
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy Practice, College of Pharmacy, Sri Ramakrishna Institute of Paramedical Sciences, Sri Ramakrishna Hospital Campus, Sarojini Naidu Road, Coimbatore, India 641044
Geriatrics represents the most vulnerable section of our society and largest consumers of prescribed drugs. Total world population consists 21% of geriatric population. The high-rate chronic problems of elderly patients’ attributes to various drug related problems (DRP). The prevalence of potentially inappropriate medication use is high among geriatrics, affecting up to 40% of patients. The main objectives of the study are to assess the prescription pattern and appropriate drug use using Beers Criteria 2022. A prospective observational study was conducted in General Medicine department of Sri Ramakrishna Hospital, Coimbatore where eligible patients were enrolled. The patient data was collected and analyzed statistically. It was observed that 83% of drugs belonged to group 1 of Beers Criteria (Potentially inappropriate drug use in older adults), 16% of drugs belonged to group 2 (inappropriate medication use in older adults sue to drug disease or syndrome) and 1% of drugs belonged to group 3 (potentially inappropriate medications to be used with caution in older adults). The use of inappropriate medications can be avoided using Beers Criteria 2022, which is one of the essential clinical tools. Hence pharmacists need to play an important role in reducing inappropriate medication use and suggest safer alternatives.
Geriatrics represent the most vulnerable section of our society and are generally the biggest consumers of prescribed drugs. Treating the elderly is the most challenging part to the physicians and it can be sorted only through a holistic multidisciplinary approach. It is predicted that the population of geriatrics in our country will rise from 8.3% - 10.7% by 2023. Geriatrics constitutes of 21% of the world population and in India it was 57 millions. Due to advances in medical technology and major social, financial and health planning implications, it has been estimated that by the year 2050, the number of elderly people would increase to about 324 million, that is 33% of the world population. India has emerged as “an aging nation” because 7.7% of its populations are more than 60 years old in that 75% of elderly persons were living in rural areas.
Life expectancy has soared by leaps and bounds in the last 100 years. In 2015, the global elderly population increased by 55 million.[1] On an average, the individuals who are 65– 69 years old take nearly 14 different prescription medications per year, and individuals who are aged 80–84 years take an average of 18 prescriptions per year.[2] Age-related physiologic changes that occur in elderly individuals may affect drug pharmacokinetics and pharmacodynamics, thus increasing the risk of medication-related problems.[3] The other reasons for drug-related problems are lack of continuity in physician contacts, lack of a consistent drug list, and inadequate prescription and monitoring of drug therapy.[4] moreover, with ageing, a high prevalence of multiple chronic diseases and comorbidity takes place, followed by the use of complicated treatment regimens and polypharmacy.[5]
Polypharmacy may be a source of concerns for the elderly because it increases the risk of elderly syndromes and a decreased functional status as well s cost in health care. Polypharmacy is the concomitant administration and use of four or more medications and it is usually common among older adults.[6] Underuse has an important relationship with older adults; it seems to have a negative effect on health outcomes for older people,[7] which include functional disability, health services use, and death. Also medication nonadherence can have drastic deleterious health effects on the elderly.[8] These factors and treated the elderly patients with higher attention.
Population Census 2011 of India reported around 104 million elderly persons in India comprises 7.4% of total population and estimated to rise by the year 2026 to 12.4%. It is seen in India, that the growth rate of the elderly population has been more than the growth in general population[9]. Due to the increase of pandemonium happened recently, world focus shifted to the poor health status and vulnerability of the elderly aged advanced group patients to disease acquisition. Inappropriate prescribing is a very common practice in older adults and has become a international healthcare concern because of its association with less desirable health outcomes that include adverse drug events (ADEs), longer hospital stay and inappropriate healthcare resource utilization [10]. Ensuring safe and effective drug therapy can be challenged by various factors such as acute and chronic disorders, reduced physiological reserves, age related alteration of pharmacokinetic and pharmacodynamic properties of a drug, cognitive changes with reduced medication adherence and organization etc can challenge the effective drug therapy .The use of five or more drugs concurrently , defined as polypharmacy and is becoming an important public health problem .Very often , it is blamed for the increase in morbidity and mortality .‘The inappropriate prescription in older patients occurs when the risk of adverse effects exceeds the clinical benefits, especially when there are more effective alternatives available’ [11] .
Commonly observed preventable drug related Problems (DRPs) include:
LITERATURE REVIEW
OBJECTIVES
MATERIALS AND METHODS
STUDY DESIGN
A well-designed patient data entry form was developed and used for this study. The following information like patient demographic details (Name, age, gender, reason for admission, duration of illness and social history were included. The patients were monitored for restricted drug-drug interactions, administration information provided regarding each medications prescribed.
METHODS
Study site:
In General medicine department of Sri Ramakrishna Hospital Coimbatore, which is a 1000 bedded multi-speciality, tertiary care private corporate teaching hospital.
Study Design: Prospective observational study.
Study duration: 6 Months
Samplesize:103 in-patients.
Statistical Analysis:
The data collected will be analyzed statistically using descriptive statistics wherever necessary, the results will be depicted in the form of graphs and percentages.
INCLUSION CRITERIA:
EXCLUSION CRITERIA
METHOD:
The prospective observational study will be conducted in General medicine, department of Sri Ramakrishna Hospital, Coimbatore. Based on the inclusion and exclusion criteria, the eligible patients were enrolled by taking/obtaining their consent. The well-designed/structured data collection forms were prepared and used. This form mainly contains demographic details, educational qualifications, social habits, current medication, past medical and medication history, laboratory data, and other relevant information. The other relevant data were collected from patient's progress records, treatment chart, laboratory reports, and by a direct patient interview.
The current medication data details include the names of all drugs, their dosage, route of administration with frequency, indication, and the date of drugs started and stopped. The past medication and medical history data consisting of patients previous allergies, co-morbidities, and the drug received previously. The laboratory data includes the various relevant laboratory investigations performed.
The drug therapy of enrolled study participants were routinely monitored and interviewed when necessary and discussed with the physician about identified MRP during ward rounds and at outpatient clinic. While collecting the data of the patients, patient or their care takers were interviewed with the help of nursing staff to get the complete details. The data collected were subjected/assessed for various DRP (inappropriate use of medication, polypharmacy, noncompliance, ADRs, drug–drug interaction, etc,) by using primary (standard literature), secondary (Micromedex), and tertiary resources (e.g.: BNF, AHFS, and Martindile) which is available in the clinical pharmacy department. Whenever the clinical pharmacist's service was required by the patients/ health care professionals, the service was provided for better therapeutic outcomes (e.g., patient counselling, drug interaction, and drug information). The assessed information was documented and subjected for a suitable statistical method.
EXPECTED OUTCOMES:
RESULTS AND DISCUSSIONS
The study entitled “Assessment of prescription pattern and appropriate drug use among geriatric population” was carried out in the General Medicine Department of a multi-speciality hospital. A total number of 103 patients who has satisfied the inclusion criteria were enrolled in the study after obtaining their consent.
GENDER DISTRIBUTION:
A total of 103 patients were included in the study, among them 67(65%) were male and 36(35%) were female. The percentage of men were more when compared to female (TABLE-1). The result on gender categorisation has revealed that the study population comprises of more number of male patients . Our study results correlate with the study conducted by Kumaraswamy M. et al, (2023) which reported that male patients were more in their study population.(13)
TABLE 1: GENDER CATEGORIZATION (n=103)
|
SR. NO |
GENDER |
NO OF PATIENTS |
PERCENTAGE |
|
1 |
Male |
67 |
65% |
|
2 |
Female |
36 |
35% |
AGE DISTRIBUTION:
A total of 103 prescriptions were screened randomly. Age distribution of the patients was analysed and it was found that 50(48.5%) of the prescriptions were in the age group of 65-69 years, 34{33.2%) in the age group of 70-74 years, 8(7.7%) in the age group of 75-79 years, 6 (5.8%) in the age group of 80-84 years, 2 (1.9%) in the age group of 85-89 years, 3 (2.9%) in the age group of 90-94 years. The study shows that the maximum number of patients in the study group were in the age group of 65-69 years (TABLE -2). Our study results correlate with the study conducted by Rims B. et al, (2011) which reported that maximum number of patients in their study were in the age group of (65-69)yrs.(14)
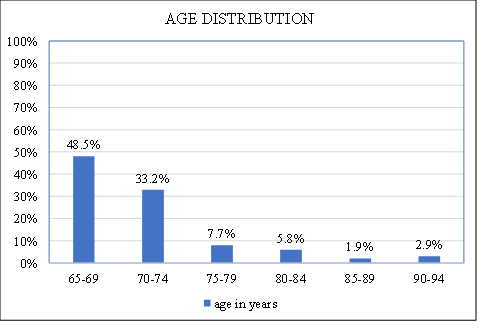
FIGURE 2: AGE DISTRIBUTION
LENGTH OF STAY:
The length of stay of the patients in the study site were also analysed and found that 62 (62.1%) of the patients were hospitalized in the for the period between 1-5 days, 40 (38.8%) had 6-10 days and 1(0.9%) had 11-15 days as a length of stay. The majority of the study population were hospitalised for a period of 1-5 days (TABLE-3). Our study results correlate with the study conducted by Harikrishna V. et al, (2023) it showed that most of the patients were hospitalised for 1-5 days in their study population. (15)
TABLE 3: LENGTH OF STAY
|
No of Days |
No of Patients |
Percentage |
|
1 to 5 |
62 |
60.19% |
|
6 to 10 |
40 |
38.8% |
|
11 to 15 |
1 |
0.9% |
MAJOR DIAGNOSIS OBSERVED IN THE STUDY POPULATION:
Major diagnosis observed in the study population were Diabetes mellitus (18.8%), followed by Systemic Hypertension (16.1), CVA (11.2%), Ischemic Heart Disease (11.2%), ACS (6.2%).
The results revealed that diabetes and hypertension is more prevalent in the study population Our study results correlate with the study conducted by Muhammed S. et al, (2015) reported that DM & Cardio vascular disorders(16 ) were noy prevalent in there study group (TABLE-4).
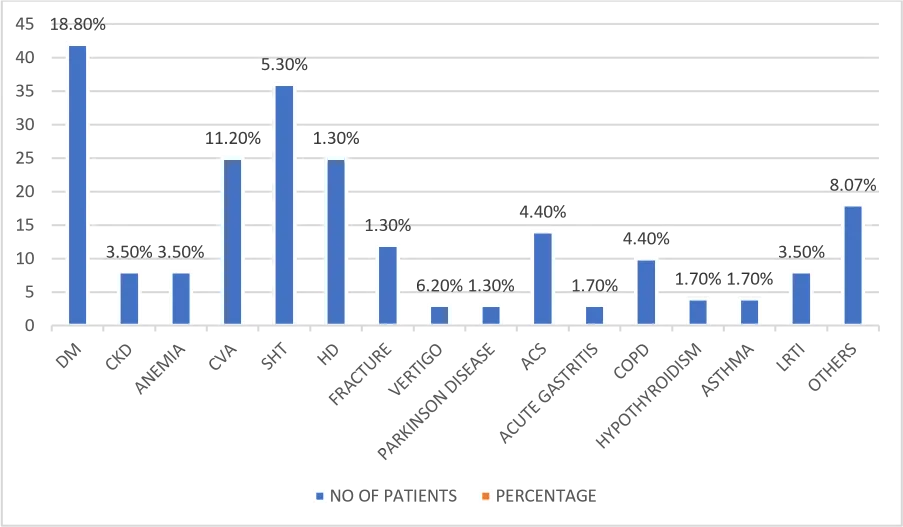
FIGURE 4: MAJOR DIAGNOSIS OBSERVED IN THE STUDY POPULATION
CATEGORIES OF DRUGS PRESCRIBED:
The commonly prescribed to the study population were Antibiotics, Antiulcers and Antiemetics, Analgesics, Antihypertensives, Antidiabetics, Steroids, Probiotics, Multivitamins, Lipid lowering drugs, Antiasthmatics, Anticoagulants, Antiplatelets, Antiepileptics, Sedatives, Antivertigo, Antiseptics, Antianginal, Nootropics and Others (TABLE 5).
The major categories of drugs in the prescriptions were Antiulcers and antiemetics (15.2%), Antibiotics (11.5%), Anti diabetics (9.02%), Multivitamins (8.2%).
TABLE 5: CATEGORIES OF DRUGS PRESCRIBED TO PATIENTS
|
Sr. No |
Categories of Drugs Prescribed |
No. of Drugs |
Percentage |
|
1. |
Antibiotics |
106 |
11.5% |
|
2. |
Anti-ulcer and anti-emetics |
140 |
15.2% |
|
3. |
Analgesics |
58 |
6.3% |
|
4. |
Antihypertensives |
54 |
5.8% |
|
5. |
Anti-diabetic |
83 |
9.02% |
|
6. |
Steroids |
19 |
2.06% |
|
7. |
Pro-biotics |
7 |
0.76% |
|
8. |
Multivitamins |
76 |
8.2% |
|
9. |
Lipid-lowering agents |
48 |
5.2% |
|
10. |
Anti-asthmatics |
55 |
5.9% |
|
11. |
Anticoagulants |
28 |
3.04% |
|
12. |
Antiplatelets |
67 |
7.2% |
|
13. |
Antiepileptics |
20 |
2.17% |
|
14. |
Sedatives |
19 |
2.06% |
|
15. |
Anti-vertigo |
12 |
1.3% |
|
16. |
Antiseptics |
13 |
1.4% |
|
17. |
Antianginal |
20 |
2.17% |
|
18. |
Nutropics |
35 |
3.8% |
|
19. |
Others |
60 |
6.5% |
NUMBER OF MEDICATIONS PER PRESCRIPTION:
The number of drugs prescribed in each prescription was evaluated and it was found that 5(4.8%) of the prescription had 1-5 drugs, 48(46.6%) had 6-10 drugs, 43(41.7%) had 1115 drugs, 8 (7.7%) had 16-20 drugs. (TABLE -6). The results revealed that, polypharmacy is more prevalent among the study population. Polypharmacy can be associated with poor medication adherence especially among elderly patients. Polypharmacy can also lead to increase risk of drug related problems such as, drug interactions, adverse drug reaction, IV compatibility and prolonged hospitalization. The study performed by Rushab J. et al ., (2020) reported that majority of their study prescriptions exhibit polypharmacy.(17)
TABLE 6: NUMBER OF MEDICATIONS PER PRESCRIPTION
|
Sr. No |
No. of Medications |
No. of Patients |
Percentage |
|
1 |
1 to 5 |
5 |
4.8% |
|
2 |
6 to 10 |
48 |
46.6% |
|
3 |
11 to 15 |
43 |
41.7% |
|
4 |
16 to 20 |
8 |
7.7% |
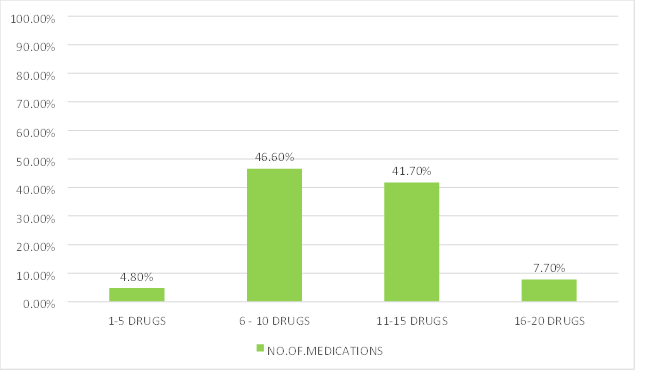
FIGURE 6: NUMBER OF MEDICATION PER PRESCRIPTION
Evaluation of prescription using Beers Criteria:
The prescriptions were thoroughly screened using Beers Criteria 2022 and the result indicate that 46.6% of prescriptions were inappropriate (TABLE-7). The study performed by Daphne Lee, Nataly martini, simon Moyes, Karen Hayman, Monica zolezzi and Ngaire Kerse, et al., (2013) showed that the majority of prescription were appropriate in their study population.
TABLE 7: EVALUATION OF PRESCRIPTION USING BEERS
|
Category of prescription screened |
Nos of Prescription |
Percentage (%) |
|
Appropriate prescription |
55 |
53.40% |
|
Inappropriate prescription |
48 |
46.60% |
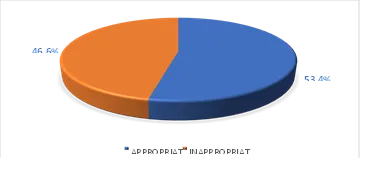
FIGURE 7: EVALUATION OF PRESCRIPTION USING BEERS
Inappropriate medications according to beers criteria
The drugs were prescribed inappropriately according to Beers Criteria were Alprazolam, Chlorthalidone, Clonazepam, Dapagliflozin, Gliclazide, Glimepiride, Oxcarbazepine, prazosin, Promethazine, Ticagrelor, Ketorolac, Hydrochlorothiazide, Dimnhydrinate, Atropine, Tramadol, Torsemide, Clonidine, Lorazepam, Chlorpheniramine, Nifedipine, diclofenac, Furosemide which are to be avoided in the elderly patients (TABLE -8)
|
S. No. |
Drugs under Beers Criteria |
Frequency of Occurrence (%) |
Reason for Inappropriateness in Geriatric Patients |
|
1 |
Alprazolam |
4 (7.0%) |
Avoid BZD, because it increases the risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents in elderly. |
|
2 |
Chlorthalidone |
2 (3.5%) |
Use with caution, it may exacerbate or cause SIADH or hyponatremia; monitor sodium level closely when starting or changing dosages in older adults. |
|
3 |
Clonazepam |
9 (15.7%) |
Avoid BZD, because it increases the risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents in elderly. |
|
4 |
Dapagliflozin |
2 (3.5%) |
Use with caution as it may be at increased risk of urogenital infections, particularly in women during the first month of treatment, and ketoacidosis in older adults. |
|
5 |
Gliclazide |
3 (5.2%) |
Avoid sulfonylureas as it has a higher risk of cardiovascular events and hypoglycemia. |
|
6 |
Glimepiride |
7 (12.2%) |
Avoid sulfonylureas as it has a higher risk of cardiovascular events and hypoglycemia. |
|
7 |
Oxcarbazepine |
1 (1.7%) |
Use with caution, it may exacerbate or cause SIADH or hyponatremia; monitor sodium level closely when starting or changing dosages in older adults. |
|
8 |
Prazosin |
2 (3.5%) |
Avoid prazosin as it increases the risk of orthostatic hypotension or bradycardia. |
|
9 |
Promethazine |
2 (3.5%) |
Avoid use as it is highly anticholinergic and its clearance is decreased with age. |
|
10 |
Ticagrelor |
1 (1.7%) |
Use with caution, particularly in adults 75 years and older, as it increases the risk of bleeding. |
|
11 |
Ketorolac |
2 (3.5%) |
Avoid ketorolac because it increases the risk of GI bleeding or PUD in older adults. |
|
12 |
Hydrochlorothiazide |
1 (1.7%) |
Use with caution, it may exacerbate or cause SIADH or hyponatremia; monitor sodium level closely when starting or changing dosages in older adults. |
|
13 |
Dimenhydrinate |
1 (1.7%) |
Avoid use as it is highly anticholinergic and its clearance is decreased with age. |
|
14 |
Atropine |
1 (1.7%) |
Avoid use as it is highly anticholinergic and its clearance is decreased with age. |
|
15 |
Tramadol |
2 (3.5%) |
Use with caution, it may exacerbate or cause SIADH or hyponatremia; monitor sodium level closely when starting or changing dosages in older adults. |
|
16 |
Torsemide |
5 (8.7%) |
Use with caution, it may exacerbate or cause SIADH or hyponatremia; monitor sodium level closely when starting or changing dosages in older adults. |
|
17 |
Clonidine |
1 (1.7%) |
Avoid as first-line antihypertensive; high risk of adverse CNS effects, may cause acute bradycardia and orthostatic hypotension. |
|
18 |
Lorazepam |
1 (1.7%) |
Avoid BZD, because it increases the risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents in elderly. |
|
19 |
Chlorpheniramine |
1 (1.7%) |
Avoid use as it is highly anticholinergic and its clearance is decreased with age. |
|
20 |
Furosemide |
7 (12.2%) |
Use with caution, it may exacerbate or cause SIADH or hyponatremia; monitor sodium level closely when starting or changing dosages in older adults. |
|
21 |
Nifedipine |
1 (1.7%) |
Avoid because of hypotension and risk of precipitating myocardial ischemia. |
|
22 |
Diclofenac |
1 (1.7%) |
Avoid because it increases the risk of GI bleeding or PUD in older adults. |
Categorization of drugs according to Beers Criteria:
The inappropriate drugs identified are categorized under Group I, Group II, Group III.
GROUP I--Drugs which are considered to be potentially inappropriate in older adults
GROUP II -Drugs which may exacerbate existing disease or syndrome
GROUP III-Drugs to be sold with caution in older adults.
|
Group 1 |
Group 3 |
|
Alprazolam Clonazepam Gliclazide Glimepiride Ketorolac Prazosin Promethazine Atropine Dimenhydrinate Clonidine Chlorpheniramine Nifedipine Lorazepam Diclofenac |
Chlorthalidone Dapagliflozin Oxcarbazepine Ticagrelor Tramadol Hydrochlorothiazide Torsemide Furosemide
|
45(65.60%) of drugs belongs to group 1 of Beers Criteria (Potentially inappropriate medication use in older adults), 8(34.40%) of drugs belongs to group 3 (Potentially inappropriate drugs to be used with caution in older adults).
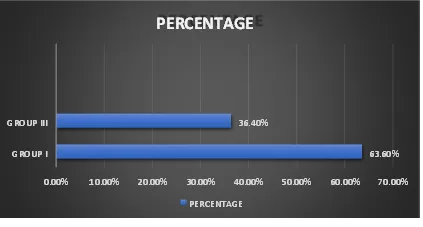
FIGURE 8: CATEGORISATION OF DRUGS ACCORDING TO BEERS CRITERIA
SAFER ALTERNATIVES IN GERIATRICS
|
Drugs |
Indication |
Concern |
Alternative |
|
Alprazolam, Clonazepam, Lorazepam |
Sleep |
Increased sensitivity to BZD, increased risk of cognitive impairment, delirium, unsteady gait, syncope, falls, accidents, and fractures |
Ramelteon: 8 mg half an hour before sleep at night. Low-dose doxepin: 3–6 mg half an hour before sleep at night. |
|
Prazosin |
Systemic hypertension |
Orthostatic hypotension |
Lifestyle modifications. Start low and go slow. Thiazide diuretics, Angiotensin Converting Enzyme Inhibitors, Angiotensin Receptor Blockers, Calcium Channel Blockers |
|
Dapagliflozin |
Type 2 diabetes mellitus |
Increased risk of urogenital infections and ketoacidosis |
Monitor blood sugar level |
|
Ticagrelor |
Congestive heart failure |
Increases the risk of bleeding in adults 75 years old and older |
Clopidogrel 75 mg once daily |
|
Gliclazide, Glimepiride |
Type 2 diabetes mellitus |
Higher risk of cardiovascular events and hypoglycemia |
Dipeptidyl peptidase-4 inhibitors (e.g., Sitagliptin, Vildagliptin) |
|
Oxcarbazepine |
Partial seizure |
Syndrome of inappropriate antidiuretic hormone (SIADH)/hyponatremia |
Monitor serum sodium levels |
|
Chlorthalidone, Hydrochlorothiazide, Torsemide, Furosemide |
Hypertension |
Syndrome of inappropriate antidiuretic hormone (SIADH)/hyponatremia |
Monitor serum sodium levels |
|
Promethazine, Chlorpheniramine, Dimenhydrinate |
Allergic conditions |
Anticholinergic effects |
Second-generation antihistamines like cetirizine, fexofenadine, loratadine |
|
Ketorolac, Diclofenac |
Pain |
GI bleeding risk increased in elderly population |
Mild-to-moderate pain: Acetaminophen 500 mg–1 g every 4–6 hours. Celecoxib: Initially 400 mg, followed by 200 mg twice daily. Meloxicam: 7.5–15 mg as a single dose. Use gastroprotective agents like Proton Pump Inhibitors or Histamine Receptor Antagonists. |
|
Atropine |
Antispasmodic |
Highly anticholinergic |
Baclofen: 20 mg orally 3 times daily (Max dose: 80 mg/day). Tizanidine: 2 mg orally per day. |
|
Tramadol |
Pain |
Syndrome of inappropriate antidiuretic hormone (SIADH)/hyponatremia |
Monitor serum sodium levels |
|
Nifedipine |
SHT |
Avoid because of hypotension and risk of precipitating myocardial ischemia |
Nisoldipine: 17 mg orally once daily on an empty stomach, 1 hour before or 2 hours after meals. Maintenance dose: 17–34 mg once daily. |
|
Clonidine |
SHT |
Avoid as first-line antihypertensive. High risk of adverse CNS effects; may cause acute bradycardia and orthostatic hypotension |
Lifestyle modifications. Start low and go slow. Thiazide diuretics, Angiotensin Converting Enzyme Inhibitors, Angiotensin Receptor Blockers, Calcium Channel Blockers |
CONCLUSION
The current study could assess the prescribing pattern of the medicines in the geriatric population according to beers criteria 2022.The study report shows that the prevalence of PIMs are steadily increasing .The use of inappropriate medications can be avoided using the beers criteria 2022 ,which is one of the important clinical tool which can be wisely used by physicians ,pharmacist ,and health care providers. Beers criteria can be used as a guideline by the physicians while prescribing the drugs to the geriatric populations .
Before dispensing the medicine to the geriatric patient ,the pharmacist should play an important in assessing the appropriateness of the prescription so that .the quality and efficacy of medical care given to geriatrics can be increased . Pharmacist can also discuss with the physician about drugs and suggest a better and safer alternative to the geriatrics so that a proper decision is made regarding the right choice of drug Hence this study will help physicians in clinical decision making in geriatrics ,where better pharmaceutical care can be provided in the geriatric population .
REFERENCES


Shivashankar V, Akash P, Akshayamathi M, Alginpraise S, Amruth Vishnu R. Nair, Assessment of Prescription Pattern and Appropriate Drug use among Geriatric Population, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6568-6582. https://doi.org/10.5281/zenodo.20910934
 10.5281/zenodo.20910934
10.5281/zenodo.20910934