
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1. Dr.M.Prasada Rao, Professor & Principal of M.A.M College of Pharmacy.
2. Dr.Y.Narasimha Rao, Professor , Department of Pharmacology.
3. Dr.S.Rajini, Professor, Department of Pharmacy Practice.
4. N.MAHESH, Pharm D Student of M.A.M College of Pharmacy
Schizophrenia is a challenging and diverse mental health condition with a lifetime prevalence of approximately 1.41% and a current active prevalence of 0.42%. Schizophrenia usually manifests in late adolescence or early adulthood and is associated with high disability and a reduced life expectancy. Risk factors include genetic predisposition, prenatal and birth complications, infections and immune dysfunction, and cannabis use as well as psychosocial factors such as childhood trauma or migration. The first psychotic episode is often preceded by a long prodromal phase that can last for several years. No markers are yet available for clinical use that allow prediction of disease development or a diagnosis to be established. A leading theory postulates that excitatory–inhibitory (that is, glutamate–GABA) imbalance in the cortex ultimately leads to dysfunction of the dopaminergic system. Schizophrenia is a heterogeneous disease with different manifestations, including psychotic symptoms as well as negative symptoms and global cognitive deficit, that do not respond to antipsychotic drugs, making management very difficult. Pharmacological treatment coupled with psychotherapeutic interventions, such as cognitive behavioural therapy, cognitive remediation and psychoeducation, remains the mainstay of treatment; however, treatment resistance is frequent. The first medication that targets neurotransmitter systems other than dopamine has been approved for use. Current attempts to use virtual reality and avatars to improve psychotic symptoms and smartphone applications to prevent relapses seem promising.
Schizophrenia is the major mental illness of our time. It was first described by Kraepelin (1896) as “dementia praecox” and later given the name “schizophrenia” by Bleuler in 1911. It is a condition characterised by disturbances of thought, perception and a blunting of affect. These disturbances “involve the most basic functions that give the normal person a feeling of individuality, uniqueness, and self-direction” (WHO 1992). In 1959 a German Psychiatrist identified what he considered to be first rank symptoms of schizophrenia (Schneider 1959). Schneider grouped the collection of symptoms into three main categories, namely, auditory hallucinations, passivity experience and delusional thinking. Schizophrenia sufferers experience hallucinatory “voices” which may either provide a running commentary on one’s movements or instruct the person to carry out certain tasks. Some sufferers experience voices which are derogatory or insulting. Passivity feelings refer to those feelings, thoughts or behaviours which the individual experiences as being under the influence of a third party. Delusional thinking arises from perceptions which may be distorted. Delusional thinking is often insightless and unamienable to reason. Although these symptoms are no longer used as the sole diagnostic aid Schneider’s categorisation of the symptoms gives a glimpse of the level of disturbance those with schizophrenia experience. Schizophrenia however is also associated with a wide range of other symptoms including social withdrawal, incongruent affect and thought disturbances, which contribute to the devastating effects this illness can have on the person. The cost of schizophrenia in both human terms and in its cost to the nation is immense. As well as the symptoms described above loss of social contacts and career prospects often go hand-in-hand with the illness. Davies and Drummond (1994) estimated the cost of schizophrenia to the country at £397m, or 1.6% of the total health care budget. This paper will attempt to review current developments in the classification, causes and treatment of schizophrenia and hopefully draw some conclusions from the literature on the future developments in the treatment of this illness.
Fig 1 schizophernia
Classification and Diagnostic Criteria
The classification of schizophrenia has been described mostly by psychiatrists. While there are numerous diagnostic texts for mental illness many are used solely for the purposes of research and are seldom seen in clinical practice. This paper will therefore concentrate on those used in clinical practice. There are currently two main texts which are used in clinical settings to classify, and describe for diagnostic purposes, mental illnesses including schizophrenia. These are namely the International Classification of Diseases-10 (ICD-10) and the Diagnostic and Statistical Manual of Mental Disorders -IV (DSM-IV).
The International Classification of Diseases-10 (ICD-10) provides diagnostic categories for mental illnesses including schizophrenia (WHO 1992). Schizophrenia is described as “a syndrome with a variety of causes, and a variety of outcomes, depending on the balance of genetic, physical, social and cultural influences”. ICD-10 describes a number of sub-categories of schizophrenia.
These are :
Paranoid Schizophrenia: the most common type of schizophrenia in most parts of the world. It is characterised by “stable, often paranoid, delusions usually accompanied by (auditory) hallucinations and perceptual disturbances” (WHO 1992).
Hebephrenic Schizophrenia: hebephrenic schizophrenia usually commences in late adolescence or early adulthood and is considered to have a poor outcome. It is characterised by affective changes, fleeting delusions and hallucinations, irresponsible or unpredictable behaviour (WHO 1992).
Catatonic Schizophrenia : Catatonic schizophrenia is rarely seen in industrial countries for reasons which are as yet unknown. It is characterised by disorders of movement and volition. As well as episodes of extreme stupor, sudden violent excitement has been described.
Undifferentiated Schizophrenia:
Undifferentiated schizophrenia is an outdated medical term for a condition where a person experiences schizophrenia symptoms—such as delusions, hallucinations, or disorganized behavior—but their clinical presentation does not fit neatly into specific subtypes like paranoid or catatonic.
Residual Schizophrenia : Residual schizophrenia refers to a past-defined subtype of schizophrenia where a person has previously experienced at least one major psychotic episode, but is no longer suffering from intense "positive symptoms" (like hallucinations or delusions). Instead, they experience milder, lingering "negative symptoms" such as flat emotions, poor motivation, and social withdrawal.
The person should have had a period of at least a year when the intensity of these florid symptoms have been substantially reduced (WHO 1992). ICD-10 suggests a one month period between onset of symptoms before a diagnosis of schizophrenia is arrived at. This is to help distinguish schizophrenia from acute psychotic episodes which may resolve without treatment within 2-3 weeks.
The Diagnostic Statistical Manual of Mental Disorders-IV (DSM-IV) categorises schizophrenia for the purposes of diagnosis (American Psychiatric Association 1994). Diagnostic criteria within DSM-IV differs slightly to that of ICD-10. DSM-IV criteria advise that signs and symptoms of schizophrenia must be present for “a significant portion of time during a 1 month period with some signs of the disorder persisting for at least 6 months”. This is in contrast to the ICD-10 criteria which requires symptoms to be present for a one month period. DSM-IV descriptions of subtypes of schizophrenia are largely similar to that of ICD-10. It describes 5 main subtypes namely Paranoid, Disorganised, Catatonic, Undifferentiated and Residual types. Descriptions of the subtypes are largely similar in both texts. The similarities are a result of wide international consultation between the two texts and the desire to have similar descriptions to facilitate compatibility for research purposes.
CORE SYMPTOMS
When the disease is active, it can be characterized by episodes in which the person is unable to distinguish between real and unreal experiences. As with any illness, the severity, duration, and frequency of symptoms can vary; however, in persons with schizophrenia, the incidence of severe psychotic symptoms often decreases as the person becomes older. Not taking medications as prescribed, the use of alcohol or illicit drugs, and stressful situations tend to increase symptoms.
Symptoms fall into three major categories (fig 2):
Positive symptoms: (Those abnormally present) Hallucinations, such as hearing voices or seeing things that do not exist, paranoia, and exaggerated or distorted perceptions, beliefs, and behaviors.
Negative symptoms: (those abnormally absent) A loss or a decrease in the ability to initiate plans, speak, express emotion, or find pleasure. Disorganized symptoms: Confused and disordered thinking and speech, trouble with logical thinking, and sometimes bizarre behavior or abnormal movements. Cognition is another area of functioning that is affected in schizophrenia leading to problems with attention, concentration, and memory, and declining educational performance. Symptoms of schizophrenia usually first appear in early adulthood and must persist for at least six months for a diagnosis to be made. Men often experience initial symptoms in their late teens or early 20s while women tend to show first signs of the illness in their 20s and early 30s. More subtle signs may be present earlier, including troubled relationships, poor school performance, and reduced motivation. Before a diagnosis can be made, however, a psychiatrist should conduct a thorough medical examination to rule out substance misuse or other neurological or medical illnesses whose symptoms mimic schizophrenia.
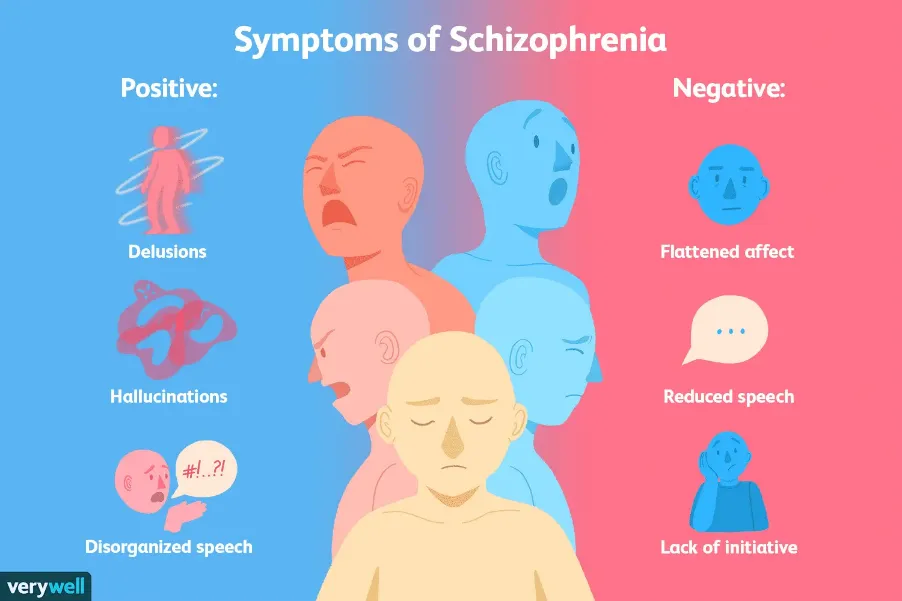
Fig no 2 : core symptoms of schizophrenia
ETIOLOGY
The exact cause is unknown but ,Several studies postulate that the development of schizophrenia results from abnormalities in multiple neurotransmitters, such as dopaminergic, serotonergic, and alpha-adrenergic hyperactivity or glutaminergic and GABA hypoactivity. Genetics also plays a fundamental role - there is a 46% concordance rate in monozygotic twins and a 40% risk of developing schizophrenia if both parents are affected. The gene Neuregulin (NGR1), which is involved in glutamate signaling and brain development, has been implicated, alongside Dysbindin (DTNBP1), which helps glutamate release, and Catecholamine O-Methyl Transferase (COMT) polymorphism, which regulates dopamine function. As a forementioned, there are also several environmental factors associated with an enhanced risk of developing the disease:
DIAGNOSIS OF SCHIZOPHRENIA
A schizophrenia diagnosis is a clinical process made by a mental health professional using criteria from the DSM-5-TR. It requires observing at least two core symptoms—such as delusions, hallucinations, or disorganized speech—for a significant portion of one month, with continuous signs of disturbance lasting for at least six months.
Because there is no definitive laboratory or imaging test for schizophrenia, the diagnostic process heavily involves ruling out other medical and psychiatric conditions.
The Diagnostic Process
Symptom Evaluation: A psychiatrist or mental health professional evaluates the presence of active psychotic, negative, and cognitive symptoms, often supplemented with information from family or caregivers.
Medical Rule-Outs: Doctors perform physical exams, blood and urine tests, and potentially brain imaging (like an MRI or CT scan) to ensure that similar symptoms are not caused by substance use, neurological conditions, brain injuries, or other underlying medical illnesses.
Psychiatric Rule-Outs: The provider ensures the symptoms cannot be attributed to schizoaffective disorder, bipolar disorder with psychotic features, or autism spectrum disorder.
Core DSM-5-TR Diagnostic Criteria
To receive a formal diagnosis, an individual must meet the following thresholds:
1.Characteristic Symptoms: Two or more of the following, each present for a significant portion of a 1-month period (or less if successfully treated):
2.Functional Impairment: A marked decline in one or more major areas of functioning (such as work, interpersonal relations, or self-care) since the onset of the disturbance.
3.Duration: Continuous signs of the disturbance must persist for at least 6 months. This period must include at least 1 month of active symptoms (or less if treated), and may include periods of prodromal (warning signs) or residual (milder) symptoms.
TREATMENT OF SCHIZOPHRENIA
Treatment of Schizophrenia usually involves a combination of medication, psychological therapies, and social support.
1. Antipsychotic Medications
These are the mainstay of treatment and help reduce symptoms such as hallucinations, delusions, and disorganized thinking.
2. Psychological Therapies
3. Community and Social Support
4. Treatment of Acute Episodes
If symptoms become severe and the person is a danger to themselves or others, hospitalization may be necessary for stabilization and safety.
5. Treatment-Resistant Schizophrenia
When symptoms do not improve after adequate trials of antipsychotic medications, Clozapine is often considered the most effective option, though it requires regular blood monitoring.
CONCLUSION
The conclusion about the whole picture of Schizophrenia could be drawn to point out what actually it is how it is prognosed, diagnosed, treated, and related. This clinical condition affects a person mentally which indirectly is an indication or whether to say a precautious warning to start living a "mentally healthy" life along with being socially & physically competent. Presented below are the words of John Forbes Nash Jr. (noble prize winning mathematician and subject of the award winning book and movie: A Beautiful Mind) He shares a piece of him while recalling his battle against schizophrenia: "I thought of the voices as...something a little different from aliens. i thought of them more like angels...It's really my subconscious talking, it was really that...i know that now.
REFERENCES

M.Prasada Rao*, Y.Narasimha Rao, S.Rajini , N.Mahesh, A Review on the Clinical Presentation of Schizophernia, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6198-6205. https://doi.org/10.5281/zenodo.20661490
 10.5281/zenodo.20661490
10.5281/zenodo.20661490