
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Ezhuthachan College of Pharmaceutical Sciences, Marayamuttom Neyyattinkara, Thiruvananthapuram
Acute immune-mediated demyelinating disease is an acute immune-mediated inflammatory demyelinating disorder of the central nervous system that predominantly affects children and young adults. Spinal cord involvement may occur in some cases and can contribute to significant neurological deficits. We report a rare case of multifocal demyelination involving both the brain and spinal cord in a pediatric patient presenting with acute onset fever, altered sensorium, seizures, limb weakness, and impaired motor function following a preceding febrile illness. Magnetic resonance imaging revealed multifocal hyperintense demyelinating lesions involving the cerebral white matter along with extensive spinal cord involvement suggestive of an acute inflammatory demyelinating process. Cerebrospinal fluid and laboratory investigations aided in excluding infectious and other autoimmune etiologies. The patient was managed with corticosteroid therapy and supportive care, resulting in gradual clinical improvement. This case highlights the importance of early recognition of acute demyelinating disorders with spinal involvement, timely neuroimaging, and prompt initiation of immunomodulatory therapy to reduce neurological morbidity and improve clinical outcomes.
Acute immune-mediated demyelinating disease is an acute immune-mediated inflammatory demyelinating disorder of the central nervous system characterized by widespread demyelination involving the brain and, occasionally, the spinal cord. It is predominantly a monophasic illness affecting the paediatric population and commonly develops following viral or bacterial infections. The disorder is characterized by multifocal neurological deficits associated with encephalopathy resulting from inflammation and destruction of myelin within the central nervous system[1].
The exact etiology of ADEM remains unclear; however, it is commonly associated with antecedent infections such as upper respiratory tract infections, influenza, measles, mumps, varicella, Epstein–Barr virus infection, and other viral illnesses. In some cases, vaccination may act as a triggering factor. Children and young adults are more frequently affected due to heightened immune responsiveness. Additional risk factors include recent febrile illness, genetic susceptibility, immune dysregulation, and exposure to infectious agents capable of inducing autoimmune responses against neural tissues[2].
The pathogenesis of ADEM is believed to involve an autoimmune-mediated inflammatory response triggered by molecular mimicry between microbial antigens and myelin proteins. Following exposure to an infectious or immunological trigger, autoreactive T lymphocytes cross the blood–brain barrier and initiate inflammation within the central nervous system. This inflammatory process results in perivenular infiltration, edema, and destruction of myelin sheaths leading to multifocal demyelinating lesions involving the cerebral white matter, basal ganglia, brainstem, cerebellum, and spinal cord[3].
Clinically, ADEM presents with rapid onset neurological manifestations including fever, headache, vomiting, altered sensorium, seizures, irritability, focal neurological deficits, motor weakness, gait disturbances, visual impairment, and features of myelopathy in cases with spinal cord involvement. Severe cases may progress to respiratory compromise, quadriparesis, or coma. Complications associated with the disease include persistent neurological deficits, cognitive impairment, recurrent seizures, motor dysfunction, bladder and bowel disturbances, and rarely mortality if diagnosis and treatment are delayed[4].
Diagnosis of ADEM is primarily based on clinical presentation, neurological examination, and characteristic neuroimaging findings. Magnetic resonance imaging is the investigation of choice and typically demonstrates multifocal hyperintense lesions involving the white matter of the brain and spinal cord on T2-weighted and FLAIR sequences. Cerebrospinal fluid analysis may reveal mild lymphocytic pleocytosis and elevated protein levels. Additional laboratory investigations are essential to exclude infectious encephalitis, multiple sclerosis, neuromyelitis optica spectrum disorders, metabolic disorders, and other autoimmune encephalopathies[5].
Management of ADEM mainly involves immunomodulatory therapy and supportive care. High-dose intravenous corticosteroids are considered the first-line treatment to reduce inflammation and promote neurological recovery. Intravenous immunoglobulin and plasmapheresis may be considered in steroid-resistant or severe cases. Symptomatic management includes antiepileptic therapy for seizures, physiotherapy for motor rehabilitation, nutritional support and close monitoring of neurological and respiratory status. Early initiation of therapy is associated with improved clinical outcomes and reduced long-term neurological sequelae[6].
Multifocal demyelination involving both the brain and spinal cord represents a rare and diagnostically challenging presentation of ADEM due to its overlap with infectious, autoimmune, and other demyelinating disorders. Prompt recognition through clinical and radiological evaluation is crucial for timely therapeutic intervention and favorable prognosis[7].
Here, we report a rare case of multifocal demyelination involving the brain and spinal cord in a pediatric patient, highlighting its clinical presentation, diagnostic approach, therapeutic management and outcome.
CASE PRESENTATION
A 5 years old male child was presented with an c/o fever × 3 days and the child had an history of one episode of seizure lasted for one minute,uprolling of eyes associated with deviation of angle of mouth to left side, vomiting × 5 days, headache × 3 days, abdominal pain ×3 days and cough.
The laboratory investigation report showed elevated parameters are ALP, CRP and declined parameters were polymorphs. CSF fluid examination showed presence of high percentage of lymphocytes, sugar and protein and low percentage of WBCs and polymorphs.
MRI brain report showed abnormal T2/FLAIR hyperintense signals involving the bilateral capsuloganglionic regions, mainly affecting the lentiform nucleus and caudate nucleus, along with subtle involvement of the bilateral fronto-parietal cortical and subcortical regions. These hyperintense areas indicate inflammation or demyelination within the brain tissue. The remaining brain structures, including the ventricles, thalami, corpus callosum, brainstem, cerebellum, pituitary gland, and optic pathways, appear normal, with no evidence of diffusion restriction, hemorrhage, mass effect, or midline shift. Based on the imaging findings, the radiological impression favors Acute Disseminated Encephalomyelitis (ADEM) rather than acute viral encephalitis. ADEM is an immune-mediated inflammatory demyelinating disorder that commonly occurs in children following infections or vaccinations and can present with symptoms such as weakness, altered sensorium, or neurological deficits. Clinical and biochemical correlation was advised to confirm the diagnosis and exclude infectious causes.

Figure 1: MRI Brain Report
MRI whole spine revealed straightening of the cervical and lumbar spine curvature with loss of normal lumbar lordosis. Linear T2 hyperintense signals were noted along the anterior aspect of the spinal cord, predominantly involving the mid cervical and mid to lower dorsal regions, suggestive of inflammatory or demyelinating changes within the spinal cord. The vertebral bodies, posterior elements, facet joints, marrow signal intensity, and paravertebral soft tissues appeared normal, with no focal vertebral abnormalities identified. Based on the imaging findings, the possibility of an inflammatory demyelinating disorder such as acute disseminated encephalomyelitis (ADEM) or transverse myelitis was considered and clinical correlation was recommended.
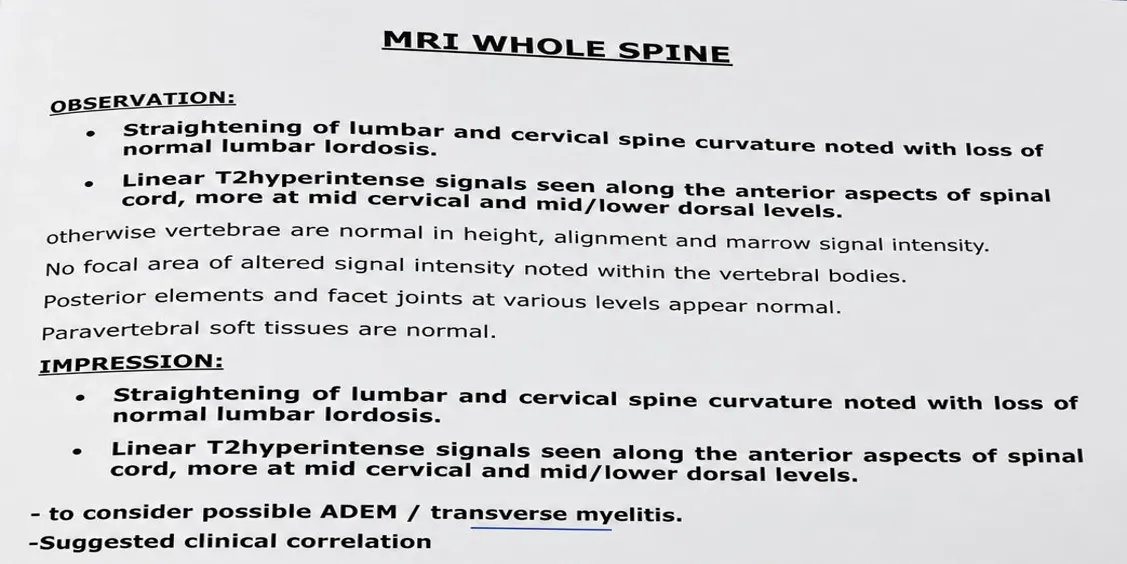
Figure 2: MRI Spine Report
The child was treated with SYRUP TRICLOFOS SODIUM 10ml P/O BD, SYRUP PARACETAMOL 5ml P/O BD, INJECTION CEFTRIAXONE 1.1gm IV BD, INJECTION ACYCLOVIR 230 mg IV Q8H, SYRUP AZITHROMYCIN 5ml P/O OD, INJECTION PANTOPRAZOLE 40mg IV OD, INJECTION LEVETIRACETAM 220 mg IV BD, NEBULIZATION LEVOSALBUTAMOL+ OXYGEN P/N Q8H, TABLET DOPXYCYCLINE 100 mg P/O 1/2 BD and INJECTION METHYL PREDNISOLONE 600 mg IV OD.
DISCUSSION
Multifocal demyelination involving both the brain and spinal cord represents a diagnostically challenging and clinically heterogeneous spectrum of inflammatory demyelinating disorders. The present case demonstrates simultaneous multifocal central nervous system (CNS) involvement with radiological evidence of demyelinating lesions affecting cerebral and spinal structures, thereby broadening the differential diagnosis to include acute disseminated encephalomyelitis (ADEM), multiple sclerosis (MS), neuromyelitis optica spectrum disorder (NMOSD) and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD). Similar overlap syndromes have increasingly been described in recent literature, emphasizing the need for careful clinical, radiological, serological and therapeutic evaluation[8].
In comparison with the case reported by Roy et al[9]. the present case shares the characteristic presence of extensive brain lesions associated with longitudinal spinal cord involvement. However, their patient was ultimately diagnosed with aquaporin-4 antibody-positive NMOSD with tumefactive demyelinating lesions mimicking multiple sclerosis. In contrast, the current case demonstrated multifocal demyelinating lesions without classical relapsing optic neuritis or definitive diagnostic features of NMOSD, thereby highlighting the diagnostic ambiguity that frequently accompanies overlapping inflammatory demyelinating disorders.
Spiezia et al[10]. described a rare double-positive AQP4 and MOG antibody-associated demyelinating disorder involving both central and peripheral nervous systems. Similar to their report, the present case demonstrated multifocal CNS involvement with simultaneous brain and spinal cord lesions. However, peripheral nervous system manifestations were absent in our patient. Their study further emphasized the importance of antibody testing in differentiating atypical demyelinating disorders from classical multiple sclerosis. The absence or unavailability of specific antibody markers in many resource-limited settings may therefore complicate accurate categorization of such rare presentations.
Several previously published reports of MOG antibody-associated disease have demonstrated combined brainstem and spinal cord demyelination similar to the current case. In the report by Kato et al[11]. extensive brainstem lesions associated with MOGAD presented with multifocal neurological deficits and radiological abnormalities involving the pons and cerebellar peduncle. Although our patient also demonstrated multifocal CNS involvement, the distribution of lesions extended beyond the brainstem into wider cerebral and spinal regions, suggesting a more diffuse inflammatory process.
Comparatively, studies evaluating tumefactive demyelinating lesions have shown that multifocal lesions involving both cerebral hemispheres and spinal cord are often difficult to distinguish from infectious, neoplastic, or autoimmune etiologies. Wang et al[12]. observed that patients with tumefactive demyelination frequently developed later diagnoses of MOGAD, NMOSD, or MS after longitudinal follow-up. Similar diagnostic uncertainty was observed in the present case, where neuroimaging initially raised broad differentials including inflammatory demyelination, infectious encephalomyelitis, and autoimmune pathology.
The present case also resembles recurrent ADEM-like disorders described in adults. In the case presented by Lee et al[13]. recurrent fulminant ADEM-like episodes occurred despite negative neuronal and glial antibodies. Their report emphasized that adult-onset multifocal demyelination may not always fit conventional diagnostic criteria for MS or NMOSD. Likewise, the current case demonstrated overlapping radiological and clinical features without definitive categorization during the initial presentation.
Comparison with pediatric and adult MOGAD-associated ADEM cases further supports the evolving understanding of multifocal demyelination syndromes. Jurynczyk et al[14]. reported that MOG-associated disorders frequently present with diffuse bilateral brain lesions and longitudinally extensive transverse myelitis. Similar radiological patterns were identified in our patient, particularly the coexistence of extensive cerebral lesions with spinal cord involvement. However, unlike classical pediatric ADEM, the current case lacked profound encephalopathy, thereby making differentiation from other inflammatory demyelinating disorders more challenging.
Another important comparison can be made with patients exhibiting recurrent demyelinating disease after initial monophasic episodes. Reports evaluating MOGAD and atypical CNS demyelination have demonstrated that relapses are increasingly recognized, especially in adults. Failure of conventional disease-modifying therapies, as described by Cobo-Calvo et al[15]. in MOGAD patients treated with alemtuzumab, highlights the therapeutic complexity of atypical demyelinating syndromes. In the present case, close long-term monitoring is essential because recurrence or evolution into a defined neuroimmunological disorder remains possible.
The radiological characteristics observed in this case also parallel findings reported in MOGAD and NMOSD cohorts, where lesions commonly involve deep white matter, brainstem, periventricular regions, and long spinal segments. MRI findings remain crucial for differentiating inflammatory demyelination from infectious myelitis, vasculitis, lymphoma, and metabolic disorders. The simultaneous involvement of brain and spinal cord in our patient strongly supported a diffuse immune-mediated demyelinating pathology[16].
Therapeutically, most reported cases of multifocal CNS demyelination responded favorably to high-dose corticosteroids, plasma exchange, intravenous immunoglobulin, or rituximab depending on disease severity and underlying antibody profile. Similar therapeutic approaches were considered in the present case. Early initiation of immunotherapy is important to reduce inflammation, prevent irreversible axonal injury, and improve neurological recovery. Nevertheless, treatment-related challenges remain significant because atypical demyelinating disorders frequently exhibit unpredictable clinical courses and variable responses to immunomodulatory therapy[17].
Overall, the present case contributes to the growing body of evidence regarding rare multifocal demyelinating disorders involving both the brain and spinal cord. Comparison with previously reported cases demonstrates substantial overlap among ADEM, MOGAD, NMOSD, and tumefactive demyelinating syndromes. This overlap emphasizes the importance of early neuroimaging, cerebrospinal fluid analysis, autoimmune antibody testing, and long-term clinical follow-up for accurate diagnosis and optimal therapeutic management. Recognition of such rare presentations is essential to avoid diagnostic delay, inappropriate treatment, and long-term neurological disability.
CLINICAL SIGNIFICANCE
Multifocal demyelination involving both the brain and spinal cord represents a rare and clinically significant neurological condition characterized by widespread inflammatory damage to the myelin sheath within the central nervous system. Simultaneous cerebral and spinal cord involvement often leads to diverse neurological manifestations including motor weakness, sensory deficits, altered consciousness, visual disturbances, seizures, ataxia, and autonomic dysfunction. The overlap of symptoms with other neurological disorders such as multiple sclerosis, neuromyelitis optica spectrum disorder, acute disseminated encephalomyelitis, infectious encephalitis, and metabolic encephalopathies makes early diagnosis particularly challenging. Early recognition through neuroimaging and cerebrospinal fluid analysis is essential because delayed diagnosis may result in irreversible neurological deficits and long-term disability.
The rarity of multifocal demyelination with combined brain and spinal cord lesions highlights the importance of documenting such cases to improve current understanding of disease presentation, radiological patterns, therapeutic response, and prognosis. MRI findings demonstrating multifocal hyperintense lesions in both cerebral white matter and spinal cord regions provide crucial diagnostic clues and help differentiate inflammatory demyelination from neoplastic, vascular, or infectious etiologies. Timely initiation of immunomodulatory therapy, especially high-dose corticosteroids, may significantly improve neurological recovery and reduce disease progression.
This case also emphasizes the importance of a multidisciplinary approach involving neurologists, radiologists, clinical pharmacists, physiotherapists, and rehabilitation specialists for optimal patient management. Long-term follow-up is necessary because some patients may later develop recurrent demyelinating disorders such as multiple sclerosis or neuromyelitis optica spectrum disorder. Reporting rare presentations contributes to the growing body of evidence required for establishing standardized diagnostic and therapeutic protocols.
THERAPEUTIC CHALLENGES
Management of multifocal demyelination involving the brain and spinal cord presents several therapeutic challenges due to the heterogeneity of clinical presentation, uncertain etiology, and lack of universally established treatment guidelines. One major challenge is differentiating inflammatory demyelination from infectious, autoimmune, neoplastic, or metabolic disorders before initiating immunosuppressive therapy. Administration of corticosteroids in undiagnosed infections may worsen the patient’s condition; therefore, careful exclusion of infectious causes is critical prior to treatment initiation.
Another challenge lies in the variability of treatment response. Although high-dose intravenous corticosteroids remain the first-line therapy, some patients demonstrate incomplete neurological recovery or steroid resistance, necessitating escalation to intravenous immunoglobulin or plasmapheresis. The decision regarding second-line therapy depends on disease severity, lesion burden, and clinical progression, which may vary considerably among patients. Monitoring therapeutic effectiveness can also be difficult because radiological improvement may not always correlate with clinical recovery.
Long-term management poses additional difficulties, particularly in preventing relapse and minimizing neurological sequelae. Persistent motor deficits, gait disturbances, neuropathic pain, bladder dysfunction, cognitive impairment, and psychological stress may significantly affect quality of life and require prolonged rehabilitation. Adverse effects associated with prolonged corticosteroid use, including immunosuppression, hyperglycemia, osteoporosis, and gastrointestinal complications, further complicate management. Limited availability of disease-specific treatment protocols for rare multifocal demyelinating disorders highlights the need for individualized patient-centered therapeutic strategies and continued clinical research.
CONCLUSION
This case highlights a rare presentation of multifocal demyelination involving both the brain and spinal cord, emphasizing the diagnostic complexity and therapeutic challenges associated with extensive central nervous system demyelinating disorders. The coexistence of multifocal cerebral and spinal cord lesions produced diverse neurological manifestations that required careful clinical evaluation, radiological assessment, and exclusion of infectious, autoimmune, metabolic, and neoplastic etiologies. Early neuroimaging and prompt initiation of appropriate immunomodulatory therapy played a crucial role in improving clinical outcome and preventing further neurological deterioration.
The case underscores the importance of maintaining a high index of suspicion for inflammatory demyelinating disorders in patients presenting with acute multifocal neurological deficits. A multidisciplinary approach involving neurologists, radiologists, clinical pharmacists, and rehabilitation specialists is essential for accurate diagnosis, effective management, and long-term follow-up. Documentation of such rare presentations contributes valuable clinical evidence to the existing literature and may aid in improving future diagnostic and therapeutic strategies for complex demyelinating disorders involving both the brain and spinal cord.
REFERENCES


Ardra S A, Grace N Raju, Shaiju S Dharan, A Rare Case of Multifocal Demyelination Involving the Brain and Spinal Cord, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 994-1002. https://doi.org/10.5281/zenodo.20532440
 10.5281/zenodo.20532440
10.5281/zenodo.20532440