
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
HIMT College of Pharmacy, Greater Noida Uttar Pradesh.
Synovial inflammation, joint destruction, and a marked reduction in quality of life are the hallmarks of rheumatoid arthritis (RA), a chronic, progressive autoimmune inflammatory disease. The mainstay of RA treatment is still disease-modifying anti-rheumatic medications (DMARDs), which are designed to prevent structural damage, control disease activity, and maintain functional ability. The mechanisms of action, clinical efficacy, safety profiles, and pharmacoeconomic implications of conventional synthetic DMARDs (csDMARDs) and biologic DMARDs (bDMARDs) are all critically assessed in this comparative review. Because of their proven effectiveness, oral administration, and affordability, csDMARDs such as methotrexate, sulfasalazine, leflunomide, and hydroxychloroquine have long been utilized as first-line treatments. However, their long-term usefulness in certain patients is limited by drawbacks like delayed onset of action, inconsistent response, and organ-specific toxicities. On the other hand, bDMARDs specifically target important inflammatory mediators involved in the pathophysiology of RA, including B cells, T-cell co-stimulation pathways, interleukin-6, and tumor necrosis factor-?. With a quicker onset of action and more inhibition of radiographic disease progression, these agents show superior efficacy in patients who do not respond well to csDMARDs. Notwithstanding their clinical benefits, bDMARDs are linked to increased expenses, a higher risk of infection, immunogenicity issues, and difficulties with accessibility, especially in low- and middle-income environments. A treat-to-target approach is recommended by current international guidelines, which place csDMARDs as the first line of treatment and escalate to bDMARDs depending on response and disease severity. The landscape of RA treatment is changing due to new treatments like biosimilars and targeted synthetic DMARDs like JAK inhibitors
Persistent synovial inflammation, progressive joint destruction, and a variety of extra-articular symptoms are the hallmarks of rheumatoid arthritis (RA), a chronic, progressive, systemic autoimmune disease. In contrast to degenerative joint disorders, RA is caused by immune-mediated mechanisms that cause persistent inflammation of the synovial membrane. If treatment is not received, this can result in irreversible joint deformities, cartilage damage, and bone erosion. Rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPAs) are common serological markers associated with the disease, which usually manifests as symmetrical inflammatory polyarthritis that primarily affects the small joints of the hands and feet [1].
RA is one of the most common chronic inflammatory rheumatic diseases, affecting 0.5–1% of adults worldwide. With a female-to-male ratio of almost 3:1, the condition disproportionately affects women. It typically appears between the ages of 30 and 60, which is a crucial time for social and economic productivity. Patients, healthcare systems, and society at large are all continuously burdened by the chronic and lifelong nature of RA.
Significant physical disability, psychological distress, and systemic complications are just a few of the many aspects of RA's disease burden that go beyond joint pathology. Daily living activities and job performance are significantly hampered by persistent pain, morning stiffness, exhaustion, and progressive loss of joint function [2]. Uncontrolled inflammation eventually causes irreversible joint damage, deformities, and reduction in independence, all of which lower one's quality of life in terms of health. Furthermore, RA is becoming more widely acknowledged as a systemic illness with extra-articular symptoms that impact the neurological, musculoskeletal, pulmonary, and cardiovascular systems. Notably, chronic systemic inflammation is a major contributing factor to the markedly elevated risk of cardiovascular morbidity and early mortality in RA patients [3].
RA is a significant public health concern from a socioeconomic standpoint. High direct healthcare costs for long-term medication, frequent doctor visits, laboratory monitoring, imaging, and hospital stays are linked to the illness. Indirect costs, such as early retirement, decreased productivity, and absenteeism from work, frequently surpass direct medical costs, especially for patients with moderate to severe illness. The burden of disease and health disparities are made worse in low- and middle-income nations by delayed diagnosis, restricted access to advanced therapies, and insufficient access to specialized care [4].
The discovery and approval of disease-modifying anti-rheumatic medications (DMARDs) has changed the therapeutic landscape and improved long-term outcomes over the past 20 years due to substantial advances in our understanding of RA pathogenesis. It has been demonstrated that reducing disease activity, preventing structural damage, and improving functional outcomes can be achieved through early diagnosis, timely therapy initiation, and adoption of treat-to-target strategies. Despite these developments, a significant percentage of patients do not experience low disease activity or sustained remission, underscoring ongoing unmet clinical needs [5].
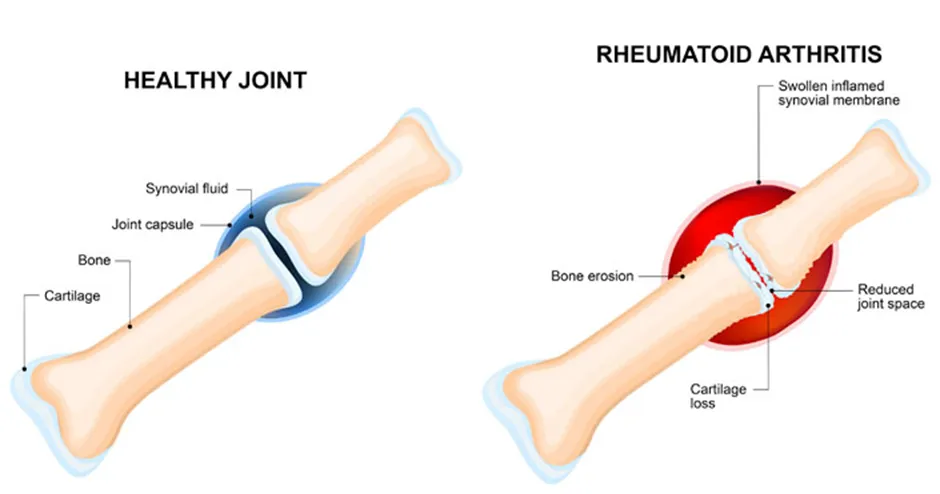
Fig 1: Comparison between Healthy Joint and Rheumatoid Arthritis [6]
A breakdown of immunological tolerance and persistent activation of both innate and adaptive immune responses cause rheumatoid arthritis (RA), a complicated inflammatory disease mediated by the immune system. Genetic predisposition, environmental triggers, immunological dysregulation, and chronic inflammation interact in a complex way during the pathogenesis of RA, which eventually results in synovial hyperplasia, cartilage degradation, and bone erosion. Finding important therapeutic targets that serve as the cornerstone of contemporary RA treatment has been made possible by an extensive knowledge of these pathogenic pathways [7].
Autoantibodies such rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPAs) are produced in RA due to a loss of immunological tolerance, sometimes years before the illness manifests clinically. When paired with environmental triggers like smoking and microbial exposure, genetic factors specifically, HLA-DRB1 "shared epitope" alleles promote aberrant antigen presentation and autoreactive T and B cell activation. Persistent inflammation is caused by these immune cells infiltrating the synovial tissue. By producing pro-inflammatory cytokines and encouraging macrophage and fibroblast activation, activated CD4⁺ T helper cells particularly Th1 and Th17 subsets play a crucial role. B cells play a crucial role in the continuation of illness because they not only produce autoantibodies but also present antigens and secrete cytokines [8].
Chronic synovitis, which is typified by synovial fibroblast proliferation and immune cell infiltration, comprising macrophages, lymphocytes, and dendritic cells, represents one of the defining characteristics of RA. The pannus, an invasive tissue created by this inflammatory synovium, actively erodes nearby bone and cartilage. Activated synovial fibroblasts have a tumor-like appearance and release matrix metalloproteinases (MMPs), which break down the extracellular matrix of cartilage [9].
A multifaceted network of cytokines dominates the inflammatory environment in RA. By enhancing inflammatory signaling, encouraging leukocyte recruitment, and triggering other pro-inflammatory mediators, tumor necrosis factor-α (TNF-α) plays a crucial role. Acute-phase reactions, systemic symptoms such anemia and exhaustion, and synovial inflammation are all influenced by interleukin-6 (IL-6). Additional cytokines that promote inflammation and tissue damage include granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-1, and IL-17. These cytokines trigger intracellular signaling pathways that control gene expression related to inflammation and immune cell survival, including nuclear factor-κB (NF-κB), mitogen-activated protein kinases (MAPKs), and Janus kinase–signal transducer and activator of transcription (JAK-STAT) [10].
Receptor activator of nuclear factor-κB ligand (RANKL), which is elevated by activated T cells and synovial fibroblasts, is the driving force behind increased osteoclastogenesis in RA. Bone degradation progresses when osteoclast activity is elevated and osteoblast function is compromised. Under inflammatory circumstances, synovial fibroblasts and chondrocytes produce proteolytic enzymes that cause cartilage destruction [11].
Numerous treatment targets have been identified because to the clarification of RA pathogenesis. Methotrexate and other csDMARDs often inhibit the synthesis of inflammatory mediators and immunological activation. TNF-α, IL-6 receptors, CD20-positive B cells, and T-cell co-stimulation pathways are among the important chemicals and cells that biologic DMARDs specifically target. More recently, intracellular signaling cascades essential for cytokine function have been directly disrupted by targeted synthetic DMARDs, especially JAK inhibitors [12].
Since they are the only category of medications that can change the disease's natural course, disease-modifying anti-rheumatic medicines (DMARDs) are the cornerstone of treatment for rheumatoid arthritis (RA). DMARDs target the underlying immunopathological mechanisms that cause chronic inflammation, joint destruction, and disease development, in contrast to corticosteroids and non-steroidal anti-inflammatory medications (NSAIDs), which relieve symptoms. Achieving clinical remission or prolonged low progression of the disease, preventing structural joint deterioration, maintaining physical function, and enhancing long-term quality of life are the main objectives of DMARD therapy [13].
DMARDs work by reducing cellular processes involved in synovial growth and tissue degradation, decreasing inflammatory pathways, and modifying immunological responses. It is currently repeatedly demonstrated that early DMARD medication beginning, ideally within the "window of opportunity" shortly after diagnosis, improves clinical results and lessens irreparable joint damage. As a result, the current worldwide treatment guidelines strongly advise starting DMARD as soon as RA is diagnosed [14].
DMARDs are generally divided into three categories based on their molecular targets, mode of action, and development process: conventional synthetic DMARDs (csDMARDs), biologic DMARDs (bDMARDs), and targeted synthetic DMARDs (tsDMARDs). This categorization shows how RA treatments have changed over time, moving from widely acting immunosuppressive drugs to much targeted, mechanism-driven treatments [15].
Methotrexate, sulfasalazine, leflunomide, and hydroxychloroquine are examples of conventional synthetic DMARDs that have been used for many years and are still the first-line treatment for the majority of patients [16]. These substances have a wide range of immunomodulatory and anti-inflammatory actions and are prized for their oral delivery, shown effectiveness, and affordability. However, organ-specific toxicity, inter-individual response heterogeneity, and delayed beginning of action may restrict their therapeutic usage.
Because they specifically target important cytokines or immune cells involved in the pathophysiology of the illness, biologic DMARDs provide a significant development in the treatment of RA. Tumor necrosis factor-α inhibitors, interleukin-6 signaling inhibitors, B-cell depletion treatments, and T-cell co-stimulation modulators are some of these medications. In individuals who do not respond well to csDMARDs, biologic DMARDs have proven to be more effective, especially when it comes to stopping radiographic progression. However, parenteral administration, greater risk of infection, and higher expenses are linked to their usage [17].
In more recent times, oral medications that specifically disrupt intracellular signaling pathways essential for cytokine-mediated inflammation have been made available by targeted synthetic DMARDs, especially Janus kinase (JAK) inhibitors. Although long-term safety is still being assessed, these medications combine the ease of oral administration with tailored immunomodulation [18].
The first-line pharmacological treatment for rheumatoid arthritis (RA) is conventional synthetic disease-modifying anti-rheumatic medications (csDMARDs), which continue to be the cornerstone of disease management in all worldwide treatment recommendations. These substances have widespread immunomodulatory and anti-inflammatory properties that diminish structural joint damage, delay the course of illness, and lower synovial inflammation. Because of their proven effectiveness, long-term clinical experience, oral administration, and affordability, csDMARDs continue to play a crucial role despite the rise of biologic and tailored synthetic DMARDs [19].
csDMARDs are frequently started as monotherapy or in combination regimens as soon as a diagnosis is made, and they are frequently continued even when more sophisticated treatments are offered. To maximize therapeutic results, their usage necessitates thorough evaluation of pharmacokinetic characteristics, dosage schemes, mechanisms of action, and safety monitoring [20].
Instead of specifically targeting a particular cytokine or immune cell type, conventional synthetic disease-modifying anti-rheumatic medicines (csDMARDs) achieve their therapeutic effects by modulating immunological and inflammatory pathways in a wide and complex manner. Because of their pleiotropic mechanism of action, csDMARDs can decrease the advancement of structural joint deterioration in rheumatoid arthritis (RA), lower immune cell activation, and control synovial inflammation. These drugs have different main molecular targets, but they all aim to reduce the inflammatory cascades and aberrant immune responses that fuel the pathophysiology of RA [25].
Methotrexate: The mainstay of csDMARD treatment is still methotrexate, which has anti-inflammatory properties that are different from its antitumor effects. Methotrexate inhibits purine metabolism-related enzymes at low levels utilized in RA, which causes extracellular adenosine a powerful endogenous anti-inflammatory mediator to build up [26]. Adenosine inhibits the activation and proliferation of T cells and macrophages in the synovium, as well as the generation of important pro-inflammatory cytokines including interleukin-6 (IL-6), interleukin-1β, and tumor necrosis factor-α (TNF-α). Methotrexate also limits leukocyte recruitment and tissue damage by decreasing the production of adhesion molecules and matrix metalloproteinases [27].
Sulfasalazine: Sulfasalazine uses a variety of anti-inflammatory pathways to provide its immunomodulatory effects. It prevents nuclear factor-κB (NF-κB) signaling pathway activation, which is a key modulator of inflammatory gene transcription in RA. Sulfasalazine decreases the production of chemokines, adhesion molecules, and pro-inflammatory cytokines via inhibiting NF-κB activation. Sulfasalazine also lowers T-cell proliferation and antibody formation, which contributes to its disease-modifying effects, and inhibits the cyclooxygenase and lipoxygenase pathways, which results in reduced prostaglandin and leukotriene generation [28].
Leflunomide: By blocking dihydroorotate dehydrogenase, a mitochondrial enzyme necessary for de novo pyrimidine production, leflunomide mainly targets adaptive immune responses. This pathway is crucial for the rapid multiplication of activated T and B cells. When pyrimidine synthesis is inhibited, activated lymphocytes undergo cell cycle arrest, which lowers autoantibody production, cytokine-mediated inflammation, and clonal growth. Leflunomide further suppresses synovial inflammation by interfering with tyrosine kinase signaling and lowering the synthesis of inflammatory mediators [29].
Hydroxychloroquine: Through its impact on intracellular processing and innate immunological signaling, hydroxychloroquine modifies immune responses [30]. Hydroxychloroquine inhibits antigen-presenting cells' ability to digest and present antigens by raising the pH of lysosomes and endosomes, which lowers autoreactive T cell activation. Furthermore, toll-like receptor (TLR) 7 and 9 signaling, which is linked to the activation of plasmacytoid dendritic cells and the generation of type I interferons, is inhibited by hydroxychloroquine. Particularly in early or moderate RA, this leads to reduced cytokine release and reduction of inflammatory responses [31].
When it comes to absorption, distribution, metabolism, and elimination, conventional synthetic DMARDs (csDMARDs) have unique pharmacokinetic characteristics. These variations have a substantial impact on long-term tolerability, safety monitoring, commencement of action, and dosage schedules. In order to maximize treatment, reduce toxicity, and guarantee long-term disease management in rheumatoid arthritis (RA), it is crucial to comprehend these factors [32].
Methotrexate (MTX): For RA, methotrexate (MTX) is given at modest weekly dosages, usually beginning at 7.5-10 mg once weekly and gradually increasing to 20-25 mg/week based on tolerability and clinical response. Subcutaneous or intramuscular injection increases bioavailability and lessens gastrointestinal intolerance; oral bioavailability varies from 60-70% at low dosages but falls at larger doses owing to saturable absorption [33]. Methotrexate is mostly removed unaltered by the kidneys, having an elimination half-life of 6–9 hours at low dosages [34]. It is around 50% protein bound and somewhat metabolized by the liver. To lessen mucosal, gastrointestinal, and hematologic damage, regular folic acid intake (5–10 mg/week) is advised. The hazards of hepatotoxicity, myelosuppression, and nephrotoxicity necessitate periodic surveillance of liver enzymes, renal function, and complete blood counts.
Sulfasalazine: Sulfasalazine is taken orally, starting at 500 mg once or twice a day and progressively increasing to a maintenance dosage of 2-3 g/day in split doses. Because intestinal bacteria substantially convert it into sulfapyridine and 5-aminosalicylic acid (5-ASA), it has variable oral absorption (10-30%) [35]. 5-ASA mostly works locally, whereas sulfapyridine is absorbed systemically and contributes to both positive and negative effects. Acetylator status affects sulfapyridine's plasma half-life, which varies from 6 to 17 hours. To increase gastrointestinal tolerance, gradual dosage escalation is used, and it is advised to periodically check the liver's functioning and blood counts [36].
Leflunomide: Leflunomide is taken orally once daily at a dosage of 10–20 mg. The medication's therapeutic action is attributed to its active metabolite, teriflunomide, which has a lengthy elimination half-life of around 14 to 18 days, mostly because of significant enterohepatic circulation [37]. Although it makes once-daily dosage simple, its extended half-life makes it difficult to manage toxicity or prepare for pregnancy. A cholestyramine washout regimen (8 g three times daily for 11 days) is necessary if there are significant side effects or if quick medication clearance is needed. Leflunomide is linked to hepatotoxicity, especially when used with methotrexate, hence monitoring liver enzymes is essentiall [38].
Hydroxychloroquine: After oral treatment, hydroxychloroquine has been effectively absorbed, with a bioavailability of around 70-80%. To reduce toxicity, the usual dosage is 200-400 mg/day, not to exceed 5 mg/kg/day (real body weight) [39]. Due to its wide tissue distribution and lengthy terminal half-life of 40-50 days, hydroxychloroquine accumulates in tissues such the skin, liver, and retina. Baseline and frequent ophthalmologic exams (annually after 5 years of medication, or earlier in high-risk individuals) are necessary to identify retinal toxicity, even though regular laboratory surveillance for hepatic or renal toxicity is not required [40].
A significant development in the treatment of rheumatoid arthritis (RA) is the use of biologic disease-modifying anti-rheumatic medications (bDMARDs), which are the result of a better knowledge of the immunopathological processes underlying the condition. bDMARDs are genetically modified proteins intended to specifically target particular cytokines, receptors, or immune cell populations that are crucial to the pathophysiology of RA, in contrast to traditional synthetic DMARDs, which have widespread immunosuppressive effects. Patients with moderate to severe RA who do not respond well to or are intolerant to csDMARDs, especially methotrexate, are the main candidates for these medications [41].
Superior effectiveness in lowering disease activity, preventing radiographic progression, and enhancing functional outcomes has been shown by bDMARDs. However, parenteral administration, greater susceptibility to infections, and higher expenses are linked with their usage, making cautious patient selection and monitoring necessary [42].
Classification of Biologic DMARDs
Agents: Etanercept, Infliximab, Adalimumab, Golimumab and Certolizumab pegol.
Mechanism of Action: Tumor necrosis factor-α, a crucial pro-inflammatory cytokine implicated in synovial inflammation, leukocyte recruitment, angiogenesis, and joint degeneration, is neutralized by TNF-α inhibitors. These drugs restrict inflammation and structural damage by inhibiting TNF-α signaling, suppressing downstream cytokine cascades, lowering adhesion molecule expression, and preventing osteoclast activation. Methotrexate and TNF inhibitors are frequently used together to increase effectiveness and lower immunogenicity [43].
Administration and Dosing
Agents: Tocilizumab and Sarilumab
Mechanism of Action: IL-6 inhibitors prevent IL-6-mediated signaling by blocking the IL-6 receptor. Synovial inflammation, acute-phase reactions, chronic disease anemia, and systemic RA symptoms are all significantly influenced by IL-6. Systemic symptoms improve and inflammation is rapidly reduced when IL-6 signaling is inhibited. IL-6 inhibitors can be administered alone or in conjunction with csDMARDs [44].
Administration and Dosing
Agent: Rituximab
Mechanism of Action: A monoclonal antibody called rituximab targets the surface antigen CD20, which is expressed on B cells. Through complement-mediated cytotoxicity and apoptosis, it causes B-cell depletion, which lowers the formation of autoantibodies and attenuates immunological activation. Patients with seropositive RA and those who do not respond to TNF-α medications benefit most from rituximab [45].
Administration and Dosing
Agent: Abatacept
Mechanism of Action: The fusion protein abatacept prevents T-cell activation by obstructing the CD80/CD86–CD28 co-stimulatory signal, which is necessary for complete T-cell activation. Reduced cytokine production and subsequent immune activation follow from this.
Administration and Dosing
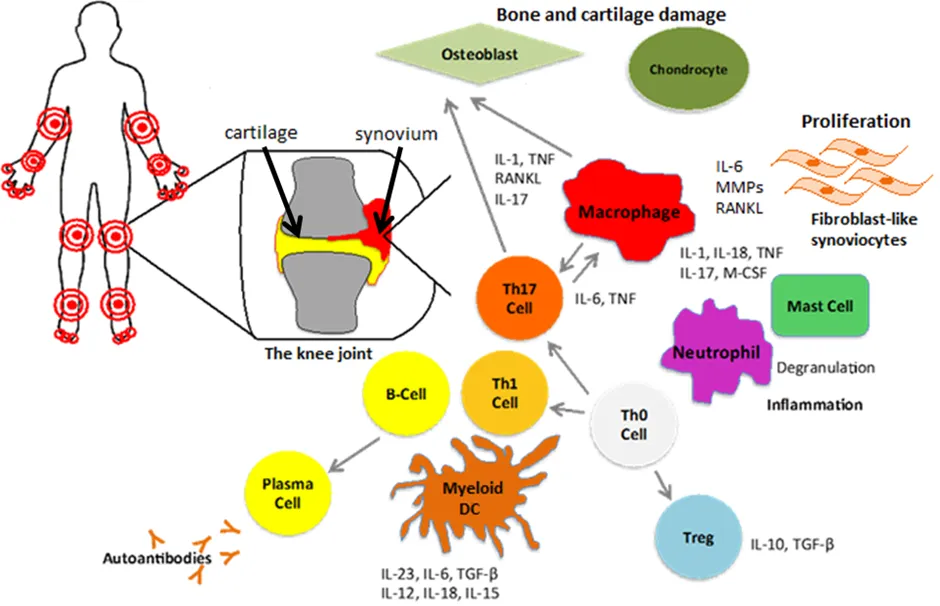
Fig 2: Mechanisms of Action of DMARDs in Rheumatoid Arthritis [47]
|
Parameter |
Conventional Synthetic DMARDs (csDMARDs) |
Biologic DMARDs (bDMARDs) |
Key Clinical Evidence (Bentham style) |
|
Clinical Response |
In early RA, the response is moderate to good; in advanced RA, the effectiveness varies. |
Increased and more reliable clinical response, particularly in cases of csDMARD failure, in moderate-to-severe RA. |
Smolen et al., 2014; van der Heijde et al., 2013 |
|
Disease Activity Scores (DAS28, SDAI, CDAI) |
DAS28 and SDAI gradually decline; remission rates are lower and take longer to reach. |
Significant and quick decline in DAS28/SDAI; increased remission and low rates of disease activity. |
Emery et al., 2015; Fleischmann et al., 2017 |
|
Onset of Action |
Delayed onset: notable improvement takes six to twelve weeks. |
Fast onset: 2-4 weeks, especially with TNF-α and IL-6 inhibitors |
Keystone et al., 2004; Genovese et al., 2008 |
|
Duration & Sustainability of Response |
Although subsequent loss of effectiveness is typical, sustained response is feasible. |
Longer-lasting reaction; persistence is enhanced when combined with MTX |
Maini et al., 2004; Smolen et al., 2016 |
|
Radiographic Progression |
Partial prevention of structural damage; in active RA, development may continue. |
Radiographic advancement is strongly inhibited or completely stopped. |
van der Heijde et al., 2006; Breedveld et al., 2006 |
|
Joint Damage Prevention |
Mostly effective in low-activity or early disease |
Better protection against bone erosion and cartilage loss |
Klareskog et al., 2004; Taylor et al., 2011 |
|
Efficacy in csDMARD-Refractory RA |
Restricted benefit following MTX failure |
High effectiveness in responders who don't respond well to MTX |
Weinblatt et al., 1999; Kremer et al., 2003 |
|
Systemic & Extra-Articular Control |
Systemic inflammation is somewhat controlled |
Improved management of systemic symptoms (CRP, anemia, tiredness) |
Jones et al., 2010; Gabay et al., 2013 |
|
Overall Therapeutic Impact |
First-line treatment that is affordable yet has less predictable and delayed results |
Better structural protection and disease management, but more expenses and safety oversight |
Smolen et al., 2020 (EULAR update) |
Since treatment for rheumatoid arthritis (RA) frequently necessitates chronic and perhaps lifetime medication, safety and tolerability are crucial factors in the long-term management of RA. Drug selection, treatment sequencing, and monitoring procedures are influenced by the different safety profiles of biologic DMARDs (bDMARDs) and conventional synthetic DMARDs (csDMARDs). Optimizing patient outcomes and reducing therapy-related issues need a thorough awareness of their side effects, infection risks, and long-term safety considerations [65].
Although csDMARDs are typically well-known medications with decades of clinical experience, a variety of organ-specific side effects are linked to their extensive immunomodulatory processes.
Strong immunosuppression and heightened vulnerability to infections are the outcomes of bDMARDs' selective targeting of important immune pathways. The biggest risk associated with biologic treatment is serious infections, such as pneumonia, sepsis, and opportunistic infections.
Long-term usage of both csDMARDs and bDMARDs raises concerns regarding malignancy risk, cumulative immunosuppression, and cardiovascular safety. Although early research indicated that biologic therapy may raise the risk of lymphoma, more recent data suggests that the fundamental inflammatory disease activity itself, rather than biologic treatment alone, is a significant factor in malignancy risk [72].
The significance of preventative measures like vaccination, infection screening, and information for patients is highlighted by the possibility that prolonged immunosuppression may also affect vaccine responses and infection consequences. Furthermore, long-term safety statistics have shown that older patients and those with several comorbidities require rigorous risk categorization [73].
Because rheumatoid arthritis (RA) necessitates long-term, sometimes lifetime medication and places a significant financial burden on patients, healthcare systems, and society as a whole, pharmacoeconomic variables are crucial to its management. Economic evaluation is increasingly crucial for directing treatment choices, policy-making, and guideline creation due to the availability of several therapeutic alternatives, such as biologic DMARDs (bDMARDs), conventional synthetic DMARDs (csDMARDs), and more recent targeted medicines. Cost-effectiveness, affordability and accessibility, and their influence on treatment adherence are important pharmacoeconomic factors [74].
Because of their cheap acquisition costs, oral administration, and proven effectiveness in early illness, csDMARDs methotrexate in particular are considered the most economical treatments for RA. csDMARD-based therapies offer positive cost-utility ratios, particularly when implemented early and within a treat-to-target paradigm, as several economic assessments have shown. On the other hand, because too complicated manufacturing procedures, parenteral administration, cold-chain requirements, and monitoring expenditures, bDMARDs are linked too much higher direct costs [75]. Although biologic treatments are more clinically beneficial in csDMARD-inadequate responders, especially when it comes to enhancing quality-adjusted life years (QALYs) and reducing radiographic progression, their additional cost-effectiveness ratios are much greater. As a result, rather than using bDMARDs as first-line treatment, the majority of health economic models advocate using them after csDMARDs have failed. By lowering acquisition costs while preserving comparable performance and safety, the development of biosimilars has heightened the cost-effectiveness profile of biologic therapy and increased the financial viability of advanced RA treatment [76].
The availability of RA treatments varies greatly between areas and healthcare systems. Access to biologic drugs is made easier in high-income nations by insurance coverage and payment systems, albeit step-therapy and prior authorization are frequently necessary. On the other hand, access to bDMARDs is severely restricted in middle-income and low-income nations due to high out-of-pocket costs, lack of reimbursement, and inadequate healthcare financing. As a result, even patients with severe illness continue to rely on csDMARDs. One of the biggest obstacles to the best management of RA is still affordability. High medication costs may delay treatment beginning, limit therapy escalation, or result in early termination. Significant access gaps still exist worldwide, despite the growing readily accessible biosimilars and the inclusion of necessary csDMARDs in national formularies [77].
Treatment adherence and persistence, two important factors in determining therapeutic effectiveness in RA, are strongly impacted by economic strain. Adherence to bDMARD therapy may be adversely affected by high prescription prices, frequent hospital stays for infusions, and indirect expenses including missed productivity and travel [78]. On the other hand, because of its oral dosage and cost, csDMARDs are typically linked to higher long-term adherence, especially in settings with low resources. The immediate advantages of lower medication expenses are eventually countered by non-adherence motivated by financial limitations, which can result in poor disease control, more flare-ups, permanent joint damage, and greater long-term healthcare expenditures. To achieve long-term, patient-cantered RA therapy, pharmacoeconomic factors must be included into therapeutic decision-making [79].
The care of rheumatoid arthritis (RA) now places a strong emphasis on patient-centred outcomes, which reflects a change from just regulating clinical and laboratory indicators to enhancing patients' lived experiences and general quality of life (QoL). RA is a long-term, incapacitating illness that impacts not just physical function but additionally social engagement, psychological health, and productivity at work. Consequently, successful RA care must target objectives that matter significantly to patients, particularly pain alleviation, functional independence, tiredness reduction, mental health, and the capacity to sustain daily and work-related activities [80].
Patients with RA have considerably worse health-related quality of life (HRQoL) because to persistent joint pain, stiffness, exhaustion, and growing functional restriction. It is crucial to include patient-reported outcome measures (PROMs) in addition to clinical disease activity ratings since these symptoms frequently continue even after inflammatory indicators resolve. Patient perspectives on physical function, mental health, and social functioning are frequently recorded using tools like the Health Assessment Questionnaire (HAQ), Short Form-36 (SF-36), and patient global assessment scores [81].
Both csDMARDs and bDMARDs enhanced patient-reported outcomes, according to comparative studies. However, biologic DMARDs typically provide larger and faster advancements in pain, fatigue, physical function, and overall quality of life, especially in patients with moderate to serious disease or those who do not respond well to csDMARDs. bDMARDs can improve involvement in social and professional activities and restore functional capacity by avoiding structural damage and attaining quicker disease management. These advantages must be weighed against the treatment burden, which includes regular monitoring, injection-related pain, and infection worry [82].
Important elements of patient-centered care include collaborative decision-making, treatment adherence, and patient satisfaction. Patient preferences and therapeutic persistence are significantly influenced by factors including simplicity of administration, frequency of treatment, safety concerns, and financial load [83]. While bDMARDs may enhance QoL but provide logistical and financial difficulties that impact long-term adherence, csDMARDs are frequently preferred due to their oral administration and cost. Crucially, superior patient-centered outcomes, such as decreased disability, improved mental health, and improved long-term quality of life, are consistently linked to attaining durable remission or low disease activity with treat-to-target techniques. Therefore, enhancing RA care requires incorporating preferences of patients, requirements, and PROMs into therapeutic decision-making [84].
By converting clinical information into useful, patient-centered recommendations, international treatment guidelines are essential to standardize the therapy of rheumatoid arthritis (RA). To prevent irreparable joint damage and disability, leading rheumatology organizations place a strong emphasis on early diagnosis, quick DMARD beginning, frequent disease activity evaluation, and prompt therapy escalation. The most extensively used worldwide are the recommendations published by the European Alliance of Associations for Rheumatology (EULAR) and the American College of Rheumatology (ACR) [85].
For the majority of patients with recently diagnosed RA, conventional synthetic DMARDs (csDMARDs), especially methotrexate, are regularly recommended as first-line treatment by both ACR and EULAR recommendations. Methotrexate is preferred because of its proven effectiveness, long-term safety records, and affordability. Alternative csDMARDs such sulfasalazine, leflunomide, or hydroxychloroquine are advised for individuals who are intolerant to or contraindicated for methotrexate [86]. Treatment escalation is recommended for individuals who do not obtain sufficient disease control with csDMARD monotherapy. This may involve adding a biologic DMARD (bDMARD) or targeted synthetic DMARD (tsDMARD) to csDMARD combination therapy [87].
Disease severity, prognostic variables, comorbidities, patient desire, and pharmacoeconomic considerations all play a role in the decision between these choices. Before starting biologic therapy, both ACR and EULAR emphasize the significance of screening for latent infections, including hepatitis and TB. Significantly, new guidelines acknowledge the expanding importance of biosimilars and suggest using them as affordable substitutes for original biologics where clinically appropriate [88].
The treat-to-target (T2T) approach is a cornerstone of contemporary RA care that is supported by both ACR and EULAR. This strategy entails establishing a specific therapeutic objective, ideally clinical remission or, alternatively, low disease activity, then modifying therapy on a frequent basis until the goal is reached. The following are important T2T strategy tenets:
When compared to traditional, non-targeted therapies, clinical data shows that T2T techniques improve functional results, lower radiographic progression, improve disease control, and improve quality of life. Additionally, this approach encourages the sensible placement of bDMARDs and csDMARDs, guaranteeing prompt escalation while preventing needless overtreatment [90].
Rheumatoid arthritis (RA) care has gone a long way, but there are still many obstacles and unmet goals that prevent the best possible long-term results and disease control. Even while disease-modifying anti-rheumatic medications (DMARDs) have made RA less incapacitating and more tolerable for many patients, a significant percentage of people still struggle to achieve full remission, indicating persistent treatment gaps. Heterogeneity in the presentation of the disease and response to treatment is one of the main obstacles to managing RA. Patients with RA respond differently to target synthetic drugs, biologic DMARDs, and csDMARDs due to the disease's clinical and biological diversity.
As of right now, there are no reliable biomarkers that can accurately predict treatment failure, side effects, or therapeutic response. Because of this, choosing a course of treatment mostly depends on trial and error, which can postpone effective disease control and subject patients to needless harm. Another significant restriction is incomplete or subsequent loss of responsiveness. Although csDMARDs are useful in the early stages of the illness, many individuals have intolerance or insufficient response. Similarly, due to immunogenicity or illness adaptability, a considerable percentage of patients on bDMARD treatment have secondary non-response. This makes it necessary to switch between therapies often, which raises the complexity of therapy and medical expenses [91].
Specifically with long-term immunosuppression, safety issues continue to be a crucial unmet requirement. While bDMARDs and tsDMARDs increase vulnerability to severe infections, opportunistic pathogens, and reactivation of latent infections, csDMARDs are linked to cumulative organ damage. There is also a dearth of long-term safety information on cardiovascular results, cancer risk, and usage in specific populations such the elderly, pregnant women, and patients with several comorbidities. The high cost of biologic and targeted medicines is a significant obstacle from the standpoint of pharmacoeconomics and healthcare access, particularly in low- and middle-income nations. Health disparities and worse than ideal illness outcomes are caused by limited access, delayed commencement of sophisticated medicines, and uneven payment systems.
Despite the fact that biosimilars are now more affordable, patient, prescriber, and regulatory variables continue to influence their acceptance. Patient-centered outcomes that may continue even when inflammatory disease activity appears to be under control, such as chronic pain, exhaustion, depression, and decreased productivity at work, also have unmet requirements. These aspects are not adequately addressed by current treatment methods, highlighting the need for more individualized and comprehensive treatments.
The desire for enhanced clinical outcomes, satisfy unmet requirements, and increase the sustainability of long-term treatment is driving a rapid evolution in the therapeutic landscape for rheumatoid arthritis (RA). The development of biosimilars and targeted synthetic DMARDs (tsDMARDs), especially Janus kinase (JAK) inhibitors, which are changing treatment paradigms and extending therapy choices beyond traditional and biologic DMARDs, is one of the most significant developments [92].
Biosimilars are biologic drugs that have no clinically significant variations in effectiveness, safety, or immunogenicity from authorized reference biologic DMARDs. In order to address the high cost and restricted accessibility of originator biologics, international organizations have vigorously supported the development and regulatory licensing of biosimilars. In major randomized trials and real-world investigations, biosimilars of TNF-α inhibitors along with additional biologics have shown similar clinical effectiveness, safety, and pharmacokinetic characteristics to their reference drugs in the treatment of RA. Considerable cost reductions have resulted from their launch, promoting earlier consumption of biologic treatment where clinically appropriate and expanding patient access to cutting-edge medicines.
Furthermore, even original biologics have seen price decreases due to heightened market competition. In the future, it is anticipated that greater use of biosimilars may lessen healthcare inequities, especially in low- and middle-income nations. Maintaining physician and patient trust as well as supporting interchangeability and switching methods will need ongoing pharmacovigilance and the creation of real-world data.
A new line of oral medications known as targeted synthetic DMARDs specifically blocks intracellular signaling pathways that are essential for cytokine-mediated inflammation. Amongst these, JAK inhibitors have been a significant development in RA treatment. The Janus kinase–signal transducer and activator of transcription (JAK–STAT) pathway, which carries signals from several pro-inflammatory cytokines, such as interleukins and interferons, is blocked by JAK inhibitors. JAK inhibitors offer broad yet focused immunomodulation by focusing on intracellular signaling instead of external cytokines.
JAK inhibitors have been shown in clinical studies to provide quick start of action, high clinical effectiveness, and considerable reduction of radiographic progression, even in individuals who do not respond well to biologic DMARDs or csDMARDs. JAK inhibitors are appealing substitutes for injectable biologics because the oral route of administration provides a significant benefit in terms of patient comfort and adherence. However, new safety issues have brought attention to the necessity of cautious patient selection, risk stratification, and long-term safety monitoring. These issues include a higher probability of infections, thromboembolic events, and cardiovascular problems in specific patient populations [93].
In the future, it is anticipated that the combination of tailored synthetic DMARDs and biosimilars will provide a more individualized and adaptable approach to RA therapy. Improvements in pharmacogenomics, biomarker discovery, and practical data analytics might make it possible to coordinate patients with the safest and most effective treatment more precisely. Combination tactics, cost-effective treatment algorithms, and optimal therapy sequencing are anticipated to significantly enhance results.
CONCLUSION
Despite significant treatment advancements, rheumatoid arthritis (RA) continues to be a complicated, diverse, and progressive inflammatory disease that places a significant clinical, financial, and societal burden. Over the past two decades, the therapeutic paradigm of RA has advanced considerably with the development of disease-modifying anti-rheumatic medications (DMARDs), permitting earlier intervention, greater disease management, and better long-term results. This study examined the functions, advantages, and disadvantages of biologic DMARDs (bDMARDs) and conventional synthetic DMARDs (csDMARDs) in the treatment of RA today. Because of their demonstrated effectiveness, low cost, and wealth of clinical experience, csDMARDs especially methotrexate remain the mainstay of first-line treatment.
However, in a subgroup of individuals, their efficacy is limited by delayed initiation of action, inconsistent response, and organ-specific toxicity. On the other hand, in patients with moderate-to-severe illness or those who do not respond well to csDMARDs, bDMARDs offer focused inhibition of important inflammatory pathways and show higher effectiveness, especially in avoiding radiographic progression and enhancing patient-reported outcomes. Higher expenses, a higher risk of infection, and immunogenicity issues outweigh these advantages. Prominent rheumatology organizations' international guidelines regularly endorse a treat-to-target approach, stressing early diagnosis, frequent evaluation of disease activity, and prompt medication escalation to attain remission or low disease activity. By increasing accessibility, providing oral therapy choices, and facilitating more customized care, emerging medications like biosimilars and targeted synthetic DMARDs like JAK inhibitors are further changing the therapeutic landscape.
Significant obstacles and unmet requirements still exist in spite of these developments, such as inconsistent treatment response, long-term safety issues, financial constraints, and lingering quality of life degradation. Future developments in precision medicine, biomarker-guided therapy selection, long-term safety optimization, and fair access to efficient medicines will be critical to the management of RA. In summary, a balanced, patient-centered, evidence-based strategy that incorporates clinical effectiveness, safety, pharmacoeconomics, and quality-of-life concerns is necessary for the best possible care of RA. It will be crucial to keep comparing csDMARDs, bDMARDs, and new treatments in order to improve treatment plans and lessen the prevalence of rheumatoid arthritis worldwide.
REFERENCES


Reeta Yadav, Firdaus Rana, Biologic Dmards Vs Conventional Dmards in Rheumatoid Arthritis: A Comparative Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1539-1562, https://doi.org/10.5281/zenodo.20567690
 10.5281/zenodo.20567690
10.5281/zenodo.20567690