
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1.Dr.M.Prasada Rao, Professor & Principal of M.A.M College of Pharmacy.
2.Dr.Y.Narasimha Rao, Professor , Department of Pharmacology.
3.Dr.S.Rajini, Professor, Department of Pharmacy Practice.
4.G. RAGHU, Pharm D Student of M.A.M College of Pharmacy
Diabetes mellitus”, is one of the most common non-communicable diseases worldwide. India faces several challenges in diabetes management, including a rising prevalence in urban and rural areas, lack of disease awareness among the public, limited health care facilities, high cost of treatment, suboptimal glycaemic control and rising prevalence of diabetic complications. Insulin therapy for diabetes is most commonly delivered via subcutaneous injections, up to four times a day. Long-term insulin therapy, compounded by the invasive nature of its administration, has caused problems with patient compliance, ultimately influencing patient outcomes. There is an increase in the prevalence of type 1diabetes also, but main cause of diabetic epidemic is type2 diabetes mellitus, which accounts for more than 90 percent of all diabetes cases. Type2 diabetes is a serious and common chronic disease resulting from a complex inheritance- environment interaction along with other risk factors such as obesity and sedentary lifestyle.
Diabetes mellitus is taken from the Greek word diabetes, meaning siphon - to pass through and the Latin word mellitus meaning sweet. A review of the history shows that the term "diabetes" was first used by Apollonius of Memphis around 250 to 300 BC. Ancient Greek, Indian, and Egyptian civilizations discovered the sweet nature of urine in this condition, and hence the propagation of the word Diabetes Mellitus came into being. Mering and Minkowski, in 1889, discovered the role of the pancreas in the pathogenesis of diabetes. In 1922 Banting, Best, and Collip purified the hormone insulin from the pancreas of cows at the University of Toronto, leading to the availability of an effective treatment for diabetes in 1922. Over the years, exceptional work has taken place, and multiple discoveries, as well as management strategies, have been created to tackle this growing problem. Unfortunately, even today, diabetes is one of the most common chronic diseases in the country and worldwide. In the US, it remains as the seventh leading cause of death. Insulin and glucagon hormones both are secreted by the pancreas. Insulin is secreted by the beta (ß) cells and glucagon is secreted by the alpha (α) cells both are located in the islets of Langerhan’s. Insulin decreases the blood glucose level by the glycogenesis and transport glucose into the muscles, liver and adipose tissue. Neural tissue and erythrocytes do not required insulin for glucose utilization whereas alpha (α) cells plays an important role in controlling blood glucose by producing the glucagon and it increases the blood glucose level by accelerating the glycogenolysis.
In addition to increased risk of obesity, metabolic and cardiovascular disorders, and malignancy in future life of fetus after delivery [6]. Type II diabetes mellitus comprises 80% to 90% of all cases of diabetes mellitus. Geographical variation can contribute.
in the magnitude of the problems and to overall morbidity and mortality [7, 8]. Moreover, people with diabetes who undertake moderate amounts of physical activity are at inappreciably lower risk of death than inactive persons [24] It is now well established that a specific genetic constitution is required for such an event to cause [9] The growing burden of diabetes and other noncommunicable diseases is one of the major health challenges to economic developments bedeviling WHO African Region states. In diabetes, there is an aberration either in the synthesis or secretion of insulin as seen in Type 1 diabetes mellitus (T1DM) and stenosis in the pancreatic duct, or the development of resistance to insulin or its subnormal production as in the case of Type 2 diabetes (T2DM) and certain secondary diabetes.
Diabetes mellitus (DM) is a metabolic disease, involving inappropriately elevated blood glucose levels. DM has several categories, including type 1, type 2, maturity-onset diabetes of the young (MODY), gestational diabetes, neonatal diabetes, and secondary causes due to endocrinopathies, steroid use, etc. The main subtypes of DM are Type 1 diabetes mellitus (T1DM) and Type 2 diabetes mellitus (T2DM), which classically result from defective insulin secretion (T1DM) and/or action (T2DM). T1DM presents in children or adolescents, while T2DM is thought to affect middle-aged and older adults who have prolonged hyperglycemia due to poor lifestyle and dietary choices. The pathogenesis for T1DM and T2DM is drastically different, and therefore each type has various etiologies, presentations, and treatments.
Classification of Diabetes Mellitus
The first mostly accepted classification of diabetes mellitus was published by WHO in the year 1980 [11] and, it is modified in the year 1985 [12]. The most common and important form of Primary or idiopathic diabetes mellitus, which is focus of our discussion. It must be different from secondary diabetes mellitus which includes forms of hyperglycemia associated with identifiable causes in which destruction of pancreatic islets is induced by inflammatory Pancreatic diseases, surgery, tumors, certain drugs, iron overloaded (Hemochromatosis) and certain acquired or genetic endocrinopathies [1].The classification encompasses both clinical stages and aetiological types of diabetes mellitus and other categories of hyperglycemia [13].
Assigning a type of diabetes to an individual often depends on the circumstances present at the time of diagnosis, and many diabetic individuals do not easily fit into a single class [14]Primary diabetes mellitus probably represents a heterogeneous group of disorders that have hyperglycemia as a common feature [1].
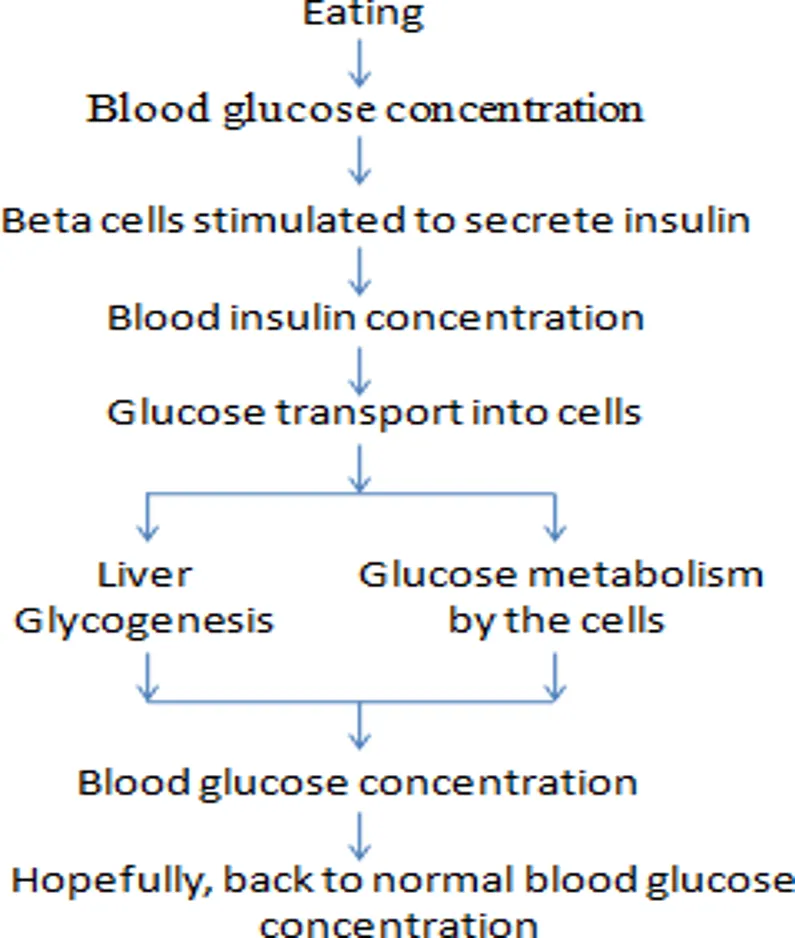
Fig 1: Glucose Metabolism
The new classification of diabetes mellitus contains stages which reflect the various degrees of hyperglycemia in individual subjects with any of the disease processes which may lead to diabetes mellitus.
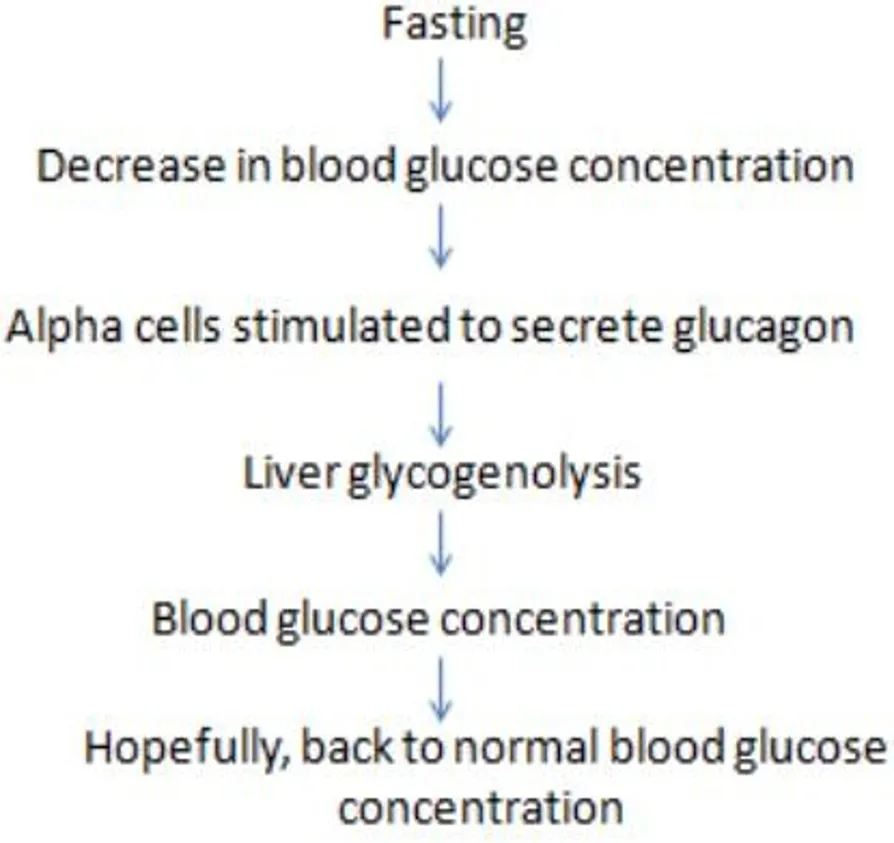
Fig 2: Normal response to fasting
The old and new terms of insulin-dependent(IDDM) or noninsulin-dependent (NIDDM) which were proposed by WHO in1980 and 1985 have disappeared and the terms of new classification system identifies four types of diabetes mellitus: type 1(IDDM), type 2(NIDDM),“other specific types” andgestational diabetes (WHO Expert Committee 1999). These were reflected in the subsequent International Nomenclature of Diseases (IND) in1991and the tenth revision of the International Classification of Diseases (ICD-10) in 1992 [13]. Hence, classification of diabetes mellitus is described as below.
Type 1 diabetes, once known as juvenile diabetes or insulin-dependent diabetes, is a chronic condition. In this condition, the pancreas makes little or no insulin. Insulin is a hormone the body uses to allow sugar (glucose) to enter cells to produce energy.
Different factors, such as genetics and some viruses, may cause type 1 diabetes. Although type 1 diabetes usually appears during childhood or adolescence, it can develop in adults. Even after a lot of research, type 1 diabetes has no cure.
Treatment is directed toward managing the amount of sugar in the blood using insulin, diet and lifestyle to prevent complications. Type I diabetes mellitus is also known as insulin- dependent diabetes mellitus (IDDM), this occurs mainly in children and young adults; the onset is usually sudden and can be life threatenin. Type 1 is usually characterized by the presence of anti–glutamic acid decarboxylase, islet cell or insulin antibodies which identify the autoimmune processes which leads to beta-cell destruction . Type 1 diabetes (due to the destruction of b-cell which is usually leading to absolute insulin deficiency) (American Diabetes Association, 2014). The rate of destruction of betacell is quite variable; it can be occur rapidly in some individuals and slow in others . There is a severe deficiency or absence of insulin secretion due to destruction of ß-islets cells of the pancreas. Treatment with injections of insulin is required . Markers of immune destruction, including islet cell auto-antibodies, and/or auto antibodies to insulin, and auto antibodies to glutamic acid decarboxylase (GAD) are present in 85-90 % of individuals with Type 1 diabetes mellitus when fasting diabetic hyperglycemia is initially detected. The exact cause of diabetes mellitus is remain unknown, although, in most people, there is evidence of an autoimmune mechanism involving auto-antibodies that destroy the betaislet cells.
Type 2 diabetes mellitus is also known as adult-onset diabetes.The progressive insulin secretary defect on the background of insulin resistance (American Diabetes Association, 2014) . People with this type of diabetes frequently are resistant to the action of insulin . The long-term complications in blood vessels, kidneys, eyes and nerves occur in both types and are the major causes of morbidity and death from diabetes . The causes are multifunctional and predisposing factor includes: Obesity, Sedentary lifestyle, increasing age (affecting middleaged and older people), Genetic factor (Ross and Wilson 2010), such patients are at increased risk of developing macro vascular and micro vascular complications.
3.Gestational Diabetes Mellitus
The glucose intolerance occurring for the first time or diagnosed during pregnancy is referred to as gestational diabetes mellitus (GDM) . Women who develop Type1 diabetes mellitus during pregnancy and women with undiagnosed asymptomatic Type 2 diabetes mellitus that is discovered during pregnancy are classified with Gestational Diabetes Mellitus (GDM). Gestational diabetes mellitus (GDM) (diabetes diagnosed during pregnancy that is not clearly over diabetes) . The gestational diabetes mellitus may develops during pregnancy and may disappear after delivery; In the longer term, children born to mothers with GDM are at greater risk of obesity and type 2 diabetes in laterlife, a phenomenon attributed to the effects of intrauterine exposure to hyperglycaemia.
The most common form of monogenic types of diabetes is developed with mutations on chromosome 12 in a hepatic transcription factor referred to as hepatocyte nuclear factor (HNF)-1a.They also referred to as genetic defects of beta cells. These forms of diabetes are frequently characterized by onset of hyperglycemia at an early age (generally before age of 25 years). They are also referred to as maturity onset diabetes ofthe young (MODY) or maturity-onset diabetes in youth or with defects of insulin action; persons with diseases of the exocrine pancreas, such as pancreatitis or cystic fibrosis; persons with dysfunction associated with other endocrinopathies (e.g. acromegaly); and persons with pancreatic dysfunction caused by drugs, chemicals or infections. Some drugs also used in the combination with the treatment of HIV/ AIDS or after organ transplantation. Genetic abnormalities that result in the inability to convert proinsulin to insulin have been identified in a few families, and such traits are inherited in an autosomal dominant pattern. They comprise less than 10% of DM cases.
Core Symptoms & Signs
Extreme Hunger (Polyphagia): A constant feeling of hunger, as the body is unable to process and use the food consumed for energy.
Other Potential Indicators
While Type 1 diabetes symptoms can appear suddenly (sometimes in a matter of weeks), Type 2 diabetes symptoms develop much more slowly and can go unnoticed for years.
Etiology of Diabetes Mellitus
The word etiology is derived from Greek word “aetiologia”. Hence, etiology is defined as the science of finding causes and origins in which a disease is arise, It includes –
Causes of diabetes mellitus
Diabetes Mellitus (DM) occurs when the body cannot properly produce or use insulin, leading to high blood sugar. Causes vary by type: Type 1 is an autoimmune disease where genes and environmental triggers destroy insulin-making cells; Type 2 is driven by insulin resistance, genetics, and lifestyle factors.
Specific causes and triggers differ depending on the specific type of the condition:
Type 1 Diabetes
Type 2 Diabetes (Most Common)
Gestational Diabetes
Secondary & Monogenic Diabetes
Diagnosis of Diabetes Mellitus
Diabetes is diagnosed using specific blood tests that measure your blood sugar or average glucose levels over the past few months. Common tests include the A1C, Fasting Blood Sugar, and Oral Glucose Tolerance Test. A diagnosis must be confirmed by a healthcare professional
Healthcare providers use one or more of the following tests to confirm a diagnosis:
Treatment of Diabetes Mellitus
The treatment is to overcome the precipitating cause and to give high doses of regular insulin. The insulin requirement comes back to normal once the condition has been controlled the aims of management of diabetes mellitus can be achieved by:
1.Stem cell therapy
Researchers have shown that monocytes/ macrophages may be main players which contribute to these chronic inflammations and insulin resistance in T2DM patients. Stem cell educator therapy, a novel technology, is designed to control or reverse immune dysfunction’s. The procedure includes: collection of patients’ blood circulating through a closed-loop system, purification of lymphocytes from the whole blood, co-culture of them with adherent cord blood-derived multi-potent stem cells (CB-SCs) in vitro and administration of the educated lymphocytes (but not the CB-SCs) to the patient’s circulation.
2.Antioxidant therapy
A variety of antioxidants, such as vitamins, supplements, plant-derived active substances and drugs with antioxidant effects, have been used for oxidative stress treatment in T2DM patients. Vitamin C, vitamin E and β carotene are ideal supplements against oxidative stress and its complications . Antioxidant which play an important role in lowering the risk of developing diabetes and its complications.
1.Anti-inflammatory treatment
The changes indicate that inflammation plays a pivotal role in the pathogenesis of T2DM and its complications . In T2DM, especially in adipose tissue, pancreatic islets, the liver, the vasculature and circulating leukocytes, which include altered levels of specific cytokines and chemokines, the number and activation state of different leukocyte populations , increased apoptosis and tissue fibrosis . Immunomodulatory drugs are provided.
Dietary Management
Adequate caloric value Dietary management should be taken properly by the both diabetic and non-diabetic patient such as:
C.Newer Insulin Delivery Devices
A number of innovations have been made to improve ease and accuracy of insulin administration as well as to achieve tight glycaemia control. These are insulin syringes, pen devices, inhaled insulin, insulin pumps, implantable pumps, other routes of insulin delivery.
D.Oral Hypoglycaemic or Antidiabetic Agents
Clinically useful biguanide phenformin was produced parallel \to sulfonylurea’s in 1957. Newer approaches have constantly been explored and have lately yielded thiazolidinediones, meglitinide analogues, α-glucosidase inhibitors, and the latestare dipeptidyl peptidase-4(DPP-4) inhibitors.
CONCLUSION AND DISCUSSION
Diabetes mellitus poses a significant global health challenge due to its increasing prevalence and associated complications, including cardiovascular disease, kidney failure, and neuropathy. Early diagnosis and appropriate management are crucial in preventing or delaying these complications.
Recent advances in diabetes care, such as CGM, insulin analogs , and personalized medicine, offer promising tools to enhance the quality of life for individuals with diabetes.
Moreover, public health efforts must focus on diabetes prevention through education, lifestyle interventions, and policies that promote healthy eating and physical activity. By addressing the social determinants of health and reducing disparities in diabetes care, we can make significant strides in mitigating the impact of this chronic condition.
In conclusion, diabetes mellitus is a complex and pervasive disease that demands a multidisciplinary approach to diagnosis, treatment, and prevention. With ongoing research and innovations in diabetes care, there is hope for better outcomes and an improved quality of life for individuals living with diabetes.
REFERENCES

M. Prasadarao*, Y. Narasimharao, S. Rajini, G. Raghu., A Review on Diabetes Mellitus, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3045-3054. https://doi.org/ 10.5281/zenodo.20647244
 10.5281/zenodo.20647244
10.5281/zenodo.20647244