens when medicines have effects at normal doses. The World Heath Organization (WHO) says that an adverse drug reaction is a response to a drug that we do not expect and that happens at normal doses used by people. In trials these ADR can be very serious. Pharmacovigilance is the process of finding these problems and keeping patients safe. Every year thousands of drug reactions happen all around the world. Some drugs are even banned completely because of this. For example, Thalidomide caused birth defects in the 1960s. Rofecoxib caused heart attacks in 2004. These tragedies show us why it is so important to monitor drug reactions. Pharmacovigilance uses tools like the World Health Organization causality assessment to decide if a drug caused harm. This helps doctor s make choices when it comes to treating patients. Adverse drug reactions a problem and pharmacovigilance is the key to solving it.
India started the Pharmacovigilance Programme of India (PvPI) in 2010 under the Indian Pharmacopoeia Commission. This program collects reports of drug reactions from more than 250 Adverse Drug Monitoring Centres across India. When clinical trails are being done they must report any drug reactions within 14 days to the Central Drugs Standard Control Organization (CDSCO). This system has caught problems with drugs like Nimesulide and Pioglitazone early on. Clinical trials for diabetes like the one called IN004 have risks. Drugs used to treat diabetes can often cause ADRs, such as high blood sugar and high triglycerides . Data from hospitals shows that 10 to 20 % of patients get mild to adverse drug reactions. Most of the time these reactions can be. The patient will be okay but severe cases need to be taken care of right away. The Pharmacovigilance Programme of India uses a scale to assess causality of drug reactions: Certain, Probable, Possible, Unlikely and Unassessable. The data from In004 trials shows that most of the cases were classified as Unlikely, which is typical for trails that are being closely monitored. Adverse Drug Reactions are concern in India and the Pharmacovigilance Programme of India is working to address this issue.
This paper looks at data from a clinical trial called IN004 SARO. 21.003. The data shows events that happened to subjects in the trails. These events include triglycerides, high blood sugar and the common cold. We looked at how severe these events were what happened to the patients and how the causality of the drug reactions was assessed. Our goals were to show how pharmacovigilance can monitor drug reactions in real time to demonstrate how the World Health Organization causality assessment is used and to prove that structured reporting can help prevent patient harm. The study found that high triglycerides were then common adverse drug reactions. One subject, IN0040019 had case of high triglycerides that got better after treatment. Most of the events were not related to the study drug, which shows that the trial was being closely monitored and problems were caught early. Using data from the IN004 trial we looked at the patterns of drug reactions how patients responded to treatment and the pharmacovigilance processes that were used. This research helps fill the gap between what students learn in school and what actually happens in hospitals. The results will help future pharmacists understand how to manage drug reactions, in the real world. The IN004 study is an example of how pharmacovigilance can be used to keep patients safe.
Table 1. Classification of Adverse Drug Reactions (ADRs)
|
ADR Category |
Characteristics |
Common Examples |
|
Type A (Augmented) |
Predictable reactions usually related to drug dose and pharmacological action |
Bleeding associated with anticoagulants |
|
Type B (Bizarre) |
Uncommon and unpredictable reactions not related to normal drug action |
Allergic reaction to penicillin |
|
Type C (Chronic) |
Adverse events occurring after prolonged therapy |
Adrenal suppression caused by corticosteroids |
|
Type D (Delayed) |
Reactions that appear after a long latency period |
Drug-induced carcinogenic effects |
|
Type E (End-of-use) |
Effects observed after abrupt discontinuation of therapy |
Withdrawal symptoms following opioid cessation |
|
Type F (Failure) |
Inadequate therapeutic response during treatment |
Reduced efficacy due to antimicrobial resistance |
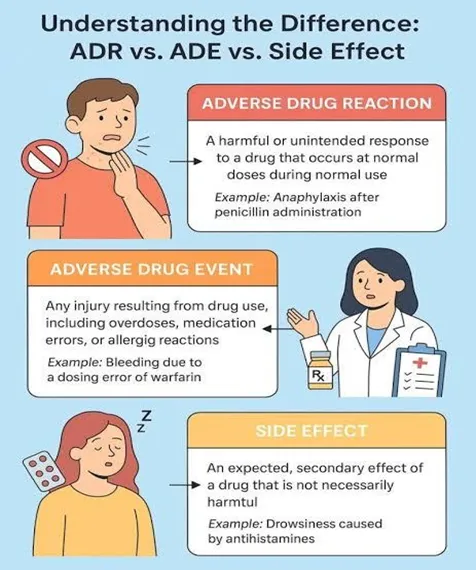
Figure 1. Difference Between ADR, ADE, and Side EffectsFigure
CONCEPT OF PHARMACOVIGILANCE:
Pharmacovigilance is an important branch of healthcare that focuses on the detection, assessment, understanding, and prevention of adverse drug reactions (ADRs) and other medicine- related problems. The term Pharmacovigilance is derived from the Greek word “pharmakon”, meaning drug and the Latin word “vigilare”, meaning to keep watch. The World Health Organization (WHO) defines Pharmacovigilance as the science and activities associated with identifying and preventing harmful effects caused by medicines.
The need for Pharmacovigilance has increased significantly due to the growing use of Pharmaceutical products worldwide. Although medicines undergo extensive clinical testing before approval, certain adverse reactions may appear only after the drug is widely used in large populations. Clinical Trials are usually conducted under controlled conditions and may not detect rare, delayed or population-specific adverse effects. Therefore, continuous monitoring after marketing approval is essential to ensure patient safety.
Pharmacovigilance systems collects safety information from hospitals, healthcare professionals, patients, clinical trials and post-marketing surveillance programmes. The collected data are analyzed to identify possible safety signals and evaluate the relationship between a drug and an observed adverse event. Effective pharmacovigilance practices support safer prescribing, rational use of medicines, and timely regulatory actions when necessary.
In recent years, pharmacovigilance has expanded beyond conventional ADR reporting and now includes monitoring of vaccines, biological products, herbal medicines and medical devices. Technological advancements such electronic health records and digital reporting systems have further strengthened pharmacovigilance activities and improved drug safety monitoring worldwide

Figure 2. Key Goals of Pharmacovigilance
METHODS FOR ADVERSE DRUG REACTION (ADRs) MONITORING:
Monitoring of Adverse drug reactions (ADRs) is an essential component of pharmacovigilance and plays a significant role in ensuring medication safety. Various methods are used to identify, evaluate and prevent harmful drugs-related effects in patients. These monitoring systems help healthcare professionals detect previously unknown reactions and assess the safety profile of medicines during clinical use.
1. Spontaneous Reporting System:
The spontaneous reporting system is one of the most widely used methods for monitoring adverse drug reactions. In this approach, healthcare professionals such as physicians, pharmacists, and nurses voluntarily report suspected ADRs to pharmacovigilance centres or regulatory authorities. Patients may also submit reports in certain reporting systems. This method is especially useful for detecting rare, serious, and previously unknown adverse reactions. That may not be identified during clinical trials. Despite its importance spontaneous reporting is often affected by underreporting, incomplete documentation, and lack of awareness among healthcare providers.
2. Active Surveillance:
Active surveillance involves systematic and continuous monitoring of patients to identify adverse drug reactions. Unlike passive reporting systems, this method actively collects safety data through direct follow-up, patient interviews, or regular clinical assessment. Active surveillance provides more reliable information regarding the frequency and severity of ADRs because patients are closely observed during treatment. This method is commonly used in hospitals, specialized clinics, and post-marketing safety studies.
3. Cohort Event Monitoring:
Cohort event monitoring is a prospective observational method used to evaluate the safety profile of medicines in a defined group of patients. Individuals receiving a particular drug are followed over a specific period to record adverse events and treatment outcomes. This method is useful for identifying patterns of drug-related problems in real-world clinical practice. Cohort studies provide valuable information regarding long-term safety and incidence of ADRs in larger populations.
4. Prescription Event Monitoring:
Prescription event monitoring is a pharmacovigilance technique in which patients receiving a newly marketed medicine are monitored through prescription records. Information regarding adverse events is collected from prescribing healthcare professionals after the drug has been dispensed. This method helps identify uncommon or delayed adverse effects associated with routine clinical use. It is particularly useful for evaluating the safety of medicines after marketing approval.
5. Hospital-Based Monitoring:
Hospital-based monitoring is an important pharmacovigilance approach because hospitalized patients often receive multiple medications and require continuous clinical observation. Healthcare professionals monitor patients for suspected ADRs during treatment and document adverse events accordingly. This method allows early identification and management of serious reactions, thereby reducing complications and improving patient safety. Clinical pharmacists play a significant role in strengthening hospital pharmacovigilance activities.
6. Electronic Databases and Data Mining:
Technological advancements have important pharmacovigilance through then use of electronic health records computerized databases, and data mining techniques. Large volumes of patient safety data can be analyzed rapidly to identify possible safety signals and trends. Data mining methods help detect unusual patterns of adverse events that may indicate previously unrecognized drug-related risks. These systems support faster and more efficient pharmacovigilance activities.
7. Causality Assessment Methods:
Causality assessment methods are used to determine the likelihood that a suspected drug caused a particular adverse event. Various standardized tools, including the WHO- Uppsala Monitoring Centre (UMC) scale, are commonly used for this purpose. These methods evaluate factors such temporal association, response after drug withdrawal, alternative causes, and previous evidence related to the reaction. Causality assessment improves the accuracy and reliability of ADR reporting and supports better clinical decision-making.
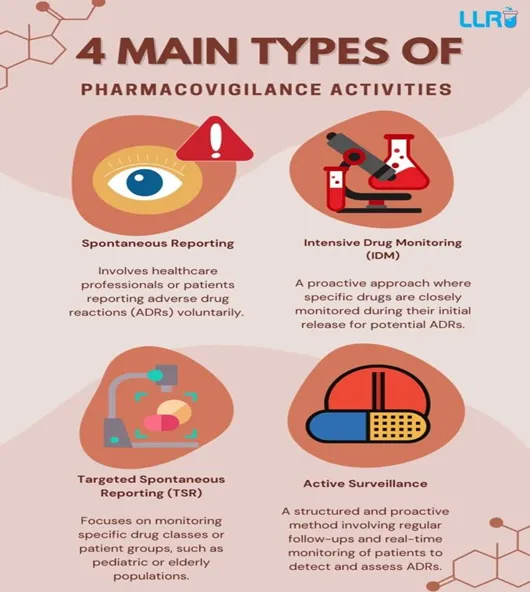
Figure 3. Major Pharmacovigilance Activities Used in ADR Monitoring
NATIONAL AND GLOBAL PHARMACOVIGILANCE SYSTEMS:
Keeping a close eye on the safety of medicines is crucial, and that’s where national and global pharmacovigilance systems come in. They help reduce the risk of bad reactions to drugs, known as adverse drug reactions or ADRs. These systems collect, analyze, and evaluate data on drug safety from various sources like healthcare professionals, hospitals, pharmaceutical companies, and patients. By constantly monitoring this data, regulatory authorities can spot potential safety issues with medicines and take action to protect people’s health. This ongoing surveillance is key to ensuring that medicines are safe for use and hat any problems are caught and addressed quickly.
The World Health Organization (WHO) has set up a program to make sure medicines are safe all around the world. This program is called the International Drug Monitoring Programme and it’s run by Uppsala Monitoring Centre (UMC) in Sweden. The UMC has a big database where it keeps track of all the bad reactions people have to medicines. Countries that are part of the program send in reports of these bad reactions, which helps find problems with medicines that might not be obvious at first. By working together, countries can spot potential issues with medicines more easily and make better decisions about how to regulate them. This helps keep people safe and makes sure that medicines are used in the best way possible. The database is really important because it allows countries to share information and learn from each other, which can help prevent bad things from happening to people who take medicines. Overall, the program big step forward in making sure that medicines are safe for everyone, no matter where they live.
In India, the Pharmacovigilance Programme of India (PvPI) was launched in 2010 under the Indian Pharmacopoeia Commission (IPC). The programme function through a network of Adverse Drug Reaction Monitoring Centres located in medical colleges, hospitals, and healthcare institutions across the country. Healthcare professionals are encouraged to report suspected ADRs using standardized reporting forms. The collected data are analyzed and forwarded to national and international monitoring systems for further evaluation.
National and global programs that monitor the safety and medicines play a big role in keeping patients safe. They help doctors and other healthcare professionals report problems with medicines quickly, and they teach these professionals about the importance of using medicines safely. These programs also help update the information that comes with medicines, warn people about potential dangers, and remove harmful medicines from the market when needed. To keep improving healthcare around world, it’s crucial that we continue to strengthen these programs. This will help us stay on top of any issues with medicines and make sure people get the best care possible. By working together, we can make a big difference in patient safety and overall healthcare outcomes.
CASE STUDY:
The present case study was based on adverse event data collected during the Phase IV clinical trial of Saroglitazar conducted in patients diagnosed with Non-alcoholic Fatty Liver Disease in a hospital setting. The study identified as IN004-SARO.21.003 was evaluated to understand the practical role of pharmacovigilance in monitoring and assessment of adverse drug reactions during clinical research. A total of 15 representative adverse events were selected for analysis from the reported clinical trial data.
The reported adverse events included hypertriglyceridemia, hyperglycemia, elevated alanine aminotransferase levels, common cold symptoms, and musculoskeletal complaints. Each adverse events was assessed according to severity, outcome, and possible causal relationship with Saroglitazar therapy using the WHO- Uppsala Monitoring Centre (WHO-UMC) causality assessment scale. Most adverse events were mild to highlight the importance of pharmacovigilance systems in identifying potential drug-related risks and improving patient safety during Phase IV clinical trials.
Table 2. Summary of Clinical Trial Details
|
Sr no |
Parameter |
Details |
|
1 |
Study Code |
IN004_SARO.21.003 |
|
2 |
Study Type |
Phase IV Clinical Trial |
|
3 |
Study Drug |
Saroglitazar |
|
4 |
Disease Condition |
Non-alcoholic Fatty Liver Disease |
|
5 |
Study Setting |
Hospital-based clinical study |
|
6 |
Objective |
Evaluation of adverse drug reactions and safety monitoring |
|
7 |
Numbers of Cases Evaluated |
15 representative adverse events |
|
8 |
ADR Monitoring Method |
Pharmacovigilance assessment and adverse event reporting |
|
9 |
Causality Assessment Tool |
WHO-Uppsala Monitoring Centre (WHO- UMC) Scale |
|
10 |
Commonly Observed ADRs |
Hypertriglyceridemia, Hyperglycemia, Elevated ALT levels |
|
11 |
Outcomes of ADRs |
Majority recovered after clinical management |
Table 3. Representative Adverse Events Reported During IN004_SARO.21.003 Clinical Trial
|
Sr no |
Subject No. |
Adverse event |
Severity |
Any medication received for this ADR |
Outcome |
Serious AE |
Relationship with study Drug |
|
1 |
IN004003 |
Alanine Aminotransferase |
Mild |
No |
Recovered/ Resolved |
No |
Unlikely |
|
2 |
IN004006 |
Type 2 diabetes mellitus |
Moderate |
Yes |
Recovered/ Resolved |
No |
Unlikely |
|
3 |
IN004007 |
Hypertriglyceridemia |
Mild |
No |
Recovered/ Resolved |
No |
Unlikely |
|
4 |
IN004008 |
Hypertriglyceridemia |
Moderate |
Yes |
Recovered/ Resolved |
No |
Unlikely |
|
5 |
IN004009 |
Hyperglycemia |
Moderate |
Yes |
Recovered/ Resolved |
No |
Unassessable/ Unclassifiable |
|
6 |
IN0040012 |
Common cold |
Mild |
Yes |
Recovered/ Resolved |
No |
Unlikely |
|
7 |
IN0040013 |
Common cold |
Mild |
Yes |
Recovered/ Resolved |
No |
Unlikely |
|
8 |
IN0040019 |
Hyperglycemia |
Moderate |
Yes |
Recovered/ Resolved |
No |
Unlikely |
|
9 |
IN0040023 |
Right Shoulder R. Cuff Tendinosis |
Mild |
Yes |
Recovered/ Resolved |
No |
Unlikely |
|
10 |
IN0040035 |
Common cold |
Mild |
Yes |
Recovered/ Resolved |
No |
Unlikely |
|
11 |
IN0040049 |
Hyperuricemia |
Mild |
Yes |
Recovered/ Resolved |
No |
Unassessable/ Unclassifiable |
|
12 |
IN0040053 |
Hypertriglyceridemia |
Severe |
No |
Not Recovered/ Resolved |
No |
Unlikely |
|
13 |
IN0040055 |
Hyperglycemia |
Mild |
No |
Not Recovered/ Resolved |
No |
Unlikely |
|
14 |
IN0040060 |
Hyperuricemia |
Mild |
Yes |
Recovered/ Resolved |
No |
Unassessable/ Unclassifiable |
|
15 |
IN0040062 |
Hypertriglyceridemia |
Moderate |
No |
Recovered/ Resolved |
No |
Unassessable/ Unclassifiable |
DISCUSSION:
Pharmacovigilance plays an essential role in improving drug safety by enabling early detection, assessment, and prevention of adverse drug reactions. The present review highlights the significance of ADR monitoring system in both clinical trials and routine healthcare practice. Although medicines provide therapeutic benefits, they may also produce undesirable effects that can affect patient compliance, treatment outcomes, and overall quality of life. Continuous pharmacovigilance activities therefore remain important for ensuring the safe and rational use of medicines.
The case study findings from the Phase IV clinical trial of Saroglitazar in patients with Non- alcoholic Fatty Liver Disease demonstrated the practical application of pharmacovigilance in hospital setting. Most reported adverse events were mild to moderate in severity and improved after appropriate in clinical management. Hypertriglyceridemia and hyperglycemia were among the commonly observed reactions during the study. Causality assessment using the WHO-Uppsala Monitoring Centre (WHO-UMC) scale helped determine the possible relationship between the study drug and reported adverse events. Most reactions were categorized as unlikely or unassessable, indicating the importance of systematic evaluation before establishing direct drug association.
The study also emphasizes the value of accurate ADR documentation and timely reporting in reducing potential drug-related risks. Hospital-based monitoring systems and clinical trial pharmacovigilance programmes contribute significantly to patient safety by supporting early identification and management of adverse events. Strengthening awareness among healthcare professionals regarding ADR reporting can further improve the effectiveness of pharmacovigilance systems.
CONCLUSION:
Pharmacovigilance is a vital part of healthcare that focuses on ensuring the safe and effective use of medicines through continuous monitoring of adverse drug reactions. Proper identification, evaluation, and reporting of ADRs help in reducing drug-related complications and improving overall patient safety. Effective pharmacovigilance practices also support healthcare professionals in making informed therapeutic decisions and promoting rational use of medicines.
The present review and case study emphasize the significance of ADR monitoring during Phase IV clinical trials involving Saroglitazar therapy in patients with Non-alcoholic Fatty Liver Disease. The reported adverse events were systematically monitored and assessed using established pharmacovigilance methods, including causality assessment tools. Most reactions observed during the study were mild to moderate in severity and responded well to appropriate clinical management and follow-up.
The findings demonstrate that structured ADR reporting systems and regular patient monitoring are essential for early detection of potential drug-related risks. Strengthening pharmacovigilance activities in hospitals and clinical research settings can contribute significantly to safer treatment practices, better healthcare outcomes and enhanced patient care in the future.
REFERENCES


Ishika Dargude, Lalan Wagh, Dr. Avinash Darekar, Role of Pharmacovigilance in Monitoring of Adverse Drug Reaction: A Case Study Approach, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 6817-6826. https://doi.org/10.5281/zenodo.20392137
 10.5281/zenodo.20392137
10.5281/zenodo.20392137