
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy Practice, JSS College of Pharmacy, Ooty
Background: Fixed drug eruption (FDE) is a common adverse cutaneous reaction to drugs, but it is a complex and unusual diagnostic and clinical scenario that is not often encountered, particularly in the same patient for whom nephrolithiasis, stasis eczema and history of urinary tract intervention occur. Case Summary: A 48-year-old male chronic alcoholic, chronic smoker for 15 years, with bilateral renal calculi managed by RIRS + DJ stenting (in October 2025) and DJS exchange under anaesthesia in October 2025, presented in OPD of dermatology department at Government Medical College Hospital, The Nilgiris with one month history of well-defined bullous lesions present over bilateral palms on hyperpigmented skin with one hyperpigmented plaque over right leg (4x5 cm), one oral erosion (1x1 cm) over lower lip. The diagnosis was confirmed by dermatological evaluation (Fixed Drug Eruption due to Aceclofenac, differential diagnosis: Stasis Eczema). Urology work up (USG abdomen) showed tiny left renal calculi, fatty liver (Grade I), and a 2.4x2.3 cm cortical cyst in the upper pole of the left kidney and urine analysis was positive for sub clinical UTI with mild pus cells (6-8/HPF) and occasional bacteria. Conclusion: This case points out the need for being vigilant in FDE after urological procedures in patients using NSAIDs, the overlapping presentations of dermatological conditions, and the need for a multi-disciplinary approach. The use of the underreported FDE inducing agent aceclofenac is discussed in the context of the continuing urological disease.
Fixed drug eruption (FDE) is a unique type of cutaneous adverse drug reaction with the development of recurrence of lesions in the same body locations after re-exposure to the drug. Classically, FDE manifests as sharply delineated, round to oval erythematous or violaceous plaques which leave behind post-inflammatory hyperpigmentation, as described by Bourns in 18891. Then the vesicles or bullae filled with fluid develop on top of the hyperpigmented macules, which further increase the diagnostic possibilities and should be distinguished from Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) and pemphigoid2.
The non-steroidal anti-inflammatory drugs (NSAIDs), such as aceclofenac, are the most commonly reported drug classes involved in FDE worldwide3,4. Aceclofenac, a potent COX-2 preferring inhibitor is very commonly used in India for musculoskeletal pain and for post procedural analgaesis after urological procedures like DJ stenting and RIRS. Though widely used, aceclofenac induced FDE is not as reported as other NSAIDs like ibuprofen and diclofenac in literature5.
The presence of FDE in conjunction with stasis eczema, nephrolithiasis, renal cortical cyst and history of prior urological surgeries in a chronic alcoholic patient presents a very challenging clinical picture. There is no systematic literature about the interaction between impaired renal function, altered drug metabolism, chronic alcohol use and cutaneous hypersensitivity to drugs. This case report proposes to document this uncommon multisystem presentation, to understand the pharmacologic background of aceclofenac induced FDE and to suggest a diagnostic and therapeutic approach for cases in various clinical scenarios.
2. Case Presentation
2.1 Patient Demographics and History
Mr. Manikandan appeared at the Department of Dermatology, Venereology and Leprosy (DVL) at the Government Medical College Hospital, The Nilgiris on June 5-6, 2026 and was aged 48 years. He was referred from the Urology OPD of Sree Abirami Hospital, Coimbatore, under follow-up for bilateral urolithiasis after 10 months. He was a 10-months follow-up patient in Urology OPD, Sree Abirami Hospital, Coimbatore.
His urological past included: (1) Bilateral RIRS + DJS done on October 6, 2025, for Left UU Calculus; (2) Left DJS exchange under anaesthetic on October 27, 2025 (with documentation of pullout/reinsertion); and (3) 7-month follow-up. He came to urology with new onset left flank pain of 1 month duration, without any dysuria. Urology provided uroprotective agents and imaging was arranged.
Alcoholic for 15 years and a smoker for 15 years. Personal history included normal bowel and bladder habits, and normal appetite and sleeping pattern. No dyspnea nor chest sign history.
2.2 Dermatological Presentation
At the time of examination at the DVL department, the patient was conscious, oriented, and had a good hydration status without fever. Vital signs were: BP 130/80 mmHg, SpO2 94%, PR 68 bpm. Systemic: CNS S1S2+, RS BLAE+, P/A Soft BS+, CNS NFND.
Dermatological exam (D/E) showed:

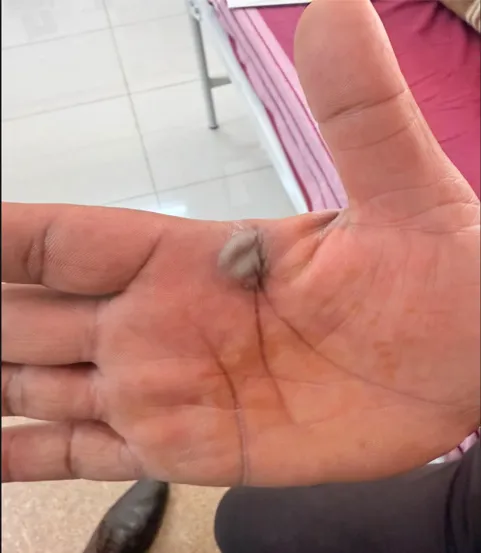
Figure 1. Fixed drug eruption: Cutaneous reactions.
(A)Clearly visible tense bulla with hyperpigmentation around the bulla on the palm side of the hand. (B) Residual hyperpigmentation with central bullous changes seen on the palm, typical of the fixed drug eruption.
Table 1: Summary of Laboratory Investigations
|
Investigation |
Result |
Normal Range |
Clinical Significance |
|
Urine Colour |
Pale Yellow |
Pale Yellow |
Normal |
|
Urine Appearance |
Slightly Turbid |
Clear |
Suggests infection/inflammation |
|
pH |
6.5 (Acidic) |
5.0–7.5 |
Normal |
|
Specific Gravity |
1.010 |
1.005–1.020 |
Normal hydration |
|
Albumin |
Nil |
Nil |
No renal protein loss |
|
Sugar |
Nil |
Nil |
No glycosuria |
|
Bile Salts/Pigments |
Negative |
Negative |
No hepatobiliary disease |
|
Ketone Bodies |
Negative |
Negative |
Normal |
|
Nitrite |
Negative |
Negative |
UTI not ruled out by nitrite alone |
|
Pus Cells |
6–8/HPF ▲ |
0–5/HPF |
ELEVATED — suggests subclinical UTI |
|
RBCs |
1–2/HPF |
0–5/HPF |
Normal |
|
Epithelial Cells |
2–4/HPF |
0–5/HPF |
Normal |
|
Bacteria |
Present (occasional) |
Nil |
Indicates subclinical bacteriuria |
Above normal range. HPF = High Power Field. (Sree Abirami Hospital Laboratory Report, 29/05/2026)
2.4 Imaging: USG Abdomen (Abirami Ultra Sonography Centre, 29/05/2026)
Table 2: USG Abdomen Findings — Mr. Manikandan Rao (Age 48/Male, Date: 29/05/2026)
|
Organ |
Findings |
Impression |
|
Liver |
Normal sized, increased echoes, no focal lesions; portal vein and biliary radicles normal. |
Grade I Fatty Liver ▲ |
|
Gallbladder |
Usually distended, with no stones or sludge. |
Normal |
|
Pancreas |
Normal size, shape, echopattern; duct is normal; no calculi. |
Normal |
|
Spleen |
N: 11.3cm, normal size, shape, echopattern |
Normal |
|
Right Kidney |
11.2x5.1cm, normal pelvicalyceal system, present corticomedullary differentiation, no calculi. |
Normal |
|
Left Kidney |
The size is 12.5 x 5.8 cm, and the cavity surrounding the kidney is normal, with a few small stones in the lower pole and a small cyst in the upper pole that measures 2.4 x 2.3 cm. |
Renal calculi, small (left) ▲; Cortical cyst ▲ |
|
Urinary Bladder |
Dilated; normal outline; No thickening/calculus; bilateral jets seen; Post-void residual: Nil. |
Normal |
|
Prostate |
In this case, it is normal size (Volume 16 cc) and echoes. |
Normal |
|
Para-aortic Area |
No swelling of the lymph nodes or presence of fluid in the abdomen/pleural cavity. |
Normal |
▲ Abnormal findings. CT KUB is recommended for further evaluation of calculi.
3. Diagnosis
3.1 Primary Diagnosis
Fixed Drug Eruption (FDE) - Aceclofenac-Induced / Stasis eczema
3.2 Differential Diagnosis
Table 3: Diagnostic Criteria for FDE - Applied to This Case (Based on Mahboob & Haroon, 1998; Lee et al., 2017)
|
Diagnostic Criterion |
Standard |
Present (palms together, leg): |
|
Discrete, round/oval lesion(s) |
Required |
Present |
|
Post-inflammatory hyperpigmentation (PIH) |
Characteristic |
These are small (3x2 to 3x3 cm) and present. |
|
Bullous/vesicular variant |
Severe form |
Present (1x1 cm erosion) |
|
Oral mucosal involvement |
Supports diagnosis |
Aceclofenac used post-DJS |
|
Use the word "use" to refer to the time of a drug's consumption. |
Essential |
Not re-challenged (ethical) |
|
When re-exposed, recurrence at the same site. |
Pathognomonic |
Pending follow-up |
|
At the age of 10, she began to improve after she stopped taking the drugs. |
Expected |
Absent — supports FDE |
|
Non-systemic drug reaction without features (fever, LFT, organ failure) |
FDE vs. SJS/TEN |
Present (palms together, leg): |
4. Management
4.1 Dermatology Treatment (Govt. Medical College Hospital, The Nilgiris)
Table 4: Prescribed Treatment Protocol
|
Drug |
Dose/Route |
Frequency |
Indication |
|
Inj. Dexamethasone |
2 cc IV |
OD |
Acute FDE anti-inflammatory |
|
Inj. Pantocid (Pantoprazole) |
IV |
OD |
GI protection with steroids |
|
Tab. Vitamin C |
250 mg |
0-0 |
Wound healing, antioxidant |
|
Tab. Cetirizine (Cephalexin 500mg?) |
500 mg |
2-2-2 |
Antipruritic/antihistamine |
|
Tab. TPN 4 mg (Trypsin-Papain-Bromelain) |
4 mg |
0.5-0-1 |
Enzymatic debridement, anti-oedema |
|
Silver Sulphadiazine Cream |
External |
B/D |
Bullae/wound antimicrobial |
|
Saline Gauze Dressing |
External |
V-V-V |
Wound management |
|
Clotrimazole + Betamethasone Ointment |
External O/E |
0-0 |
Plaque/eczema management |
|
Tab. Prednisolone (Prednisolone?) |
C/A |
V-V-V |
Stepdown steroid therapy |
Note: Aceclofenac was found to be the cause and was promptly withdrawn. Orders placed: Investigations: USG abdomen + pelvis, Arterial Doppler B/L legs (DVL, 5/6/26).
4.2 Urological Follow-Up
Given the USG findings (small left renal stones, cortical cyst, fatty liver Grade I), a CT KUB was recommended to further characterise the stones. Uroprotective agents were continued on. Urine culture was recommended as active UTI was ruled out due to mildly elevated pus cells. Counselling of dietary modification (low oxalate, increased fluid) was provided.
5. Discussion
5.1 Epidemiology and Pathophysiology of Aceclofenac-Induced FDE
NSAIDs are one of the major groups of drugs responsible for FDE, which make up about 6–16% of all reported cutaneous adverse drug reactions in India6 along with antimicrobials and anticonvulsants. Aceclofenac is a phenylacetic acid derivative with preferential COX-2 inhibition which is one of the most widely used NSAIDs in the Indian subcontinent especially post orthopaedic and urological surgery7.
Immunopathogenesis of FDE involves activation of CD8+ T-lymphocytes at the site of the lesion, which on subsequent re-exposure release mediators of cell-mediated immunity such as perforin and granzyme B, which are responsible for the apoptosis of keratinocytes and the subsequent separation of the epidermis and dermis to form bullae8,9. FDE differs from other drug reactions by the recurrence of the reaction at the same site resulting in “memory T cells” in the dermis and in the epidermis. Studies in recent years have suggested that drug specific MHC-I restricted immune activation and memory intraepidermal effector T cells (CD69+CD103+) are the mechanism10.
FDE has a well-established predilection for involvement of acral sites (palms, soles) for mucosal surfaces. Palmar involvement as in this case can be confusing or difficult to diagnose because of the similar appearance with eczema of palms and soles, pompholyx, and contact dermatitis11.
5.2 Chronological Timeline and Drug Causality Assessment
Table 5: Clinical and Treatment Timeline
|
Date |
Event |
Dermatological Correlation |
|
October 2025 |
RIRS + bilateral DJ stenting, NSAIDs (including aceclofenac) are prescribed for post-op analgesia. |
Initial sensitisation to aceclofenac probably. |
|
October 27, 2025 |
Under anaesthetic DJS changes (pull out + reinsertion), and NSAIDs re-prescribed. |
Second exposure - FDE elicitation will likely occur. |
|
November 2025 onwards |
Follow up at 7 months and continued NSAID use for pain associated with the flanks. |
Accumulation of drug exposure; lesion formation. |
|
May 2026 |
Recurrence of left flank pain; Onset of skin lesions (bullae, plaque, oral erosion) ~1 month. |
The onset of lesions was around 1 month prior to presentation in FDE. |
|
29/05/2026 |
Urology OPD- urine analysis and USG abdomen done at Sree Abirami hospital, Coimbatore. |
Urological work-up; subclinical UTI and calculi diagnosed. |
|
05-06/06/2026 |
DVL department, Govt. Medical College Hospital, The Nilgiris, diagnosed and started treatment for FDE. |
Aceclofenac identified and stopped; treatment begun. |
Causality assessment was done by using the Naranjo Adverse Drug Reaction Probability Scale. The patient's score was +6 due to the following reasons: prior literature regarding aceclofenac-FDE (+1); improvement upon rechallenge (+1); recurrence on continued use (+2); the presence of alternative explanations that were not related to his current disease (+1); objective documentation of drug reaction (+1)12.
5.3 The Significance of Co-existing Urological Disease
Physiologic nephrolithiasis is associated with renal cortical cyst, which adds to the clinically relevant pharmacokinetic consideration. NSAIDs such as aceclofenac are excreted to a large extent by the kidney. Drug hypersensitivity reactions may occur at lower threshold levels due to prolonged plasma levels which can result from impaired renal clearance (due to obstructive uropathy, e.g., from previous DJ stenting or remaining calculi) [13]. The USG shows the fatty liver as Grade I, which further indicates reduced hepatic Phase I metabolism of aceclofenac (CYP2C9) that may lead to increased formation of the reaction metabolites involved in the pathogenesis of FDE14.
Another metabolic risk factor of chronic alcoholism (defined here as 15 years' duration) is CYP2E1 induction and CYP2C9 activity suppression, drug protein binding (decreased albumin), impaired immune regulation, and hepatic steatosis. The “perfect storm” for drug hypersensitivity is the combination of alcohol-related hepatic changes, renal insufficiency, and chronic NSAID use15.
Also worth noting is that stasis eczema features as a differential diagnosis and may also be a co-morbidity. Chronic venous insufficiency (suggested by the DVL team and requires arterial Doppler B/L legs) can result in palmar/plantar eczematous changes, hyperpigmentation, which can mimic or mask FDE. Arterial Doppler was ordered to rule out peripheral arterial disease which may be affecting skin changes on lower extremities16.
5.4 Novelty and Contribution to Literature
Table 6: Comparison with Published Cases of NSAID-Induced FDE
|
Author/Year |
Drug |
Site(s) |
Variant |
Special Features |
Outcome |
|
Bhutani et al. 2018 [3] |
Ibuprofen |
Lips, genitalia |
Non-bullous |
No systemic disease |
Resolution |
|
Nair et al. 2020 [5] |
Aceclofenac |
Trunk, thigh |
Bullous |
No prior surgery |
Resolution |
|
Singh et al. 2021 [17] |
Diclofenac |
Palms, soles |
Non-bullous |
Chronic kidney disease |
Partial resolution |
|
Current Case, 2026 |
Aceclofenac |
B/L palms, R leg, oral |
Bullous + oral + eczema |
Renal calculi, DJ stenting, fatty liver, alcoholism |
Under treatment |
The features of this case which make it different from previous reports are: (1) The temporality with DJ stenting and RIRS procedures where aceclofenac was the main post-operative analgesic, (2) Trifocal FDE (bilateral palms, lower limb, and oral mucosa), which is a rare distribution pattern, (3) Complex pharmacokinetic milieu with the presence of renal calculi, cortical cyst, and Grade I fatty liver, (4) Alcohol use as a modifying factor for drug metabolism and immune response, and (5) The co-existence of features that suggest stasis eczema as an overlapping dermatological condition, which adds to the diagnostic complexity.
6. Patient Perspective
The bilateral bullae caused the patient a great deal of distress and did not allow him to perform his daily routines and work. He did not know that it was the pain medications causing his skin rash as he had thought that the rash was due to an infection or an allergic reaction to some unknown environmental triggers. He explained that the reason for the appearance of the drug, and questioned him about what he would do if he had pain in the future in connection with the condition of his kidneys. Advised about alternative analgesics (paracetamol, tramadol and selective COX-2 inhibitors with caution) and provided with a Medic Alert Card to avoid using Aceclofenac.
7. Conclusions
A rare and clinically complex case of aceclofenac induced bullous fixed drug eruption in a patient with multifaceted urological history, chronic alcoholism and fatty liver Grade 1. The case highlights the following key points in the clinical management of paediatric patients:
8. Learning Points for Clinicians
|
Clinical Point |
Practical Implication |
|
Oral erosion and bullous palms on bilateral palms after NSAID use are clinical features of FDE. |
Always take drug history in bullous skin disease. |
|
Aceclofenac is one of the most frequently reported, but underreported, FDE inducing NSAID in India. |
Consider aceclofenac in all suspected NSAID-FDE in Indian patients. |
|
Drug ADRs are increased with impaired renal/hepatic function. |
Avoid/Do not use NSAIDs in CKD/fatty liver. |
|
Stasis eczema and FDE may occur together, Doppler legs recommended if changes in lower limbs occur. |
Do vascular work up if the diagnosis FDE is made with changes in lower limbs. |
|
Urine culture is indicated in post-stent patients who have pus cells. |
Don't overlook mild pyuria post-urological procedure. |
|
Cortical renal cysts need periodic USG follow up, CT KUB for calculi stratification. |
Important to have a structured urological follow-up plan. |
Disclosures
Conflicts of interest: None declared.
Patient consent: Written informed consent was obtained from the patient for publication of this case report and accompanying clinical photographs.
Ethics approval: This case report was conducted in accordance with the Declaration of Helsinki. Patient data has been de-identified where possible.
REFERENCES

Ranilboopathi S., Kanthimathi Meenal C. T., Naveen N. Prabhu, A Rare Multisystem Presentation of Fixed Drug Eruption Due To Aceclofenac in A Patient with Bilateral Renal Calculi and Stasis Eczema – A Case Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 7345-7354. https://doi.org/10.5281/zenodo.21042397
 10.5281/zenodo.21042397
10.5281/zenodo.21042397