
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Government College of Pharmacy, Kathora Naka, Amravati, Maharashtra-444604, India
Background: ?-agonists remain a cornerstone in asthma therapy but are associated with adverse effects, necessitating risk assessment and evaluation of treatment outcomes. This study aimed to assess the adverse drug effects, risk stratification, and treatment outcomes of ?-agonists among asthma patients at a tertiary care hospital.1,2 Methods: A prospective observational study was conducted at District General Hospital, Amravati, involving patients diagnosed with asthma and prescribed ?-agonists. Clinical data, adverse effects, and treatment responses were documented and evaluated using Naranjo’s scale and Common Terminology Criteria for Adverse Effects (CTCAE).7,8 Statistical analysis focused on the frequency and severity of adverse effects and therapeutic outcomes. Results: The majority of patients were aged 51–70 years, with a higher prevalence among Males. Salbutamol was the most frequently prescribed ?-agonist. The most common adverse effects included headache, and muscle cramps. According to Naranjo’s scale, 71% of reactions were ‘probable,’ or ‘definite.’7 Most adverse effects were mild to moderate. Cardiovascular manifestations such as tachycardia and ECG changes were noted in a subset of patients. Following dose modification or discontinuation. symptom improvement was observed in over 88% of cases. Conclusion: ?-agonists, though essential in asthma management, can produce clinically significant adverse effects. Regular monitoring, individualized dosing, and pharmacovigilance interventions are recommended to minimize risks and improve therapeutic outcomes.
Asthma is a chronic inflammatory disorder of the airways characterized by reversible airflow obstruction, bronchial hyperresponsiveness, and recurring episodes of wheezing, breathlessness, chest tightness, and coughing.1,2 It represents a significant global health burden, affecting individuals of all age groups and contributing to reduced quality of life and increased healthcare utilization. Effective management of asthma requires both control of chronic inflammation and prompt relief of acute bronchospasm.3,4
Among the cornerstone therapies in asthma management are β-agonists, which act by stimulating β?-adrenergic receptors in the bronchial smooth muscles, leading to rapid bronchodilation. Short-acting β-agonists (SABAs) are commonly used as rescue medications for immediate symptom relief, while long-acting β-agonists (LABAs) are used in combination with inhaled corticosteroids for maintenance therapy.5,10 Despite their clinical efficacy, β-agonists are associated with a range of adverse drug effects, including tremors, tachycardia, hypokalemia, and, in some cases, paradoxical bronchospasm. Prolonged or inappropriate use may also lead to tolerance, reduced responsiveness, and increased risk of asthma exacerbations.9
Assessment of adverse drug effects and associated risk factors is essential to optimize therapeutic outcomes and ensure patient safety. Factors such as age, comorbid conditions, dosing patterns, inhalation technique, and concomitant medications may influence both the efficacy and safety profile of β-agonists. Therefore, systematic evaluation of these parameters is crucial in clinical practice, particularly in hospital settings where diverse patient populations are treated.
Drug utilization studies and pharmacovigilance play a vital role in identifying patterns of adverse drug reactions and evaluating treatment outcomes. Monitoring these aspects in a tertiary care hospital setting, such as District Government Hospital (DGH) Amaravati, provides valuable real-world evidence that can guide clinicians in improving prescribing practices and patient management strategies.
This study aims to assess the adverse drug effects, evaluate associated risk factors, and analyse treatment outcomes of β-agonist therapy in asthma patients at DGH Amaravati. The findings of this study are expected to contribute to safer and more effective use of β-agonists, ultimately enhancing the quality of care and clinical outcomes in asthma management.
Aim & Objectives
To comprehensively evaluate the adverse drug effects, risk factors, and treatment outcomes associated with β-agonist therapy in patients with asthma at District Government Hospital (DGH), Amravati.
To monitor and analyse changes in key clinical and biochemical parameters, including serum potassium levels, electrocardiographic (ECG) findings, blood glucose levels, and leukocyte count during β-agonist therapy.
MATERIALS AND METHODS
Study Design and Setting
A hospital-based prospective observational study was conducted at the District Government Hospital (DGH), Amaravati. The study was carried out in the Departments of General Medicine, Paediatrics, and Intensive Care Unit (ICU).
Study Duration
The study was conducted over a period of six months, from October 2024 to March 2025.
Study Population
A total of 130 patients diagnosed with asthma and receiving β-agonist therapy were included in the study. Patients were selected from inpatient departments of General Medicine, Paediatrics, and ICU.
Inclusion Criteria
Patients of all age groups diagnosed with asthma
Patients receiving β-agonist therapy (current or past use)
Patients with a history of asthma or related respiratory diseases
Patients willing to participate and provide informed consent
Exclusion Criteria
Patients attending outpatient departments (OPD).
Patients unwilling to participate in the study Pregnant and breastfeeding women
Data Collection
Data were collected using a pre-designed and validated patient data collection form. Information was obtained through:
The collected data included:
Adverse drug effects were evaluated and classified using:
Outcome Measures
The primary outcomes assessed included:
Treatment outcomes, including symptom improvement, exacerbations, and overall patient well-being.
Study Approval & Ethical Considerations Informed consent was obtained from all participants (with verbal consent and a witness for illiterate patients), and confidentiality was maintained. Institutional Ethics Committee approval was secured prior to conducting the study at District General Hospital, Amravati.
Statistical Analysis
Data were analysed using appropriate descriptive statistical methods. Results were expressed in terms of percentages and frequency distributions.
RESULTS
A total of 130 asthma patients receiving β-agonist therapy were included in the study conducted at District Government Hospital (DGH), Amaravati.
Table 1: Demographic and Clinical Profile of Participants (n = 130)
Demographic Characteristics
Out of 130 patients, the majority were in the adult age group (18–60 years), followed by paediatric and geriatric populations. A slight female predominance was observed compared to male patients. Most patients were admitted to the General Medicine department, followed by Paediatrics and ICU.
Pattern of β-Agonist Use
Among the β-agonists prescribed, short-acting β-agonists (SABAs) were the most commonly used for acute symptom relief, while long-acting β-agonists (LABAs) were prescribed mainly in combination therapy for maintenance treatment. Nebulization was the most frequently used route of administration in hospitalized patients.
Incidence of Adverse Drug Effects (ADEs) Out of the total study population, a significant proportion of patients experienced at least one adverse drug effect associated with β-agonist therapy. The most commonly reported ADEs included:
Causality Assessment
Based on Naranjo’s Adverse Drug Reaction Probability Scale, most of the reported adverse drug effects were categorized as: Probable.
Followed by Possible, very few cases were classified as Definite.
Table 2: Treatment Pattern and Adverse Drug Effects
Severity Assessment
Using CTCAE criteria, the majority of adverse drug effects were classified as:
A small number of cases showed severe reactions, particularly hypokalaemia and significant tachycardia requiring intervention.
Risk Factors Associated with ADEs:
Treatment Outcomes
Most patients showed significant clinical improvement with β-agonist therapy, including relief from bronchospasm and improved breathing.
Reduced frequency of asthma exacerbations was observed in patients receiving appropriate combination therapy
A small proportion of patients required dose adjustment or discontinuation due to adverse effects
Overall, β-agonists were found to be effective and relatively safe when used appropriately.
Table 3: Monitoring Parameters and Treatment Outcome
DISCUSSION
The present study evaluated the adverse drug effects, risk assessment, and treatment outcomes of β-agonists in asthma patients at District Government Hospital (DGH), Amaravati. β-agonists remain one of the most commonly prescribed bronchodilators for the management of asthma because of their rapid bronchodilatory action and effectiveness in relieving airwayobstruction. However, their use is often associated with clinically significant adverse effects that may influence treatment adherence and patient safety.
In this study, the majority of patients belonged to the 51–70 years age group, indicating that respiratory diseases requiring β-agonist therapy were more common among older adults. A higher proportion of male patients (63%) was observed compared to females, which may be related to increased environmental exposure, smoking history, and occupational risk factors among men. Similar findings have been reported in previous respiratory pharmacovigilance studies where elderly males constituted a large proportion of hospitalized respiratory patients.
Among respiratory conditions, asthma accounted for 55% of cases, followed by COPD. Salbutamol was the most frequently prescribed β-agonist (64.61%), reflecting its widespread use as a short-acting bronchodilator for rapid symptom relief. This finding is consistent with current treatment guidelines that recommend short-acting β?-agonists as rescue therapy in acute bronchospasm17
Fig.no.1. Utilization of Beta-agonist drugs
The most frequently observed adverse drug effects were headache, muscle cramps, and tachycardia, with tachycardia reported in 44.61% of patients.11 These adverse effects can be explained by systemic β-receptor stimulation caused by repeated or high-dose administration. Similar adverse reactions have been documented in earlier studies, where β-agonist therapy was associated with cardiovascular stimulation and skeletal muscle effects.
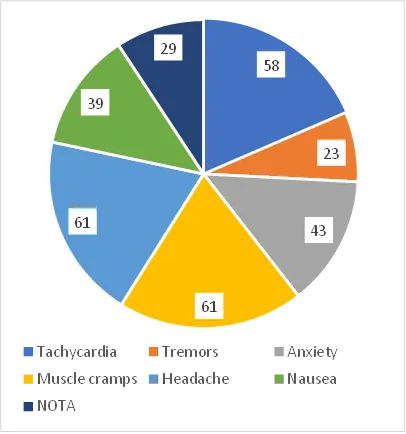
Fig.no.2. Adverse Drug effects
Laboratory monitoring revealed a considerable incidence of hypokalaemia (70%) and hyperglycaemia (84%), indicating the metabolic effects of β-agonists. β?-receptor stimulation promotes intracellular potassium shift and glycogenolysis, which may predispose susceptible patients to electrolyte imbalance and elevated blood glucose levels. Additionally, ECG abnormalities were identified in 93.10% of patients, emphasizing the importance of cardiac monitoring, especially in patients with pre-existing cardiovascular disease.
The causality assessment performed using Naranjo’s scale demonstrated that 71% of adverse drug reactions were categorized as probable or definite, supporting a strong association between β-agonist use and the observed adverse effects. Most reactions were graded as mild to moderate in severity (81%) according to CTCAE criteria, suggesting that although adverse effects were common, they were generally manageable with appropriate monitoring and dose adjustment.
Despite the occurrence of adverse effects, the treatment outcomes were favourable in most patients. Approximately 88% of patients showed symptomatic improvement, and 87.67% reported improved general well-being, indicating that β-agonists remain effective in controlling asthma symptoms when used appropriately. However, the presence of adverse effects highlights the need for individualized therapy, patient counselling, and regular follow-up to improve safety and therapeutic outcomes
The findings of this study emphasize the importance of pharmacovigilance and routine risk assessment in patients receiving β-agonist therapy. Early identification of adverse effects can help healthcare professionals optimize treatment, prevent complications, and enhance the overall quality of asthma management.
Fig.no.3. Treatment outcomes
CONCLUSION
The present study highlights that β-agonists are highly effective bronchodilators in the management of asthma, with the majority of patients showing significant improvement in symptoms and overall well-being. However, their use is associated with a considerable incidence of adverse drug effects, particularly tachycardia, headache, muscle cramps, hypokalaemia, and hyperglycaemia.
Most adverse drug reactions were found to be mild to moderate in severity and showed a probable association with β-agonist therapy, indicating that these effects are generally manageable with proper monitoring. The study also identified key risk factors such as high dosage, frequent use, comorbid conditions, and advanced age, which may increase the likelihood of adverse outcomes.
The high prevalence of electrolyte imbalance and ECG abnormalities observed in this study underscores the importance of regular clinical and laboratory monitoring, especially in patients with underlying cardiovascular conditions. Additionally, the low level of patient awareness regarding potential risks emphasizes the need for patient education and counselling to improve safe medication use.
Overall, β-agonists remain an essential component of asthma therapy; however, their rational use, careful dose optimization, and continuous pharmacovigilance are crucial to minimize adverse effects and enhance treatment outcomes. Implementation of these strategies can significantly improve patient safety and the quality of asthma care in clinical practice.
ACKNOWLEDGEMENTS
The authors express their sincere gratitude to the management and staff of District Government Hospital (DGH), Amaravati, for granting permission and providing the necessary facilities to carry out this study. We are especially thankful to the physicians, nursing staff, and supporting healthcare professionals of the Departments of General Medicine, Paediatrics, and Intensive Care Unit for their valuable cooperation and assistance during data collection.
We extend our heartfelt appreciation to our academic mentors and faculty members for their continuous guidance, encouragement, and support throughout the study. Their expertise and constructive suggestions played a crucial role in the successful completion of this work.
We are also grateful to all the patients who willingly participated in this study and contributed valuable information, without whom this research would not have been possible.
Finally, we acknowledge the support of our colleagues and friends who directly or indirectly contributed to the completion of this study.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest regarding the publication of this study. The research was conducted independently, and no financial or commercial relationships that could be construed as a potential conflict of interest were involved.
SUMMARY
Asthma is a chronic respiratory disorder requiring effective bronchodilator therapy for symptom control and prevention of exacerbations. β-agonists are widely used due to their rapid bronchodilatory effect; however, their use is associated with various adverse drug effects that may influence patient safety and treatment outcomes.
This prospective observational study was conducted at District Government Hospital (DGH), Amaravati, including 130 patients receiving β-agonist therapy. The study assessed the incidence of adverse drug effects, associated risk factors, and overall treatment outcomes. The majority of patients were elderly males, and short-acting β-agonists, particularly salbutamol, were the most commonly prescribed drugs.
Commonly observed adverse drug effects included headache, muscle cramps, and tachycardia. Significant metabolic and cardiac effects such as hypokalaemia, hyperglycaemia, and ECG abnormalities were also noted. Most adverse drug reactions were categorized as probable and were mild to moderate in severity. Identified risk factors included high dosage, frequent drug use, comorbid conditions, and advanced age.
Despite the occurrence of adverse effects, the majority of patients showed significant clinical improvement and better overall well-being, indicating the effectiveness of β-agonists when used appropriately.
In conclusion, β-agonists remain a key component in asthma management; however, careful monitoring, dose optimization, and pharmacovigilance are essential to minimize adverse effects and improve therapeutic outcomes
REFERENCES





Yogesh Agrawal, Mona Agrawal, Aditya Badhe*, Anamika Kavitkar, Sakshi Kakde., Adverse drug effects, Risk assessment & Treatment outcomes of Beta Agonist in Asthma Patients in DG Hospital, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6,6159-6169. https://doi.org/10.5281/zenodo.20835503
 10.5281/zenodo.20835503
10.5281/zenodo.20835503