
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Arunai college of Pharmacy, Tiruvannamalai, Tamil Nadu 606603
Diabetic retinopathy (DR) is a common microvascular complication of diabetes mellitus and is the leading cause of visual loss in the elderly. Hyperglycaemia and altered metabolic pathways lead to oxidative stress and the development of neurodegeneration in the initial stage of diabetic retinopathy. Diabetic retinopathy (DR) remains a leading cause of vision loss among adults with diabetes, necessitating a multifaceted approach to management. Current treatment strategies are tailored to disease severity and include strict metabolic control, intravitreal anti-VEGF injections, corticosteroid implants, laser photocoagulation, and surgical interventions such as vitrectomy for advanced cases. Despite availability of effective screening and treatment, patients often present late due to poor awareness and practices. Effective prevention relies heavily on patient awareness and adherence to regular ophthalmological screening, making the assessment of patient knowledge, attitudes, and practices a critical step in identifying barriers to care. This study aimed to assess the Knowledge, Attitude, and Practice (KAP) concerning diabetic retinopathy among a cohort of diabetic patients to identify gaps in patient education and preventative care, among diabetes mellitus outpatients at a primary health centre. A cross-sectional survey was conducted among 300 diabetic individuals (71.3% rural, 81.1% Type 2 diabetes). The results revealed significant knowledge deficits: only 42.5% of respondents had heard of DR, and a mere 26.8% could identify its correct cause. A majority (71.3%) were unaware that DR could be prevented or treated. Despite this, attitudes were largely positive, with 81.9% agreeing that DR is a serious complication and over 85?knowledging the importance of early detection. A striking attitude-practice gap was identified; while most endorsed the need for annual eye exams, 70.1% had never undergone a retinal screening (fundus examination), and 66.5% reported never visiting an eye doctor. This poor adherence to eye care contrasts sharply with high self-reported adherence to daily diabetes. Management, such as regular blood sugar monitoring (88.2%). Furthermore, 72.8% of participants reported never having received counseling on DR from a healthcare professional, suggesting a critical lapse in patient education.
EPIDEMIOLOGY
The economic burden of vision impairment and blindness due to diabetic retinopathy in globally is considerable. A global study in 2017 found that of the leading causes of vision impairment and blindness, the crude global prevalence (all ages) of diabetic retinopathy as a cause increased between 1990 and 2015, while more than460 million people live with diabetes, and this number is expected to rise to 700 million by 2045. Approximately one-third of individuals with diabetes have signs of DR, and about one in fifteen have vision-threating disease (proliferative DR or DME).
In India
A recent study from an urban population in Chennai, India estimated the age-standardised. The incidence VT-DR was higher (10.2%) among those who had diabetes for ≥15 years compared with those with 0–4 year’s duration (2%). Progression was associated with poor glycaemic control, systolic hypertension and anaemia.
CLINICAL FEATURES
DIABETIC MACULAR EDEMA (DME) retinal thickening and hard exudates near the macula, leading to central vision loss.
MICROANEURYSS (MA) small, balloon-like bulges in the tiny blood vessels of the retina.
NEOVASCULARIZATION (NV) The growth of new, abnormal blood vessel in the retina, a hallmark of proliferative diabetic retinopathy
SYMPTOMS
DR is characterized by blurred or fluctuating vision, Floaters, Dark or empty areas in vision, Poor night vision, Faded or washed-out colour, sudden vision loss. (Figure 1: symptoms)

Figure 1: SYMPTOMS
RISK FACTORS
The development of diabetic retinopathy Strongly correlates with a longer duration of diabetes, greater hyperglycemia, and hypertension. Other factors such as High cholesterol and triglycerides, Male sex, Older age, Diabetic neuropathy, Nephropathy, Foot ulcers, Smoking, Anemia, Pregnancy, Family history, High salt intake, Glilatzone drugs.
LEVEL OF AWARENESS OF DIABETIC RETINOPATHY AMONG PATIENT, PROVIDERS IN INDIA
In India, levels of awareness about DR amongst DM in terms of their knowledge and the importance of annual eye examinations is low. Awareness amongst health care professionals is also not as good. There is limited evidence of the availability of services for patients with DR.
STAGES OF DIABETIC RETINOPATHY
This Classification system based on the ETDRS (Early Treatment Diabetic Retinopathy Study Research Group) can be found in the International Council of Ophthalmology (ICO) guidelines for diabetes eye care (International Council of Ophthalmology, 2017; Wong et al., 2018).
DR is divided into two broad stages: Non-proliferative DR (NPDR) and Proliferative DR (PDR). NPDR represents the earlier stages of the disease, characterized (progressively) by retinal Microaneurysm (MA), intra retinal hemorrhages, hard extrudes (HE), venous beading, and Intra microvascular Microaneurysms (IRMA)
PROLIFERATIVE DIABETIC RETIOPATHY (PDR):
Proliferative diabetic retinopathy (PDR) is the more advanced form of the disease, which is characterized by abnormal blood vessel growth (neovasculation) on the retina or optic disc.
NON-PROLIFERATIVE DIABETIC RETINOPATHY (NPDR):
Non-Proliferative diabetic retinopathy is further charaterizsed by three stages:
1. Mild NPDR: Characterized by microaneurysms
2. Moderate NPDR: Involves more microaneurysms, haemorrhages, cotton-wool spots and hard exudates.
3. Severe NPDR: Definite by the “4-2-1 rule”
PATHOPHYSIOLOGY
The various metabolic mechanisms, pathologic processes, and systemic comorbidities involved in the development and progression of DR each provide important targets for disease-modifying therapeutics
As a complication of diabetes mellitus, hyperglycemia is one of the essential contributions to DR development. Several underlying mechanisms of elevated blood glucose leads to DR are identified, including the hexosamine pathway, advanced glycation end products accumulation, polyol pathway, protein kinase C pathway and poly polymerase activation.The metabolic dysregulations, together with oxidative and inflammatory imbalance, lead to the pathological presentation of DR. (figure 2: pathology of diabetic retinopathy)
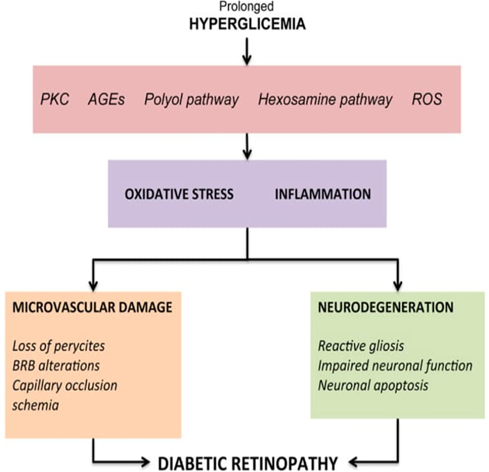
Figure 2: PATHOLOGY OF DIABETIC RETINOPATHY
Inflammation is also documented as a key component of DR pathogenesis via capillary damage and hypoxia induction, leading to increased VEGF expression and Neovascularization. Finally, endothelial proliferation driven by chronic microvascular ischemia results in the formation of visible intraretinal microvascular abnormalities (IRMA) and neovascularization (NV), with consequent vision-threatening complications such as Vitreous hemorrhage (VH) and tractional retinal detachment (TRD).
DIAGNOSIS OF DIABETIC RETINOPATHY
Early detection of DR is critical, as the disease is often asymptomatic in its initial stages and vision loss can be prevented or minimized with timely intervention. DR often develops without symptoms in its early stages. Vision loss typically occurs only when the disease has advanced or when complications such as diabetic macular edema (DME) or proliferative diabetic retinopathy (PDR) arise.
SCREENING RECOMMENDATIONS
DIAGNOSITC TOOLS USED IN DIABETIC RETINOPATHY
A variety of diagnostic tools and imaging modalities are used to identify, monitor, and guide the treatment of DR.
Emerging Technologies
II. MANAGEMENT OF DIABETIC RETINOPATHY
1. MEDICAL MANAGEMENT
Effective management of DR begins with optimizing systemic health
2. OPHTHALMIC TREATMENT
3. INTRAVITREAL INJECTIONS
DR. Agents: Ranibizumab, Aflibercept, Bevacizumab, Brolucizumab. Reduce vascular leakage, neovascularization, and improve visual acuity.
Drugs: Dexamethasone (Ozurdex), Fluocinolone (Retisert), Triamcinolone. Suppress inflammation, VEGF expression, and reduce oedema.
4. SURGICAL OPTIONS
Success rates: Anatomical (90–95%), visual improvement (60–80%).
5. EMERGING THERAPIES
III. OBJECTIVES
General Objective: To assess the knowledge, attitude, and practice regarding diabetic retinopathy among patients with diabetes mellitus.
Specific Objectives:
IV. MATERIALS AND METHODS
STUDY DESIGN: Cross-sectional descriptive study, Questionnaire-based KAP survey
STUDY SETTING AND DURATION: Conducted at
STUDY POPULATION:
Patients aged ≥18 years with a confirmed diagnosis of type 1 or type 2 diabetes mellitus attending the outpatient clinic.
SAMPLE SIZE AND SAMPLING METHOD:
A total of 300 participants were selected using simple random sampling, based on a 95% confidence level and 5% margin of error.
INCLUSION CRITERIA:
Adults (≥18 years) with type 1 or type 2 diabetes. Willing to provide informed consent.
EXCLUSION CRITERIA:
Patients with cognitive impairment or severe illness. Individuals unable to communicate effectively.
DATA COLLECTION TOOL:
A structured, pre-tested questionnaire divided into four sections:
DATA COLLECTION PROCEDURE:
Face-to-face interviews conducted in the local language by trained data collectors after obtaining written informed consent. Each interview lasted 10–15 minutes.
DATA ANALYSIS:
V. RESULTS
The study's findings reveal significant gaps in the knowledge and practices of diabetic patients regarding diabetic retinopathy (DR), despite a generally positive attitude towards eye care.
SOCIO-DEMOGRAPHIC CHARACTERISTICS
The study included 300 diabetic patients. The majority of participants (55%) were between 40 and 60 years of age
KNOWLEDGE ASSESSMENT:
Overall knowledge about the specifics of diabetic retinopathy was found to be low, with a high frequency of "don't know" answers.
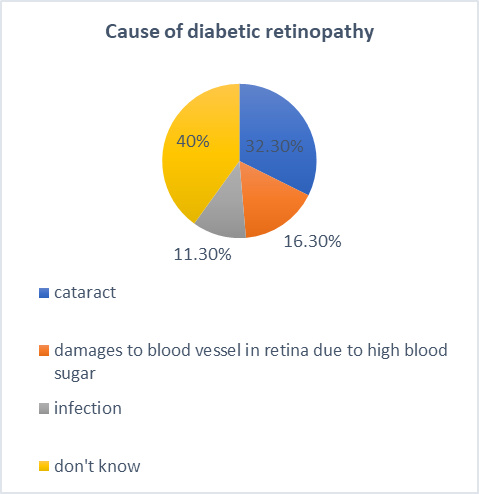
Figure 3: CHART REPRESENTATION
ATTITUDE ASSESSMENT:
Respondents generally displayed a positive and concerned attitude towards diabetic retinopathy, even when their specific knowledge was lacking.
?3.1% agree that visiting an ophthalmologist is necessary for all diabetic patients.
?70.1% believe a yearly eye examination is necessary.
PRACTICE ASSESSMENT:
Despite positive attitudes, the self-reported practices for preventing and screening for DR were alarmingly poor. This indicates a significant gap between belief and action.
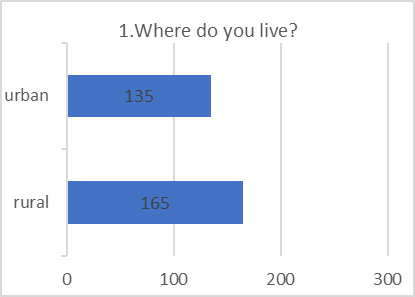
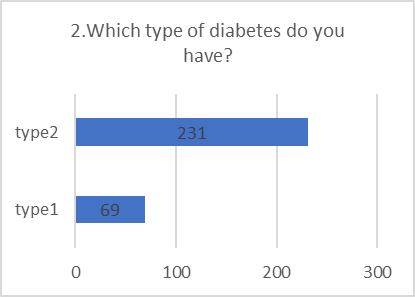
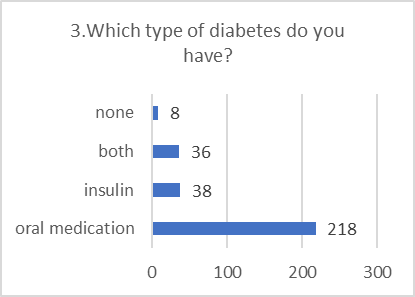
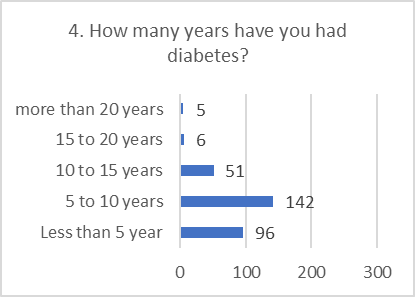
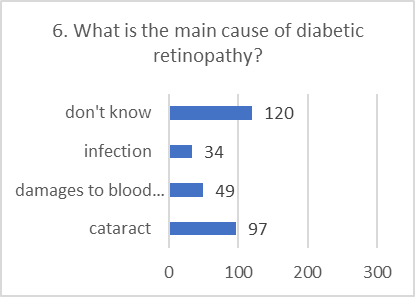
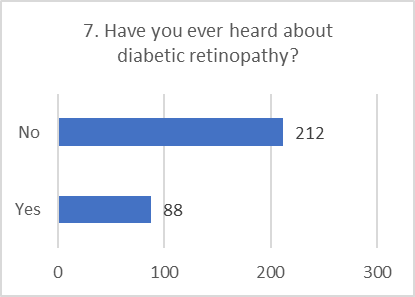
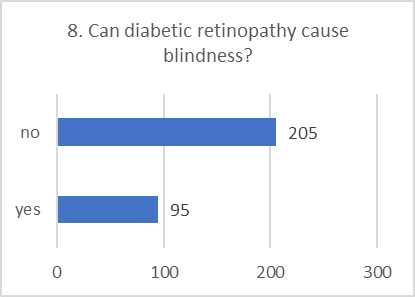
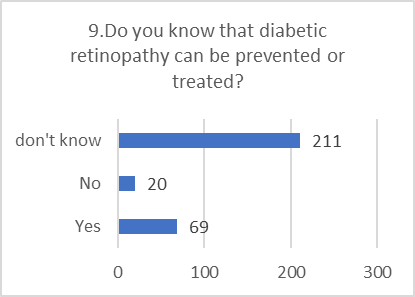
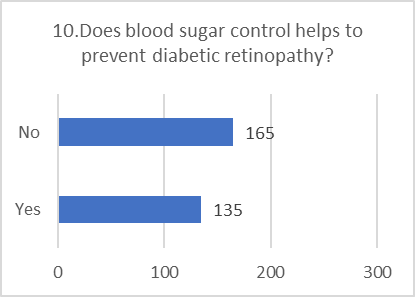
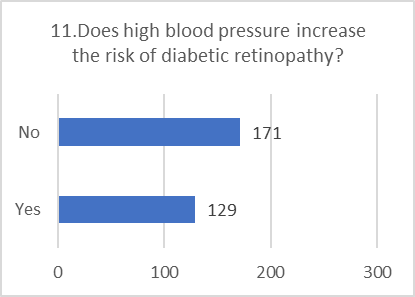
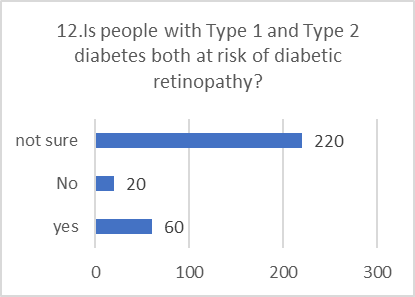
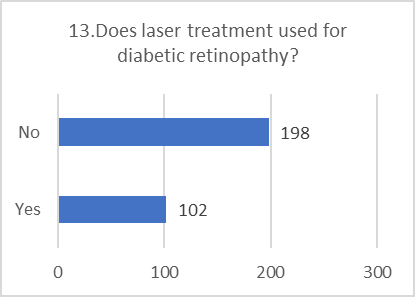
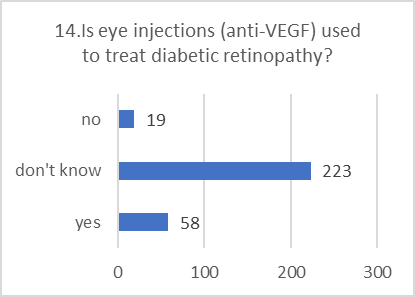
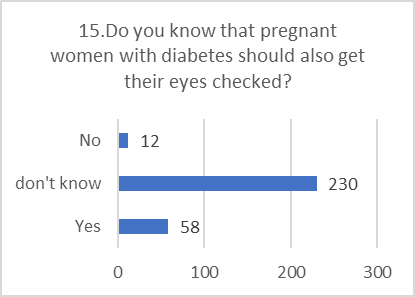
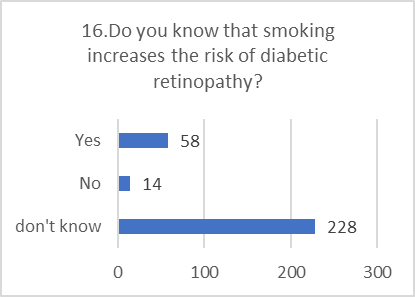
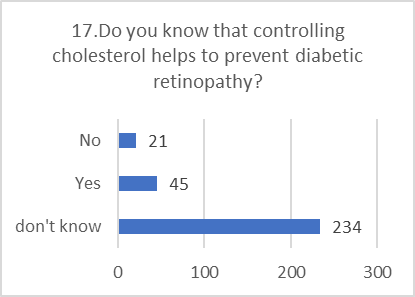
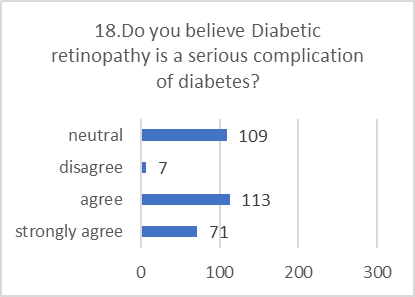
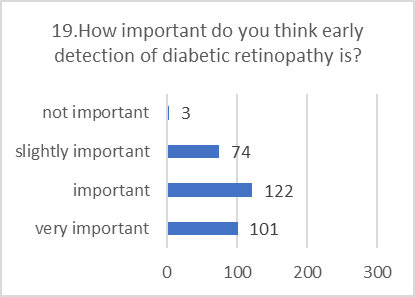
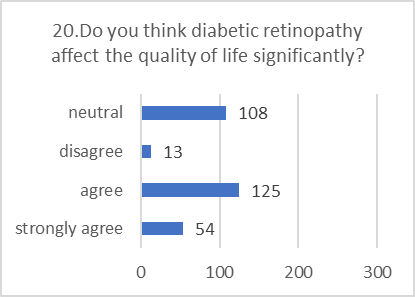
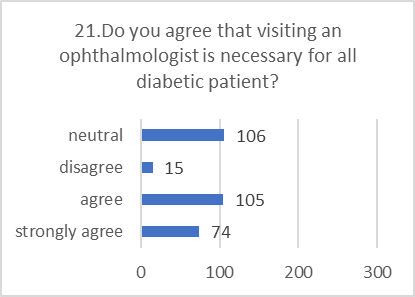
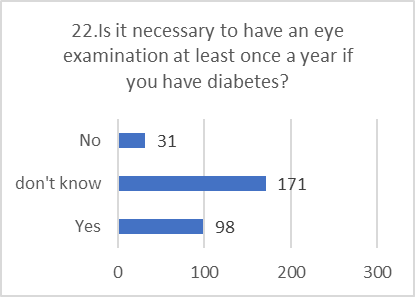
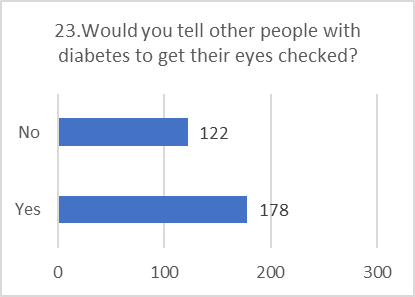
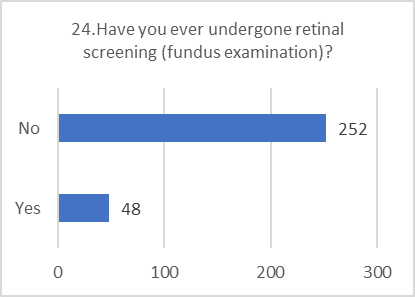
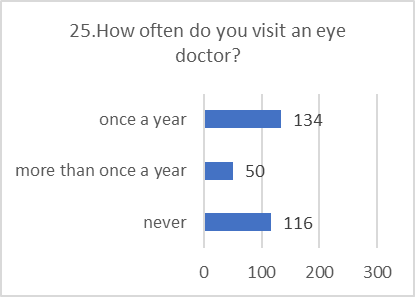
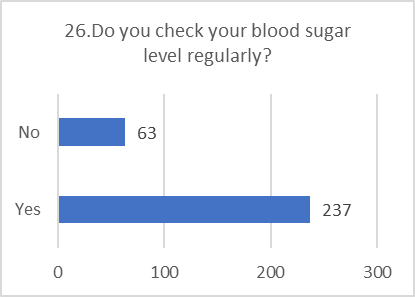
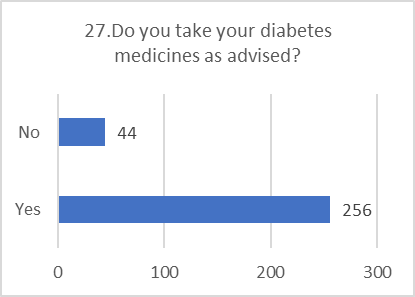
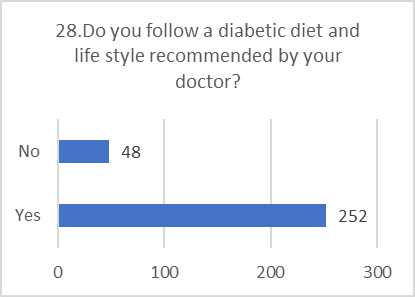
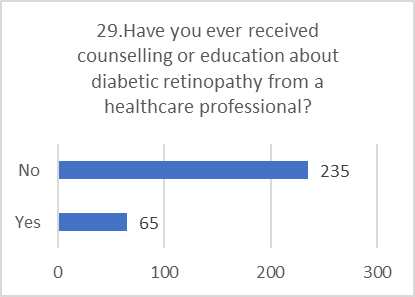
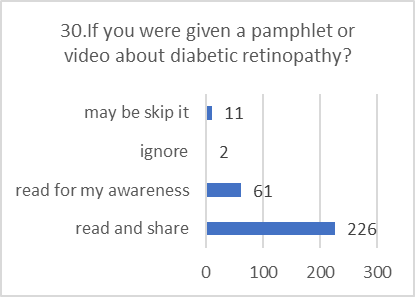
Figure 5: CHART REPRESENTATION
VI. DISCUSSION
The study reveals a critical disconnect in patient care for diabetic retinopathy. While patients demonstrate responsible behavior in managing their daily blood sugar, diet, and medication, they largely neglect the specific, sight-threatening complication of DR.
The Knowledge-Practice Deficit
The most significant finding is the wide gap between what patients believe and what they do. A vast majority agrees that DR is serious and that yearly eye exams are necessary. However, an almost identical majority has never had a retinal screening and never visits an eye doctor. This suggests that the primary barrier is not a lack of concern, but a combination of other factors.
Even among those who have "heard" of DR, specific knowledge is severely lacking. Most could not identify the correct cause, and the majority were unaware that controlling blood sugar helps prevent it. This indicates that awareness is superficial. Patients may have heard the term but do not understand the mechanism, the asymptomatic nature of early stages, or the direct link between their daily diabetes management and saving their sight.
?The Critical Role of Healthcare Providers
?The fact that nearly three-quarters of respondents have never been educated about DR by a healthcare professional is a major red flag. This points to a potential systemic failure in patient education. Patients are diligent in the practices their doctors emphasize (e.g., blood sugar checks, medication). The lack of practice in eye care is likely a direct reflection of a lack of emphasis and education from their healthcare providers.
VII. CONCLUSION
This study highlights a population of diabetic patients who are diligent in their general disease management but critically deficient in their knowledge and practice related to diabetic retinopathy. Their positive attitude and concern are not translating into the essential preventative action of regular eye screenings. This inaction is strongly associated with a lack of specific knowledge and a failure of the healthcare system to provide targeted education on this complication. There is an urgent need for targeted interventions to bridge this gap and improve eye care practices among individuals with diabetes.
VIII. LIMITATIONS
The study has certain limitations that should be considered when interpreting the results:
IX. RECOMMENDATIONS
Based on the study's conclusions, the following recommendations are proposed to reduce the burden of blindness from diabetic retinopathy:
Targeted Public Health Campaigns: Campaigns are needed, especially in rural areas, to move beyond simple awareness. They must clearly explain why annual screenings are essential even when vision is good and directly link blood sugar control to eye health.
REFERENCES


P. Praveen Kumar, S. K. Senthil Kumar, S. Tamil Priya, V. Tamilarasan, S. Thamizharasi, K. Vaishnudevi, A Cross-Sectional Kap Study on Diabetic Retinopathy and its Treatment Among Diabetic Mellitus Patients, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 3695-3711. https://doi.org/10.5281/zenodo.17235897
 10.5281/zenodo.17235897
10.5281/zenodo.17235897