
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3 School of Pharmaceutical Sciences, RIMT University, Mandi, Gobindgarh
4 Faculty of Pharmaceutical Sciences, Motherhood University, Dehradhun.
Ulcerative colitis (UC) is a chronic idiopathic inflammatory bowel disease (IBD) characterised by continuous mucosal inflammation extending proximally from the rectum, affecting approximately 5 million people worldwide as of 2023, with rising incidence in developing regions including India. First described by Samuel Wilks in 1859, UC typically presents in the second or third decade of life with cramping abdominal pain and bloody diarrhoea, following a relapsing–remitting course. Its multifactorial pathogenesis involves genetic susceptibility (NOD2/CARD15, IL23R, IL10 variants), immune dysregulation through NF-?B, JAK/STAT, NLRP3, and IL-23/IL-17 signalling pathways, gut microbiome dysbiosis, and epithelial barrier dysfunction. A major pharmaceutical challenge is that over 40% of anti-inflammatory drug candidates exhibit poor aqueous solubility (BCS Class II/IV), severely limiting oral bioavailability. Self-Emulsifying Drug Delivery Systems (SEDDS) — isotropic mixtures of oils, surfactants, and co-solvents — overcome this by spontaneously forming fine oil-in-water emulsions in gastrointestinal fluids; advanced variants SMEDDS (100–250 nm) and SNEDDS (<100 nm) offer nanoscale droplets with superior absorption and thermodynamic stability. This review integrates current knowledge of UC pathogenesis with the therapeutic potential of SEDDS-based colon-targeted delivery as a strategy to improve drug bioavailability and clinical outcomes.
Ulcerative colitis (UC) is an idiopathic inflammatory bowel disease (IBD), first described by Samuel Wilks in 1859 [1]. It is characterized by continuous inflammation of the colonic mucosa extending proximally from the rectum. UC is a chronic illness that typically manifests in the second or third decade of life with cramping abdominal pain and bloody diarrhoea [2]. Clinical manifestations during flares include bloody diarrhoea, disordered gut motility, systemic effects, and in severe cases, surgical complications [3].
UC is classified by the extent of inflammation — limited to the rectum (proctitis), one-sided (left-sided colitis), or widespread (pancolitis) — and by symptom severity. Treatment decisions are guided by these parameters. The condition has no definitive cure short of colectomy, and most patients require ongoing long-term management [4,5].
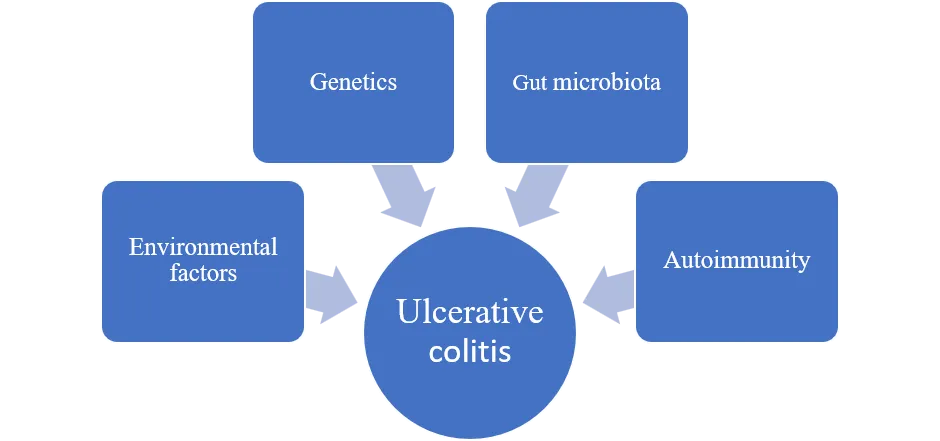
The pathogenesis of UC involves a complex interplay of genetic susceptibility, environmental factors, immune dysregulation, and microbial imbalance [6]. Disruption of the intestinal barrier — including reduced mucus-producing cells and increased epithelial permeability — along with dysregulated T-cell responses, elevated chemokines and cytokines, and reduced microbial diversity are key pathogenic mechanisms [7-8].
Extra-intestinal manifestations are common, particularly affecting joints (arthritis, spondylitis, enthesopathy) in 10–25% of IBD patients, with activity often correlating with gut disease [9].

Figure 1. Colon-targeted drug delivery to the UC area.
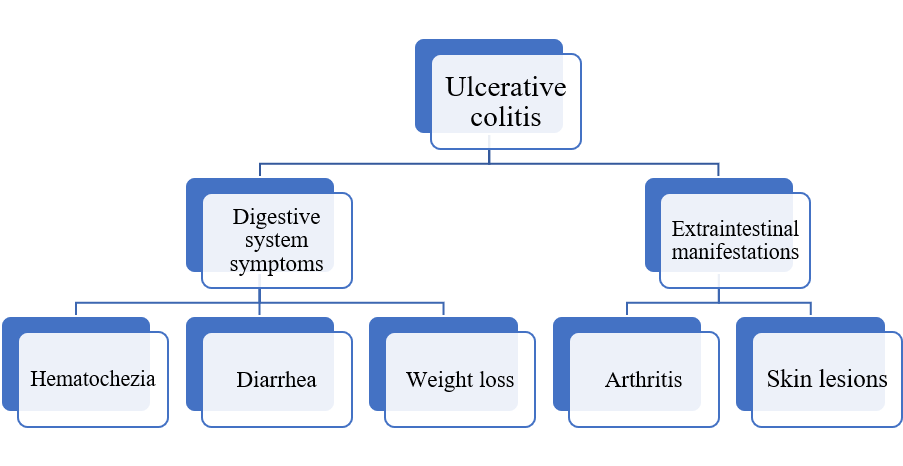

Figure 2: Clinical manifestations of UC
Ulcerative Colitis is a kind of IBD (Inflammatory Bowel Disease). Immune systems reacting oddly to bacteria in the gut, again and again. These flare-ups strike the digestive tract without warning. Though both are long-term gut disorders, their patterns within the bowel lining aren’t identical. One spreads continuously. The other might skip sections.
1. Crohn’s disease
2. Ulcerative Colitis
The lining of the colon and the rectum become inflamed when someone has ulcerative colitis. Ulcerative colitis is an autoimmune disease in which the large intestine’s inner lining becomes inflamed and ulcerated. Even though ulcerative colitis may appear at any age, it often shows up between young adulthood and middle years. The gut tissue swells up, sometimes forming raw sores where healing fails.
Normal liver ulcerative liver
Figure 3: Normal liver and ulcerative liver
There are different types or classifications of ulcerative colitis dependent on the extent and location of the inflammation within the colon. The types of ulcerative colitis include:
1. Ulcerative proctitis
2. Proctosigmoiditis
3. Left-sided Colitis
4. Acute Severe Ulcerative Colitis
1. Diarrhoea (may or may not be bloody)
2. Blood, mucus or pus in your stool
3. Severe belly cramping
4. Fatigue (extreme tiredness)
5. Sudden weight loss
1. Diarrhoea (may or may not be bloody)
2. Increased bowel movements or episodes of diarrhoea (four or fewer episodes daily)
3. Urgent bowel movements (sudden need to poop)
4. Tenesmus (feeling like you have to poop but being unable to)
5. Mild abdominal (belly) cramping or tenderness
6. Nausea [11]
There are both genetic and environmental factors that contribute to IBD, although there is still much to learn about the pathophysiology of ulcerative colitis. Some factors have been repeatedly assessed and shown to be crucial to the development and course of the condition. The primary contributing factors include: a dysregulated immunological response, a compromised epithelial barrier, alterations in the gut microbiome, genetic vulnerability, and the exposome.
6.1 Genetic Factors
There is a significant genetic component to UC. Individuals with a family history of IBD, particularly first-degree relatives with UC, exhibit an increased risk of developing the condition. Multiple genes have been implicated in the susceptibility to UC, including the NOD2/CARD15 gene and the interleukin genes (IL23R and IL10). Although a family history of IBD is present in approximately 25% of UC patients, most cases are sporadic [12]. Identified genetic associations include HLA-DQA1 variants, and genes involved in epithelial barrier integrity (CDH1, LAMB1), immune signalling (TNFRSF15, TNFRSF9, IL1R2, IL8RA/RB, IL7R), and others [13].
6.2 Dysregulation of the Immune System
One of the key elements in the pathogenesis of UC is an abnormal immune response. Normal gut bacteria are mistakenly perceived as foreign invaders, causing the intestinal lining to become chronically inflamed. Immune cells such as T-cells, B-cells, and macrophages infiltrate the gut lining and release pro-inflammatory cytokines. These cytokines are involved in the inflammatory process and further damage the intestinal tissue.
6.3 Intestinal Barrier Dysfunction
When ulcerative colitis is present, the gut wall weakens. Bacteria slip through cracks they normally cannot enter. Once inside, they trigger the immune system. Immune cells jump into action as a result, perpetuating the inflammatory cycle.
6.4 Gut Microbiome Dysbiosis
In healthy individuals, the gut microbiota is predominantly made up of four bacterial phyla — Firmicutes, Bacteroidetes, Proteobacteria, and Actinobacteria — accounting for roughly 97% of the total. Firmicutes and Bacteroidetes alone represent about 90% of the entire microbial community. These dominant phyla produce short-chain fatty acids (SCFAs), especially butyrate and propionate, through the fermentation of dietary components like non-digestible fibres. SCFAs are vital for preserving intestinal balance and have been shown to regulate immune homeostasis [14].
When ulcerative colitis shows up, that balance shifts — harmful microbes grow more while helpful kinds fade, causing further inflammation. Probiotics appear to benefit individuals with UC mainly by influencing key signalling pathways — such as NF-κB, MAPK, TLR, JAK/STAT, Wnt/β-catenin, and TGF-β — alongside their well-known effects on gut microbiota composition [15].
6.5 Key Inflammatory Signalling Pathways
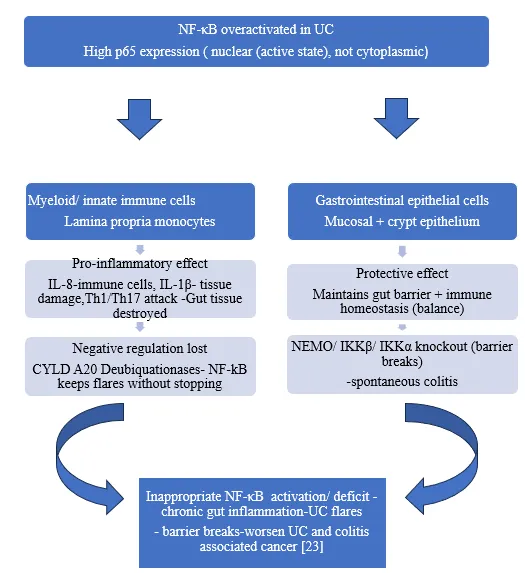
NF-κB Pathway: The NF-κB transcription factor plays a central role in driving inflammation and immune responses. Evidence indicates that probiotics help dampen intestinal inflammation in UC by suppressing NF-κB pathway activity [16,17].
NLRP3 Inflammasome: Pathogen-associated molecular patterns (PAMPs) and danger-associated molecular patterns (DAMPs) activate the NLRP3 inflammasome, leading to Caspase-1 activation and subsequent release of pro-inflammatory cytokines IL-1β and IL-18, contributing to colonic mucosal inflammation [18].
PI3K/Akt Pathway: In addition to controlling and releasing inflammatory factors, the PI3K/Akt signalling pathway can also indirectly activate the transcription factor NF-κB via phosphorylated IKK. TLR4 signalling triggers the PI3K/Akt signalling pathway and induces downstream mTOR activation [19-20].
The overview of inflammatory signalling pathways involved in UC
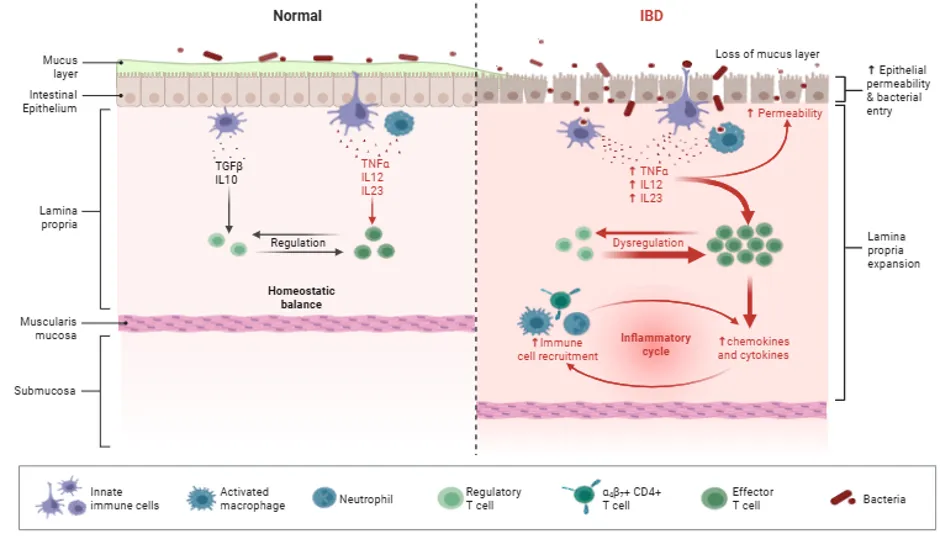
Figure 3: Pathophysiological mechanism of ulcerative colitis (UC).
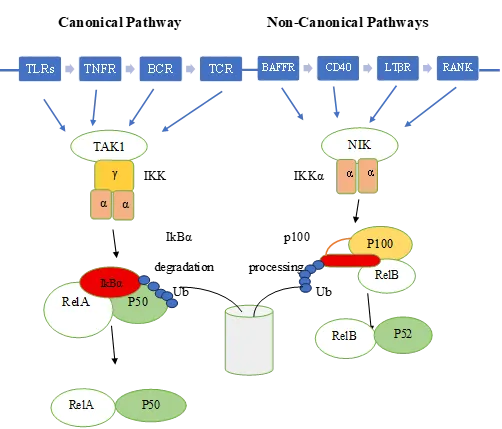
Figure 4: Canonical and non-canonical NF-κB signaling pathways [21]
Curcumin- SEDDS – blocks IKKβ & p65 nuclear translocation entry
Budesonide-SEDDS- Induces IKBα-locks NF-kB
Quercetin-SEDDS- Blocks IKK+ IkB Stabilisation
Thymoquinone-SEDDS- Inhibits IkB Degradation & NF-kB DNA binding. SEDDS enhances its colonic retention and anti-inflammation potency. Blocks IkB Degradation
7. SELF EMULSIFYING AND SELF MICRO EMULSIFYING DRUG DELIVERY SYSTEM
7.1. Introduction
Oral administration remains the most widely preferred and convenient route of drug delivery. However, more than 40% of new drug candidates exhibit poor water solubility, which presents a significant challenge in oral drug delivery due to inadequate absorption, high intra- and inter-subject variability, and poor dose proportionality [24]. Various formulation strategies have been employed to overcome these limitations, including the use of surfactants, lipids, permeation enhancers, micronization, salt formation, cyclodextrins, nanoparticles, and solid dispersions [25].
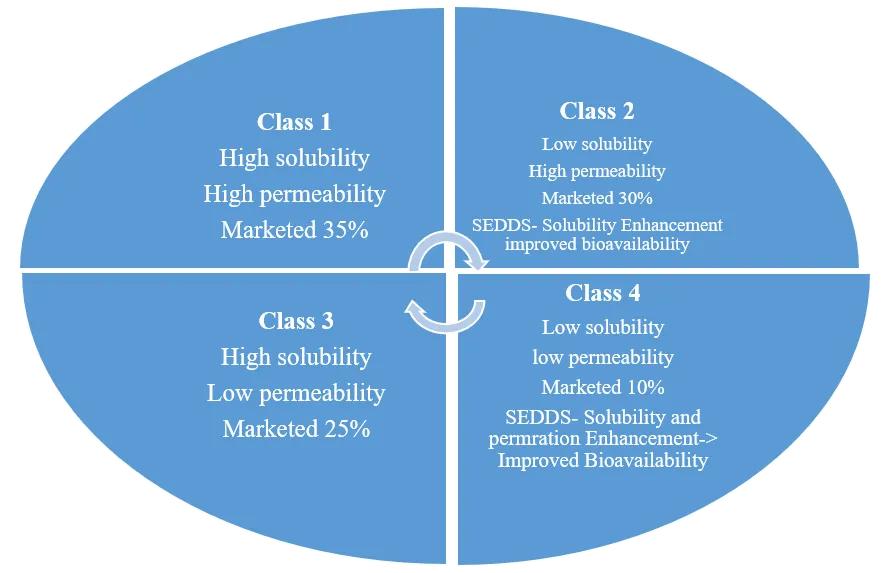
Figure 5. Biopharmaceutics classification system
Solubility and permeability are the two fundamental parameters governing drug absorption following oral administration. The Biopharmaceutics Classification System (BCS), developed by Amidon et al. in 1995, classifies drugs into four categories based on these two parameters, as illustrated in Figure 1 [26,27]. Among the four BCS classes, Class II and Class IV drugs are particularly problematic due to their poor water solubility and low oral bioavailability. Consequently, enhancing the dissolution profile of BCS Class II and IV drugs remains one of the most critical challenges in pharmaceutical research.
Since dissolution is considered the rate-limiting step in the absorption of poorly water-soluble drugs [28], achieving efficient self-emulsification through ultra-low oil-water interfacial tension can significantly enhance drug bioavailability and ensure a more consistent and predictable absorption profile from the gastrointestinal tract.
7.1.1. Self-emulsifying drug delivery systems
SEDDS are defined as isotropic mixtures of solid or liquid surfactants, natural or synthetic oils, and/or one or more hydrophilic solvents and co surfactants/solvents [29]. Once more, as previously mentioned, they dilute the drug in the system (aqueous media), such as GI fluids, with mild agitation, forming fine oil-in-water (o/w) emulsions (0.1-100μm) or microemulsions (10-300 nm), which spread easily into the GIT where the movement of the stomach and intestinal fluid provides agitation, creating a self-emulsified system [30].
7.1.2. Properties of SEDDS
7.1.3. Advantages associated with SEDDS
Table: 1: It shows lipid formulation classification
|
Type |
Composition |
SEEDS Category |
Behaviour in Aqueous media |
Why it's used |
|
Type I |
Oil + drug only (no surfactant) |
Conventional SEDDS |
Reduced drug dissolution; increased drug precipitation post-digestion; slower lipolysis via bile salts & phospholipids |
Simple formulation for lipophilic drugs; low cost |
|
Type II |
Oil + water-insoluble surfactant (HLB < 12) |
Conventional SEDDS |
Enhances dissolution & emulsification, but inadequate solubilization in vivo |
Improves dissolution of poorly water-soluble drugs vs Type I |
|
Type IIIa |
Oil + co-surfactant + surfactant (HLB > 12) |
SMEDDS |
Forms stable o/w emulsion with minimal agitation; transitions readily to aqueous phase after steatolysis |
Forms stable O/W emulsion; enhances oral absorption significantly |
|
Type IIIb |
Oil + co-surfactant + surfactant (HLB > 12) |
SNEDDS |
Similar to IIIa; high emulsification efficiency |
Forms nanoemulsion; best for maximum drug absorption |
|
Type IV |
Surfactant ± co-surfactant (no oil) |
— |
Excellent dissolution properties; unstable in GI tract upon dilution |
Excellent dissolution; used when oil-free formulation is needed |
Self-emulsifying drug delivery systems are made using a lot of excipients. Although co-surfactants can also be utilized, oil and surfactant are essential ingredients. The kind of dose form controls the use of various excipients in SEDDS. SEDDS of different medications have been formulated using a variety of oils, including natural, synthetic, and semi-synthetic. Table 1 lists a few instances of the oils utilized in the commercial products. Table 2 lists the oils utilized in the formulation of SEDDS with various medications.
Table 2: Type of oils used in marketed SEDDS
|
Type of oil |
Marketed Product |
Drug |
|
Corn oil |
Depakene capsule |
Valproic acid |
|
Olive oil |
Sandimmune oral solution |
Cyclosporine |
|
Sesame oil |
Marinol soft gelatin capsule |
Dronabinol |
|
Soya bean oil |
Accutane soft gelatin capsule |
Isotretinoin |
|
Peanut oil |
Prometrium soft gelatin capsule |
Progesterone |
|
Bees wax |
Vesanoid soft gelatin capsule |
Tretinoin |
|
Hydrogenated soya bean oil |
Accutane soft gelatin capsule |
Isotretinoin |
Table 3: Type of oils used with different drugs in SEDDS
|
Oil |
Drug |
|
Soya bean oil |
Probucol, Ibuprofen |
|
Ethyl oleate |
Vinpocetine |
|
Oleic Acid |
Puerarin |
|
Maisine oil |
Lercanidipine |
|
Polyoxy castor oil |
Simvastatin |
|
Peanut oil |
Griseofulvin |
Table 4: Type of surfactants used in marketed SEDDS
|
Surfactant |
Marketed Product |
Drug |
|
Span 80, Tween 80 |
Gengraf soft gelatin capsule |
Cyclosporine |
|
Tween 20 |
Targretin Hard gelatin Capsule |
Bexarotene |
|
Cremophor RH 40 |
BCNU self-emulsifying implant |
Carmustine |
|
D-alpha Tocopheryl Poly ethylene Glycol Carmustine Amprenavir 1000 Succinate (TPGS) |
Agenerase Soft Gelatin capsule, Agenerase oral solution |
Amprenavir |
|
Labrafil M 1944 CS |
Sandimmune oral solution. |
Cyclosporine |
Table 5: Type of surfactants used with different drugs in SEDDS
|
Surfactant |
Drug |
|
Tween 80 |
Ketoprofen, Carvedilol |
|
TPGS |
Tacrolimus |
|
Labrafil M 1944 CS |
Probucol |
|
Tween 85 |
Indomethacin |
|
Cremophor EL |
Loratadine [32] |
Table 6: Type of Co surfactants used in marketed SEDDS
|
Co surfactants |
Marketed preparation |
|
Poly Ethylene Glycol |
Targretin soft gelatin Capsule, Gengraf hard gelatin capsule, Agenerase soft gelatin |
|
Glycerine |
Sandimmune soft gelatin capsule |
|
Propylene glycol |
Neoral soft gelatin, Neoral oral solution, Gengraf hard gelatin, Lamprene soft gelatin capsule. |
|
Ethanol |
Neoral Soft gelatin & Neoral oral, sandimmune soft gelatin & oral sol, gengraf hard gelatin capsule |
Examples: Naproxen, Carbamazepine, Danazol, Ketoconazole, Nifedipine, vitamin E, simvastatin, and mefanimic acid Finasteride
9. SOLID SELF EMULSIFYING DRUG DELIVERY SYSTEM (S--SEDDS)
Although SEDDS are available in both liquid and solid dose forms, solid SEDDS are typically favoured over liquid SEDDS due to their superior stability and simplicity of handling and transportation. A variety of different solid SEDDS, including pellets, microspheres, tablets, beads, implants, and suppositories, have recently been developed.
Table 7. Comparison of SEDDS, SMEDDS, and SNEDDS [33,34].
|
Characteristics |
SEDDS |
SMEDDS |
SNEDDS |
|
Mean droplet size |
250 nm–5 µm |
100–250 nm |
<100 nm |
|
Appearance |
Turbid/Cloudy |
Clear to translucent |
Optically clear |
|
Solubilizing capacity |
High |
High |
High |
|
Stability |
Thermodynamically unstable |
Thermodynamically stable |
Kinetically stable |
|
Bioavailability |
Moderate |
Enhanced |
Superior |
|
Oil Types |
Long-chai–n triglycerides (e.g., soybean oil, olive oil) |
Medium-chain triglycerides (e.g., Labrafac®, Captex® 355) (MC triglycerides) |
Medium- and short-chain triglycerides (e.g., Capmul®, Miglyol®) (caprylic and capric triglycerides) |
|
HLB of surfactants |
<10 |
10–12 |
>12 |
|
Co-surfactants |
Not essential |
Short-chain alcohols (e.g., propylene glycol) |
Polyethylene glycol (PEG), Transcutol® |
Table 8: Marketed Preparations of SEDDS.
|
Brand Name |
Generic Drugs |
Dosage Forms |
Manufacturer |
|
Convulex |
Valproic acid |
Soft gelatin capsule |
Gerot Pharmazeutika |
|
Norvir |
Ritonavir |
Soft gelatin capsule |
Abbvie, Abbot |
|
Fortovase |
Saquinavir |
Soft gelatin capsule |
Hoffman- Roche |
|
Neoral |
Cyclosporine |
Soft gelatin capsule |
Novartis |
|
Agenerase |
Amprenavir |
Soft gelatin capsule |
GSK |
|
Lipirex |
Fenofibrate |
Hard gelatin capsule |
Sanofi- Aventis |
|
Solufen |
Ibuprofen |
Hard gelatin capsule |
Sanofi- Aventis |
|
Depakene |
Valproic acid |
Soft gelatin capsule |
Abbvie |
|
Accutane |
Isotretinoin |
Soft gelatin capsule |
Hoffman Le Roche |
|
Prometruim |
Progesterone |
Soft gelatin capsule |
Virtus |
CONCLUSION
Ulcerative colitis remains one of the most challenging chronic inflammatory diseases of the modern era. With a global prevalence of approximately 5 million cases and a steadily rising incidence in previously low-burden regions — particularly in South Asia, Africa, and South America — UC represents a growing public health concern. In India, rapid urbanisation, dietary westernisation, and changing hygiene standards are contributing to an accelerating disease burden, especially in northern regions such as Punjab, where community-based studies have documented prevalence rates comparable to some Western nations. The relapsing-remitting nature of the disease, combined with its long-term risk of colorectal cancer and need for colectomy in a subset of patients, underscores the urgent need for effective and patient-friendly therapeutic strategies.
The pathogenesis of UC is complex and multidimensional, involving a dynamic interplay between genetic predisposition, dysregulated immune responses, gut microbiome imbalance, and compromised intestinal barrier function. Key inflammatory signalling pathways — including NF-κB, NLRP3 inflammasome, PI3K/Akt, JAK/STAT, and the IL-23/IL-17 axis — drive chronic mucosal inflammation and tissue damage. Dysbiosis, characterised by loss of short-chain fatty acid-producing bacteria such as Firmicutes and Bacteroidetes, further amplifies the inflammatory cascade. Understanding these mechanisms has not only expanded our knowledge of disease biology but has also identified novel therapeutic targets. Despite advances in biologics and small molecules, a significant number of patients remain refractory to current treatments, highlighting the continued need for innovative drug delivery approaches that can enhance therapeutic efficacy at the site of colonic inflammation.
A central pharmaceutical barrier in UC therapy is the poor aqueous solubility of many candidate drugs. Over 40% of new anti-inflammatory compounds fall into BCS Class II or IV, meaning their therapeutic potential is undermined by inadequate dissolution and absorption in the gastrointestinal tract. SEDDS directly address this limitation by forming isotropic, thermodynamically stable mixtures of oils, surfactants, and co-solvents that spontaneously self-emulsify upon contact with gastrointestinal fluids under gentle agitation. The resulting fine oil-in-water emulsions present drug molecules in a pre-dissolved or nano-dispersed state, dramatically increasing the surface area available for absorption and bypassing the rate-limiting dissolution step. The enhanced wettability, improved membrane permeation, and protection from enzymatic degradation collectively contribute to a significantly elevated oral bioavailability compared to conventional solid dosage forms. Drugs with a log P above 5 show the greatest benefit within SEDDS formulations, as they partition effectively into the lipid phase and are subsequently incorporated into chylomicrons for lymphatic transport, further circumventing hepatic first-pass metabolism.
The successful commercialisation of SEDDS-based products including Neoral (cyclosporine), Norvir (ritonavir), and Accutane (isotretinoin) provides clinical proof of concept and a strong foundation for developing SEDDS formulations tailored specifically for UC-targeted therapy.
Future research should focus on comprehensive in vivo evaluation of SEDDS-loaded colon-targeted formulations for key UC drugs such as mesalazine, budesonide, and curcumin; rigorous stability testing under simulated gastrointestinal conditions; and scale-up feasibility for industrial manufacturing. Advances in nanotechnology, surface functionalisation, and computational formulation design will further accelerate the development of next-generation SEDDS. In summary, SEDDS-based colon-targeted delivery systems hold substantial promise as a transformative therapeutic strategy for UC, and sustained investment in this field is essential to translate laboratory advances into improved patient outcomes.
REFERENCES


Asha, Gautam Raj Puri, Neha Srivastava, Seema Tomar, A Review on SEDDS for Ulcerative Colitis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1211-1224. https://doi.org/10.5281/zenodo.20550960
 10.5281/zenodo.20550960
10.5281/zenodo.20550960