
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Kamalakshi Pandurangan College of Pharmacy, Ayyampalayam, Tiruvannamalai 60603, Tamilnadu, India.
Cefotaxime is classified as a third-generation cephalosporin antibiotic, recognized for its extensive activity against both Gram-positive and Gram-negative bacteria. It is commonly employed in treating severe bacterial infections such as septicemia, meningitis, pneumonia, and urinary tract infections. The distinctive pharmacokinetic characteristics of cefotaxime, along with its effective tissue penetration and resistance to numerous beta-lactamases, render it an essential component of contemporary antimicrobial therapy. This article provides a comprehensive review of the pharmacology, mechanisms of action, clinical applications, resistance issues, and safety profile associated with cefotaxime.
Antibiotic medicine was transformed by the discovery of cephalosporins, with cefotaxime marking a significant turning point in the development of third-generation drugs. Cefotaxime, one of the first cephalosporins to be introduced in the 1980s, was able to efficiently target a variety of Gram-negative bacteria, including some that were resistant to previous cephalosporins [1]. Its extensive coverage makes it a popular empirical therapy in hospital settings.
2. Chemical Structure and Classification:
Cefotaxime is a member of the third-generation cephalosporins category of the β-lactam antibiotic class. Its structure includes an oxime side chain that provides resistance to numerous β-lactamases made by resistant bacterial strains, as well as a β-lactam ring that is essential for antibacterial activity [2]. C16H17N5O7S2 is its chemical formula.
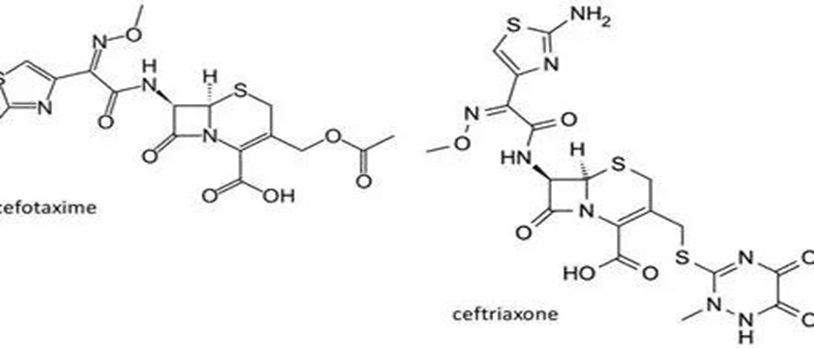
Fig.1 Structure of Third generation Cephalosporins
3. Mechanism of Action:
Cefotaxime works by preventing the formation of bacterial cell walls, just like other β- lactam antibiotics. By attaching itself to penicillin-binding proteins (PBPs) found within the bacterial cell wall, it disrupts the last transpeptidation stage of the formation of peptidoglycan. Bacterial cell death is the ultimate effect of this, which also causes osmotic instability and weaker cell walls [3].
4. Pharmacokinetics and Pharmacodynamics:
Cefotaxime's low oral bioavailability means it is typically given intravenously or intramuscularly. It is well distributed throughout bodily fluids and tissues, including the cerebrospinal fluid, most notably in inflammatory meninges [4]. Its half-life is around an hour, and the kidneys are the main organs that eliminate it. Desacetylcefotaxime, the drug's antibacterial activity-retaining form, is produced via hepatic metabolism [5].
5. Clinical Indications:
Cefotaxime is used in the treatment of a wide variety of infections:
1) Respiratory tract infections (e.g., pneumonia, bronchitis) [6]
2) Urinary tract infections
3) Gastrointestinal infections
4) Gynecological infections
5) Sepsis and bacteremia
6) Meningitis, especially due to H. influenzae, N. meningitidis, and Streptococcus pneumoniae [7]
7) Prophylaxis in surgical procedures
It is often used in paediatric and neonatal populations for its safety profile and efficacy against central nervous system infections.
6. Spectrum of Activity:
Cefotaxime has potent antibacterial properties against a variety of microbes. Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Hemophilus influenzae, and Neisseria gonorrhoeae are among the Gram-negative bacteria that it works well against. Streptococcus pneumoniae and Streptococcus pyogenes are two Gram-positive bacteria that it effectively combats. But its effectiveness against other organisms, as Pseudomonas aeruginosa and some Enterococci strains, is greatly diminished, which restricts its usage in infections brought on by these pathogens [8].
7. Resistance Mechanisms:
Cefotaxime resistance develops through a variety of routes, which makes it extremely difficult for it to remain effective in clinical settings. One of the most well-known methods is the synthesis of Extended-Spectrum Beta-Lactamases (ESBLs), which are enzymes that may hydrolyze the β-lactam ring and make cefotaxime inactive [9]. Some bacterial strains produce ESBLs in addition to using efflux pumps, which actively remove the antibiotic from the cell, lowering its intracellular concentration and decreasing its bactericidal action. Penicillin-binding protein (PBP) mutation is another cause of resistance that lowers cefotaxime's binding affinity and diminishes its ability to suppress cell wall formation. The therapeutic usefulness of cefotaxime has been severely weakened in a number of areas due to the extensive proliferation of Enterobacteriaceae that produce ESBLs, especially in hospital and community-acquired infections [10].

Fig.2 Cefotaxime Resistance Mechanism
Additionally, cefotaxime resistance spreads more quickly due to horizontal gene transfer of resistance genes between bacteria, making combination therapy or other antibiotics necessary for severe infections. To lessen the effects of cefotaxime resistance and maintain its therapeutic effectiveness, ongoing monitoring, prudent antibiotic usage, and infection control procedures are crucial.
8. Adverse Effects and Safety:
Like all drugs, cefotaxime might have negative side effects, but most patients tolerate it well. Among the most often reported adverse effects are nausea, vomiting, and diarrhea, which are all digestive problems. Severe anaphylaxis to moderate skin rashes and urticaria are examples of allergic reactions that might happen, especially in people who have previously experienced hypersensitivity to β-lactam medicines. Hematologic disorders such as thrombocytopenia and eosinophilia have been reported, although they are not very prevalent. Injection site pain or inflammation may be localized, particularly when administered intramuscularly. Rarely, neurotoxic side effects such seizures have been linked to cefotaxime, especially when taken in large dosages or by individuals with renal impairment [11]. As with all antibiotics, it's critical to keep an eye out for side effects, especially in patients who already have medical issues or are undergoing long-term treatment.
9. Drug Interactions:
Cefotaxime has the potential to enhance the nephrotoxic effects of aminoglycosides when administered simultaneously. Probenecid reduces the renal elimination of cefotaxime, which results in a higher plasma concentration of the drug. The anticoagulant effects may be intensified when cefotaxime is used in conjunction with warfarin [12].
Fig.3 Drug Interaction
10. Special Considerations:
1) Pregnancy: Categorized as Category B; use must be justified but there is no proof of fetal harm.
2) Renal Impairment: A dose modification is required.
3) Use in Paediatrics: Safe and efficient, especially for treating meningitis and newborn sepsis [13].
11. Recent Advances and Research:
The use of cefotaxime in combination therapy with beta-lactamase inhibitors and other antibiotics to fight resistance is being investigated in recent research [14]. Additionally, research is being done on nanoparticle-based drug delivery methods to increase cefotaxime's bioavailability and targeted delivery in chronic infections [15].
12. CONCLUSION:
Due to its broad-spectrum activity, advantageous pharmacokinetics, and proven effectiveness in treating severe bacterial infections, cefotaxime is still a useful antibiotic in clinical practice. But in order to maintain its usefulness, the increase in resistance—particularly from species that produce ESBLs—requires careful application, ongoing monitoring, and innovative combination treatments. The role of cefotaxime in empirical and targeted therapy is constantly changing as antibiotic stewardship gains importance, necessitating that clinicians remain up to date on new trends in resistance and treatment recommendations.
REFERENCES


R. V. Sivaprakash*, S. Sathish, K. Udayanithi, N. Vadivarasan, D. Rajalingam, Cefotaxime: A Comprehensive Clinical and Pharmacological Review of its Spectrum, Efficacy, Resistance, and Safety Profile, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2210-2215. https://doi.org/10.5281/zenodo.15957115
 10.5281/zenodo.15957115
10.5281/zenodo.15957115