
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Loknete Dr. J. D. Pawar College of Pharmacy, Manur
Mucoadhesive drug delivery systems have gained significant attention in recent years as an effective strategy to improve both systemic and local drug administration, particularly for drugs that suffer from poor oral bioavailability due to enzymatic degradation and first-pass hepatic metabolism. The buccal mucosa, a non-keratinized and highly vascularized region of the oral cavity, offers a convenient and accessible route for transmucosal drug delivery of small molecules, peptides, proteins, and other therapeutic agents. Mucoadhesion involves the attachment of polymers to the mucosal surface through mechanisms such as wetting, diffusion, adsorption, mechanical interlocking, and electronic interactions, leading to prolonged residence time and enhanced drug absorption. The process occurs in two stages: initial contact and spreading of the dosage form followed by consolidation through interpenetration and bonding between polymer chains and mucus glycoproteins. Various physiological factors, including epithelial thickness, salivary flow, mucus composition, and blood supply, influence drug permeability and absorption across the buccal mucosa. Despite advantages such as avoidance of first-pass metabolism, improved bioavailability, ease of administration, and suitability for patients with swallowing difficulties, limitations like limited drug loading capacity, mucosal irritation, and variability in absorption remain challenges. Advances in mucoadhesive polymers and novel formulation approaches, including films, patches, gels, and nanoparticle-based systems, continue to enhance the efficiency and applicability of buccal drug delivery, making it a promising approach for controlled and targeted therapeutic delivery.
Mucoadhesion research has grown significantly over the past 20 years due to its promise to enhance systemic and tailored medication delivery. The oral delivery of peptide and protein-based drugs is limited by liver metabolism and enzyme breakdown, despite the fact that oral administration is frequently preferable.1 There are benefits to transmucosal medication delivery versus oral administration. Mucoadhesion targets medications to particular body parts for prolonged periods of time by using bioadhesive polymers.2 Different mucosal linings can be used for transmucosal medication delivery, with the oral mucosa being the most practical and favored method.3 The buccal mucosa, which lines the inside of the cheek, is used for both local and systemic drug delivery. The buccal route is appropriate for proteins, oligonucleotides, and traditional small molecules. Bioadhesive formulations lower dosage requirements and negative effects while increasing medication concentration and boosting bioavailability. For buccal administration, drugs with partition coefficients (40–20,000) and pKa values (2–10) work best.4, 5
Structure of the Oral Cavity:
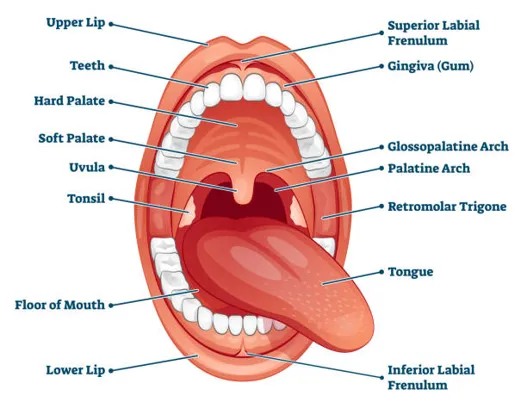
Fig 1: Structure of the Oral Cavity
The Buccal Cavity: The tonsils, floor of the oral cavity, hard and soft palates, cheeks, and lips that surround the vestibule outside the mouth comprise the buccal cavity. The mouth cavity is lined with a thick, dense mucous membrane that is multilayered and highly vascularized.6 Under the mucosal barrier, a network of capillaries and arteries allows drugs to enter the systemic circulation. The term "buccal drug delivery" refers to the release of a medication that may occur when the dosage is placed inside the external vestibule, which is the membrane that covers the cheeks and is situated between the gingival and buccal mucosa.7
Oral Mucosa Overview:
The buccal mucosa is made up of two layers: connective, foundation membrane, and epithelial tissue.
A) Epithelium: The epithelium serves as a barrier against foreign particles and protects the tissue. 40–50 layers of stratified square epithelial cells make up the thickness, which varies from 500 to 800 µm.
B) Connective Tissue and Basement Membrane: The basement membrane separates the connective tissue from the basal layer of epithelium. It is made up of extracellular elements. The bulk of connective tissue is what gives the tissue its mechanical stability, extensibility, and resistance to deformation.8, 9
The Mucosal Layer: Mucus, which resembles a thin, continuous gel coating, is a transparent, viscous, and sticky liquid that sticks to the mucosal epithelial surface. The thickness of this layer in people ranges from 50 to 450 µm. Mucus is produced and secreted by specialized exocrine glands or goblet cells in the epithelial lining. While the precise makeup of the mucus layer varies greatly between animals, regions, and medical situations, it often comprises of the following common components: 10
Table 1: Composition of the Mucosal Layer
|
Water |
95% |
|
Lipids and Glycoproteins |
0.5 to 5% |
|
Mineral salts |
0.5 to 1% |
|
Free Proteins |
0.5 to 1% |
Buccal absorption is influenced by physiological variables:
1. Epithelial Permeability: The epithelial layer controls absorption and affects permeability by acting as a selective barrier. Significantly, more medication absorption is made possible by the sublingual mucosa's higher porosity compared to the buccal mucosa.11
2. Epithelial Thickness: The thickness of the buccal mucosa varies between 500 and 800 µm. Additionally, the thickness varies throughout the oral cavity.
3. Blood supply: With a flow rate of 2.4 ml/min/cm, the rich blood supply of the buccal mucosa allows medication molecules to enter the systemic circulation quickly thanks to the lymphatic network in the lamina propria.
4. Metabolic activity: First-pass processing at the liver or intestinal wall is not necessary because the medication is given directly into the bloodstream. Enzymatically labile medications, like proteins and peptides, are administered via this technique.12
5. Saliva and mucus: The salivary gland regularly secretes 0.5–2L of saliva, which regularly cleans the mucosa of the mouth. By quickly dissolving drugs, the sublingual region's high salivary flow speeds up drug absorption.
6. Retention Capability: The buccal cavity's capacity to hold onto medication delivery devices, like tablets or patches, for a considerable amount of time, enabling prolonged drug release and absorption.13
7. Transport Pathways and Mechanisms: There are two distinct ways that drugs can cross the epithelial barrier:
Table 2: Physiological Factors and Tissue Characteristics Affecting Buccal Drug Absorption
|
Tissue |
Structure |
Epithelial Thickness (µm) |
Permeability |
Residence Time |
Blood (ml/min/cm2 ) |
|
Buccal |
Non keratinized |
500-600 |
Intermediate |
Intermediate |
2.4 |
|
Sublingual |
Non keratinized |
100-200 |
Very good |
Poor |
0.97 |
|
Gingival |
Keratinized |
200 |
Poor |
Intermediate |
1.47 |
|
Palatal |
Keratinized |
250 |
Poor |
Very good |
0.89 |
Overview of Oral Mucosal Tissue:
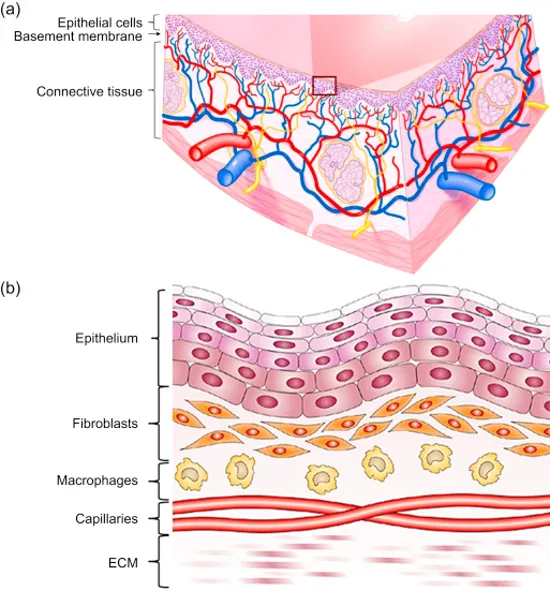
Fig 2: Anatomy of Buccal Mucosa
The oral mucosa's outer layer is made up of a stratified squamous epithelial layer that is covered in mucus and offers underlying tissues mechanical protection. The submucosa and lamina propria are located beneath this layer. The degree of keratinization in the oral mucosa varies; non-keratinized portions, like the buccal mucosa, are more permeable than keratinized areas, including the gingiva and hard palate. Because of its makeup and structure, the oral mucosa might act as the main location in the oral cavity for medication absorption.15
Mucoadhesion:
The most basic definition of adhesion is the "fixing" of surfaces that are adhered to one another. The adherence of an organic or synthetic polymer to a biological substrate is known as bioadhesion in a biological setting; if this adhesion occurs on mucosal membranes or a mucus layer, it is called mucoadhesion.16 Mucoadhesive drug delivery methods improve drug distribution and extend release by utilizing the sticky qualities of particular polymers to target particular body parts. Despite the prevalence of oral delivery, certain drugs are less bioavailable due to first-pass metabolism and acidic stomach conditions. Mucoadhesive methods for non-oral routes like buccal, nasal, and vaginal distribution are being developed to get around these restrictions. Mucoadhesive systems are being employed in continuing research to create a variety of drugs, such as those for angina, hypertension, pain, inflammation, eye disorders, and hormonal treatments. 17
Mucoadhesion Mechanism:
The precise process by which macromolecules adhere to mucosal tissue is yet unknown. The adhesive must be able to spread over the whole surface area in order to facilitate close contact and encourage chain diffusion within the mucus for mucoadhesion to be effective. Attractive and repulsive forces must be balanced during this process, and for mucoadhesion to be successful, the attractive forces must predominate.18 As a result, the mucoadhesion mechanism is divided into two phases: consolidation and contact (Fig.3).
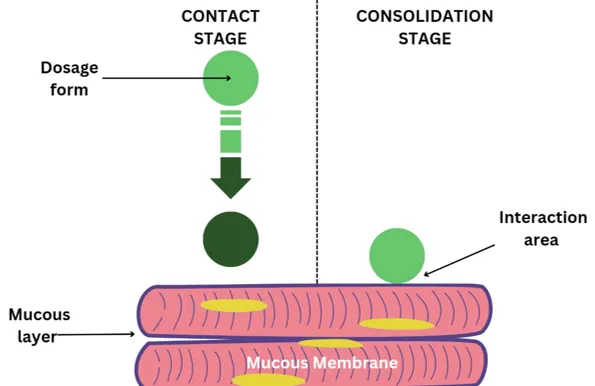
Fig 3: Phases of the Mucoadhesion Mechanism
Stage 1: Mucoadhesion starts when the mucoadhesive comes into touch with the mucous membrane. It then spreads and expands to create a strong attachment with the mucus layer. While nasal administration depends on aerodynamic forces for deposition, vaginal or ocular formulations mechanically assist the contact. Direct adhesion in the gastrointestinal tract is difficult, however oesophageal adhesion and peristaltic motion can helps.19
Stage 2: Moisture activates mucoadhesive molecules during the consolidation stage, which is the second condition. This allows the molecules to relax and form bonds through weakened hydrogen and van der Waals contacts. This phase can be explained by two theories: diffusion theory and dehydration theory. According to diffusion theories, mucoadhesive substances and mucus glycoproteins interact by entangling their chains and generating additional connections, resulting in a combination that extends the duration of contact with the mucous membrane. On the other hand, solid or highly hydrated formulations are less important to the notion of dehydration.20
Fig 4: Theory of Mucoadhesion for Dehydration
Mucoadhesion Theories:
SAB=yB-yA-yAB
The energy required to separate two phases is represented by the adhesion work (WA), which rises when the interfacial energy surpasses the individual surface energies.21
WA=yA+yB-yAB
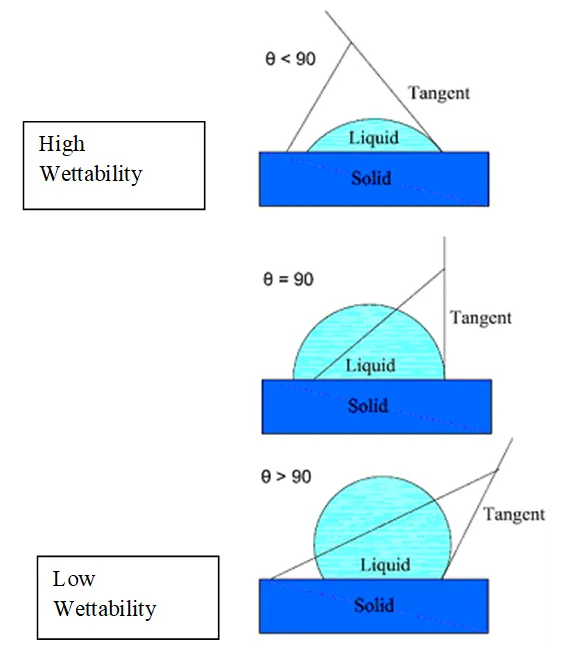
Fig 5: Diagrammatic representation of how contact angle affects bioadhesion.
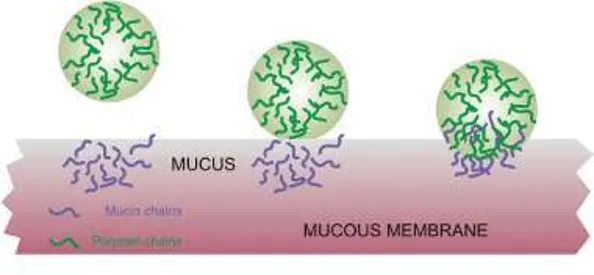
Fig 7: Possible sites of Mucoadhesive bond failure
Buccal Medication Delivery Methods:
Drug distribution via buccal cavity membranes can be divided into the following categories:
1. Buccal Drug Administration: Delivery via the buccal mucosa, which is the cheek's inner lining
2. Drug Sublingual Delivery: Administration via the mucosal membrane beneath the tongue.
3. Transmucosal Drug Delivery: Through the Mucosa delivery via the palate, gums, or other oral mucous membranes.23
Oral Cavity Drug Delivery Benefits:
1. Convenient administration: Therapy is simple to start and stop.
2. Prolonged localized delivery: Enables medications to be released continuously in the oral cavity.
3. Suitable for unconscious patients: Patients who are unconscious or have trouble swallowing can receive this medication.
4. Enhanced bioavailability: Offers a different pathway for systemic medication administration, avoiding first-pass metabolism for some medications. 24
5. Decreased dose and adverse effects: This minimizes dose-dependent side effects by enabling a large dose reduction.
6. Perfect for sensitive medications: Suitable for medications that are broken down by enzymes or unstable in alkaline or acidic settings.
7. No activation is necessary: Absorption does not require activation.
8. Enhanced tissue permeability: Facilitates protease inhibition and targeted tissue permeability modulation.
9. Suitable for patients experiencing nausea or difficulty swallowing: Those who are experiencing nausea, vomiting, or difficulty swallowing may use this medication.
10. Sufficient drug dissolution: Saliva ensures that there is sufficient water to dissolve the drug.25, 26
Limitations of Buccal Drug Delivery:
1. Mucosal irritation and unpleasant taste/odour: Drugs causing irritation or having unpleasant characteristics are unsuitable.
2. pH instability: Drugs unstable at buccal pH cannot be administered via this route.
3. Dose limitations: Only drugs requiring small doses can be delivered bucally.
4. Limited absorption mechanisms: Only drugs absorbed through passive diffusion can be administered bucally.
5. Practical challenges: Eating and drinking may be restricted, and tablets may be swallowed accidentally.
6. Variable bioavailability: Buccal delivery can result in unpredictable bioavailability due to low permeability for most drugs.27, 28
CONCLUSIONS
A potential area of research is buccal mucoadhesive drug administration, which provides a gentle method for the systemic distribution of strong peptide/protein molecules and poorly absorbed oral medications. The creation of safe and efficient permeation enhancers is necessary to advance buccal medication delivery. Predicting, tracking, and regulating delivery rates, biodegradation, and site-specific targeting are critical to maximizing therapeutic results. When administering medications that are susceptible to intestinal enzymes, gastric pH, or the hepatic first pass effect, the buccal mucosa offers a practical substitute. Mucoadhesive systems will probably be essential to novel drug delivery strategies as new medications are developed.
REFERENCES


Kanchan Tarle, Mitesh Sonawane, A Systemic Review on Mucoadhesive Buccal Tablet, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1142-1151. https://doi.org/10.5281/zenodo.20550691
 10.5281/zenodo.20550691
10.5281/zenodo.20550691