
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Pharmaceutical Research Division, Department of Pharmaceutics, Amar Shaheed Baba Ajit Singh Jujhar Singh Memorial College of Pharmacy, BELA (Ropar), Punjab, India, 140111
Drug delivery by oral route is one of the best methods of drug delivery due to some major advantages over other routes. However, in conventional oral dosage forms, low oral bioavailability is one of the significant problems. Gastroretentive drug delivery systems are designed to overcome drawbacks of conventional oral dosage forms. These systems help to increase gastric residence time and enhance the drugs bioavailability especially those with narrow absorption window. The conventional approaches such as floating, expandable, and mucoadhesive systems have demonstrated promising outcomes but each method has its own limitations. Therefore, this review focuses on combination approaches in GRDDS that combines two or more retention mechanisms to improve gastric retention, controlled drug release, and enhanced therapeutic efficacy. The article begins with an overview of major GRDDS strategies, outlining their principles, advantages, polymers used in distinct systems. It then emphasizes hybrid systems, including floating–expandable, expandable–mucoadhesive, and floating–mucoadhesive combinations, supported by a comparative table summarizing previously reported studies. Special attention is given to floating mucoadhesive tablets by providing the details of formulation components, preparation methods, and underlying mechanistic principles. The mechanistic foundations of floating mucoadhesive systems are discussed, with particular focus on buoyancy, polymer swelling, and bioadhesion processes. Key evaluation parameters such as floating lag time, total floating time, swelling index, mucoadhesive strength, and in vitro drug release studies are also mentioned in this review. The review also presents the current challenges of gastroretentive technologies and future prospects of combined approaches as well. Overall, combination approaches represent potential methods of gastroretention to achieve more predictable and effective effects and results.
Drug administration through oral route is considered to be one of the most preferred route for drug delivery. Nearly 90% of all medications are taken orally. There are several reasons for preference of this route that includes its benefits of patient compliance, non-invasive and properties of ease of administration. Due to properties of easy storage and transportation, cost-effectiveness and no specialized medical personnel are required to administer, tablets are commonly used dosage forms tablets have remained one of the most commonly used dosage forms over time [1]. However, many oral medications that have a limited window of absorption or pH-dependent solubility or stability may have inadequate bioavailability. When developing a formulation, these characteristics must be taken into account because they may result in insufficient medication absorption when the dosage form is moved to the lower gastrointestinal tract (GIT) [2-3].
Gastroretentive Drug Delivery system is one of the simplest and efficient approaches which can overcome all the limitations associated with conventional tablets. GRDDS serves as an effective controlled release system by prolonging gastric residence time and ensures sustained drug delivery at the desired site of absorption. By retaining drug in stomach for long time, complete solublisation and complete absorption of drug takes place that further results in minimum plasma fluctuation and increased bioavailability. GRDDS is suitable for drugs with short half life, drugs that are unstable and poorly soluble at alkaline pH, and exhibit local action at the upper section of the gut [4]. Another benefit of this system includes less frequent administration of drugs that further increases patient compliance [5].
A number of gastroretentive drug delivery techniques have been developed over the past few decades, such as mucoadhesive systems that cause bioadhesion to the stomach mucosa, low-density systems that create buoyancy in gastric fluid, and high-density systems that are retained in the bottom of the stomach, systems that are swellable, unfoldable, or extendible that restrict the dosage forms ability to pass past the stomach's pyloric sphincter, ultra porous hydro [6]. Although each of these approaches has its own limitations, combination approaches can effectively overcome the drawbacks of individual systems [7].
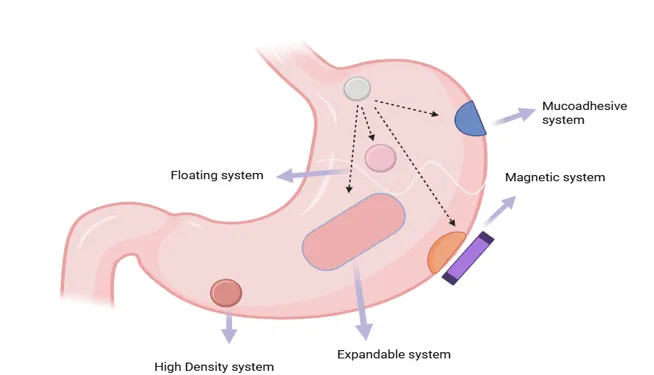
Fig 1. GRDDS Approaches
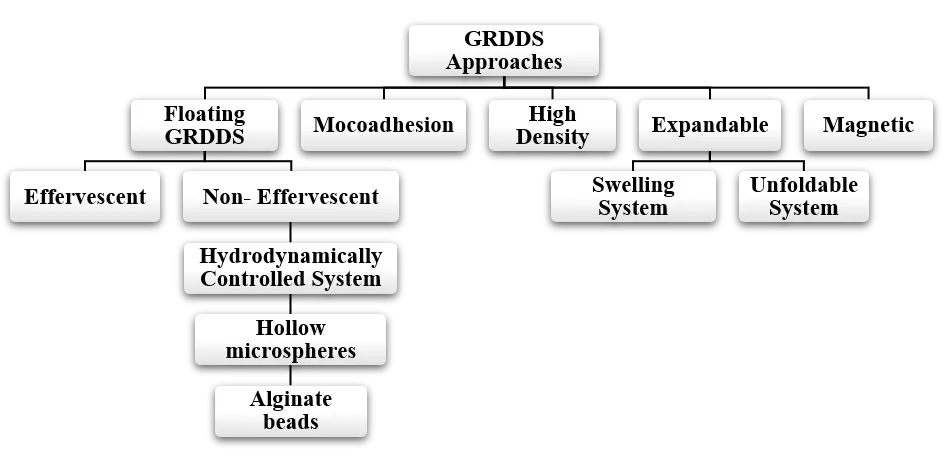
Fig 2. Flowchart representation of GRDDS
Although all of these individual gastroretentive drug delivery approaches are efficient in retaining drugs in stomach and for controlled release medications but each individual system have its limitation as well. Floating system shows high dependency on gastric contents and fluid in stomach. Due to high mucus turnover rate, mucoadhesive sometimes lacks the ability of stomach retention [18]. The magnetic system needs external device which keeps the drug at a particular location in stomach due to which it compromises with patient compliance. High density systems are difficult to formulate and this system also reduce patient compliance as patient might feel fullness which cause discomfort. Expandable systems can cause pyloric obstruction if does not shrink back to a safe size after drug release. Combination approach can tackle all the disadvantages of individual approaches. This is the reasons of combination therapies are now being studied extensively. Some of the main combination approaches that are now being researched are as follows:
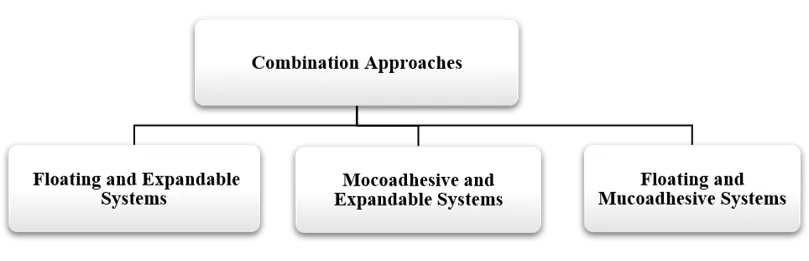
Fig 3. Combination Approaches
This gastroretention approach involves systems that are capable of floating as well as expanding or swelling. Such formulations should meet four key requirements. First, the size of dosage form should be small enough so that can be swallowed easily. After reaching the stomach, it must float and stay buoyant to prevent early escape from the gastric environment. Then upon exposure to gastric fluid, it must quickly expand to a size which is large enough to block its passage through the pyloric sphincter. Lastly, once prolonged gastric retention is no longer required, the formulation should decrease in size so it can safely exit the stomach. Polymers than can swell enough to block pyloric sphincter, HPMC K4M, K15M and K100M, PEO and chitosan are used in this formulation [19]. The research conducted on this combination gastroretentive system is summarized in Table 1.
Table 1. Research conducted on Floating and Expandable Systems
|
Drug |
Formulation Strategy and Performance Outcomes |
References |
|
Losartan |
Polymers Used: Hydroxyethyl cellulose + Chitosan. |
[20] |
|
Additional Functional Agent: Sodium bicarbonate (gas-generating agent). |
||
|
Key Findings: Lower-viscosity chitosan improved swelling due to faster medium penetration. Sodium bicarbonate negatively affected chitosan swelling by neutralizing pH; therefore, an optimal polymer:sodium bicarbonate ratio is required. |
||
|
Release Behavior: Sustained release for 16 hours in vitro; drug release followed Case-II diffusion model (swelling-controlled). |
||
|
In vivo / Other Notes: Good swelling and buoyancy achieved with 1:1 polymer ratio. |
||
|
Ranitidine |
Polymers Used: Polyethylene oxide (PEO) + HPMC K4M (release-retarding polymer). |
[21] |
|
Additional Functional Agent: Camphor (optimal sublimating agent). |
||
|
Key Findings: Sublimation produced a highly porous gastro-retentive layer promoting buoyancy and swelling. PEO provided persistent swelling for 12 h with high wet strength. HPMC K4M slowed drug release. |
||
|
Release Behavior: Sustained release for 12 hours in vitro; release strongly dependent on percentage of HPMC K4M (percolation threshold: 11.48–21.69% v/v). |
||
|
In vivo / Other Notes: In vivo studies in Beagle dogs showed effective gastric retention, especially in the fed state. |
This system combines properties of expansion and mucoadhesion in such as manner that firstly after oral administration, dosage form expand or swell to a size that prevents passage through the pylorus. The main reason is presence of highly swellable polymers in formulation. Simultaneously, mucoadhesive polymers anchor it to the stomach wall. This dual mechanism enhances gastric residence time, reduces variability in retention, and supports a more sustained and predictable drug release profile. Various studies demonstrate that Expandable and Mucoadhesive Systems have capability of better gastric retention for release of drugs in upper GIT tract and some of them are listed in table 2.
Table 2. Research done on Expandable and Mucoadhesive system
|
Drug |
Formulation Strategy and Performance Outcomes |
References |
|
Alendronate |
System / dosage form: Compressed tablets made from lyophilised chitosan / ring-opened PVP (roPVP) complexes. |
[22] |
|
Additional functional / processing steps: Preparation with NaOH and heat; lyophilisation to produce powders, then compression into tablets. |
||
|
Key findings: Chitosan/roPVP complexes showed a synergistic increase in mucoadhesion versus chitosan alone. Viscosity and mucoadhesive force increased with higher chitosan content; complexes interacted more strongly with mucin regardless of chitosan MW. |
||
|
In-vitro release & mechanism: Provided 24-h in-vitro release. Release rate increased with swelling ratio (larger gel volume → less hindered diffusion). |
||
|
In-vivo / other notes: In rabbits, high-MW chitosan/roPVP tablets were retained in the stomach and produced higher AUC, longer t½, improved bioavailability and lower Cmax versus a quarter Fosamax® tablet — indicative of reduced toxicity risk and improved efficacy. |
||
|
Furosemide |
System / dosage form: Bilayer unfolding capsule (folded films inside a capsule). |
|
|
Polymers / materials: Controlled-release mucoadhesive film: Carbopol® 971P + HPMC E4M; plus an immediate-release polymeric film. |
||
|
Additional functional / processing steps / geometries tested: Two folding geometries tested — Case I: controlled film folded zig-zag with IR film rolled over it; Case II: both films folded zig-zag. Key findings: Case II (both films folded zig-zag) allowed better unfolding in acidic media. Carbopol® 971P provided mucoadhesion via H-bonding with gastric mucosa; HPMC E4M aided swelling. Good unfolding, mucoadhesion and controlled release — formulation considered promising for in-vivo use. |
||
|
In-vitro release & mechanism: Controlled release followed Fickian diffusion (HPMC contributed to swelling-controlled release). |
||
|
In-vivo / other notes: Demonstrated suitable unfolding and mucoadhesive behaviour suggesting potential for in-vivo gastric retention. |
The floating–mucoadhesive gastroretentive approach combines buoyancy with bioadhesion to enhance gastric retention. In these combination systems both kind of polymers are present. Some polymers help the formulation to remain buoyant in stomach while mucoadhesive polymers promote attachment of formulation to the gastric mucosa. This dual mechanism reduces the risk of premature gastric emptying and ensures more consistent and prolonged drug release [26].
Table 3. Research done on Floating and Mucoadhesive system
|
Drug |
Formulation Strategy and Performance Outcomes |
References |
|
Cilnidipine |
Polymers used: Gellan gum (bioadhesive), HPMC K4M |
[24] |
|
Additional functional agent / type: Sodium bicarbonate (effervescent/gas-generating). |
||
|
Main mechanisms: Effervescent floatation + mucoadhesion. |
||
|
Key findings: ↑ polymer content → ↓ floating lag time and ↑ total floating time (swelling + CO₂ entrapment). Gellan gum and HPMC produced strong mucoadhesion (mucin interactions and polymer entanglement). |
||
|
Release behaviour: Sustained release up to ~12 h; non-Fickian (combined diffusion + erosion) mechanism. |
||
|
Other notes / in-vivo: Human volunteer studies showed increased gastric retention, prolonged half-life and decreased elimination rate versus conventional tablet. |
||
|
Alfuzosin |
Polymers used: Chitosan + HPMC (gastroretentive sponges). |
[25] |
|
Additional functional agent / type: — (form is low-density sponge). |
||
|
Main mechanisms: Immediate floatation + mucoadhesion (electrostatic interactions of chitosan with mucin). |
||
|
Key findings: Very low density → immediate floatation; chitosan sponges exhibited higher mucoadhesion. Drug release decreased with increasing polymer concentration. |
||
|
Release behaviour: Sustained; non-Fickian diffusion. |
||
|
Other notes / in-vivo: In vivo studies in healthy male volunteers confirmed gastroretentive potential. |
||
|
Ranitidine |
Polymers used: Chitosan + PEO; crosslinker: sodium tripolyphosphate (TPP). |
[28] |
|
Additional functional agent / type: — (cross-linking agent used to strengthen matrix |
||
|
Main mechanisms: Mucoadhesion + non-effervescent floatation (high porosity). |
||
|
Key findings: Cross-linking enhanced mucoadhesion and stability; high porosity produced immediate floatation and buoyancy >24 h; cross-linked mats reduced burst release and prolonged release up to 24 h. |
||
|
Release behaviour: Prolonged controlled release with reduced initial burst. |
||
|
Other notes / in-vivo: Promising controlled-release GRDDS with improved retention and stability. |
||
|
Nizatidine |
Polymers used: Cross-linked chitosan/PEO nanofibres. |
[29] |
|
Additional functional agent / type: Cross-linking (to strengthen fibres). |
||
|
Main mechanisms: Mucoadhesion + floatation. |
||
|
Key findings: Cross-linked nanofibres showed significantly stronger mucoadhesion than uncross-linked; sustained release with reduced burst effect. |
||
|
Release behaviour: Sustained release (reduced burst). |
||
|
Other notes/ in-vivo: In vivo (rats) showed significant gastroprotective activity superior to drug solution and uncross-linked fibres. |
Floating-mucoadhesive tablets are oral dosage forms that combine mucoadhesion and buoyancy to improve drug bioavailability by increasing gastric retention of drugs that absorb in the upper gastrointestinal tract. In formulation of these tablets mucoadhesive polymers like chitosan, carbopol and sodium alginate are used to adhere drug to mucus membrane. Also the swellable or gas-generating polymers like HPMC, sodium bicarbonate are responsible for floating of tablets in upper GIT. Based on formulation, floating mucoadhesive tablets exist as single-layer systems or bilayer systems. These tablets are beneficial because these formulations helps to maintain the drug at the absorption site for extended durations, ensure predictable release of drug, reduces dosing frequency, and minimize plasma fluctuations [30]. They also enhance bioavailability of poorly soluble drugs, improve stability of drug that are drugs unstable at alkaline pH, and also helps to increase half life of drugs.
In the wet granulation method, the drug and polymers are mixed and converted into granules by using a binder solution. The detailed process can be described as:

Fig 4.Wet Granulation Method of Tablet Preparation
Firstly after weighing every component precisely, components are mixed and blended properly. Afterwards, by using a suitable solvent a wet mass is prepared. The wet mass is then dried overnight at in a hot air oven for 24 hours at 40°C after which it is passed through a 40 mesh screen. Then, the dried granules are mixed with magnesium stearate. Lactose is used as a filler or channeling agent [13].
The uniformly lubricated granules compressed into tablet by using a tablet punching. The compression force is adjusted between 6.2 and 6.9 kg/cm2 by using Monsanto or Pfizer hardness tester. The process is simply described in figure 4 clearly [13].
Dry granulation is particularly useful when the drug and excipients are moisture or heat sensitive. For preparation of floating mucoadhesive tablet, firstly weigh drug and all excipients precisely and pass all ingredients through a sieve. Then except effervescent agents, all powders are slugged in punching machine or passed through a roller compactor. The prepared slugs are then passed by a sieve to form granules. At final step, lubricants and effervescent agents are mixed with granules and press mixture in tablet punching machine to obtain final formulation. A simple flowchart of process is shown below in fig 5.

Fig 5. Dry Granulation
This method is used when drug and excipients are freely flowing, compressible moisture or heat sensitive. The process is simple; firstly after mixing all the excipients and drug, materials are passed through a sieve. Then mixture is blended and compressed into tablet after adding lubricants at last.
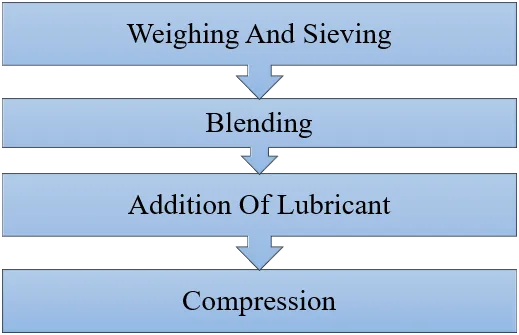
Fig 6. Direct Compression
The concept of floating and sinking was first described by Archimedes, who proposed that an object placed in a fluid experiences an upward buoyant force equal to the weight of the fluid it displaces. To explain this statement, he considered three cases which are - a body whose density equals the fluid’s density, a body whose density is lesser than that of the fluid, and a body whose density is more than that of the fluid [31]. The bulk density of floating systems is less than gastric content that is less than 1.004 g/cm3 which makes them capable to float in stomach [33].
If, ρ dosage form <ρ gastric fluid, the dosage form will float
And if, ρ dosage form> ρ gastric fluid, the dosage form doesn’t float
The buoyancy can either be achieved by entrapping air or CO₂ within the polymer matrix or by increasing the volume of the system through swelling. The low-density excipients can also be used for this purpose.
In this system matrix forming hydrophilic polymers are used for controlled floatation. Polymers like HPMC, PEO hydrate, form a gel layer around tablet or formulation. This gel layer traps CO2 inside swollen matrix that makes the dosage form dense and keeps it buoyant for longer durations. This system is applicable to non-effervescent as well as effervescent floating tablets.
In these systems, sodium bicarbonate and acidic components are used to achieve floatation. In presence of gastric acid, effervescent agents react and produce CO₂ which becomes entrapped within polymer matrix that decreases density of dosage form. The reaction can be represented as follows:
NaHCO3 + H+ → Na+ + CO2↑ + H2O
Some systems float without gas generation. Polymers like HPMC K4M, PEO and xanthan gum absorb water and swell 2–5 times their original size [32]. Swelling increases volume of dosage form and the density drops.
ρ = mv

If volume (v) increases and mass (m) is constant, density (ρ) decreases, hence tablet floats.
There are two stages of mucoadhesion, named as contact and consolidation stage which are clearly shown in diagram shown below:

Fig 7. Mechanisms of Mucoadhesion
If θ < 90° , it indicates good wetting, favorable for mucoadhesion
θ > 90° , represents poor wetting
θ = 0° , represents complete wetting
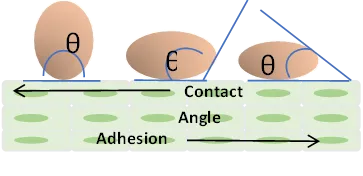
Fig 8. Wetting Theory
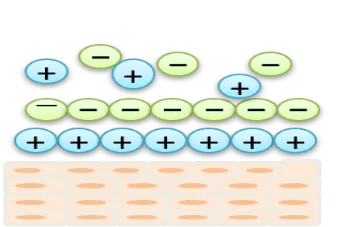
Fig 9. Electronic Theory
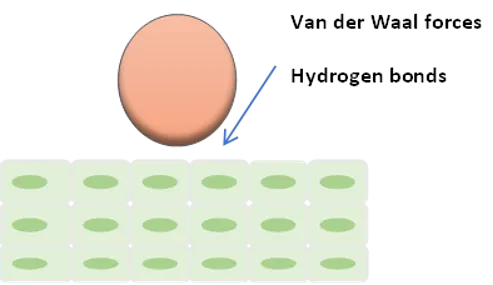
Fig 10. Adsorption Theory
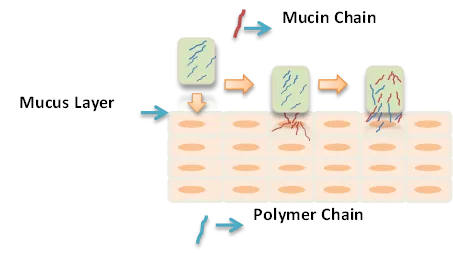
Fig 11. Diffusion Theory
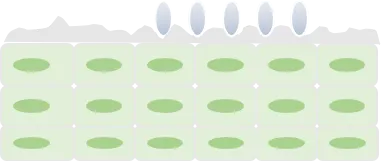
Fig 12. Mechanical Theory
σ=(E*Ԑ/L
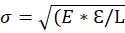
This theory does not take into account the diffusion parameters or the interpenetration parameters of polymer chains since it considers the forces that are involved in breaking and separating the surfaces [42].
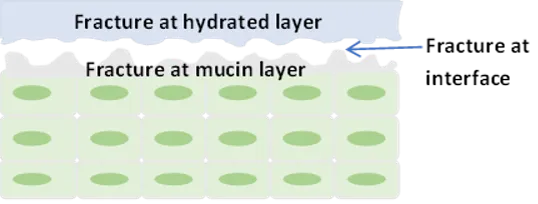
Fig 13. Fracture Theory
The floating mucoadhesive tablets can be evaluated by performing several evaluation tests. Firstly, preformulation studies are done to determine characteristics of drug and polymers. Then, flow properties of powder blends are determined. After that tablet is formulated and are evaluated to obtain an optimized tablet. Some of the important evaluation tests are enlisted in figure 14.
Fig 14. Evaluation Parameters of Floating Mucoadhesive Tablet
ρb = mb/ vb
Where, ρb

= bulk density
mb

= mass of powder
vb

= bulk volume of powder
ρt = mt/ vt
Where, ρt

= tapped density
mt

= mass of powder
vt

= tapped volume of powder
θ = tan-1hr

where, θ = Angle of repose
h = height of powder heap
r = radius of powder heap
Index = Tapped Density-Bulk DensityTapped Density

×

100
Hausner’s ratio = Tapped DensityBulk Density
The compendial and non compendial tests are done to evaluate the final formulation. Some of the tests are explained below:


The future of gastroretentive drug delivery systems (GRDDS) will be defined by combination approaches that integrate complementary retention mechanisms to deliver predictable gastric residence and controlled drug release. Hybrid platforms merging floating, mucoadhesive, swelling/expandable, and density-modulating functions will be rationally engineered through advanced polymer chemistry. Stimuli-responsive, biodegradable, and multifunctional polymers, together with computational formulation modeling and machine-learning–assisted optimization, will enable tailored, patient-centric release profiles. Manufacturing innovations such as three-dimensional printing and continuous hot-melt extrusion will allow precise geometry, dose personalization, and scalable production. Improved in vitro–in vivo correlations, standardized evaluation protocols, and real-time imaging will accelerate translational success. Regulatory harmonization and comprehensive safety assessment must accompany technological progress to ensure clinical adoption. Addressing inter- and intra-patient gastric variability and integrating pharmacokinetic– pharmacodynamic modeling will enhance therapeutic predictability for narrow-absorption-window drugs. Combination GRDDS are poised to improve bioavailability, reduce dosing frequency, and increase patient adherence, expanding therapeutic options for challenging molecules clinically.
CONCLUSION
Hybrid approaches for gastroretentive drug delivery, employing combination mechanisms, may provide promising approach to overcome the limitations of single-mechanism gastroretentive systems. Such hybrid systems may combine the benefits of buoyancy, mucoadhesion, and/or expansion with adhesion to prolong the gastric residence time helps to minimize intersubject variability, and achieve more effective and controlled release of the active pharmaceutical ingredient, especially for drugs with narrow absorption window. For instance, the concept of floating-mucoadhesive tablets exemplifies the potential benefits of hybrid systems that can combine the benefits of buoyancy and adhesion in a synergistic manner to achieve effective gastroretentive action without compromising patient acceptability. A clear understanding of the underlying mechanisms of buoyancy, swelling, and bioadhesion, including the underlying science, will be crucial in the design of effective gastroretentive drug delivery systems, including hybrid systems that combine the benefits of more than one mechanism of gastroretentive action. Furthermore, robust in vitro testing, including floating lag time, swelling index, mucoadhesive strength, and dissolution, in addition to in vivo testing, will be important in establishing in vitro–in vivo correlations, and the challenges and limitations that remain to be overcome include physiological variability, reproducibility in large-scale manufacture, and the need to meet regulatory requirements for performance and safety. With the development of newer and more advanced polymers, including stimuli-responsive and multifunctional polymers, and the application of computer-aided optimization techniques, development of hybrid gastroretentive technologies will gain momentum in the near future, and the emphasis on understanding the underlying science, in vitro and in vivo testing, and the need to address the challenges and limitations that remain to be overcome will be crucial in the development of effective and safe gastroretentive drug delivery systems in the near future.
REFERENCES





Harshita Sharma, Shailesh Sharma, Barsha Deb, Sukhvir Kaur, Sukhpreet Kaur, Combination Strategies for Gastroretention: A Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6178-6195. https://doi.org/10.5281/zenodo.20835650
 10.5281/zenodo.20835650
10.5281/zenodo.20835650