
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Yashodeep Institute of Pharmacy Chh. Sambhajinagar.
This study aimed to develop and characterize a topical gel formulation of Calotropis gigantea extract for the treatment of arthritis. The gel was prepared using a combination of polymers and evaluated for its physicochemical properties, stability, and anti-arthritic activity. The results showed that the gel formulation had suitable viscosity, pH, and spreadability, and exhibited significant anti-inflammatory and analgesic activity in animal models. The gel also showed sustained release of the active compounds, indicating its potential for prolonged therapeutic effect. The study suggests that the Calotropis gigantea gel formulation may be a promising alternative for the topical treatment of arthritis.
Dosage forms, also known as unit doses, are pharmaceutical drug products in the form in which they are marketed for use. They consist of aspecific combination of inactive ingredients andactive ingredients, or excipients, apportioned into a specific dose and in a particular configuration, like a capsule shell. Sometimes, the word "dosage form" refers only to the pharmaceutical formulation of the active ingredient in a drug product and any mixes that are used; it does not take into account other factors, such as how the product is eventually designed to be consumed, like a capsule, patch, etc. It is frequently advisable to exercise caution when speaking with someone who might not be familiar with another person's use of the phrase due to the relatively hazy limits and ambiguous overlap of these terms, as well as various variants and qualifiers within the pharmaceutical industry.
Depending on the routes of administration, dosage forms come in several types. The dosage form includes the liquid dosage form, solid dosage form, and semisolid dosage forms. The common dosage forms include pills, tablets, capsule, syrup.
A combination of knowledge in formulations, stability, dissolution, and controlled release (pharmaceutics); absorption, distribution, metabolism, and excretion (pharmacokinetics); concentration-effect relationships and drug-receptor interaction (pharmacodynamics); and treatments of the disease state (pharmacotherapeutics) is used in the creation of dosage forms within the field of biopharmaceutics[1].
To achieve clinical efficacy and safety, medication dosage optimization is also essential. A pharmacokinetic-pharmacodynamic model that characterizes the drug response is becoming more and more the cornerstone of dose optimization. The idea that a drug's receptors and free drug inthe systemic circulation are in balance connects pharmacokinetics and pharmacodynamics. Pharmacodynamics explains how a medication interacts with a receptor to cause events that are postreceptor-related and ultimately result in a pharmacological effect[1].
The dosage form determines the route of administration for drug delivery. Different dosage forms could be available for a same medication since certain medical
Conditions, such unconsciousness, canl imit the route of administration. Forinstance, nausea might make it difficult to take a medication orally, especially when combined with vomiting. In this situation, a different route such as inhalation, buccal, sublingual, nasal, suppository, or parenteral topical medication may be required. Furthermore, certain types of medications may need a particular dosage form due to problems with pharmacokinetics or chemical stability, among other things.
Topical administration is utilized for transdermal distribution of medicinal substances, externaland internal parasite control, and localized skin treatment. Drugs used topically for localized effects include skin emollients, antifungals, antiseptics, and anti-inflammatory drugs. The semisolid base thatisutilized primarily determines the rate of drug release from ointments, creams, and pastes[1].
In order to nourish and shield the skin from damage, topical medicine is another option. Some topical drugs are applied locally, while others are intended to take effect throughout the body after being absorbed via the skin[2].
Topical formulations are composed of a base, or vehicle, that may be tailored to a specific body part or skin type. The purpose of the product's design could be to maximize the penetration of an active ingredient—typically a medication—throughout the skin or to providemoisture[3].
a. Gel:
The formulation for the topical medication includes pastes, ointments, oils, creams, lotions, eye drops, ear drops, foams, tinctures, powders, sprays, patches, and gels
Gels are a unique kind of water-based cream. Their main constituents are thickeners, such as starch, which have the ability to bind large amounts of water and dissolve active chemicals. Gels are fatfree, readily applied to the skin, and can include a variety of active substances. For instance, thereare gels that reduce pain or that contain anti-itchingingredients. Dueto water evaporatingon the skin, gels form a film on the skin and chill the area[3].
Semisolid formulations called gels are meant to be applied to the skin or to mucosal membranes that are accessible, such as the oral cavity. Gels consist of two interpenetrating systems in which the colloidal particles, called gallant or gelator, are uniformly distributed in a solvent or dispersion media to form a three-dimensional matrix called the gels[4].
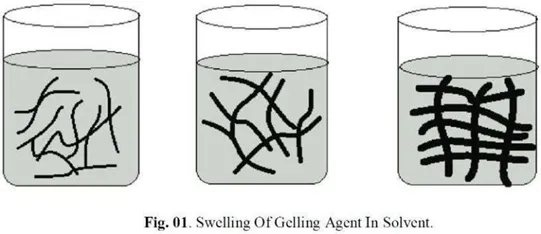
A gelling agent (gelator), which can be a low molecular weight small molecule or a natural, synthetic, or semi-synthetic polymer, is added to an organic, inorganic, or aqueous solvent or solvent systems to form the gels (fig. 1). In gels, the polymer serves as the gel matrix's structural support. The structural strength, enhanced adhesion to the surface, and lower permeability of bigger molecules are all attributed to the polymeric meshwork of gel, which also enables retention.
Gels can be irreversible or reversible depending on the kind of bonding used. Reversible gels typically have hydrogen bonds, while irreversible gels typically have covalent bonds. A gel can exhibit two distinct phases: a single phase with no obvious boundaries or a two phase system with discrete particle floccules[4]
4.2.Properties of Gels
There are various important properties associated with gels. Some of the key properties are as follows [5]:
1. Safety and Inertness:
The gelling agent should ideally be safe, chemically inert, and non-reactive with other ingredients in the formulation.
2. Solid-State Behavior:
Gelsexhibitcharacteristicsofthesolidstateduetotheirinternalstructuralnetwork.
3. Phase Attraction:
There is a strong attraction between the aqueous medium and the dispersion phase, which prevents the gel from settling and helps maintain uniformity over time.
4. Response to Shear Forces:
The gelling agent should provide a noticeable solid-like consistency during storage, which easily breaks down when shear forces are applied—such as squeezing a tube, shaking a bottle, or topical application.
5. Non-Stickiness:
Topical gels must not be sticky upon application to ensure comfort and better patient compliance.
6. System Uniformity:
All the components within the gel system should remain constant and evenly distributed throughout.
7. Viscosity and Temperature Sensitivity:
The apparent viscosity or gel strength increases with the effective crosslink density of the gel. However, this viscosity may vary with temperature, depending on molecular interactions between the solvent and the polymer.
8. Antimicrobial Protection:
An appropriate antimicrobial agent must be included in the formulation to ensure product safety during use.
9. Sterility for Ophthalmic Use:
Eyegels,inparticular,mustbesteriletopreventinfectionorirritationuponapplication.
Formulation Of Gels
Gel development by achieving a balance between the polymer and the solvent, a geliscreated. The gel, often referred to as the gelling point, is produced at a critical concentration; viscosity grows significantly above this point, while gel cannot form below it. The hydrophilic and lipophilic balance of the polymer, the solvent and polymer interaction, the structure's homogeneity, the polymer's molecular weight, and the polymer chain's flexibility can all be used to calculate the gelling point. There is a direct proportionality between the gelling point and the flexibility. Solvents with different affinities for that polymer can raise or lower the gelling point.
For certain gels to develop, temperature must be adjusted. The basic process for their production involves heating the liquid, adding the polymer, thoroughly mixing it, and then allowing it to cool down for settling. As opposed to this approach, some gels should not be heated because doing so will cause the bonds to break (such as hydrogen bonds).
Flocculation is an additional method for gel formulation. This can be accomplished by producing the gel by adding salts to the lipophilic solutions. One instance of this kind of interaction involves theuseofmineraloilandfumedsilicatocreateagelthroughhydrogenbondingbetweenindividual particles. Another illustration would be the creation of a homogenous gel by forcefully mixing benzene and ethyl cellulose. Additionally, it was noted that the presence of electrolyte causes rheological alterations that lead to the gel's development. Examples of these are the hydroxides of iron and magnesium and the NA+–montmorillonite clay of the smectite group (bentonite). Chemical reactions such as the treatment of titanium with H202and 0.1m HCLcan also be used to make gels. The surface of titanium becomes gelled as a result of this reaction, and the thickness of the gel layer increases as the surface concentration of H2O2and 0.1 m hcl Solution Increase.
Advantages of Gel Formulations
The following are some of the main benefits or advantages that gel formulations have over other semisolid dosage forms [3][6]:
• Gels are utilized as the best possible cutaneous and percutaneous medication administration.
•Formulatinggelsissimplerthancreatingothersemisoliddoseforms.
• They can prevent gastrointestinal pH-related issues with medicine absorption in the gastrointestinal tract.
•Duetosolventevaporation,theyhavegoodspreadabilityandcoolingeffects.
•Comparedtoothertopicaldoseforms,gelshavealongerretentionperiod.
• Agelisasophisticated,non-greasymixture.
• Theyarebiodegradableandbiocompatible.
• Theyarenaturallyharmlessandwashable.
• Theirlong-termstabilityproblemsaresignificantlylesssevere.
•Theyaresuitableforgivingbothpolarandnon-polarmedications.
• In cases where oral medicine administration is not appropriate, they might serve as a substitute.
•Theycantoleratecertainstressfulsituationsratherwell.
• They can be used as controlled release formulations by entwining the polymer more than once.
•Gelshavestrongadhesionqualitiestotheapplicationsite.
• They provideabarrierthatshieldstheapplicationplace
• Gels have the property to avoid enzymatic activity and drug interaction with food and drinks.
•Theycanescapesystemicandportalcirculationaftergastrointestinalabsorption.
• They can prevent the first-pass effect, which is the first time a pharmacological substance passes through the human body.
• Sincetheliver isbypassed,gelsarenotdestroyedbyliverenzymes.
• Patientscomplywiththemastheyarenon-invasive.
• They are applied topically to the skin for aprotracted, gradual absorption.
• In pharmacies, gels have also been used to apply viscous suspensions for oral use, such as aluminium hydroxide gel. • They have minimal adverse effects and a confined effect.
Disadvantages/LimitationsofGelFormulations
Gel formulations have some benefits, but they can also have certain drawbacks or restrictions [3][6]:
• Certain gels include covalent connections that make them indestructible, enclosing the medication within the gel matrix.
•Evaporationoftheformulation'ssolventmightcausethegeltodry.
• Rheology of certain gels may change as a result of changes in humidity, temperature, and other environmental conditions.
• The inclusion of polymers in gel formulation may cause certain medications to deteriorate.
• Therecouldbeanallergicreactiontogels.
•Precipitationofthegellingagentsmaycausesaltingout.
•Gelmedicationmaybedenaturedbyanenzymeintheepidermis.
•Drugswithbiggerparticlesdon'tpassthroughtheskinandabsorb.
• Gelshavealonger-lasting,relativelyslowereffect.
• Irritationmay becausedby thegelatorsortheadditives.
• Thewatercontentmay increasethechancesofmicrobialorfungalattackingels.
• Gels may experience syneresis, or the evacuation of solvent from the gel matrix, while being stored.
•Incertaingels,flocculationmightresultinanunstablegel.
• Sterilizationisnecessaryforgelsthatare insertedintothebody ortheeyes.
•Somemedicationsarenotwellabsorbedviatheskin,i.e.,theyhavepoorpermeability.
•Duringapplication,gelscouldresultinskinallergies.
•Carefulselectionoftheareatobeevaluatedbeforeapplyinggelsisnecessary.
•Sideeffectsfromapplicationscouldresultfromgels.
Gel Uses
Therearevarioususesofgels.Someofthecommonusesareasfollows[7]:
•Phosphategelandsodiumfluoridegelareusedfor preventativetoothcare.
• Lubricantforcatheters.
• Baseforpatchtests.
• Forelectrocardiogram,NaClgelisused.
• Binders are used in granulation of tablets, in suspensions for protective colloids, and in oral liquids as thickeners.
• Used in cosmetic products such as perfumes, dentifrices, shampoos, and preparations for skin and hair care.
• Along-actingmedicationthatisimplantedinthebody orinjectedintoamuscle.
• Gel formulations that are external and meant to be applied directly to the skin, mucous membranes, or eyes.
•Gelcanbeusedasanoraldrugdeliverysystem.
3. METHOD AND MATERIAL
Method
a. ExcipientsProfile
1. Carbopol 940 oRole: High molecular weight cross-linked polyacrylic acid polymer used in topical and cosmetic formulations. o Function: Acts as a thickening agent, stabilizer, and suspending agent. It provides viscosity, helps suspend particles, and stabilizes emulsions.
2.DisodiumEDTA(EthyleneDiamineTetraaceticAcid)o Role:Chelatingagent.o Function:Bindstometalions,preventingthemfromcatalyzingoxidativedegradationoftheformulation,thusactingasanantioxidantandenhancingformulation
stability.
3. Triethanolamine(98%)o Role:pHadjusterandneutralizingagent.o
Function: Neutralizes acidic polymers (e.g., Carbopol), forming salts that contribute to viscosity and adjusting the pH to optimize formulation stability.
4. Propylene Glycol o Role: Humectant and solvent. o Function: Retains moisture in the formulation and solubilizes active ingredients or excipients, enhancing skin penetration and formulation consistency.
5. Methyl Paraben o Role: Preservative. o Function: Exhibits antimicrobial activity against a range of bacteria and fungi, thereby preventing microbial contamination and extending shelf life.
6. Diclofenaco Role:ActivePharmaceuticalIngredient(API).o Function:Anonsteroidalanti-inflammatorydrug(NSAID)thatprovides analgesic,antipyretic,andanti-inflammatoryeffects.
7. SodiumChlorideo Role:Tonicity-adjustingagent.
o Function: Adjusts osmotic pressure to make the formulation isotonic with physiological fluids, minimizing irritation upon application.
8. Disodium Hydrogen Phosphate o Role: Buffering agent. o Function: Maintains the pH of the formulation within a desired range to ensure chemical stability and efficacy of active ingredients.
9. Potassium Hydroxide (Corrected name; sometimes incorrectly referred to as Potassium Dihydroxide)
o Role: Strong base and pH adjuster.
o Function: Used to raise pH levels of formulations, especially when neutralizing acidic components such as Carbopol.
b. Material used for the experimental work:
|
Sr.No. |
Material |
NameofCompany/Manufacturer |
|
1 |
Carbapol940 |
ResearchLabFineChem.Industries, Mumbai |
|
2 |
Di-sodiumEDTA |
ThomasBaker(Chemicals)Pvt.Ltd. |
|
3 |
Triethanolamine98% |
ThomasBaker(Chemicals)Pvt.Ltd. |
|
4 |
PropyleneGlycol |
ResearchLabFineChem.Industries,Mumbai |
|
5 |
MethylParaben |
ThomasBaker(Chemicals)Pvt.Ltd. |
|
6 |
Diclofenac |
ResearchLabFineChem.Industries,Mumbai |
|
7 |
SodiumChloride |
ResearchLabFineChem.Industries, Mumbai |
|
8 |
Di-sodiumHydroxidePhosphate |
ResearchLabFineChem.Industries,Mumbai |
|
9 |
PotassiumDihydroxide |
ThomasBaker(Chemicals)Pvt.Ltd. |
4. DRUG PROFILE
Calotropis Gigantea
The conventional medical field is regarded as the most reliable source for new drug discoveries. However, herbal treatments are gainingincreasing popularity worldwide. Nowadays, it is common to use herbal remedies either alone or alongside prescription medications to treat and manage various illnesses. Historically, plants have been a vital source for developing medicines for a wide range of ailments.
Herbal plants are used to promote and maintain health, prevent disease, and treat illnesses. The World Health Organization (WHO) encourages and promotes the practice of traditional medicine as long as it is proven to be safe and effective. Globally, approximately 80% of people rely on traditionalmedicinesforprimaryhealthcare,themajorityofwhichinvolveextractsfrommedicinal plants. Traditional medicine forms the core of alternative health care systems worldwide.
Previously, herbal remedies were administered based on the knowledge, experience, and skill of practitioners. In modern times, medication therapy depends more on demonstrated safety and effectiveness. Numerous recent studies document the use of herbal medicines for treating various diseases.
Since prehistoric times, plants and other natural products have profoundly influenced human ethnicity and civilization, including India. People have revered and utilized plants as natural resources for food, fuel, manure, fiber, and medicinal purposes.
One such significant plant is Calotropis Gigantea, known as one of the best shrubs for treating various ailments. Using herbs and plants has been aneconomical and natural methodtotre
moderateto serious illnesses. Most herbs area bundantin nature or canbe easilyand inexpensively cultivated.
Calotropis Gigantea is a common herb native to Asian countries that flourish extensively. It belongs to the Apocynaceae family and is also known by several names such as Shallow Wort, Gigantic Indian Milkweed, and Crown Flower. In India, it is often called Aak or Madar. The plant is widespread in India, Bangladesh, Indonesia, Malaysia, Sri Lanka, China, Pakistan, and Nepal.
InIndia, Calotropis plant sare found mainly in two types:
•Calotropis Gigantea: produces white flowers.
•Calotropis Procera: produces lavenderflowers.
Despite being considered potentially toxic, Calotropis has been used for generations in traditional Ayurvedic medicine for its remarkable healing properties. It is a key ingredient in many herbal formulations used to treat chronic health conditions.
The plant gets its name "Crown Flower" due to its five-petaled, white-lavender, crown-shaped flowers. Calotropis shrubs can grow between five to seven meters tall. Its stem exudes a milky latex, and the leaves are oval-shaped and light green.
Characteristics of Calotropis Gigantea

Calotropis Gigantea
Geographical Distribution
Calotropis Gigantea is widely available worldwide. It originates from India, China, and Malaysia, and is mainly found in South India, Lower Bengal, the Himalayas, Punjab, Assam, and Madras. It grows abundantly in waste areas, railway embankments, androadsideelevations upto1000meters in the Himalayas, from Punjab to Assam.The plant is also found in many countries across Asia, Africa, the Middle East, and parts of the Americas, including:
• Afghanistan, Algeria, Burkina Faso, Cameroon, Chad, Democratic Republic of Congo, Egypt, Eritrea, Ethiopia, Gambia, Ghana, Guinea-Bissau, India, Iran, Iraq, Israel, Kenya, Netherlands Antilles, Nicaragua, Panama, Paraguay, Peru, Puerto Rico, Kuwait, Lebanon, Libya, Mali, Mauritania, Morocco, Mozambique, Myanmar, Nepal, Niger, Nigeria, Oman, Pakistan, Saudi Arabia, Senegal, Sierra Leone, Barbados, Bolivia, Brazil, Chile, Colombia, Cuba, Dominica, Dominican Republic, Ecuador, French Guiana, Somalia, Sudan, Syria, Tanzania, Thailand, Uganda, United Arab Emirates, Vietnam, Yemen, Zimbabwe.
• Exotic locations include Saint Kitts and Nevis, St Lucia, St Vincent and the Grenadines, Surinam, Trinidad and Tobago, Uruguay, Venezuela, Virgin Islands, Grenada,Guadeloupe, Guatemala, Guyana, Haiti, Honduras, Jamaica, Martinique, Mexico, and Montserrat.
Morphology of the Plant
a) Macroscopic Characteristics:
• General Description:
Calotropis Gigantea is a well-branched, upright shrub or small tree, growing between 1 to6 meters tall. It thrives in tough, arid soils with moderate rainfall.
• Root System:
The plant has a robust root system with woody roots that are circular, cylindrical, circuitous, and repeatedly branching. The bark of the root system is fissured, corky, yellowish, and peels off regularly. The roots are 3–10 cm in diameter with a white interior. The bark is 2–4 mm thick, mucilaginous, and bitter in taste.
• StemandLeaves:
The stem exudes a milky latex. Leaves are oval, light yellowish-green (pale green),simple, subsessile, opposite decussate, and exstipulate.They measure 5to30cm in length and 2.5 to 16 cm in width, with sharp quadrilateral elliptic to broadly elliptic shapes. Leaf apex is edged and mucuronate (heart-shaped) at the base with apiculate tips. Leaves have white, short, tomentose petioles along the edges.
• Flowers:
Flowers are bracteate, actinomorphic (radially symmetrical), bisexual, and pentamerous (five petals). They are unscented with a delicate crown at the center housing the stamens. Flowers form multi-flowered peduncled cymes emerging from nodes at the terminal ends. The calyx is glabrescent, polysepalous, and quickly unites at the base. The corolla is twisted and gamopetalous (fused petals).
• Fruitand Seeds:
The fruit is subglobose, inflated, floppy, and simple. Seeds are tiny, flat, obovate, and have white silky pappus hairs around 3–4 cm long, which help them float freely in the air.
• Cultural Significance:
In India, the crown flower is used in Lord Shiva temples symbolizing harmony, peace, prosperity, and social stability.
b) Microscopic Characteristics:
• Root:
The cork layer is the uppermost, consisting of 15-20 rectangular cells with no intracellular spaces in transverse sections. Cortex cells have abundant starch granules. Parenchymatic cells are asymmetrical and irregular, containing laticiferous tubes and calcium oxalate crystals.
• Leaves:
Transverse sections reveal epidermal cells covered by a thick, striated, hard cuticle on both sides. The xylem mainly consists of tracheids and veins.
• Ecological Note:
The plantattractsa wide range of insects and butterflies.
Active Constituents Of Calotropis Gigantea:
There are lots of Chemical constituents present in the plant of Calotropis Gigantea, the every part of the plant contains different Active constituents[11].
|
Sr. No |
Plant Part |
Active Constituents |
|
1 |
Root |
Calotropnaphthlene, Calotropinsespenol |
|
2 |
RootBark |
Β-Amyrin, Two Isomeric Crystalline Alcohols, Giganteol, Isogiganteol, Cardenolides |
|
3 |
Stembark |
Β-Calotropeol,Β-amyrin,Giganteol |
|
4 |
Leaves |
Alkaloids,Glycosides,Mudarine |
|
5 |
Latex |
Proteinase, Cysteine, 3’-Methyl Butanoates of Alpha Amyrin and Sigma Taraxasterol, Triterpine Ester, Akundarin, Uscharin, Calotoxin, Calactin, Α-calatropeol, Β-Calotropeol, Β-Amyrin, CalciumOxalate |
|
6 |
Flower |
BitterResins,Akundarin,Nα-Calatropeol,Β-Calotropeol, Amyrin, Cardioactive Glycosides, Mudarine, Asclepin, Calotropin |
6 Flower Bitter Resins, Akundarin, Nα-Calatropeol, Β-Calotropeol, Amyrin, Cardioactive Glycosides, Mudarine, Asclepin, Calotropin
Activities Shown By Calotropis gigantea Anti-Inflammatory Activity
Many experimental animal models were used to assess the anti-inflammatory properties of Calotropis gigantea. The anti-inflammatory effects of chloroform, n-butanol, ethanol, and distilled water extracts of Calotropis gigantea leaves were examined. The carrageenan-induced rat paw oedema method was employed to compare this activity with the standard medication, paracetamol.
Additionally, the anti-inflammatory efficacy was assessed in the rat paw oedema model caused by carrageenin for acute inflammation and in cotton pellet granuloma, an adjuvant-induced arthritis model used for chronic inflammation. It was also demonstrated that the antiinflammatory effect outperformed the albumin denaturation procedure [10].
Anti-Arthritic Activity
Rheumatoid arthritis, which affects about one percent of adults worldwide, is a persistent inflammatory autoimmune disease characterized by increased joint pain, stiffness, swelling, and loss of joint function. Pro-inflammatory cytokines, including IL-1β, TNF-α, IL-6, and IL-10, are elevated in this condition. Because lupeol is present in Calotropis gigantea, it has been claimedto possess anti-inflammatory and anti-arthritic properties [11].
Antidiabetic Activity
Several studies have reported that Calotropis gigantea exhibits antidiabetic efficacy by lowering increased blood glucose levels (Rathod et al., 2011). Extracts of the plant have hypoglycemic properties. Furthermore, Calotropis gigantea helps prevent body weight loss in diabetic conditions. In the pancreatic islets, it increases the number of granulated cells and normal beta cells. The plant extract has shown promising results in lowering high serum glucose levels in experimental animals [11].
Vasodilation Activity
The vasodilation activity of the latex extract of Calotropis gigantea was studied using the Rana hexadactyla (green frog). Cardiac output increased significantly when the crude extract diluted at 1:10and1:100concentrations was mixed with purified water. The1:10dilutionresultedina 50% increase in cardiac output, while the higher dilution (1:100) increased it by 66%. This indicates that at a certain dose, the latex exhibits vasodilatory action [10].
Analgesic Activity
The alcoholic extract of Calotropis gigantea flowers was reported to have analgesic activity in various preclinical studies. Oral administration of the alcoholic extract significantly decreased the incidences of writhing reflexes and paw licking time. The analgesic activity was studied using the acetic acid writhing model and the hot plate method [11].
Theoretical Analysis
1. Role of Ingredients:
• Calotropis Gigantea (Latex): Serves as the active ingredient. Its quantity varies across batches, with having higher concentrations, potentially enhancing therapeutic efficacy.
• Carbopol 940: Functions as a gelling agent. The difference in its concentration (1 g vs. 0.5 g) affects the gel’s viscosity and overall stability.
• Di Sodium EDTA: Acts as a chelating agent, helping to stabilize the formulation by binding metal ions. It is used consistently in all batches, indicating a standard stabilization approach.
Triethanolamine: Used for pH adjustment and to neutralize Carbopol. The uniform amount across all formulations indicates pH uniformity.
• Propylene Glycol: Works as a humectant and solvent, contributing to skin moisturization and ingredient solubilization. Its constant use across batches ensures consistent hydration.
• Water: Serves as the primary vehicle, bringing the total volume to 100 mL in each batch.
2. Formulation Variations:
•The main variations are in Calotropis Gigantea (Latex)andCarbopol940 concentrations.
3. Theoretical Implications:
• Efficacy: Likely higherinF3andF4duetoincreasedactiveingredientconcentration.
• Stability and pH: Presumed consistent across all batches due to the uniform inclusion of Di Sodium EDTA and Triethanolamine, supporting formulation integrity.
|
Sr. No |
Ingredients |
|
1 |
Calotropis Gigantea (Latex) |
|
2 |
Carbapol940 |
|
3 |
Di Sodium EDTA |
|
4 |
Triethanolamine |
|
5 |
Propylene Glycol |
5. Evaluation Parameter
Procedure of Evaluation Of Gel
Organoleptic Properties
Organoleptic properties are those aspects of formulation that an individual experiences via senses including taste, sight, smell, and touch.
•a) Colour: The colour of all the formulation swas observed visually.
•b)Odour: The odour was evaluated through smell.
•c) Appearance and Homogeneity Test: Physical appearance and homogeneity of the prepared gels were evaluated by visual perception.
pH Measurement
pH measurement of the gel was carried out using a digital pH meter by dipping the glass electrode completely into the gel system to cover the electrode. The measurement was carried out in triplicate and the average of the three readings was recorded [19].
Spreadability Test
Two sets of glass slides of standard dimensions were taken. The herbal gel formulation wasplaced over one of the slides. The other slide was placed on top of the gel so that the gel was sandwiched between the two slides over an area of 7.5 cm. A 100 g weight was placed on the upper slide to uniformly press the gel into a thin layer. After removing the weight, the excess gel was scraped off. The slides were fixed to a stand such that the upper slide could slip off freely when a 20 g weight was tied to it.
The time taken for the upper slide to travel 7.5 cm was noted. The experiment was repeated three times and the mean time was used for calculation [20].
Spreadability was calculate dusing the following formula:
S =M×L/T Where:
S =Spreadability
M= Weight tied to upper slide(20 g) L
= Length of glass slide (7.5 cm) T=Time taken in seconds
Skin Irritation Test of Gel
An area on the dorsal surface of the left hand was marked. The cream was applied to the marked area and the time was noted. Allergic or toxic reactions were observed at regular intervals over24 hours and noted [21].
Viscosity of gel was determined using a Brookfield Viscometer (S-64, Model LVDV-E) at 25°C. The spindle speed of the viscometer was rotated at 1, 1.5, 2, 2.5, 3, and 4 rpm [22].
Evaluation of Anti-Arthritic Activity of Gel Inhibition of Protein Denaturation Method Using Egg Albumin:
In vitro anti-arthritic activity of Calotropis gigantea was analyzed using the protein denaturation method with fresh hen’s egg albumin.
A5mlreactionmixturewaspreparedconsistingof:
• 0.2mlofeggalbumin(fromfreshhen’segg)
• 2.8mlofphosphate-bufferedsaline(pH6.4)
• 2 ml of various concentrations (25, 100, and 400 µg/ml) of Diclofenac sodium,
PBS served as the control. The mixtures were incubated at 37 ± 2°C for 15 minutes, then heated at 70°C for 5 minutes.After cooling,absorbance wasmeasured at 660 nm using vehicle as blank.
Percentage inhibition of protein denaturation was calculated using the formula [23]: % Inhibition = 100 × [(Absorbance of Test Sample / Absorbance of Control) – 1]
The herbal gel consists natural values and less amount of chemicals, it reduced various type of side effect of the largest organ of the body [skin]or mucous membrane the gelis prepared by simple method.the herbal gel containing antioxidant that can be used as the prevention of a barrier to protect skin. And the formulations are safe to use for the skin.
REFERENCES


Najim Pathan, Vidya Kale, Development And Characterization of Antiarthritic Gel of Calotropis Gigantea, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1049-1060, https://doi.org/10.5281/zenodo.20539218
 10.5281/zenodo.20539218
10.5281/zenodo.20539218