
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, LCIT School of Pharmacy Bilaspur (C.G).
Psoriasis is a chronic immune-mediated inflammatory skin disorder characterized by erythematous plaques, scaling, keratinocyte hyperproliferation, and infiltration of inflammatory cytokines. Conventional topical therapies often exhibit limited efficacy due to poor skin penetration, systemic adverse effects, and frequent dosing requirements. The present study focuses on the development and systematic evaluation of novel nanostructured lipid carriers (NLCs) loaded with Boswellic Acid for improved topical treatment of psoriasis. Boswellic acid possesses significant anti-inflammatory, antioxidant, and immunomodulatory properties; however, its therapeutic application is restricted by poor aqueous solubility and low bioavailability. To overcome these limitations, boswellic acid-loaded NLCs were formulated using suitable solid lipids, liquid lipids, and surfactants through the hot homogenization–technique.The developed formulations were systematically characterized for particle size, polydispersity index, zeta potential, entrapment efficiency, and in vitro drug release behavior. The optimized NLC formulation exhibited nanosized particles with high entrapment efficiency, good physical stability, and sustained drug release characteristics. boswellic acids were observed due to the occlusive and lipid-compatible nature of the NLC system. Furthermore, the formulation demonstrated improved anti-psoriatic potential by reducing inflammation, erythema, and epidermal hyperproliferations. That resulting boswellic acid-loaded NLCs represent a promising nanocarrier-based topical delivery system for psoriasis management. Novel formulation may enhance therapeutic efficacy, improve patient compliance, minimize systemic side effects, and provide controlled drug release. Therefore, NLC-based delivery of boswellic acid could serve as an effective and safer alternative to conventional topical therapies for chronic psoriasis treatment
Psoriasis: Psoriasis is a chronic immune-mediated inflammatory skin condition linked to various morbidities, including psoriatic Arthritis and cardiovascular issues. Recognized by the World Health Organization in 2014 as a serious non-communicable disease, it is often associated with misdiagnosis, inadequate treatment, and stigma. Psoriasis is a chronic condition that impacts both the skin and joints, characterized by erythematous plaques with silvery scaling and a recurrent course. Histological features include epidermal hyperproliferation, elongated blood vessels, and lymphocytic infiltrate surrounding blood vessels. Recognized as an auto-immune disease, current therapies focus on the skin immune system, which plays a crucial role in its pathogenesis. [1]
Etiology: Psoriasis is a chronic autoimmune and inflammatory skin disorder caused by a combination of genetic, immunological, and environmental factors. The causes of psoriasis are complex, with genetics playing a key role, especially in early onset plaque psoriasis. Studies show that heritability is between 60% and 90%, and over 60 susceptibility sites have been found. Important genes involved include those related to immune response and skin barrier function. The interaction between T cells, dendritic cells, and keratinocytes drives inflammation and skin cell growth, especially through the IL 23/Th17 pathway. Environmental factors like obesity, stress, certain medications, and smoking can worsen psoriasis. [2],[3]
Causing Function: Psoriasis is a chronic immune-mediated inflammatory skin disorder caused by abnormal activation of the immune system, particularly T-lymphocytes, which mistakenly attack healthy skin cells. This immune response releases inflammatory cytokines such as TNF-α, IL-17, and IL-23, leading to excessive inflammation and rapid proliferation of keratinocytes. As a result, skin cells mature and accumulate on the skin surface within a few days instead of the normal 28–30-day cycle, causing thick, red, scaly plaques. Increased blood vessel formation and persistent inflammation further contribute to redness, itching, and skin thickening associated with psoriasis. [4],[5],[6]
Treatments: Treatment of psoriasis aims to reduce inflammation, control excessive skin cell proliferation, relieve symptoms, and improve quality of life. Depending on disease severity, treatment includes topical therapies such as corticosteroids, vitamin D analogs, retinoids, coal tar, and moisturizers for mild psoriasis, while moderate to severe cases may require phototherapy, systemic drugs like methotrexate and cyclosporine, or biologic agents targeting inflammatory cytokines such as TNF-α, IL-17, and IL-23. Recently, nanocarrier-based topical delivery systems, including nanostructured lipid carriers (NLCs), have gained attention for enhancing drug penetration, controlled release, and therapeutic efficacy with reduced side effects. [7]
Available Medicines/Methods: Psoriasis can be treated using topical medicines, systemic medicines, phototherapy, and lifestyle management depending on severity. For mild to moderate psoriasis, doctors commonly prescribe topical corticosteroids (such as hydrocortisone, betamethasone, clobetasol), vitamin D analogues (calcipotriol, calcitriol), topical retinoids (tazarotene), coal tar preparations, salicylic acid, and moisturizers/emollients to reduce scaling and dryness. For moderate to severe cases, systemic medicines like methotrexate, cyclosporine, and acitretin are used, along with newer oral drugs such as apremilast. In severe psoriasis and psoriatic arthritis, highly effective biologic drugs are available, including TNF-alpha inhibitors (adalimumab, infliximab, etanercept), IL-17 inhibitors (secukinumab, ixekizumab), and IL-23/IL-12 inhibitors (ustekinumab). Another effective method is phototherapy, especially narrowband UVB and PUVA therapy, which helps slow skin cell growth. Along with medicines, supportive methods like stress control, avoiding smoking and alcohol, maintaining healthy weight, regular moisturizing, and avoiding skin injury or infections help reduce flare-ups and improve long-term control. [8]
Types of Psoriasis:

Fig.: 1.1 Plaque psoriasis

Fig.: 1.2 Inverse Psoriasis

Fig.: 1.3 Guttate Psoriasis

Fig.: 1.4 Pustular Psoriasis

Fig.: 1.5 Nail Psoriasis
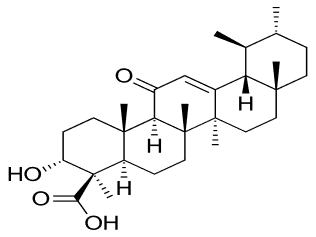
Drug Profile: Boswellic acid is a naturally occurring pentacyclic triterpenoid compound obtained mainly from the resin (gum) of the plant Boswellia serrata (Indian frankincense). It is widely used in traditional medicine and modern herbal formulations due to its anti-inflammatory, anti-arthritic, and immunomodulatory properties. Boswellic acid works mainly by inhibiting 5-lipoxygenase (5-LOX) enzyme, which reduces the formation of inflammatory leukotrienes. It also helps in reducing inflammation by inhibiting pro-inflammatory cytokines like TNF-α, IL-1β, and IL-6, and may reduce oxidative stress. Because of this mechanism, it is useful in chronic inflammatory conditions.[9],[10]


Fig.: 1.6 Boswellia Serrata
Chemical Structure: acetyl-keto-beta-boswellic acid (AKBA)
AKBA 3D Structure
Nanostructured Lipid Carriers (NLCs): Nanostructured lipid carriers (NLCs) are advanced lipid-based nanocarriers composed of a mixture of solid and liquid lipids, offering advantages such as improved drug loading, controlled release, enhanced skin permeation, and better stability. Therefore, the development and evaluation of NLCs for the topical delivery of boswellic acid represent a promising strategy to enhance its therapeutic efficacy and provide an effective and safer approach for the management of psoriasis.[2],[22]
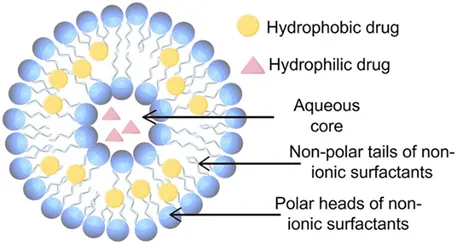
Fig.: 1.7 NLCs
Types of Nanostructured Lipid Carriers (NLCs):
Methods: The formulation process involves hot homogenization techniques. Initially, the lipid phase, containing the drug, was heated to a temperature exceeding the melting point of the lipids. Simultaneously, the aqueous phase, which included a surfactant and a co-surfactant, was also heated to this same temperature. The next step involved the gradual addition of the aqueous phase into the lipid phase while maintaining continuous stirring, resulting in the formation of a coarse emulsion. The optimized nanosystem was effectively integrated into a gel base formulated with Carbopol 934, which was initially dispersed in distilled water and hydrated overnight. Careful incorporation of the nanosystem was performed with continuous stirring to ensure uniformity, followed by pH adjustment to achieve a skin compatible range of 5.5 to 6.5, resulting in a homogeneous nano-gel.[18],[19]
Evaluations:
METHOD AND MATERIALS
Plant Profile: Boswellic Acid used as a novel topical carriers, derived from Boswellia serrata,(Family: Burseraceae) has demonstrated potent anti-inflammatory and anti-psoriatic activity by inhibiting inflammatory mediators such as leukotrienes. However, its poor aqueous solubility and limited skin penetration restrict its clinical application in topical therapy. [11],[12]
Botanical Profile: Boswellia Serrata (Indian Frankincense)
Family: Burseraceae
Part used: Oleogum resin extracted from the bark
Genus: Boswellia
Species: B. serrata
Kingdom: Plantae
Class: Anacardiales
Active Constituents: Alpha-boswellic acid and beta-boswellic acid, Essential oils, Polysaccharides.
Excipients: Excipients included solid lipids (e.g., stearic acid), liquid lipids (e.g., oleic acid), surfactants (e.g., Tween 80), co-surfactants (e.g., propylene glycol), gelling agents (e.g., Carbopol 934 or HPMC), preservatives (e.g., methyl paraben), and penetration enhancers were applicable. All chemicals and reagents used were of analytical grade and procured from approved suppliers.[17]
Method of Preparation: The formulation process involves hot homogenization techniques. Initially, the lipid phase (stearic acid, oleic acid), containing the drug (Boswellic acid), was heated to a temperature exceeding the melting point of the lipids. Simultaneously, the aqueous phase (Tween 80, propylene glycol), which included a surfactant and a co-surfactant, was also heated to this same temperature. The next step involved the gradual addition of the aqueous phase into the lipid phase while maintaining continuous stirring, resulting in the formation of a coarse emulsion.
Incorporate into gel base: The optimized nanosystem was effectively integrated into a gel base formulated with Carbopol 934, which was initially dispersed in distilled water and hydrated overnight. Careful incorporation of the nanosystem was performed with continuous stirring to ensure uniformity, followed by pH adjustment to achieve skin compatible range of 5.5 to 6.5, resulting in a homogeneous nano-gel. [23],[24],[25]
Evaluation Parameters:
RESULT
CONCLUSION
The study demonstrates that nanostructured lipid carriers (NLCs) are an effective system for the topical delivery of Boswellic Acid. The developed formulation improves drug solubility, stability, and skin penetration, resulting in enhanced therapeutic efficacy in the management of Psoriasis
DISCUSSION
REFERENCES

Chhatrapal Chandravanshi, Dr. Deepesh Lall, Dr. Ritesh Jain, Systematic Study of Psoriasis Treatment Using Boswellic Acid-Loaded Novel Nanostructured Lipid Carriers (NLCs), Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6372-6380, https://doi.org/10.5281/zenodo.20844921
 10.5281/zenodo.20844921
10.5281/zenodo.20844921