
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3,4,5 Department Of Pharmacy Practice, Sri Venkateshwara College Of Pharmacy, Madhapur, Hyderabad, Telangana, India
6 Department Of Infectious Diseases, Apollo Hospitals, Jubilee Hills, Hyderabad, Telangana, India.
Teicoplanin is a glycopeptide antibiotic widely used for the management of Gram-positive infec-tions in intensive care units (ICUs). This 6-month prospective observational study aimed to evalu-ate the usage and dosing patterns of Teicoplanin among 250 adult ICU patients in a tertiary care hospital who met the inclusion criteria. Data regarding patient demographics, dosage, frequency, duration of therapy, laboratory parameters, dialysis status, and clinical outcomes were collected and analysed using SPSS. The majority of patients were aged ?60 years (51%) and were male (60%). Sepsis (28%) was the most common indication, followed by septic shock (25%). The most frequent-ly prescribed dose was 400 mg (73%), predominantly administered twice daily (46%). Statistically significant but marginal changes were observed in haemoglobin, potassium, and serum creatinine levels (p<0.05) following therapy, while no significant changes were noted in platelet and WBC counts. Overall, Teicoplanin was widely utilized for Gram-positive coverage in ICU settings and demonstrated a favourable safety profile with acceptable clinical outcomes.
The discovery of antibiotics is considered one of the greatest medical breakthroughs of the twentieth century, although antimicrobial substances from natural sources were used empirically long before their mechanisms were understood(1,2).
Teicoplanin, a lipoglycopeptide antibiotic, is especially effective against Gram-positive organisms, including MRSA(3,4). It offers several advantages over Vancomycin and Linezolid, such as reduced nephrotoxicity, once-daily dosing, and better tissue penetration(5-7). Its role in central line-associated bloodstream infections (CLABSI) is notable, particularly in antibiotic-lock therapy and systemic treatment(8). Approved in the year 1997 for use in India but not by the US FDA, Teicoplanin is used to treat sepsis, endocarditis, osteomyelitis, and febrile neutropenia(9,10). Its long half-life and flexible administration route (IV/IM) make it suitable for outpatient therapy(11). Pharmacokinetically, it shows high protein binding, renal elimination, and minimal metabolism(12). Adverse effects include leukopenia, rash, and rare hypersensitivity reactions(13).
RATIONALE
Literature review showed that Teicoplanin is gaining popularity as a promising antibiotic to treat gram positive infections in ICU patients. This study is aimed at understanding Teicoplanin usage and dosage patterns in ICUs of tertiary care hospital.
METHODOLOGY
The aim of the study was to observe and understand the different usage and dosage patterns of Teicoplanin prescribed in intensive care unit (ICU) patients. The study included ICU patients aged above 18 years who were initiated on Teicoplanin therapy. Patients below 18 years of age, pregnant and lactating women, and patients who were not willing to provide informed consent were excluded from the study.
This is a prospective observational study which was conducted for 6 months in a tertiary care hospital. Our sample size was 250. Patients who were initiated on Teicoplanin were enrolled after consent was obtained from either the patient or his/her legally accepted relative.
Data were recorded using a structured data collection form, which was designed to capture demographic details, comorbidities, medical history, Teicoplanin dosage and duration, relevent laboratory parameters, and clinical outcomes. Information was collected from prescription charts and through physician interaction, starting from the day of Teicoplanin initiation until it is discontinued or patient discharged.
Data collection was carried out across different ICUs. Laboratory investigations (serum creatinine, electrolytes, complete blood count), dosage adjustments, and any newly occurring clinical events were recorded on daily bases. All collected data were tabulated in a Microsoft Excel sheet and subsequently analysed using SPSS software for descriptive statistics and evaluation of Teicoplanin prescribing patterns.
RESULTS AND DISCUSSION:
The following are the results acquired from the 250 patients.
The study population consisted of 250 participants, with the majority belonging to the 60 and above age group (127 participants), while 123 participants were from the 18–59 age group. In terms of gender distribution, out of 250 participants, 60% were male and 40% were female, and admissions to ICUs were observed to be predominantly among males.
DIAGNOSIS BASED TEICOPLANIN PRESCRIPTIONS
Table 1: Types of diagnosis of the participants
This table represents the breakdown number of participants with different diagnosis, who were initiated on Teicoplanin.
|
Type of diagnosis |
No of participants |
|
Sepsis |
70 |
|
Septic shock |
62 |
|
Sepsis with septic shock |
11 |
|
Encephalopathy |
20 |
|
ACS |
7 |
|
Heart failure |
4 |
|
Respiratory failure |
15 |
|
Liver failure |
1 |
|
Kidney disease |
6 |
|
COPD |
4 |
|
DM |
20 |
TEICOPLANIN DOSING PATTERNS
Table 2: Teicoplanin dosage patterns distribution among the participants
|
Doses |
No. Of patients |
Percentage |
Dose adjustments |
|
400mg |
182 |
73% |
NO |
|
800mg |
40 |
16% |
NO |
|
600mg |
10 |
4% |
NO |
|
400mg-800mg |
8 |
3% |
YES |
|
800mg-400mg |
9 |
4% |
YES |
|
600mg-400mg |
1 |
0% |
YES |
From this table it is evident that 73% of the participants received 400mg dose and 16% received 800mg, 4% received 600mg. Doses increased to 800 and decreased to 400 for 3% and 4% of the participants each.
TEICOPLANIN FREQUNECY PATTERNS
Table 3: Frequency of Teicoplanin prescribed
|
Frequency |
No.of patients |
Percentage |
|
OD |
28 |
12% |
|
BD |
117 |
46% |
|
BD to OD |
98 |
40% |
|
OD to BD |
7 |
2.50% |
This table shows the various frequencies of Teicoplanin prescribed. BD (2 times per day) was the most common frequency noted and OD (once daily) was least prescribed. Conversion from OD to BD is also observed in 7 patients and BD to OD is observed in 98 patients due to different clinical reactions.
TEICOPLANIN THERAPY DURATION
Table 4: Duration treatment of the participants
|
Number of days |
Number of participants |
|
1 |
41 |
|
2 |
98 |
|
3 |
40 |
|
4 |
29 |
|
5 |
22 |
|
6 |
14 |
|
7 |
8 |
|
8 |
4 |
|
9 |
3 |
|
10-14 |
7 |
From the table it is evident that the duration of the treatment ranged from 1 day to 14 days, in some patients started as empirical therapy and in some patients it was a full therapeutic usage. We found that 41 patients were given just for 1 day and 98 patients were given for 2 days and only 7 patients were able to complete the therapy beyond the 10 days and all others were less than 10 days. The therapy was discontinued in majority of patients after 3 days.
EFFECT ON HAEMOGLOBIN
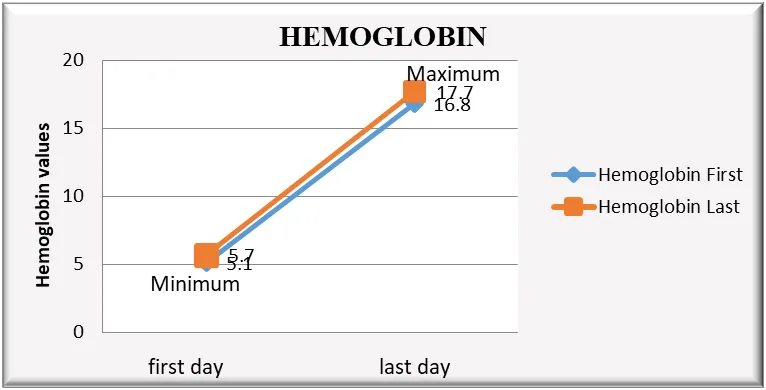
Figure 1: Graph represents Haemoglobin values from pre and post Teicoplanin therapy.
The study data was analysed using Paired T- test. The alternative (H1) & null (H0) and hypothesis as per our assumptions in every statistical analysis were:
HO = No significant variance observed in haemoglobin levels before & after Teicoplanin treatment.
H1= significant variance observed in haemoglobin levels before & after Teicoplanin treatment.
In dependent T test, P value is considered for accepting or rejecting the assumptions:
If P=<0.05 H0 is rejected, as P=0.0002<0.05 H0 is rejected
H1 is accepted, indicating that a statistically significant difference or effect is present.
EFFECT ON PLATELET COUNT

Figure 2: Graph representing the change in the platelet count during Teicoplanin therapy
Here data was analysed using Paired T- test. The alternative (H1) & null (H0) and hypothesis as per our assumptions in every statistical analysis were:
HO = No significant variance observed in platelet count before and after Teicoplanin treatment.
H1= significant variance observed in platelet count before and after Teicoplanin treatment.
In dependent T test, P value is considered for accepting or rejecting the assumptions:
If P=<0.05 H0 is rejected, as P=0.2989>0.05 H0 is accepted
H1 is rejected, indicating that therapy does not affect the platelet count in our study.
EFFECT ON WBC COUNT

Figure 3: Graph representing the change in the WBC count during Teicoplanin therapy
In the study data was analysed using Paired T- test. The alternative (H1) & null (H0) hypothesis as per our assumptions in every statistical analysis were:
HO = No significant variance observed in WBC count before & after Teicoplanin treatment.
H1= significant variance observed in WBC count before & after Teicoplanin treatment.
In dependent T test, P value is considered for accepting or rejecting the assumptions:
If P=<0.05 H0 is rejected, as P=0.0832>0.05 H0 is accepted
H1 is rejected, indicating that therapy does not affect the platelet WBC count in the study.
EFFECT ON POTASSIUM LEVELS
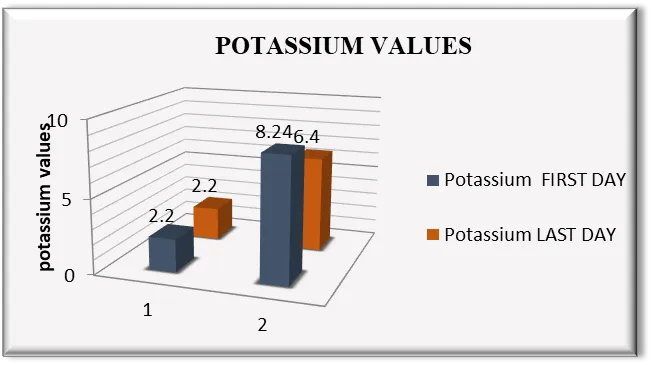
Figure 4: Graph represents the effect potassium levels participants from first day to last day of Teicoplanin therapy
In the study data was analysed using Paired T- test. The alternative (H1) & null (H0) hypothesis as per our assumptions in every statistical analysis were:
HO = No significant variance observed in potassium values before & after Teicoplanin treatment.
H1= significant variance observed in potassium values before & after Teicoplanin treatment.
In dependent T test value of P is considered for accepting or rejecting the assumptions:
If P=<0.05 H0 is rejected, as P=0.0002<0.05 H0 is rejected
H1 is accepted, indicating that a statistically significant difference or affect is present.
EFFECT ON SERUM CREATININE
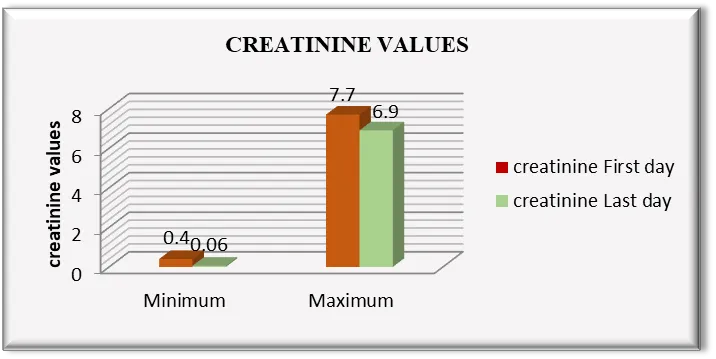
Figure 5: Graph represents the serum creatinine of participants from the initiation and termination of Teicoplanin therapy.
In the study data was analysed using Paired T- test. The alternative (H1) & null (H0) hypothesis as per our assumptions in every statistical analysis were:
HO = No significant variance observed in creatinine values before & after Teicoplanin treatment.
H1= significant variance observed in creatinine values before & after Teicoplanin treatment which is not clinically significant.
In dependent T test, P value is considered for accepting or rejecting the assumptions:
If P=<0.05 H0 is rejected, as P=0.0001<0.05 H0 is rejected
H1 is accepted, indicating that a statistically significant difference or effect is present which is again clinically not significant.
TEICOPLANIN IN DIALYSIS PATIENTS
The distribution of patients based upon their dialysis status showed that 28 participants (11% ) underwent dialysis and the others 222 participants (89%) were not on dialysis. No additional dose was prescribed post haemodialysis. From this it is evident that, this drug is not dialyzable and there is no loss of drug during haemodialysis.
CLINICAL OUTCOMES FOLLOWING TEICOPLANIN THERAPY
From the study it was found that out of 250 participants, 151 participants were shifted to step down facilities, 88 participants died due to various reasons and 11 participants were Discharged Against Medical Advice (DAMA).
CONCLUSION
This prospective observational study was carried out to understand the usage and dosing patterns of Teicoplanin in ICU patients in a tertiary care hospital. Data were obtained from 250 participants, with a higher proportion of males (60%) and individuals aged 60 years and above. The most frequent indication was sepsis, followed by septic shock. Teicoplanin was found to be predominantly prescribed at a dose of 400 mg (73%) with twice-daily (BD) frequency, and most patients received therapy for 1–3 days.
A statistically marginal difference was observed in haemoglobin (p = 0.0002), potassium (p = 0.0002), and serum creatinine (p = 0.001) values, while no significant differences were observed in platelet count (p = 0.2989) and WBC count (p = 0.0832). The overall p-value of the study was found to be < 0.05, indicating that Teicoplanin therapy produced a statistically significant effect on certain biochemical parameters.
As no additional dose was prescribed post dialysis it confirms that Teicoplanin is a not dialyzable drug. The majority of patients (55%) were shifted to step-down care, whereas 34% succumbed to illness due to various comorbidities. It may therefore be concluded that Teicoplanin was effectively utilized across ICUs with appropriate clinical outcomes, with marginal electrolyte changes but insignificant haematological effects. Timely initiation of Teicoplanin with proven culture and sensitivity test along with proper dosing can optimize efficacy and safety in critically ill patients.
CHALLENGES
STUDY OUTCOMES
This study helped us in understanding the clinical outcomes and Teicoplanin therapy in ICU patients. It is found to be a promising option in treating gram positive organism. It has minimal or no effect on important biochemical and haematological parameters. Further, being a non-dialyzable drug, no dose adjustment is needed for patients under new hemodialysis. The Antibiotic Stewardship Program was a great help in improving patient safety through optimized use of Teicoplanin.
ABBREVIATIONS
ACS – Acute Coronary Syndrome; ADR – Adverse Drug Reaction; CLABSI – Central Line–Associated Bloodstream Infection; COPD – Chronic Obstructive Pulmonary Disease; DAMA – Discharged Against Medical Advice.
ACKNOWLEDGEMENTS
The authors express their sincere gratitude to the hospital management for permitting this study and to the ICU medical and nursing staff for their continuous cooperation. We also thank the Department of Pharmacy Practice of Sri Venkateshwara College Of Pharmacy and our faculty guides for their valuable guidance and support. Finally, we acknowledge the patients and their caregivers for their participation and cooperation.
ETHICS
The study protocol was reviewed and approved by the Institutional Ethics Committee of Apollo Hospitals, Jubilee Hills, Hyderabad. The study was conducted in accordance with ethical standards, and informed consent was obtained from all participants or their legally authorized representatives.
REFERENCES


M. Nisar Ahamed, Prasanna Valluri, Nikitha Chidurala, Bandhal Vinod Mounika, Issac Illuri, Venkat Ramesh, A Prospective Observational Study On Usage Patterns Of Teicoplanin In Different Intensive Care Units Of A Tertiary Care Hospital, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 7291-7299, https://doi.org/10.5281/zenodo.21033901
 10.5281/zenodo.21033901
10.5281/zenodo.21033901