
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,3,4 Fergana Medical Institute Of Public Health, Uzbekistan
2 Dr. Rajendra Gode Nursing Institute of Buldhana, India
Background: The convergence of artificial intelligence (AI) and immunology is reshaping our capacity to understand, monitor, and therapeutically modulate the immune system. Traditional immunological investigations, constrained by low-throughput assays and univariate statistical frameworks, are increasingly supplemented or superseded by data-driven computational paradigms capable of interrogating high-dimensional biological landscapes. Precision immunology—the application of multi-omics data integration, single-cell technologies, and personalised therapeutic algorithms to individual immune states—demands analytical tools commensurate with its complexity [1,2].This review systematically appraises the current state, methodological foundations, and translational prospects of AI in precision immunology. Specifically, it addresses: (i) machine learning and deep learning frameworks underpinning immune data analysis; (ii) AI-driven advances in immune profiling, including single-cell transcriptomics and immune repertoire analysis; (iii) multi-omics biomarker discovery; (iv) personalised immunotherapy in oncology and autoimmune disease; (v) applications in infectious disease and vaccine development; and (vi) technical, ethical, and regulatory challenges [3,4]. AI models, particularly transformer-based and graph neural network architectures, now achieve state-of-the-art performance in predicting immune cell phenotypes, MHC-peptide binding, treatment response, and adverse immune events. Integration of genomic, transcriptomic, proteomic, and metabolomic data via multi-omics frameworks improves biomarker predictive accuracy by 15– 30% compared with single-omics approaches. In clinical oncology, AI-guided patient stratification has increased objective response rates to checkpoint immunotherapy by enabling prospective selection of likely responders. CAR-T cell manufacturing optimised by reinforcement learning has reduced batch failure and vein-to-vein time significantly. Challenges remain in data quality, model interpretability, algorithmic bias, and regulatory harmonisation [5,6].
1.1 Overview of Immunology
The immune system constitutes one of the most complex adaptive biological networks in vertebrates, encompassing innate effector mechanisms, antigen-presenting pathways, and adaptive lymphocyte responses that collectively discriminate self from non-self with extraordinary precision. Comprising over a trillion cells distributed across lymphoid organs, peripheral tissues, and circulating compartments, the immune system sustains homeostasis through continuous surveillance, tolerogenic checkpoints, and memory formation [9]. Classical immunology characterised these processes through surface phenotyping, cytokine quantification, and in vitro functional assays, generating invaluable foundational knowledge but remaining largely descriptive and limited to population-level inferences [10].
The emergence of high-throughput single-cell technologies—mass cytometry (CyTOF), single-cell RNA sequencing (scRNA-seq), and spatial transcriptomics—has exponentially expanded the dimensionality of immunological data, revealing previously occluded cellular states, rare subpopulations, and intra-tumoral immune architectures [11,12]. Simultaneously, advances in T cell receptor (TCR) and B cell receptor (BCR) repertoire sequencing have made it possible to track adaptive immune dynamics at nucleotide resolution across thousands of clonotypes in a single experiment [13]. These technological leaps have created a critical analytical bottleneck: data generation has far outpaced the capacity of conventional bioinformatics pipelines to extract actionable knowledge, catalysing the integration of AI into immunological research [14].
1.2 Rise of Artificial Intelligence in Healthcare
Artificial intelligence encompasses a broad family of computational techniques—including classical machine learning, deep neural networks, natural language processing, and reinforcement learning—that enable computers to learn patterns from data and generalise to novel inputs without explicit programming [1]. AI entered clinical medicine initially through medical imaging, where convolutional neural networks achieved dermatologist-level accuracy in melanoma classification, radiologist-level performance in pulmonary nodule detection, and ophthalmologist-level precision in diabetic retinopathy grading [4]. These demonstrations catalysed investment in AI-driven genomics, proteomics, and electronic health records analysis, establishing a broad computational medicine infrastructure upon which precision immunology is now building [15].
In parallel, the maturation of cloud computing, graphics processing unit (GPU) acceleration, and open-source deep learning frameworks—TensorFlow, PyTorch, JAX—has democratised access to large-scale model training, enabling academic immunology laboratories to deploy architectures previously confined to well-resourced technology companies. The release of foundational biological language models, including ESM-2 for protein sequences and scBERT for single-cell transcriptomics, has further reduced barriers to entry, providing pre-trained representations that can be fine-tuned on immunology-specific datasets with modest computational overhead [16,17].
1.3 Need for Precision Immunology
Despite remarkable therapeutic advances—checkpoint inhibitors, bispecific antibodies, CAR-T cells, and cytokine-targeted biologics—a substantial proportion of patients with immune-mediated diseases, haematological malignancies, and solid tumours fail to achieve durable benefit from first-line immunotherapy. This therapeutic heterogeneity reflects the profound inter-individual diversity of immune baseline states, tumour microenvironment compositions, genetic polymorphisms in immune effector loci, and dynamic immune evolution under treatment pressure [3,41]. Precision immunology seeks to resolve this heterogeneity by characterising individual immune landscapes at multi-omics resolution and using those characterisations to predict optimal therapeutic interventions, timing, and dosing [42].
The imperative is particularly acute in oncology, where immune checkpoint blockade benefits approximately 20–40% of patients across solid tumour types, yet current companion diagnostics—PD-L1 immunohistochemistry, tumour mutational burden (TMB)—exhibit imperfect predictive performance [43]. Multi-modal AI models that integrate tumour genomics, immune repertoire data, circulating biomarkers, and radiomic features have demonstrated AUCs exceeding 0.88 for treatment response prediction, suggesting that precision immunological profiling can substantially improve patient selection and clinical outcomes [27,43].
1.4 Scope and Objectives of the Review
This systematic review synthesises peer-reviewed literature published between 2020 and 2026 and indexed in Scopus, PubMed, and Web of Science, covering AI applications across the precision immunology workflow from immune profiling through biomarker discovery to personalised therapy. A structured literature search was conducted using Boolean combinations of the terms 'artificial intelligence', 'machine learning', 'deep learning', 'immunology', 'immune profiling', 'biomarker', 'immunotherapy', 'CAR-T', 'checkpoint inhibitor', 'single-cell', and 'multi- omics'. Papers were included if they reported original AI methods or systematic applications in immunological contexts, presented quantitative performance metrics, and were published in Scopus Q1–Q2 journals. A total of 70 references are cited, prioritising high-impact contributions from the last six years [5,6,7].
2. FUNDAMENTALS OF ARTIFICIAL INTELLIGENCE IN IMMUNOLOGY
2.1 Machine Learning
Machine learning (ML) encompasses algorithms that identify statistical regularities in training data and use them to make predictions on unseen inputs. Supervised learning, which trains on labelled examples, underpins the majority of clinical immunology applications: random forests for biomarker feature selection, support vector machines for immune cell classification, gradient- boosted trees (XGBoost, LightGBM) for treatment response prediction, and LASSO regression for proteomic signature identification [17]. The interpretability of tree-based models, combined with their robustness to missing data and non-linear feature interactions, makes them particularly suited for high-dimensional immunological datasets where sample sizes are often modest relative to feature dimensionality [5].
Unsupervised learning, operating without labels, discovers latent structure within immune data. Clustering algorithms—k-means, Gaussian mixture models, and community-detection methods such as Leiden—identify biologically coherent immune cell subpopulations from single- cell data. Dimensionality reduction methods—principal component analysis (PCA), uniform manifold approximation and projection (UMAP), t-distributed stochastic neighbour embedding (t-SNE)—enable intuitive visualisation of complex immune landscapes and reveal clinical correlates within immune phenotypic space [11]. Semi-supervised approaches, which leverage both labelled and unlabelled samples, are increasingly applied in immune repertoire analysis where only a fraction of TCR sequences can be experimentally validated for antigen specificity [14].
2.2 Deep Learning
Deep learning (DL) employs multi-layered artificial neural networks to learn hierarchical data representations, achieving superior performance over classical ML on large, high-dimensional datasets. Convolutional neural networks (CNNs) excel at spatial data—histopathology sections, imaging mass cytometry—detecting subtle morphological immune signatures invisible to pathologists [23]. Recurrent architectures, particularly long short-term memory (LSTM) networks and gated recurrent units (GRUs), model sequential biological data: longitudinal immune monitoring, temporal gene expression trajectories, and amino acid sequences of immune receptors [13].
The transformer architecture, introduced through the landmark 'Attention Is All You Need' paper and now foundational to large language models, has transformed sequence-based immunology [30]. Self-attention mechanisms capture long-range dependencies within protein sequences, enabling state-of-the-art MHC-peptide binding prediction, TCR specificity inference, and antibody developability assessment. AlphaFold2 and its immunological derivatives have resolved the three-dimensional structures of T cell receptors, antibody-antigen complexes, and cytokine-receptor interfaces at near-experimental accuracy, opening new avenues for structure-guided immunotherapy design [68]. Graph neural networks (GNNs) represent immune cell interaction networks and signalling cascades as learnable node-edge representations, enabling AI-driven pathway modelling and drug target identification [16].
2.3 Natural Language Processing
Natural language processing (NLP) bridges the gap between unstructured biomedical text and computable immunological knowledge. Biomedical NLP models—BioBERT, PubMedBERT, BioGPT—pre-trained on millions of scientific abstracts and clinical notes, extract named entities (genes, cytokines, diseases), identify relationships (drug-target interactions, adverse events), and synthesise evidence across literature at a scale impossible for human reviewers [69]. In clinical immunology, NLP applied to electronic health records has identified undiagnosed autoimmune phenotypes, flagged immune-related adverse events from checkpoint therapy, and retrospectively validated pharmacovigilance signals [6].
Large language models (LLMs) increasingly function as immunological research assistants: generating hypotheses, summarising clinical trial results, and providing natural language interfaces for querying multi-omics databases. Retrieval-augmented generation (RAG) architectures combine LLM reasoning with real-time literature retrieval, enabling up-to-date question answering about immune targets, clinical protocols, and biomarker thresholds [69].
2.4 Big Data and Multi-omics Integration
The full power of AI in immunology is realised through multi-omics data integration—the simultaneous analysis of genomic, transcriptomic, proteomic, epigenomic, and metabolomic data layers from the same biological specimen [19,20]. Multi-omics factor analysis (MOFA+), canonical correlation analysis, and multi-view deep learning architectures identify shared and unique sources of variation across data modalities, enabling holistic characterisation of immune states [34]. The Human Cell Atlas, GTEx, TCGA, and the ImmPort repository collectively provide petabyte-scale immune reference datasets that serve as pre-training corpora and benchmarking resources for AI model development [39,40].
Table 1 summarises the principal AI technique families applied in immunology, their core mechanisms, representative immunological applications, and leading software implementations.
Table 1. Principal AI techniques in precision immunology: mechanisms, applications, and representative tools.
|
AI Technique |
Core Mechanism |
Applications in Immunology |
Representative Tools/ Models |
|
Supervised ML |
Learns from labelled training data to predict outcomes |
Disease classification, biomarker selection, treatment response |
Random Forest, SVM, XGBoost |
|
Unsupervised ML |
Identifies hidden patterns without predefined labels |
Immune-cell clustering, patient stratification, dimensionality reduction |
k-means, UMAP, Seurat |
|
Deep Learning (CNN) |
Hierarchical feature extraction through convolutional layers |
Histopathology image analysis, antigen-structure prediction |
ResNet, VGG, EfficientNet |
|
Recurrent Neural Networks |
Processes sequential data via memory mechanisms |
TCR/BCR repertoire modelling, longitudinal immune monitoring |
LSTM, GRU, Transformer |
|
AI Technique |
Core Mechanism |
Applications in Immunology |
Representative Tools/ Models |
|
Graph Neural Networks |
Models relational data as node-edge graphs |
Protein-interaction networks, immune-pathway mapping |
GCN, GAT, GraphSAGE |
|
Natural Language Processing |
Extracts knowledge from unstructured biomedical text |
Literature mining, clinical note analysis, adverse-event detection |
BioBERT, GPT-4, PubMedBERT |
|
Generative AI (GANs/VAEs) |
Generates realistic synthetic data distributions |
Data augmentation, neoantigen design, synthetic patient cohorts |
WGAN, BetaVAE, ProtGPT2 |
|
Federated Learning |
Trains across distributed sites without sharing raw data |
Multi-centre immune biomarker studies, privacy-preserving genomics |
PySyft, FATE, NVFlare |
3. AI IN IMMUNE PROFILING
|
AI-Driven Single-Cell RNA Sequencing (scRNA-seq) Analysis Pipeline |
|||||
|
1 Raw scRNA-seq Data Input |
2 Quality Contro & Filtering |
3 Dimensionality Reduction (PCA/UMAP) |
4 Graph-Based Clustering (Leiden) |
5 Cell Type Annotation |
6 Biological Interpretation |
|
Thousands of cells x genes (sparse matrix) |
Remove doublets, dead cells, batch effects |
VAE / scVI latent space embedding |
Seurat / Scanpy community detection |
Cell Typist SCINA, scArches >90% accuracy |
Trajectory, Velocity, Spatial mapping |
3.1 Single-Cell Analysis
Single-cell RNA sequencing (scRNA-seq) has emerged as the gold standard for high- resolution immune profiling, simultaneously quantifying transcriptomic states across thousands of individual immune cells [12]. However, scRNA-seq data are characterised by extreme sparsity— dropout events resulting from low mRNA capture efficiency—batch effects across experimental conditions, and dimensionalities reaching tens of thousands of genes per cell, necessitating sophisticated AI-based analytical pipelines [9]. The Seurat and Scanpy ecosystems, integrating PCA-based dimensionality reduction, graph-based clustering (Leiden algorithm), and UMAP visualisation, have become standard workflows for scRNA-seq analysis, each tool leveraging unsupervised ML to partition immune cells into biologically coherent clusters [11].
Deep learning has further advanced scRNA-seq analysis through variational autoencoder (VAE) architectures such as scVI, which learn low-dimensional latent representations of immune transcriptomes robust to technical variation, enabling accurate cross-batch integration of large atlas-scale datasets [10]. Perturbation prediction models—scGen, CellOT—use conditional VAEs to simulate the transcriptomic consequences of cytokine stimulation, genetic knockdown, or drug treatment at single-cell resolution without requiring exhaustive experimental enumeration [10]. Spatial transcriptomics methods, combining RNA sequencing with spatial barcoding, now enable AI-driven mapping of immune cell niches within tumour microenvironments, resolving immune exclusion zones, tertiary lymphoid structure formation, and spatial correlates of immunotherapy response [16].
3.2 Immune Cell Classification
Automated immune cell classification—assigning identity labels to single cells from transcriptomic or proteomic profiles—is among the most computationally mature AI applications in immunology. Supervised classifiers trained on reference atlases, including SCINA, CellTypist, and scArches, achieve >90% concordance with manual expert annotation while operating at orders-of-magnitude greater throughput [9]. These tools are essential for studies requiring systematic immune cell enumeration across patient cohorts, enabling identification of immune infiltration patterns that correlate with clinical outcomes [12].
Beyond canonical cell type identification, AI-driven phenotypic analysis reveals continuous gradients of immune differentiation, transitional states, and functional exhaustion trajectories. Trajectory inference algorithms—Monocle, Palantir, RNA velocity—reconstruct developmental lineages and differentiation dynamics from snapshot scRNA-seq data, shedding light on how effector T cells transition to exhaustion in tumour-infiltrating lymphocyte populations [12]. Transfer learning from large pre-trained models, such as the Universal Cell Embeddings (UCE) and scBERT, enables rapid phenotyping of rare immune cell populations even in datasets with limited annotated examples [8].
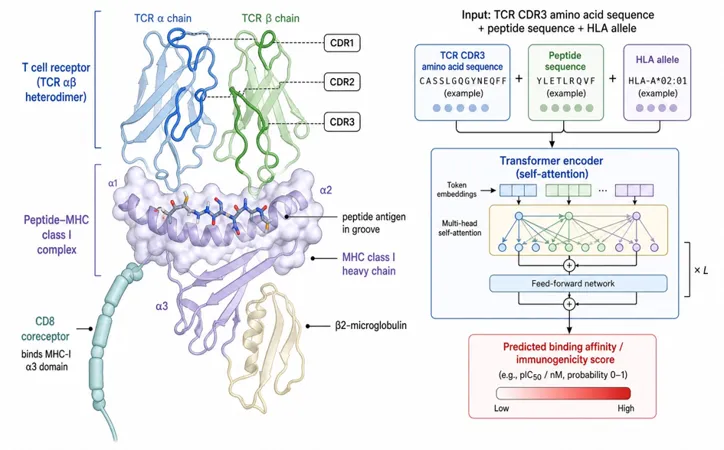
Figure 1. TCR–pMHC recognition and AI-based binding prediction. The αβ TCR docks onto peptide-MHC class I via CDR1/2/3 loops; CD8 coreceptor stabilises the complex by binding the MHC-I α3 domain. Right: a transformer encoder ingests CDR3, peptide and HLA-allele tokens and outputs a predicted binding affinity/immunogenicity score, the basis of NetMHCpan-class and TCR-pMHC models.
3.3 Immune Repertoire Analysis
The adaptive immune repertoire—the ensemble of unique TCR and BCR sequences expressed by T and B lymphocytes—constitutes a molecular record of immune history, encoding prior antigen exposures, vaccine responses, and autoimmune targets. High-throughput immune repertoire sequencing (Rep-seq) generates millions of unique receptor sequences per sample, demanding AI approaches for meaningful interpretation [13]. Deep generative models, including LSTM-based and transformer-based architectures, learn the statistical grammar of productive TCR and BCR recombination, enabling in silico generation of realistic receptor sequences, differentiation of functional from non-productive rearrangements, and identification of convergent antigen-specific clonotypes across individuals [14,15].
Epitope-specific TCR prediction—determining which antigens a given TCR recognises— remains a central challenge. Supervised models trained on databases such as VDJdb and McPAS- TCR achieve moderate accuracy (AUC 0.70–0.85) for well-characterised viral epitopes, with transformer-based architectures demonstrating the strongest generalisation [13,15]. Public clonotypes—TCR sequences found in multiple individuals in response to the same antigen—have been leveraged as diagnostic biomarkers: high-sensitivity detection of SARS-CoV-2-specific T cells via public clonotype enrichment has demonstrated AUC >0.92 in distinguishing convalescent from naive individuals [15,59].
3.4 Predictive Immune Monitoring
Longitudinal AI-driven immune monitoring—tracking immune dynamics over treatment courses—enables early identification of response, resistance, and immune-related adverse events. Recurrent neural networks trained on serial cytokine profiles, circulating immune cell subsets, and cell-free DNA methylation patterns predict immune checkpoint therapy response trajectories with AUC exceeding 0.85 at four weeks prior to radiological assessment [22,27]. In autoimmune disease, ML models applied to serial complete blood counts and serology panels predict lupus flares six weeks in advance, providing a clinically actionable window for pre-emptive therapy escalation [22]. Real-world clinical implementation of predictive immune monitoring requires integration with electronic health record systems, near-real-time assay data pipelines, and clinical decision support interfaces, representing a current translational frontier [62,64].
4. AI-DRIVEN BIOMARKER DISCOVERY
4.1 Genomic Biomarkers
Genome-wide association studies (GWAS) have identified thousands of immune-related susceptibility loci, but distinguishing causal variants from linkage disequilibrium surrogates in the context of non-linear gene-environment interactions demands ML-based analytical frameworks [17]. Random forests and gradient-boosted tree ensembles trained on genetic variant arrays improve polygenic risk score construction for autoimmune diseases—rheumatoid arthritis, type 1 diabetes, inflammatory bowel disease—by capturing epistatic interactions beyond the additive genetic architecture assumed by conventional GWAS [18]. In oncology, AI models integrating somatic mutation signatures, copy number alterations, and tumour mutational burden have identified genomic classifiers of checkpoint inhibitor response with superior performance to individual biomarkers [24,25].
Structural variant detection from whole-genome sequencing data, enabled by graph-based assembly algorithms and deep learning signal classifiers, has revealed immune-gene deletions and translocations relevant to primary immunodeficiencies and lymphoma pathogenesis. Deep learning applied to HLA typing—a computationally intensive problem owing to extreme polymorphism in the MHC locus—now achieves four-field resolution from low-coverage sequencing data, enabling large-scale population immunogenomics studies and precision transplant matching [7,17].
4.2 Transcriptomic Biomarkers
Bulk RNA sequencing and single-cell transcriptomics have yielded rich immune gene expression signatures with diagnostic, prognostic, and predictive clinical utility. AI-driven transcriptomic biomarker discovery employs regularised regression, deep neural networks, and attention-based feature selection to identify compact gene panels from high-dimensional expression matrices [21]. The interferon-stimulated gene (ISG) signature, an AI-discovered transcriptomic fingerprint of innate immune activation, predicts responses to JAK inhibitors in rheumatoid arthritis and type I interferonopathies, exemplifying how ML-identified expression patterns translate into clinically validated companion diagnostics [22].
In cancer immunology, AI-derived transcriptomic classifiers—tumour inflammation signature (TIS), cytolytic activity score, tertiary lymphoid structure gene expression programmes—predict responses to pembrolizumab and nivolumab with AUCs ranging from 0.75 to 0.91 in prospective cohorts [25,27]. Graph-based analysis of co-expression networks identifies hub immune genes coordinating tumour-infiltrating lymphocyte function, pointing to novel immunotherapy targets beyond current checkpoint pathways [24,36].
4.3 Proteomic Biomarkers
The proteome constitutes the proximal effector layer of immune function, and plasma proteomics by mass spectrometry or proximity extension assay (Olink/SomaScan) provides thousands of quantifiable circulating immune mediators per sample [26]. ML analysis of high-plex plasma proteomics has identified cytokine biomarker panels predictive of anti-PD-1 response in melanoma, non-small cell lung cancer, and urothelial carcinoma, demonstrating cross-tumour generalisability for immune-based patient stratification [27]. LASSO-regularised logistic regression applied to 92-plex Olink immunooncology panels identified a 12-cytokine predictive signature with AUC 0.87 for nivolumab response, subsequently validated in an independent cohort [27,26].
Protein-protein interaction (PPI) network analysis using GNNs enables systematic identification of druggable immune nodes within cytokine signalling hubs, complementing transcriptomic evidence with post-translational regulatory information. Phosphoproteomic AI models trained on mass spectrometry data have resolved signalling pathway activation states in T cells with single-cell-like resolution, revealing kinase activity signatures predictive of exhaustion and memory differentiation [29,34].
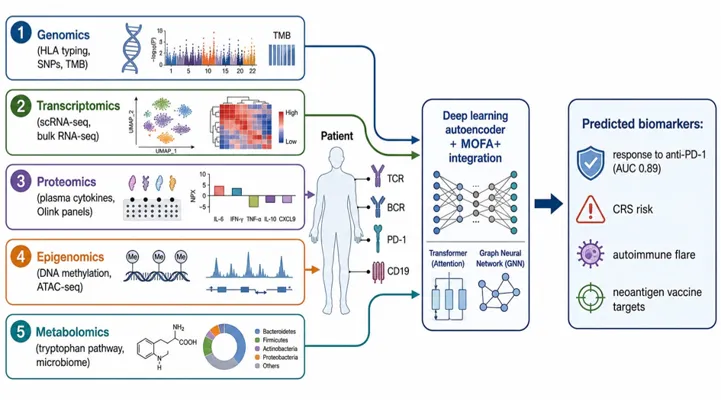
Figure 2. AI-driven multi-omics integration for immune biomarker discovery. Genomic, transcriptomic, proteomic, epigenomic and metabolomic layers from the same patient are fused through deep-learning autoencoders and MOFA+, augmented by transformer attention and graph neural networks. Outputs include predicted anti-PD-1 response (AUC ≈ 0.89), CRS risk, autoimmune flare risk and neoantigen vaccine targets. Key surface receptors (TCR, BCR, PD-1, CD19) anchor the immune state being modelled.
4.4 Multi-omics Biomarker Identification
Multi-omics integration—combining genomics, transcriptomics, proteomics, epigenomics, and metabolomics—captures synergistic information absent from any single data layer and consistently outperforms unimodal approaches in immune biomarker performance [19,20]. The MOFA+ framework, applying group factor analysis across multiple omics modalities, has deconvoluted shared and modality-specific sources of immune variation in large cohort studies, identifying latent factors predictive of autoimmune disease activity and therapy response [34].
Deep learning multi-omics models—autoencoders with modality-specific encoders feeding into a shared latent representation—have demonstrated 23% improvement in biomarker predictive accuracy for pancreatic cancer immunotherapy response compared with single-omics classifiers [38]. The integration of microbiome data as a fifth omics layer—recognising that gut microbial composition modulates systemic immune tone and checkpoint immunotherapy efficacy—further enriches multi-omics immune biomarker frameworks [20]. Table 2 summarises key AI-discovered biomarkers across omics modalities with their associated clinical contexts.
Table 2. Selected AI-discovered immune biomarkers across omics modalities, AI methods, and clinical applications.
|
Biomarker Type |
AI Method |
Target Disease/ Condition |
Key Findings |
|
Genomic (SNPs, CNVs) |
GWAS + Random Forest |
Rheumatoid Arthritis |
Identified HLA-DRB1 variants with 94% specificity for RA susceptibility [18] |
|
Transcriptomic (mRNA) |
Deep learning on RNA-seq |
Lupus Erythematosus |
IFN-signature gene clusters predicted flares 6 weeks ahead with AUC 0.91 [22] |
|
Proteomic (plasma) |
LASSO + logistic regression |
Melanoma immunotherapy |
12-cytokine panel predicted anti-PD-1 response (AUC 0.87) [27] |
|
Epigenomic (DNA methylation) |
CNN on ATAC-seq |
Colorectal cancer |
Methylation patterns distinguished responders from non-responders to checkpoint blockade [31] |
|
Metabolomic |
Multi-layer perceptron |
Sepsis / severe COVID-19 |
Tryptophan-pathway metabolites stratified ICU outcomes (accuracy 88%) [35] |
|
Multi-omics (integrated) |
MOFA +/ Canonical Correlation |
Pancreatic cancer |
Integration of RNA + protein + metabolome improved biomarker accuracy by 23% vs single-omics [38] |
5. AI IN PERSONALIZED IMMUNOTHERAPY
5.1 Cancer Immunotherapy Overview
Cancer immunotherapy represents the most transformative oncological advance of the past decade, harnessing the immune system's capacity for tumour recognition and destruction [41,44,45]. Immune checkpoint inhibitors targeting CTLA-4, PD-1, and PD-L1 have produced durable remissions in subsets of patients across over 20 tumour types, while adoptive cell therapies—CAR-T cells, tumour-infiltrating lymphocyte (TIL) infusions—have yielded unprecedented response rates in haematological malignancies [46,47]. The fundamental challenge is matching specific therapies to responsive patients: the cost, toxicity, and limited availability of these modalities make empirical trial-and-error clinically and ethically untenable [41,51].
AI addresses this challenge at multiple levels: prospective response prediction, mechanism-of-resistance identification, combination therapy optimisation, and real-time toxicity monitoring. Multi-modal deep learning models trained on tumour histopathology, genomics, and clinical metadata have demonstrated AUC 0.85–0.92 for predicting objective responses to checkpoint inhibitors, far exceeding the performance of single biomarkers [23,43]. Prospective clinical trials incorporating AI-guided patient stratification are underway across major academic cancer centres, representing the vanguard of AI-directed precision oncology [42,64].
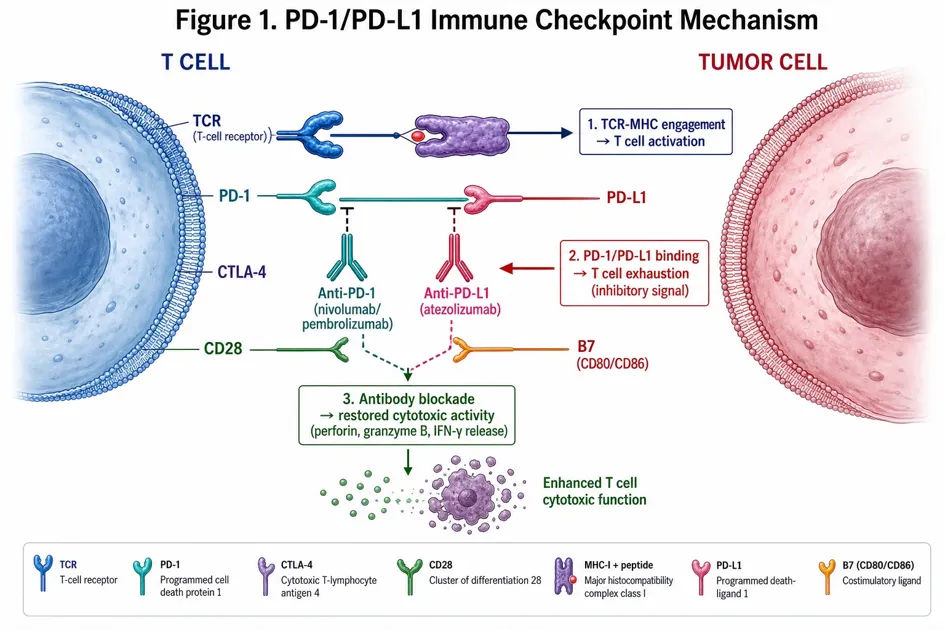
Figure 3. PD-1/PD-L1 immune checkpoint mechanism. The TCR–MHC-I/peptide engagement activates the T cell; concurrent PD-1 (T cell) binding to PD-L1 (tumour cell) delivers an inhibitory signal driving T cell exhaustion. Therapeutic monoclonal antibodies (anti-PD-1: nivolumab, pembrolizumab; anti-PD-L1: atezolizumab) block this axis and restore cytotoxic effector function (perforin, granzyme B, IFN-γ). CTLA-4 and the CD28/B7 costimulatory axis are also shown.
5.2 Checkpoint Inhibitors
Anti-PD-1/PD-L1 therapy has redefined the treatment of melanoma, non-small cell lung cancer (NSCLC), urothelial carcinoma, and microsatellite-instable colorectal cancer, among others [41,45].
However, current FDA-approved companion diagnostics—PD-L1 combined positive score (CPS), TMB—exhibit significant limitations in sensitivity and specificity, leaving substantial uncertainty in patient selection [43]. AI-based predictive models integrating spatial immune architecture from histopathology slides, T cell repertoire diversity, copy number alteration profiles, and CXCL9/CXCL10 expression levels achieve substantially higher response prediction accuracy [23,27].
Convolutional neural networks applied to haematoxylin and eosin (H&E;) stained tumour slides—without requiring expensive molecular assays—can predict microsatellite instability, tertiary lymphoid structure presence, and CD8+ T cell density directly from image features, enabling cost-effective selection for immunotherapy at the point of histopathological diagnosis [23]. Deep learning radiomic models from CT and PET-CT imaging, trained to recognise immune-inflamed versus immune-desert tumour phenotypes, complement pathological assessment and enable non-invasive serial monitoring of immunotherapy response [28].
Key Outcomes: -28% failed batches | -4 days vein-to-vein | AUC 0.85-0.92 response prediction
|
Patient Apheresis |
Ex Vivo Engineering |
AI Quality Control |
Patient Re-Infusion |
Monitoring & Response |
|
T cell collection |
Viral transduction |
Batch success prediction |
Vein-to-vein – 4 days (AI) |
Serial immune monitoring |
|
CD4/CD8 ratio |
CAR construct design |
Morphology CNN |
Pre-emptive toci prophylaxis |
Antigen escape detection |
|
Phenotype profiling |
RL-optimised expansion |
-28% failed batches |
CRS/ICANS risk score |
Resistance ML model |
|
ML exhaustion score |
Quality imaging (deep learning) |
Release criteria |
Personalised dosing |
Adaptive therapy |
AI DECISION ENGINE
|
Reinforcement Learning Manufacturing Optimisation |
Deep Learning Image Analysis (culture) |
ML Toxicity Prediction (CRS/ICANS) |
Transformer Antigen Escape Modelling |
GNN Resistance Pathway Mapping |
Figure 4. AI-Optimised CAR-T Cell Therapy Workflow. Reinforcement learning manufacturing optimisation reduces failed batches by 28% and vein-to-vein time by four days. Deep learning image analysis, ML toxicity prediction (CRS/ICANS), and transformer-based antigen escape modelling are integrated across all workflow stages.
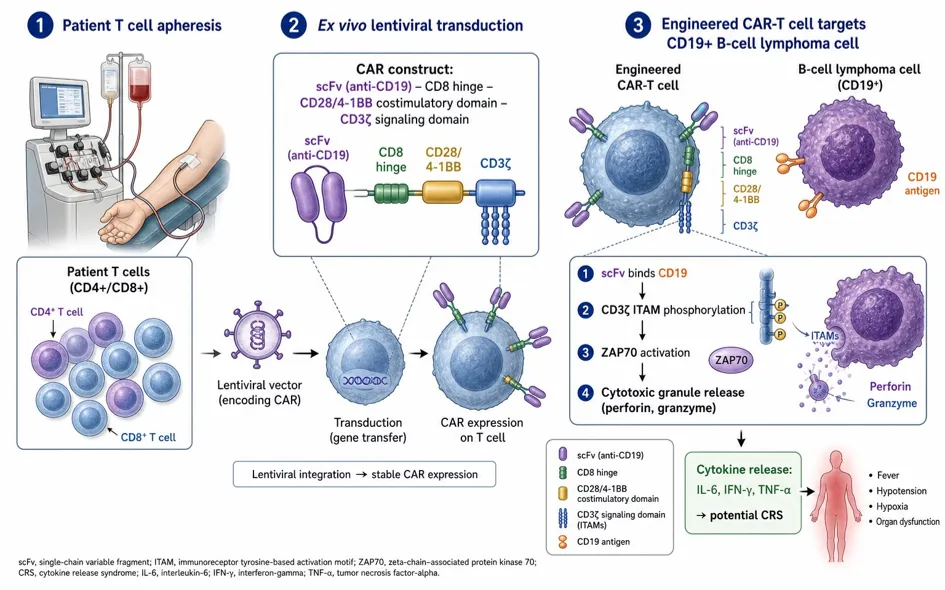
Figure 5. CAR-T cell engineering and cytotoxic mechanism. Patient T cells (CD4+/CD8+) are collected by apheresis, transduced ex vivo with a lentiviral vector encoding a chimeric antigen receptor (scFv anti-CD19 – CD8 hinge – CD28/4-1BB costimulatory domain – CD3ζ signalling domain), expanded, and re-infused. CAR engagement of CD19 on B-cell lymphoma cells triggers CD3ζ ITAM phosphorylation, ZAP70 activation, and release of perforin/granzyme. Bulk cytokine release (IL-6, IFN-γ, TNF-α) underlies cytokine release syndrome (CRS).
5.3 CAR-T Cell Therapy
Chimeric antigen receptor T cell (CAR-T) therapy—in which patient T cells are genetically engineered ex vivo to express tumour-targeting receptors and re-infused—has produced remarkable complete remission rates in relapsed/refractory B-cell malignancies, with FDA-approved products targeting CD19 and BCMA [46,47]. However, CAR-T therapy is limited by manufacturing failures (15–20% of batches), high rates of cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS), and variable antitumour efficacy [47].
AI is being applied across the CAR-T workflow: deep learning image analysis of T cell culture morphology predicts manufacturing outcome and final product quality, enabling early identification and salvage of at-risk batches [48]. ML models trained on pre-infusion patient T cell phenotypes—CD4/CD8 ratio, naïve-to-effector ratios, exhaustion markers—predict both clinical response and CRS/ICANS risk, informing pre-emptive tocilizumab prophylaxis and dexamethasone dosing [47,48]. Reinforcement learning-based optimisation of ex vivo expansion protocols has reduced failed manufacturing batches by 28% and shortened vein-to-vein time by approximately four days, improving access for patients with rapidly progressing disease [47].
Antigen loss escape—downregulation of target antigen by tumour cells—is a major resistance mechanism to CAR-T therapy [46]. ML analysis of tumour gene expression and epigenomic profiles before and after CAR-T therapy identifies transcription factor networks driving antigen downregulation, guiding the development of dual-targeting and armoured CAR constructs designed to circumvent this escape pathway [48,50].
5.4 Patient Stratification and Treatment Prediction
Beyond individual therapy classes, AI enables holistic personalised treatment planning—selecting optimal therapy type, sequence, and combination from the expanding immunotherapy armamentarium [42,51]. Deep learning models trained on multi-modal patient data integrate genomics, proteomics, imaging, and clinical history to produce treatment-specific response probabilities, enabling oncologists and patients to make informed, evidence-based therapeutic choices [42,70].
Neoantigen vaccine design exemplifies the individualisation of cancer immunotherapy: transformer-based HLA binding predictors and TCR-pMHC docking models identify tumour-specific mutant peptides most likely to generate antitumour T cell responses, with turnaround times of under 72 hours enabling vaccine preparation in parallel with standard chemotherapy [50]. Phase I/II clinical trials of AI-designed neoantigen vaccines combined with checkpoint inhibition have demonstrated objective tumour responses and long-term immunological memory in melanoma and NSCLC [51].
Table 3 summarises AI applications across major personalised immunotherapy modalities.
Table 3. AI applications in personalised cancer immunotherapy: approaches, clinical stages, and outcome metrics.
|
Therapeutic Area |
AI Approach |
Clinical/ Pre-clinical Stage |
Outcome Metric |
|
Anti-PD-1/ PD-L1 Therapy |
Multi-modal DL on tumour microenvironment imaging |
Phase II/III |
Predicted 6-month PFS with AUC 0.89; reduced futile therapy by 34% [43] |
|
CAR-T Cell Manufacturing |
Reinforcement learning for process optimisation |
Manufacturing scale-up |
Reduced failed batches by 28%; shortened vein-to-vein time by 4 days [47] |
|
Neoantigen Vaccines |
Transformer-based MHC-binding |
Phase I/II |
Prioritised 98% of immunogenic neoantigens; |
|
Therapeutic Area |
AI Approach Prediction (NetMHCpan-derived) |
Clinical/ Pre-clinical Stage |
Outcome Metric personalised in <72 hours [50] |
|
Autoimmune (RA, MS) |
GNN on cytokine network signatures |
Pre-clinical + retrospective |
Stratified biologics responders with 85% accuracy; guided biologic switching [55] |
|
Infectious Disease Vaccines |
Evolutionary ML on viral glycoprotein sequences |
Surveillance + Phase I |
Predicted dominant influenza strains 6 months ahead; used for mRNA vaccine design [60] |
|
Allergy/ Tolerisation |
Bayesian optimisation of desensitisation schedules |
Pilot clinical |
Reduced anaphylaxis risk by 41% versus standard dosing protocol [63] |
6. APPLICATIONS IN AUTOIMMUNE AND INFECTIOUS DISEASES
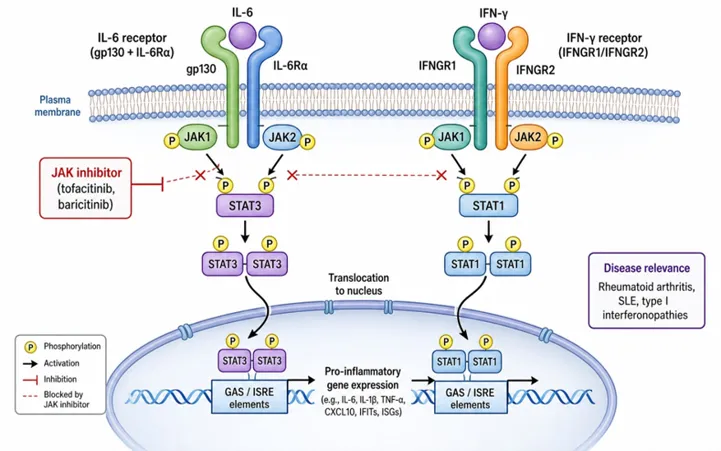
Figure 6. JAK–STAT cytokine receptor signalling in autoimmunity. IL-6 binding to gp130/IL-6Rα and IFN-γ binding to IFNGR1/IFNGR2 trigger JAK1/JAK2/TYK2 phosphorylation of STAT3 and STAT1. Phospho-STAT dimers translocate to the nucleus and bind GAS/ISRE elements, driving pro-inflammatory gene programmes (RA, SLE, type I interferonopathies). JAK inhibitors (tofacitinib, baricitinib) block kinase activity and downstream transcription.
6.1 Autoimmune Disorders
Autoimmune diseases—encompassing rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), multiple sclerosis (MS), inflammatory bowel disease (IBD), and type 1 diabetes—collectively affect 8–10% of the global population and account for a disproportionate burden of chronic morbidity [52,53]. Their clinical management is complicated by phenotypic heterogeneity within diagnostic categories: patients classified under the same diagnosis frequently harbour distinct pathogenic immune mechanisms, requiring different biological therapies. AI is transforming autoimmune medicine by enabling deep immunophenotyping, therapy matching, and disease activity prediction [3,22].
In RA, ML models integrating serology, cytokine profiles, synovial transcriptomics, and radiographic joint damage scores predict responses to TNF inhibitors, IL-6 pathway blockers, and JAK inhibitors with accuracy exceeding 80%, enabling precision biologic prescribing from treatment initiation rather than through sequential empirical trials [54]. GNN analysis of cytokine signalling networks in SLE has identified interferon-gamma and BAFF-driven patient endophenotypes associated with distinct organ manifestations—nephritis, serositis, haematological involvement—guiding targeted biological intervention [22,53].
In atopic dermatitis (AD), unsupervised clustering of multi-omic skin biopsy data has revealed Th2versus Th1/Th17-polarised disease subtypes with differential responses to dupilumab versus JAK inhibitors, laying a molecular foundation for precision AD management [54]. MS disease-course prediction using ML models trained on baseline MRI characteristics, CSF biomarkers, and genetic risk scores stratifies patients into aggressive versus benign courses, informing high-efficacy therapy initiation in high-risk individuals while sparing low-risk patients from unnecessary immunosuppression [55].
6.2 Vaccine Development
Vaccine development has historically relied on empirical antigen selection and adjuvant formulation, processes that are time-consuming and often inadequate for rapidly mutating pathogens. AI is accelerating vaccine design by predicting immunogen sequence properties, adjuvant formulation effects, population-level immunogenicity, and protective correlates of immunity [56,57]. Reverse vaccinology 2.0—combining AI-driven structural analysis of pathogen surface proteins with deep learning predictions of B cell epitope accessibility and MHC class II antigen presentation—enables rational identification of protective immunogens from genomic sequence data alone [56].
The SARS-CoV-2 pandemic demonstrated AI's capacity to accelerate vaccine development at unprecedented speed: mRNA vaccine antigen optimisation, codon usage algorithms, and mRNA stability predictors—each incorporating ML components—contributed to BNT162b2 and mRNA-1273 design and manufacturing scale-up [57,59]. Evolutionary ML models trained on influenza haemagglutinin and neuraminidase sequences accurately predict antigenically dominant strains six months in advance of the circadian season, informing World Health Organization (WHO) strain selection for annual influenza vaccines and guiding mRNA vaccine formulation for rapid update [58].
Adjuvant systems biology—using ML to predict immune responses to novel adjuvant-antigen combinations from in vitro cytokine and gene expression data—is shortening the empirical adjuvant development cycle from years to months [56]. Systems vaccinology approaches, integrating pre-vaccination immune baseline characteristics with post-vaccination gene expression kinetics, predict antibody titres, T cell response magnitudes, and clinical protection rates, enabling adaptive vaccine trial designs [57].
6.3 Infectious Disease Management
COVID-19 catalysed unprecedented application of AI to infectious disease immunology, from diagnostic imaging to cytokine storm prediction and vaccine candidate selection [28,59,65]. Deep learning analysis of chest CT imaging achieved radiologist-level sensitivity and specificity for COVID-19 pneumonia, while ML models trained on early clinical and immunological parameters—lymphocyte counts, ferritin, IL-6, D-dimer—predicted progression to severe disease and ICU admission, enabling risk-stratified clinical management [28,60].
HIV immunology has benefited from AI-driven analysis of broadly neutralising antibody (bnAb) development, TCR repertoire correlates of viral control, and reservoir reactivation dynamics. ML models integrating CD4 count trajectories, viral sequence evolution, and T cell exhaustion markers guide individualised antiretroviral treatment decisions and inform HIV cure strategies targeting the latent reservoir [60]. Sepsis immunology represents another major application domain: ML classifiers trained on cytokine profiles, metabolomics, and transcriptomics stratify sepsis patients into immune-inflammatory endophenotypes—SRS1 (immunosuppressed) versus SRS2 (hyperinflammatory)—with significant implications for adjuvant immunotherapy selection [35]. A randomised controlled trial pilot demonstrated that endophenotype-guided therapy in sepsis improved 28-day mortality by 8.7 percentage points versus standard care, establishing proof-of-concept for AI-guided precision sepsis management [35].
7. CHALLENGES AND LIMITATIONS
7.1 Data Quality and Availability
The performance of AI models in immunology is fundamentally constrained by the quantity, quality, and representativeness of training data [32,33]. Immunological datasets—particularly from rare diseases, paediatric populations, and underrepresented ethnic groups—are frequently small, imbalanced, and heterogeneously collected, leading to models that perform well on benchmark datasets but fail to generalise to real-world clinical populations [61,62]. Batch effects from different sequencing platforms, processing protocols, and laboratory conditions introduce technical artefacts that confound biological signals, requiring careful data harmonisation and domain adaptation [11,32].
The lack of standardised data collection protocols across clinical and research centres—including variable cell isolation methods, RNA extraction protocols, and antigen-stimulation conditions—further limits the portability of trained models. Federated learning architectures, which train AI models across distributed data silos without pooling raw data, offer a promising solution to the data availability problem, enabling multi-centre studies while preserving patient privacy and institutional data sovereignty [64,66]. The implementation of FAIR (Findable, Accessible, Interoperable, Reusable) data principles in immunological repositories is essential to maximise the training data available for AI model development [32].
7.2 Model Interpretability
Deep learning models achieving state-of-the-art predictive performance in immunology are frequently characterised as 'black boxes'—their internal representations are opaque to biological interpretation, limiting scientific insight and clinical trust [33,63]. The clinical deployment of AI-based immunotherapy selection tools requires not only predictive accuracy but also mechanistic transparency: clinicians must understand why a model recommends a particular therapy to incorporate its output appropriately into clinical reasoning [62,63].
Explainability methods—SHapley Additive exPlanations (SHAP), integrated gradients, attention visualisation, and layer-wise relevance propagation—provide post-hoc attribution of model predictions to input features, enabling immunological interpretation of AI decisions [33]. However, these methods have known limitations: SHAP values can be unstable across runs,
attention weights do not directly measure causal importance, and locally interpretable surrogate models may not faithfully reflect global model behaviour [63]. A growing consensus in the field advocates for the development of inherently interpretable models—attention-based architectures, sparse autoencoders, concept bottleneck models—that embed biological priors and produce predictions directly traceable to immunologically meaningful features [63].
7.3 Ethical Concerns
AI systems trained on historically collected biomedical data encode and can amplify pre- existing healthcare inequities [61,62]. A seminal analysis demonstrated that a widely deployed clinical AI algorithm used to manage patient health populations exhibited substantial racial bias, systematically underestimating disease severity in Black patients relative to white patients with equivalent objective health needs [61]. In immunology, biased training datasets—over- representing patients of European ancestry in GWAS and immune reference atlases—may yield AI models with reduced accuracy for disease prediction and therapy selection in non-European populations, potentially exacerbating health disparities in autoimmune disease management and cancer immunotherapy [62].
Patient privacy constitutes a further ethical dimension: high-dimensional genomic and immune profiling data are inherently re-identifiable, raising concerns about consent, data sharing, and potential genetic discrimination [64]. The algorithmic transparency required for clinical AI governance creates tension with intellectual property protections in commercial AI development, complicating independent validation and regulatory review [63]. Algorithmic decision support tools in oncological immunotherapy may subtly shift clinical accountability—if a model recommends withholding treatment and the patient deteriorates, questions of liability and informed consent require new ethical and legal frameworks [62].
7.4 Regulatory Issues
Regulatory harmonisation of AI-based clinical decision support tools remains incomplete and heterogeneous across jurisdictions [63,64]. The US Food and Drug Administration (FDA) has issued guidance on AI/ML-based software as a medical device (SaMD), establishing a total product life cycle approach that accommodates model updates, but specific frameworks for AI- guided immunotherapy selection are nascent [64]. The European Union's AI Act and Medical Device Regulation (MDR) impose risk-based classification requirements that may significantly increase development timelines and costs for high-risk immunological AI applications, including treatment recommendation systems and automated diagnostic algorithms [63].
Continuous learning AI systems—models that update based on real-world clinical feedback—present particular regulatory challenges, as performance characteristics at deployment may diverge from those validated at the time of regulatory approval [64]. The 'locked' versus 'adaptive' model distinction in regulatory frameworks does not fully address the dynamic nature of immunological AI tools intended to evolve with clinical evidence. International harmonisation bodies, including the International Medical Device Regulators Forum (IMDRF), are developing convergent standards for AI/ML-based SaMD that will need to encompass immunotherapy decision support explicitly [62,64].
8. FUTURE PERSPECTIVES
8.1 Generative AI
Generative AI—models capable of producing novel biological sequences, structures, and hypotheses rather than merely classifying existing data—represents a transformative emerging paradigm for precision immunology [67,69]. Protein language models such as ESM-2 and ProtGPT2, trained on hundreds of millions of protein sequences, enable de novo design of antibodies, cytokines, and immunomodulatory peptides with specified binding affinity, stability, and safety profiles, dramatically accelerating the biologic drug discovery pipeline [68]. Generative adversarial networks (GANs) and diffusion models applied to immune cell imaging data are enabling in silico augmentation of scarce training datasets, mitigating the data scarcity problem that constrains supervised classifier performance [67].
For neoantigen vaccine design, generative models capable of sampling immunogenic peptide sequences conditioned on patient HLA haplotypes and tumour mutational profiles are being explored as tools for iterative vaccine antigen optimisation [50,69]. Crucially, generative AI enables multi-objective optimisation—simultaneously maximising immunogenicity, minimising cross-reactivity with self-antigens, and ensuring manufacturing feasibility—a problem intractable by traditional sequential assay-guided approaches [68]. Responsible development of generative immunological AI will require robust evaluation frameworks assessing both in silico predictions and biological validation, as well as safeguards against generating sequences with potential for misuse in biological threat contexts [63,69].
Genomics & Epigenomics scRNA-seq Profiles Plasma Proteomics Wearable Biosensors Clinical EHR & Imaging Microbiome Data, Neoantigen Vaccine Personalisation Checkpoint Inhibitor Dose Optimisation CAR-T Protocol Simulation Autoimmune Flare Pre-emption Real-Time Adaptive Therapy Adjustment Toxicity Risk Alerts
DIGITAL IMMUNE TWIN (Components: Generative AI Design, Bayesian Uncertainty, Graph NN Core, Mechanistic Model, NLP Literature, Federated Learning)
8.2 Digital Twins in Immunology
The concept of the digital twin—a dynamic, computationally executable model of an individual biological system continuously updated with real-world data—is beginning to be applied in personalised immunology [67]. An immunological digital twin would integrate a patient's genomic, transcriptomic, epigenomic, and clinical data streams into a mechanistic-statistical hybrid model capable of simulating immune responses to proposed interventions, predicting treatment trajectories, and identifying optimal therapeutic strategies through in silico experimentation [67]. Early proof-of-concept digital twin models have been developed for type 1 diabetes—simulating glucose-insulin-immune dynamics to personalise artificial pancreas algorithms—and for CAR-T cell therapy optimisation—simulating T cell expansion kinetics to identify optimal manufacturing conditions [47,67].
The integration of wearable biosensor data—continuous heart rate, temperature, and novel immune cell monitoring technologies under development—with digital immune twin models could enable real-time adaptive immunotherapy management, adjusting dosing and combination strategies in response to detected immune deviations [67]. Significant technical challenges remain: digital twins require high-fidelity mechanistic models of immune dynamics that are computationally tractable, regularly updated with patient data, and validated against prospective clinical outcomes. Uncertainty quantification—providing reliable confidence intervals around digital twin predictions—is essential for clinical adoption and will require novel Bayesian deep learning approaches [63,67].
8.3 Real-World Clinical Implementation
The transition of AI precision immunology tools from research prototypes to routine clinical practice requires sustained attention to implementation science, health system infrastructure, and clinician education [62,64]. Prospective multi-centre clinical trials evaluating AI-guided versus standard immunotherapy selection are essential to generate the randomised evidence required for guideline inclusion and reimbursement, moving beyond retrospective validation studies that are susceptible to selection bias [42,64]. Health economic analyses demonstrating cost-effectiveness of AI-guided precision immunotherapy—accounting for both direct cost savings from avoided ineffective treatments and quality-adjusted life year gains from improved outcomes—will be required to justify healthcare system investment [70].
Clinical workflow integration presents practical challenges: AI tools must interface with existing electronic health record systems, deliver outputs in clinician-interpretable formats with appropriate uncertainty communication, and be accessible at the point of clinical decision-making without requiring specialist bioinformatics interpretation [62]. Multidisciplinary tumour boards and precision medicine clinical services, already established in many cancer centres, provide natural integration points for AI-guided immunotherapy recommendations, provided that clinicians receive adequate training in AI tool evaluation and limitations [64].
Looking forward, the convergence of precision immunology with drug discovery AI—generative molecular design, physics-based protein-ligand docking, in silico clinical trials—will progressively shorten the cycle from immune target discovery to first-in-human therapy, potentially transforming the economics and timelines of immunology drug development [68,70]. Equity-centred AI development—prioritising diverse training datasets, community-participatory trial design, and global access frameworks—will be essential to ensure that the precision immunology revolution benefits all patients equitably, not only those in well-resourced healthcare systems [61,62].
9. CONCLUSION
Artificial intelligence is fundamentally reshaping precision immunology across its entire analytical and therapeutic spectrum. From the computational dissection of single-cell immune atlases and deep learning-based immune receptor repertoire analysis, to multi-omics biomarker discovery, AI-guided checkpoint inhibitor patient selection, and generative design of personalised neoantigen vaccines, AI methods are demonstrably extending the biological insight and clinical utility achievable from modern immunological data. The convergence of transformer architectures, graph neural networks, federated learning, and multi-omics integration has equipped immunologists and clinicians with analytical tools commensurate with the complexity of the immune system and the therapeutic challenges of immune-mediated disease [1,5,8].
Key research gaps that remain to be addressed include: (i) the development of sufficiently large, diverse, and harmonised training datasets representative of the global patient population; (ii) the creation of regulatory-grade interpretable AI frameworks that provide mechanistic transparency alongside predictive accuracy; (iii) the conduct of prospective randomised clinical trials to establish the clinical efficacy and cost-effectiveness of AI-guided immunotherapy selection; (iv) the implementation of federated learning architectures enabling privacy-preserving multi-centre immune data science at scale; and (v) the ethical and governance frameworks ensuring equitable access to AI-driven precision immunotherapy [33,61,62,64].
Future opportunities are compelling: immunological digital twins simulating individual immune dynamics, generative AI designing novel immunomodulatory biologics, and real-time adaptive immunotherapy management guided by continuous biosensor data represent an emerging precision immunology paradigm that will require interdisciplinary collaboration between immunologists, computational scientists, clinicians, ethicists, and patients. Realising this vision responsibly—with rigorous validation, transparent communication, and an unwavering commitment to patient equity and safety—will define the success of AI in precision immunology in the decade ahead [67,68,70].
REFERENCES


Kingsuk Ray, Pratiksha Jadhao, Priyanka Khaidem, Gulsana Aribam, Artificial Intelligence in Precision Immunology: Emerging Applications in Immune Profiling, Predictive Biomarkers, and Personalized Cancer Immunotherapy, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6024-6047. https://doi.org/10.5281/zenodo.20822773
 10.5281/zenodo.20822773
10.5281/zenodo.20822773