
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Bachelor of Pharmacy,MUP’S College Of Pharmacy,Degaon,Risod,Maharashtra, India
2Bsc Nursing Third Year, Vivekananda nursing college Hiwara Ashram , Maharashtra, India.
Calcium supplements are among the most widely consumed dietary adjuncts globally, prescribed predominantly for the prevention and management of osteoporosis, rickets, and nutritional deficiencies. Despite their established skeletal benefits, mounting epidemiological evidence indicates that supplemental calcium—unlike dietary calcium—is associated with a measurable increase in the risk of kidney stone formation, particularly calcium oxalate and calcium phosphate urolithiasis. The underlying mechanisms involve perturbations in urinary calcium excretion, alterations in intestinal oxalate absorption, and shifts in urine supersaturation that collectively favour crystal nucleation and growth.This narrative review synthesizes existing mechanistic, epidemiological, and clinical trial data to elucidate how calcium supplements influence nephrolithiasis risk, A comprehensive literature search was conducted across PubMed/MEDLINE, Scopus, Embase, and Cochrane databases using the terms "calcium supplementation," "kidney stones," "nephrolithiasis," "urolithiasis," "hypercalciuria," "calcium oxalate," and "calcium phosphate." Studies published between 1990 and 2025 were screened; 70 high-quality references comprising randomized controlled trials, The Women's Health Initiative trial demonstrated a 17% increase in kidney stone incidence among women receiving calcium plus vitamin D supplements compared with placebo. Large prospective cohort analyses consistently differentiate supplemental calcium—which acutely raises post-prandial and fasting urinary calcium—from dietary calcium, which reduces free urinary oxalate by forming insoluble intestinal complexes. Key risk-amplifying factors include supplement doses exceeding 1,000 mg elemental calcium per day, between-meal administration, animal protein. Conversely, meal-time dosing, adequate hydration, potassium citrate co-administration, and preference for calcium citrate formulations in at-risk populations substantially attenuate lithogenic risk.Calcium supplementation confers a real but modifiable risk of nephrolithiasis. Individualized strategies encompassing dose reduction, optimized supplement timing, dietary modification, and targeted monitoring can preserve the skeletal benefits of calcium while minimizing urinary stone risk.
Kidney stone disease, medically termed nephrolithiasis or urolithiasis, represents one of the most painful and economically burdensome urological conditions encountered in clinical practice. Globally, the lifetime prevalence of urolithiasis has risen dramatically over the past four decades, affecting an estimated 10–15% of adults in Western nations and exhibiting an upward trend in both industrialized and developing countries alike [1, 2]. In the United States alone, nephrolithiasis accounts for over 2 million physician visits annually and generates healthcare expenditures exceeding $5 billion per year, a figure projected to escalate substantially as the disease burden continues to expand [3].
Concurrently, calcium supplementation has become one of the most prevalent forms of nutritional adjunct use worldwide. Driven primarily by public health campaigns targeting osteoporosis prevention—a condition affecting over 200 million people globally—calcium supplements are consumed by an estimated 43% of adults in the United States, with even higher rates among post-menopausal women and older adults [4, 5]. Medical indications beyond osteoporosis include nutritional deficiency management, hypoparathyroidism, malabsorptive syndromes, chronic kidney disease-related mineral and bone disorder, and adjunctive treatment in preeclampsia prevention [6].
The clinical intersection of these two prevalent conditions creates a therapeutic dilemma of considerable importance. Early mechanistic observations by Pak and colleagues in the 1970s raised the possibility that exogenous calcium intake could augment urinary calcium excretion, thereby promoting the conditions necessary for stone crystal nucleation [7]. However, the subsequent recognition by Curhan and colleagues in the landmark Nurses' Health Study that dietary calcium was paradoxically inversely associated with stone risk complicated the narrative substantially [8]. This divergence between supplemental and dietary calcium has since become one of the most debated topics in nephrology and nutritional medicine.
The mechanistic basis for this divergence is now understood to relate principally to the timing of calcium delivery relative to meals. Dietary calcium, consumed simultaneously with food, binds oxalate within the gastrointestinal lumen, forming insoluble calcium oxalate complexes that are excreted in the stool rather than absorbed into the systemic circulation [9, 10]. Supplemental calcium, particularly when ingested between meals in fasting conditions, lacks this co-ingestion with oxalate-containing foodstuffs; the absorbed calcium then reaches the renal filtrate as a discrete bolus, elevating urinary calcium without a compensatory reduction in urinary oxalate [11].
Beyond this mechanistic distinction, the lithogenic risk associated with calcium supplementation is heterogeneous and shaped by a constellation of pharmacological, dietary, metabolic, and genetic factors. Supplement dose, calcium salt formulation, concurrent vitamin D intake, baseline urinary chemistry, fluid intake, dietary sodium and protein, genetic polymorphisms in calcium-sensing receptors and vitamin D receptor genes, and underlying comorbidities including absorptive hypercalciuria and primary hyperparathyroidism all modulate the individual risk of stone formation [12–14].
This review aims to synthesize the mechanistic, epidemiological, and clinical evidence regarding the relationship between calcium supplementation and nephrolithiasis. By elucidating the pathophysiological pathways through which supplements influence urinary chemistry, characterizing the patient-specific determinants of risk, appraising the principal clinical studies that have informed current understanding, and translating these data into practical, evidence-based preventive strategies, this paper seeks to provide clinicians with a comprehensive, nuanced resource for navigating the dual imperatives of skeletal protection and urolithiasis prevention.
2. Calcium Homeostasis and Metabolism
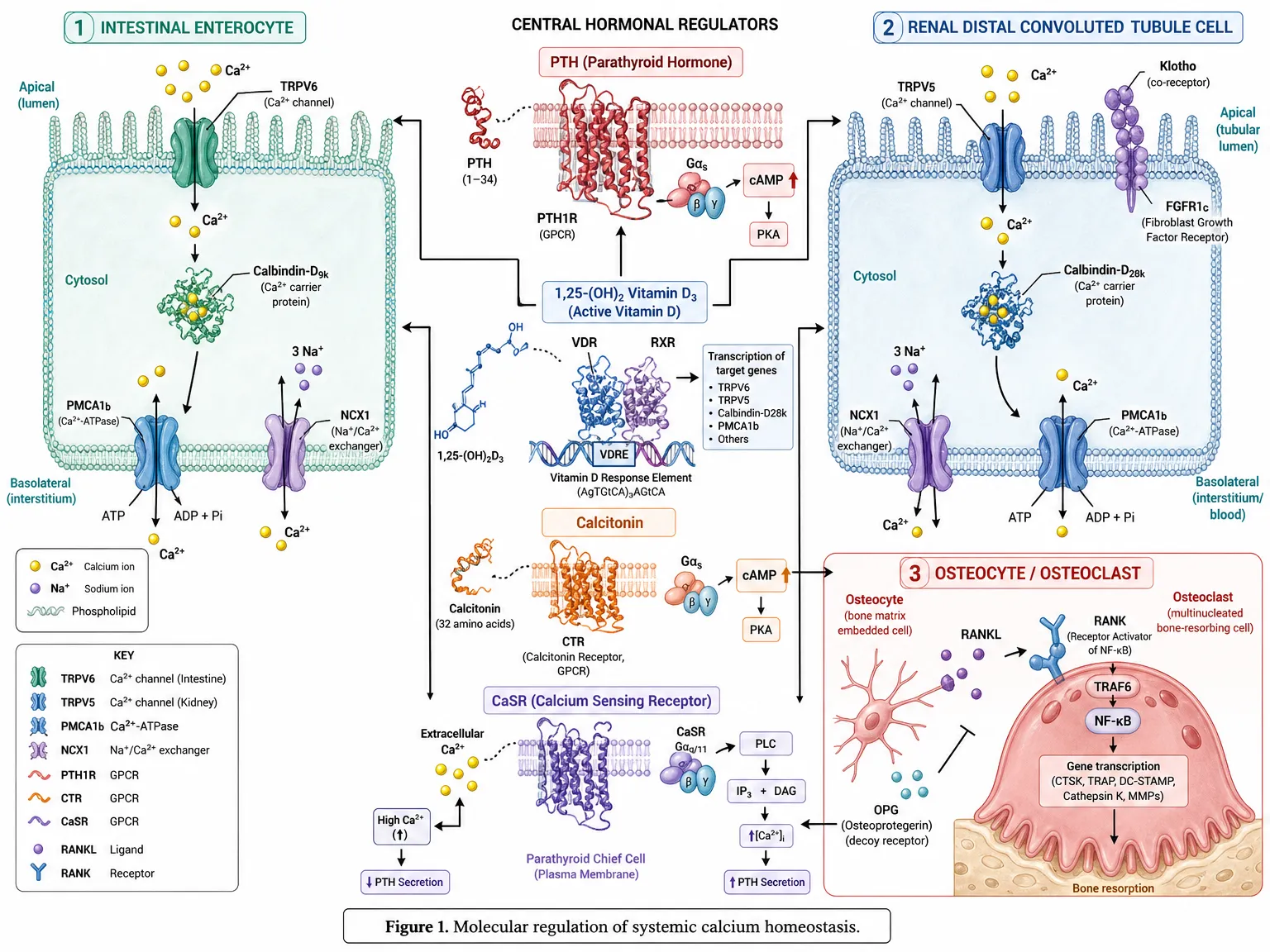
Figure 1. Molecular regulation of systemic calcium homeostasis. Coordinated action of intestinal absorption (TRPV6/Calbindin-D9k/PMCA1b), renal reabsorption (TRPV5/Calbindin-D28k/Klotho), and bone remodeling (RANK-RANKL-OPG), governed by PTH, 1,25-(OH)₂ Vitamin D₃, calcitonin, and the calcium-sensing receptor (CaSR).
2.1 Systemic Calcium Regulation
Calcium is the most abundant mineral in the human body, with approximately 99% residing in the skeletal and dental tissues as hydroxyapatite crystals [15]. The remaining 1% circulates in the blood and extracellular fluid, performing essential roles in neuromuscular transmission, cardiac conduction, hormonal secretion, coagulation, and intracellular signalling cascades [16]. The serum calcium concentration is maintained within a remarkably narrow physiological range of 8.5–10.2 mg/dL through the integrated actions of three primary regulatory hormones: parathyroid hormone (PTH), calcitriol (1,25-dihydroxyvitamin D3), and calcitonin [17].
When serum ionized calcium falls, calcium-sensing receptors (CaSR) on parathyroid chief cells detect this perturbation and trigger rapid PTH secretion. PTH exerts its principal effects on three target organs: in bone, it stimulates osteoclastic resorption, releasing calcium and phosphate into the circulation; in the kidney, it enhances calcium reabsorption in the distal convoluted tubule while reducing phosphate reabsorption; and in the kidney it activates 1-alpha-hydroxylase, the enzyme responsible for converting 25-hydroxyvitamin D to the active calcitriol form [18, 19]. Calcitriol in turn upregulates intestinal calcium absorption through transcellular and paracellular pathways, completing a tightly orchestrated feedback loop that maintains calcium homeostasis across a wide range of dietary intake levels [20].
The kidney plays a particularly central role in this regulatory axis. Under normal conditions, approximately 9,000 mg of calcium is filtered daily at the glomerulus; 98–99% is reabsorbed along the nephron, with only 100–250 mg excreted in the urine [21]. Tubular reabsorption is distributed across nephron segments: roughly 65% occurs in the proximal tubule via passive paracellular mechanisms driven by solute-linked water flux, 20–25% in the thick ascending limb of the loop of Henle, and the remaining 5–10% in the distal tubule under PTH and calcitriol regulation [22]. Disruption of any component of this intricate system—whether by exogenous calcium loading, hormonal dysregulation, or tubular dysfunction—can shift the urinary calcium balance toward hypercalciuria, the most prevalent biochemical abnormality in calcium stone formers [23].
2.2 Intestinal Calcium Absorption
Intestinal calcium absorption operates through two mechanistically distinct pathways. Transcellular active transport, the dominant route at low-to-moderate calcium intakes, involves sequential steps: luminal entry through apical transient receptor potential vanilloid type 6 (TRPV6) channels, intracellular shuttling bound to calbindin-D9k, and basolateral extrusion via the plasma membrane Ca-ATPase (PMCA1b) and sodium-calcium exchanger (NCX1) [24]. This process is tightly regulated by calcitriol, which upregulates the gene expression of TRPV6, calbindin-D9k, and PMCA1b, effectively amplifying absorptive capacity in states of calcium insufficiency [25].
Paracellular passive transport operates proportionally to the luminal calcium concentration and occurs throughout the small intestine via tight junction proteins, including claudin-2 and claudin-12 [26]. This pathway becomes increasingly important at higher calcium intakes when the transcellular route is saturated. The net fractional absorption of calcium from supplements typically ranges from 25–35%, influenced by calcium salt form, meal co-ingestion, gastric acid output, vitamin D status, age, and the baseline intestinal calcium absorption efficiency of the individual [27, 28].
2.3 Renal Calcium Handling and Urinary Excretion
The determinants of urinary calcium excretion extend well beyond simple filtration and encompass a complex interplay of dietary, hormonal, acid-base, and pharmacological factors. The calciuretic response to an oral calcium load is characteristically biphasic: an initial early phase occurring within two hours reflects enhanced filtered load from absorbed calcium, while a later phase at four to six hours corresponds to PTH suppression-mediated reduction in tubular reabsorption [29]. Supplemental calcium ingested between meals tends to produce a more pronounced and sustained calciuric response compared with meal-embedded dietary calcium, because the absence of concurrent intestinal oxalate binding allows a greater proportion of ingested calcium to be absorbed [11, 30].
Under physiological conditions, urinary calcium excretion above 250 mg/day in women or 300 mg/day in men defines hypercalciuria, which is present in approximately 40–50% of calcium stone formers [31]. In calcium supplement users, transient or sustained elevation of urinary calcium into and beyond this hypercalciuric range represents the primary lithogenic mechanism, operating synergistically with reduced urinary volume, diminished urinary citrate, and altered urinary pH [32].
3. Calcium Supplements: Types and Clinical Uses
3.1 Formulations and Elemental Calcium Content
Commercial calcium supplements are available in numerous salt forms, each differing in elemental calcium content, bioavailability, gastric acid dependence, palatability, and cost (Table 1). Calcium carbonate, the most widely prescribed and purchased over-the-counter formulation, provides the highest elemental calcium concentration at approximately 40% by mass, requiring only two to three tablets to deliver 1,000 mg of elemental calcium daily [33]. However, its dissolution and absorption are highly dependent on gastric acid; absorption is substantially reduced in individuals with achlorhydria, those taking proton pump inhibitors (PPIs), or elderly patients with age-related hypochlorhydria [34].
Calcium citrate, with an elemental content of approximately 21%, is acid-independent in its absorption and represents the preferred formulation for patients on acid-suppressive therapy, those with inflammatory bowel disease, and older individuals [35]. Several studies suggest that calcium citrate is not only more bioavailable than calcium carbonate across a range of physiological conditions but may also be associated with a somewhat lower urinary calcium excretion per milligram of elemental calcium absorbed [36]. Calcium phosphate (tribasic), calcium gluconate, calcium lactate, and calcium acetate represent additional formulations with distinct clinical niches, including phosphate binding in chronic kidney disease and emergency intravenous calcium repletion [37].
Table 1. Types of Calcium Supplements: Elemental Content, Administration, and Clinical Profile
|
Supplement Type |
Elemental Ca (%) |
Timing |
Advantages |
Disadvantages |
|
Calcium Carbonate |
40% |
With meals |
Inexpensive; most common |
Constipation, bloating; reduced absorption if achlorhydria |
|
Calcium Citrate |
21% |
Any time |
Better absorbed; suitable for elderly |
More expensive; larger tablet size |
|
Calcium Phosphate |
38% |
With meals |
Well tolerated; added phosphate benefit |
Less widely available |
|
Calcium Gluconate |
9% |
IV or oral |
Used in hypocalcaemia emergencies |
Low elemental Ca; high pill burden |
|
Calcium Lactate |
13% |
With or without meals |
Moderate absorption |
Very low elemental Ca per tablet |
|
Calcium Acetate |
25% |
With meals |
Phosphate binder in CKD |
GI side effects common |
Ca = calcium; CKD = chronic kidney disease; IV = intravenous; GI = gastrointestinal; PPI = proton pump inhibitor.
3.2 Clinical Indications for Calcium Supplementation
The medical rationale for calcium supplementation spans a broad range of conditions. Osteoporosis, the most prevalent indication, affects approximately one in three women and one in five men over the age of 50 globally, and adequate calcium intake is widely regarded as a cornerstone of skeletal preservation [38]. National guidelines from bodies including the Institute of Medicine (IOM), the National Osteoporosis Foundation, and the European Society for Clinical and Economic Aspects of Osteoporosis universally recommend calcium intakes of 1,000–1,200 mg/day for adults over 50, with supplementation advised when dietary sources are insufficient [39].
Beyond osteoporosis, calcium is supplemented in nutritional deficiency syndromes arising from malabsorptive conditions such as celiac disease, inflammatory bowel disease, and post-bariatric surgery states [40]. In the management of hypoparathyroidism, high-dose oral calcium supplementation is essential for controlling hypocalcaemia in patients whose residual PTH activity is insufficient to maintain serum calcium homeostasis without exogenous support [41]. In chronic kidney disease, calcium-based phosphate binders—particularly calcium carbonate and calcium acetate—are employed to control hyperphosphatemia and secondary hyperparathyroidism, although their use has declined with the advent of non-calcium-based alternatives [42]. Calcium gluconate by intravenous infusion remains the first-line treatment for severe acute hypocalcaemia, hyperkalemia-induced cardiac arrhythmia, and hydrofluoric acid exposure [43].
An important nuance in the epidemiology of calcium supplementation is that a substantial proportion of supplement consumption occurs outside formal medical supervision. Survey data suggest that a large majority of individuals purchasing over-the-counter calcium supplements do so based on general wellness motivations, media and marketing influences, or self-directed prevention strategies, often at doses exceeding dietary reference intake recommendations [44]. This unmonitored supplementation pattern contributes to the lithogenic risk profile, as dose optimization and appropriate timing guidance are seldom provided in non-prescription contexts [45].
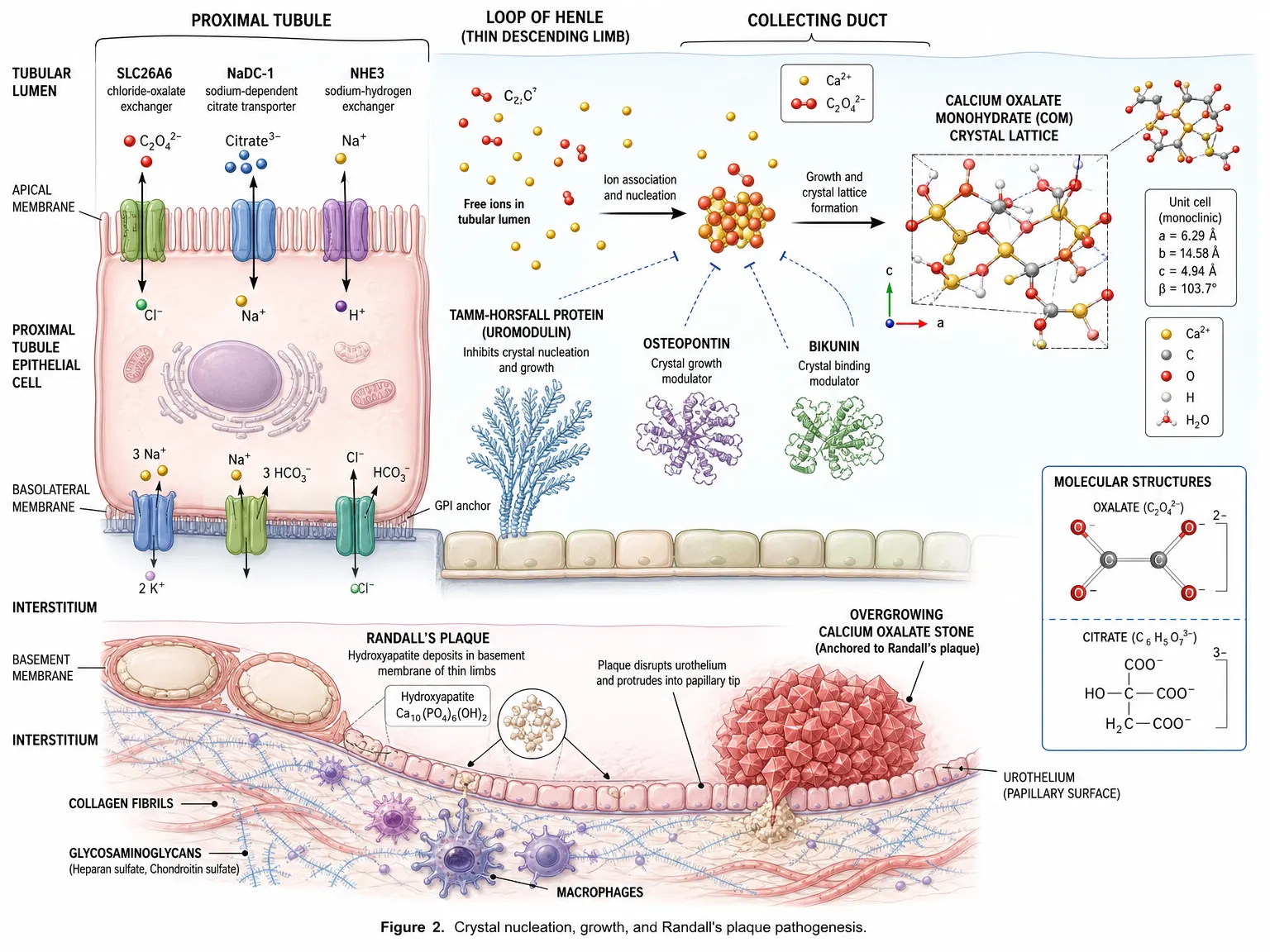
Figure 2. Crystal nucleation, growth, and Randall’s plaque pathogenesis. Free Ca²⁺ and oxalate ions in the tubular lumen associate to form calcium oxalate monohydrate (COM) crystals, modulated by uromodulin, osteopontin, and bikunin. Interstitial hydroxyapatite deposits (Randall’s plaque) anchor overgrowing calcium oxalate stones at the papillary tip..
Kidney stone disease has undergone a significant epidemiological transition over the past century. Once regarded as predominantly a disease of affluent men in temperate climates, nephrolithiasis now exhibits rising prevalence across both sexes, all racial and ethnic groups, and an expanding range of geographic regions [1, 46]. In the United States, the overall prevalence increased from approximately 3.8% in 1976–1980 to nearly 9% by 2007–2010, with more recent estimates suggesting rates approaching 11% in certain subgroups [3]. A parallel increase has been documented in Europe, the Middle East, and Asia. Particularly noteworthy is the rising incidence in women and children, demographic groups historically considered lower risk [47].
The economic and quality-of-life impact of nephrolithiasis is substantial. A kidney stone episode typically results in severe acute flank pain radiating to the groin (renal colic), haematuria, nausea, and vomiting, often necessitating emergency department attendance, urological intervention, and time away from occupational responsibilities [48]. Recurrence rates are high, with approximately 50% of first-time stone formers experiencing a subsequent episode within ten years without preventive intervention [49]. Chronic stone disease is additionally associated with the development of chronic kidney disease, hypertension, and in some cases progression to end-stage renal disease, particularly in the context of recurrent obstructive nephropathy or infection-related stones [50].
4.2 Stone Composition and Types
Kidney stones are classified by their mineralogical composition, which has direct implications for pathogenesis, prevention, and management. Calcium oxalate stones represent the most prevalent subtype, accounting for approximately 70–80% of all stones in developed nations [51]. These occur in two crystalline forms: calcium oxalate monohydrate (whewellite), which tends to form harder, more adherent stones, and calcium oxalate dihydrate (weddellite), which forms softer, more friable calculi. Calcium phosphate stones (hydroxyapatite and brushite) account for 5–10% and are particularly associated with distal renal tubular acidosis, primary hyperparathyroidism, and alkaline urine conditions [52]. Mixed calcium oxalate-phosphate stones are common, reflecting the concurrent lithogenic influence of multiple urinary risk factors.
Uric acid stones, comprising approximately 5–10% of stones in Western nations, are associated with a persistently acidic urine pH below 5.5, hyperuricosuria, metabolic syndrome, and gout [53]. Struvite (magnesium ammonium phosphate) stones, accounting for 1–5%, arise almost exclusively in the context of urinary tract infection with urease-producing organisms and are more prevalent in women with recurrent infections [54]. Cystine stones are rare, representing less than 1% of total stone burden, but are characterized by early onset, high recurrence, and challenging medical management due to the underlying genetic defect in cystinuria [55].
4.3 Pathophysiology of Stone Formation
The fundamental prerequisite for kidney stone formation is urinary supersaturation with respect to the constituent ions of a given crystal phase. Supersaturation is a thermodynamic state in which the product of ionic concentrations exceeds the solubility product of the crystal, creating a thermodynamic driving force for precipitation. However, crystallization does not occur instantaneously at the point of supersaturation; a metastable zone exists between the solubility product and the formation product at which crystals can grow on pre-existing nuclei but cannot spontaneously nucleate de novo [56]. This distinction between nucleation, growth, and aggregation underpins the role of urinary inhibitors and promoters in modulating stone formation beyond simple concentration effects.
The principal urinary inhibitors of crystallization include citrate, which forms soluble complexes with calcium and inhibits crystal growth through adsorption onto crystal surfaces; Tamm-Horsfall protein (uromodulin), which interferes with crystal aggregation; osteopontin; nephrocalcin; and urinary prothrombin fragment 1 [57]. Reduced levels of these inhibitors—frequently encountered in stone formers—contribute to crystal formation even at urinary ion concentrations that might be tolerated without consequence in individuals with robust inhibitory activity. Urinary citrate is of particular therapeutic importance because it is readily augmented through potassium citrate supplementation and dietary modification [58].
5. Mechanisms Linking Calcium Supplementation to Kidney Stone Formation
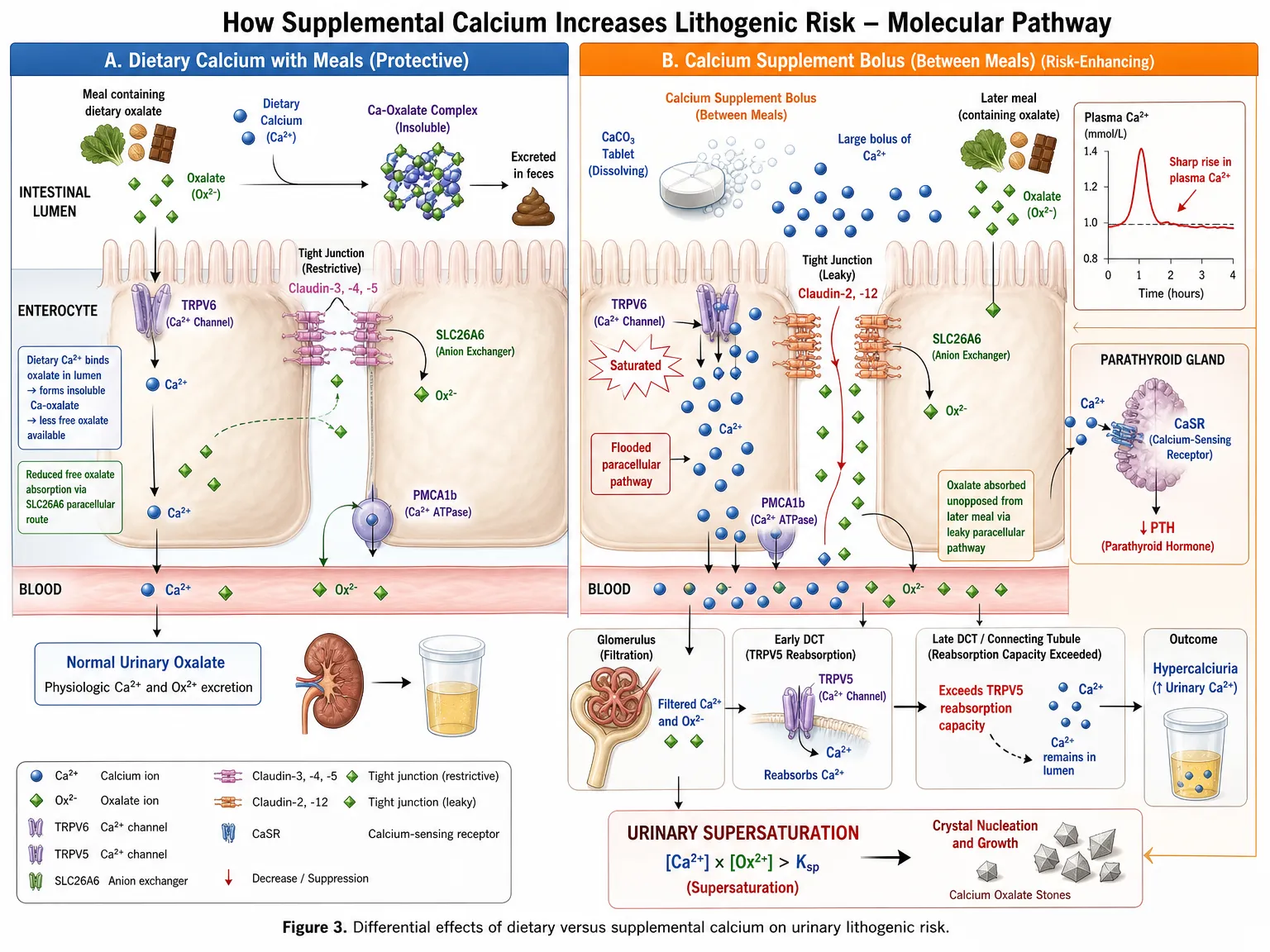
Figure 3. Differential effects of dietary versus supplemental calcium on urinary lithogenic risk. Mealtime dietary calcium binds luminal oxalate (protective), whereas between-meal supplement boluses saturate TRPV6, flood the paracellular pathway, raise plasma Ca²⁺, exceed TRPV5 reabsorption capacity, and drive urinary supersaturation.
5.1 Postprandial Hypercalciuria and Supplement Timing
The most consistently demonstrated mechanism by which calcium supplements promote nephrolithiasis is through augmentation of urinary calcium excretion, particularly when supplements are consumed in the fasting state or between meals [11, 29]. Under normal physiological conditions, a modest increase in serum calcium following intestinal absorption triggers CaSR-mediated suppression of PTH, which in turn reduces tubular reabsorption of calcium and allows the excess absorbed calcium to be cleared renally. When calcium is delivered as a concentrated supplement dose—typically 500–1,000 mg of elemental calcium—the resultant serum calcium peak is substantially greater than that produced by the same amount of calcium ingested as part of a mixed meal, where gastric emptying is slowed, absorption is distributed over a longer period, and concurrent food components buffer the absorptive rate [29, 59].
Studies employing 24-hour urine collections and timed fractionated specimens have demonstrated that supplemental calcium reliably increases urinary calcium by 25–50 mg/day at doses of 1,000 mg/day, with greater increments at higher doses [60]. The calciuric effect is more pronounced with calcium carbonate than with calcium citrate in fasting conditions, likely reflecting differences in the kinetics of calcium release and absorption in the absence of gastric acid [36]. Critically, the calciuric effect of supplements is not offset by a concomitant reduction in urinary oxalate—a distinguishing feature from dietary calcium consumption, where the binding of luminal oxalate results in reduced urinary oxalate that partially counterbalances the pro-lithogenic effect of increased urinary calcium [9, 10].
5.2 Urinary Supersaturation and Crystal Formation
The net lithogenic effect of calcium supplementation can be quantified through the relative supersaturation ratio (RSR) or supersaturation index for calcium oxalate and calcium phosphate, which integrates the concentrations of all relevant ions (calcium, oxalate, phosphate, citrate, magnesium, uric acid) within the urine matrix [61]. Studies employing Equil2 or similar ion-speciation software have demonstrated that supplemental calcium consistently increases the calcium oxalate relative supersaturation, particularly in individuals who begin with high-normal urinary oxalate or reduced urinary citrate [62].
The supersaturation-mediated risk is amplified by low urine volume, which is arguably the single most potent modifiable risk factor for all stone types. Low fluid intake reduces the dilutional capacity of the urine, compressing the same ion load into a smaller volume and disproportionately raising the activity product for crystallization [63]. This explains why calcium supplement users who maintain high fluid intake—with a target urine output exceeding 2 L/day—appear to have substantially lower stone incidence than those with poor hydration habits, even at equivalent calcium supplement doses [64].
5.3 Vitamin D Co-Administration and Synergistic Calciuresis
A substantial proportion of calcium supplements are sold in combination with vitamin D, reflecting the synergistic role of calcitriol in enhancing intestinal calcium absorption and the established association between vitamin D deficiency and poor calcium bioavailability. However, when both nutrients are supplemented concurrently, the lithogenic potential is amplified beyond the effect of calcium alone [65]. The Women's Health Initiative trial, which remains the largest randomized controlled trial addressing this question, administered combined calcium (1,000 mg) plus vitamin D (400 IU) to post-menopausal women; the observed 17% increase in kidney stone incidence was attributed to the combination product rather than vitamin D alone, as supplemental vitamin D at physiological doses has modest direct calciuric effects [66].
At higher vitamin D doses—increasingly encountered in clinical practice as supraphysiologic repletion protocols have become more prevalent—the upregulation of intestinal calcium transporter expression and the resultant increase in fractional calcium absorption can produce more pronounced elevations in urinary calcium [67]. A literature review by Gallagher and Bhalla found a dose-dependent relationship between vitamin D supplementation and urinary calcium excretion, with significant calciuria observed at 25-hydroxyvitamin D concentrations consistently above 80 ng/mL [68]. The clinical implication is that calcium supplement users who are simultaneously receiving high-dose vitamin D therapy represent a particularly high-risk group requiring targeted monitoring.
5.4 Alterations in Urinary Citrate
Urinary citrate represents a critical determinant of stone risk whose relationship to calcium supplementation is mechanistically complex and clinically underappreciated. Citrate inhibits calcium stone formation through multiple pathways: it forms soluble calcium citrate complexes that reduce the free ionic calcium available for crystallization, it directly inhibits crystal nucleation and growth through surface adsorption, and it reduces the aggregation of existing crystals into clinically significant calculi [57]. Hypocitraturia—defined as urinary citrate below 320 mg/day in women or 250 mg/day in men—is present in approximately 20–60% of calcium stone formers and represents an independent and treatable lithogenic abnormality [58].
Calcium supplements, particularly calcium carbonate, can produce a mild metabolic alkalosis following absorption, which in turn stimulates tubular reabsorption of citrate via increased peritubular bicarbonate and consequent reduced renal citrate excretion [69]. Additionally, high calcium intakes may reduce intracellular citrate availability in renal tubular cells through mechanisms related to mitochondrial citrate metabolism. Conversely, dietary patterns high in fruits and vegetables—which contribute to alkaline urine through organic anion metabolism—tend to increase urinary citrate, partially explaining why plant-rich dietary patterns are consistently associated with lower stone risk independent of calcium intake [70].
5.5 Effects on Urinary pH and Calcium Phosphate Supersaturation
Urinary pH profoundly influences the solubility of calcium phosphate, with higher pH values (above 6.0–6.5) increasing calcium phosphate supersaturation and stone-forming propensity. Calcium carbonate supplementation has been shown to transiently alkalinize urine due to the generation of bicarbonate during carbonate hydrolysis, which may promote calcium phosphate crystallization in susceptible individuals—particularly those with a pre-existing tendency toward brushite or hydroxyapatite stone formation [71]. This is of particular relevance in post-menopausal women and individuals on thiazide diuretics, where the combination of high urinary calcium and alkaline urine creates conditions favouring phosphatic stones. Calcium citrate, by providing citrate anion rather than carbonate, may have distinct effects on urinary pH and calcium phosphate supersaturation compared with calcium carbonate [72].
6. Risk Factors Affecting Stone Formation in Calcium Supplement Users
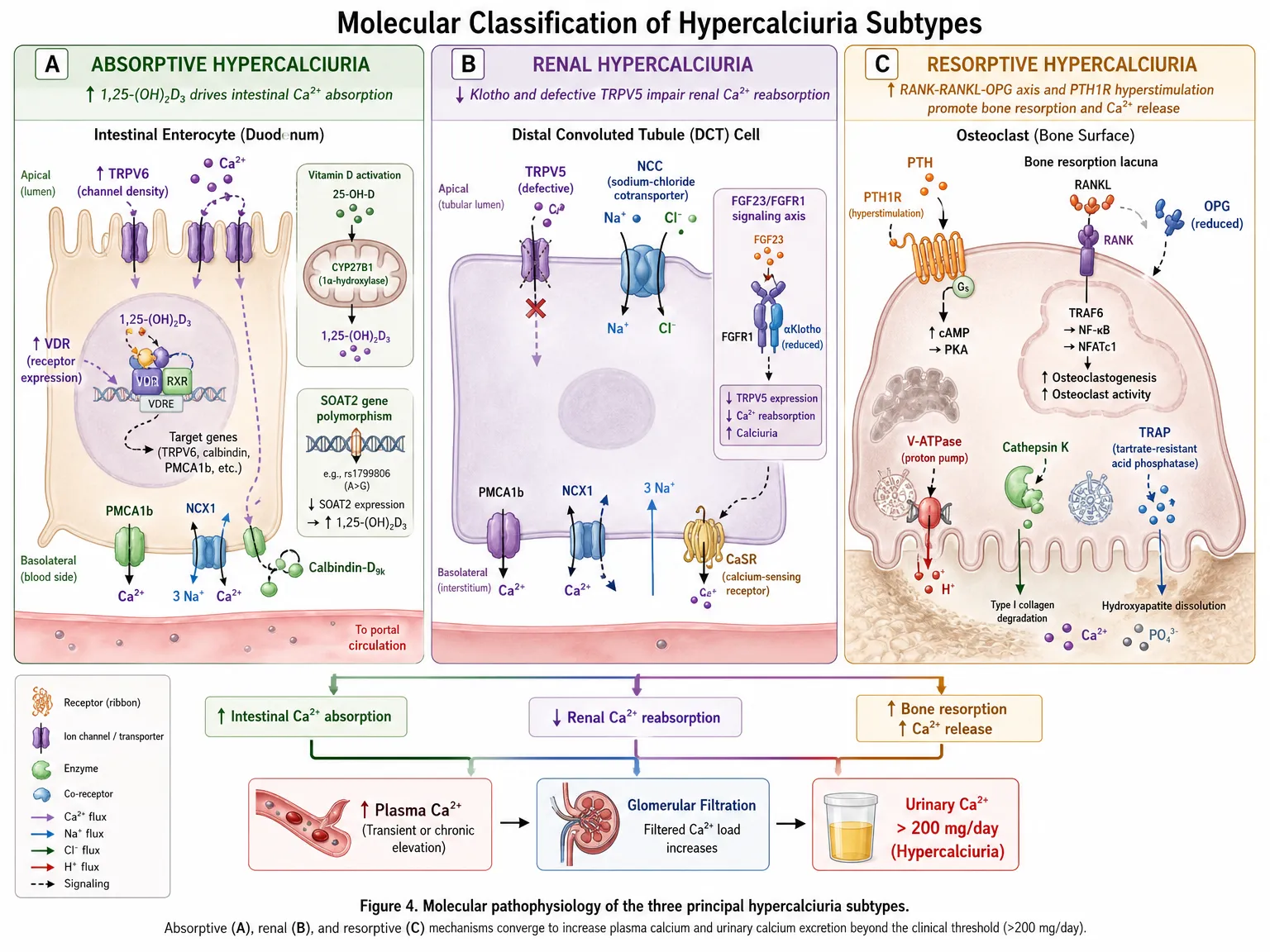
Figure 4. Molecular pathophysiology of the three principal hypercalciuria subtypes — absorptive (↑VDR/TRPV6), renal (defective TRPV5/Klotho), and resorptive (RANK-RANKL/PTH1R-driven osteoclast activity) — converging on urinary Ca²⁺ excretion >200 mg/day.
6.1 Patient-Level Risk Factors
The risk of kidney stone formation in calcium supplement users is not uniform; rather, it reflects a complex interaction between pharmacological exposures and individual biological susceptibilities. Absorptive hypercalciuria, the most common metabolic abnormality in recurrent calcium stone formers, is caused by excessive intestinal calcium absorption secondary to upregulated TRPV6 expression, increased intestinal calcitriol sensitivity, or calcitriol overproduction [23]. Individuals with this condition have a markedly elevated calciuric response to supplemental calcium, as their intestinal absorptive capacity is already operating at an augmented baseline.
Genetic polymorphisms modulate susceptibility at multiple levels. Variants in the vitamin D receptor (VDR) gene—particularly the BsmI, TaqI, ApaI, and FokI polymorphisms—influence calcitriol-mediated calcium transporter expression and have been associated with differential stone risk in calcium supplement users [73]. CaSR gene variants, including the A986S polymorphism, modulate the set-point of calcium sensing in the kidney and affect the threshold of calciuresis in response to a given calcium load [74]. Polymorphisms in the solute carrier gene SLC26A6, which encodes the intestinal oxalate-chloride exchanger, influence net intestinal oxalate handling and thereby modify the degree to which dietary and supplemental calcium reduces urinary oxalate [75].
6.2 Pharmacological and Dietary Determinants
At the pharmacological level, dose is the most directly modifiable risk determinant. The calciuric effect of supplements follows a dose-response relationship; doses exceeding 1,000 mg elemental calcium per day—whether administered as a single bolus or across multiple doses—produce significantly greater urinary calcium increments than lower doses, increasing stone risk proportionally [60]. The timing of supplement ingestion relative to meals constitutes an equally critical determinant: between-meal administration consistently produces higher urinary calcium and higher calcium oxalate supersaturation compared with meal-time ingestion [11]. These pharmacological factors interact, such that a high dose taken between meals represents the highest-risk combination.
Concurrent dietary habits critically modulate stone risk in supplement users. High sodium intake increases natriuresis; the coupled renal handling of sodium and calcium means that for every 2,300 mg increase in dietary sodium, urinary calcium rises by approximately 40 mg/day [76]. High animal protein intake creates an acid load that promotes bone-buffering calcium release, suppresses tubular calcium reabsorption, reduces urinary citrate, and increases urinary uric acid—a complex set of changes that collectively amplify lithogenic risk beyond the effect of calcium supplements alone [77]. Conversely, a high intake of dietary citrate from fruits and vegetables, adequate fluid consumption, and dietary oxalate awareness each contribute to stone risk attenuation [78].
Table 2. Risk Factors Affecting Kidney Stone Formation in Calcium Supplement Users
|
Risk Factor |
Modifiability |
Mechanism / Comment |
|
High supplement dose |
Modifiable |
Doses >1,000 mg/day elemental Ca raise urinary calcium significantly |
|
Supplement timing (between meals) |
Modifiable |
Fasting intake decouples intestinal absorption from oxalate binding |
|
Low fluid intake |
Modifiable |
Concentrates urine; increases supersaturation of calcium salts |
|
High dietary sodium |
Modifiable |
Natriuresis coupled with calciuresis |
|
High protein diet |
Modifiable |
Acid load promotes bone resorption and reduces tubular Ca reabsorption |
|
Low dietary potassium/citrate |
Modifiable |
Reduces urinary citrate, a key inhibitor of crystal growth |
|
Absorptive hypercalciuria |
Non-modifiable |
Genetic upregulation of intestinal Ca transport |
|
Primary hyperparathyroidism |
Non-modifiable (treatable) |
Elevated PTH drives renal Ca excretion |
|
Renal tubular acidosis type 1 |
Non-modifiable |
Alkaline urine promotes calcium phosphate crystallization |
|
Vitamin D supplementation |
Modifiable |
Excessive doses increase intestinal Ca absorption and urinary Ca |
|
Obesity / metabolic syndrome |
Partially modifiable |
Associated with uric acid and calcium oxalate stones |
|
Previous kidney stone history |
Non-modifiable |
Strongest single predictor of recurrence |
|
Male sex, age >50 |
Non-modifiable |
Peak incidence in 5th–6th decade |
|
Post-menopausal status |
Non-modifiable |
Loss of estrogen reduces renal Ca conservation |
CKD = chronic kidney disease; PTH = parathyroid hormone; PPI = proton pump inhibitor.
7.1 Large Prospective Cohort Studies
The foundational epidemiological insight into calcium intake and kidney stone risk emerged from the prospective cohort investigations of Curhan and colleagues, whose analyses of the Health Professionals Follow-Up Study (HPFS) and the Nurses' Health Studies I and II produced the striking observation that higher dietary calcium intake was inversely associated with stone risk in both men and women [8, 79]. In the HPFS analysis of 45,619 men followed for six years, those in the highest quintile of dietary calcium intake had a 34% lower risk of symptomatic kidney stones compared with the lowest quintile, an association that persisted after adjustment for multiple dietary and metabolic covariates. The Nurses' Health Study I, encompassing 91,731 women followed for 12 years, yielded similar findings, with high dietary calcium conferring approximately 35% risk reduction compared with low intake.
Crucially, these studies simultaneously revealed that supplemental calcium use was associated with a modest but statistically significant increase in stone risk—an association opposite in direction to that observed with dietary calcium [80]. This divergence provided the initial epidemiological foundation for the mechanistic hypothesis that the mode and timing of calcium delivery, rather than calcium per se, was the critical determinant of lithogenic risk.
The European Prospective Investigation into Cancer and Nutrition (EPIC-Norfolk) cohort study, involving 25,639 participants, corroborated these findings in a British population, demonstrating that supplement use was associated with increased stone risk while dietary calcium from dairy and other food sources was either neutral or marginally protective [81]. Taken together, these cohort data established a consistent narrative distinguishing the stone-risk profiles of supplemental versus dietary calcium across diverse populations and study designs.
7.2 Randomized Controlled Trials
The Women's Health Initiative (WHI) Calcium and Vitamin D (CaD) trial remains the most definitive randomized controlled trial evidence available on the relationship between calcium supplementation and nephrolithiasis [66]. This double-blind, placebo-controlled trial enrolled 36,282 post-menopausal women aged 50–79 years and randomized them to 1,000 mg of elemental calcium (as calcium carbonate) plus 400 IU of vitamin D3 daily versus placebo, with a mean follow-up of 7.0 years. The primary findings, published by Jackson and colleagues in 2006, demonstrated a hazard ratio of 1.17 (95% CI 1.02–1.34) for self-reported kidney stone formation in the active treatment group, representing a 17% increase in kidney stone incidence compared with placebo.
Secondary analyses of the WHI CaD trial revealed important nuances [82]. The increased stone risk was largely confined to women who were not taking personal calcium supplements at baseline; among women who were already supplement users at the time of randomization, no significant additional risk was observed with the study intervention. This suggested a possible ceiling effect in calciuresis or an adaptation of urinary chemistry to chronic calcium supplementation, though the biological basis for this observation remains debated.
The RECORD (Randomized Evaluation of Calcium or vitamin D) trial, conducted in 5,292 elderly patients who had experienced a recent low-trauma fracture, randomized participants to calcium (1,000 mg/day), vitamin D (800 IU/day), both, or placebo over a median of 24 months, with a range up to 62 months [83]. This trial did not report a statistically significant increase in kidney stone incidence, though it was underpowered to detect stone endpoints, as nephrolithiasis was a pre-specified secondary safety outcome rather than a primary endpoint. The RECORD data are thus informative but not dispositive regarding stone risk.
The trial by Borghi and colleagues, while not primarily addressing supplemental calcium, provided pivotal mechanistic and clinical evidence [84]. This Italian randomized trial enrolled 120 men with recurrent calcium oxalate urolithiasis and compared a low-calcium diet (400 mg/day) with a normal-calcium, low-protein, low-salt diet (1,200 mg/day dietary calcium). Counter-intuitively, the normal-calcium diet produced a significantly lower recurrence rate of stones after five years (38% vs. 20% recurrence), providing definitive clinical evidence that dietary calcium—consumed with meals to bind intestinal oxalate—reduces stone risk relative to calcium restriction, even in individuals with established stone disease.
Table 3. Key Clinical Studies on Calcium Supplementation and Kidney Stone Risk
|
Study |
Population |
Intervention |
Duration |
Key Findings |
|
Women's Health Initiative (WHI) RCT |
36,282 post-menopausal women |
Ca 1,000 mg + Vit D 400 IU vs placebo |
7 years |
17% increased kidney stone risk in supplement group (HR 1.17) |
|
EPIC-Norfolk Cohort |
25,639 adults |
Dietary and supplement Ca assessment |
8.5 years |
Supplement use but not dietary Ca associated with elevated stone risk |
|
Health Professionals Follow-Up Study |
45,619 men |
Dietary Ca intake quartiles |
6 years |
Highest dietary Ca quartile had 34% lower stone risk |
|
Nurses' Health Study I |
91,731 women |
Dietary Ca quintiles |
12 years |
High dietary Ca inversely associated with stone formation |
|
RECORD Trial |
5,292 elderly |
Ca 1,000 mg ± Vit D vs placebo |
24–62 months |
No significant increase in stone risk; underpowered for this endpoint |
|
Curhan et al. Meta-analysis 2012 |
3 prospective cohorts |
Pooled dietary and supplement analysis |
Variable |
Supplement Ca raised stone risk (RR 1.20); dietary Ca protective |
|
Borghi et al. RCT |
120 men, recurrent stones |
Low Ca vs normal Ca + low oxalate/protein |
5 years |
Normal dietary Ca diet significantly reduced stone recurrence |
|
USPSTF 2018 Evidence Review |
Systematic review |
All supplement types and doses |
Varied |
Confirmed modest but consistent increased stone risk with supplements |
WHI = Women's Health Initiative; EPIC = European Prospective Investigation into Cancer and Nutrition; RCT = randomized controlled trial; HR = hazard ratio; RR = relative risk.
7.3 Meta-Analyses and Systematic Reviews
Several high-quality systematic reviews and meta-analyses have synthesized the available evidence. A pooled analysis by Curhan and colleagues integrated data from three large prospective cohorts and confirmed the directionally opposing associations of dietary calcium (protective, risk reduction approximately 30–40%) and supplemental calcium (harmful, risk increase approximately 15–25%) with stone formation, after adjustment for total fluid intake, protein, sodium, and other dietary variables [85]. The biological plausibility and consistency across studies strengthen the causal interpretation.
The United States Preventive Services Task Force (USPSTF) conducted a systematic evidence review in 2018 examining the harms of calcium supplementation, which confirmed kidney stone risk as one of the most consistent and clinically relevant adverse effects of supplemental calcium [86]. The review concluded that the evidence was sufficient to recommend against daily supplementation with calcium and vitamin D in doses of 400 IU or less in post-menopausal women for primary prevention of cancer and cardiovascular disease, noting that stone risk was a contributing safety consideration.
A meta-analysis by Wallace and colleagues examined the differential effects of calcium from supplements versus food sources on kidney stone risk across 20 studies [87]. Their analysis confirmed that supplemental calcium was associated with a pooled relative risk of approximately 1.20 for kidney stone formation (95% CI 1.04–1.38), while dietary calcium was associated with a significant risk reduction. Importantly, heterogeneity analyses revealed that the degree of risk increase was substantially influenced by baseline urinary calcium excretion, supplement dose, and vitamin D co-administration, underscoring the importance of individual risk stratification.
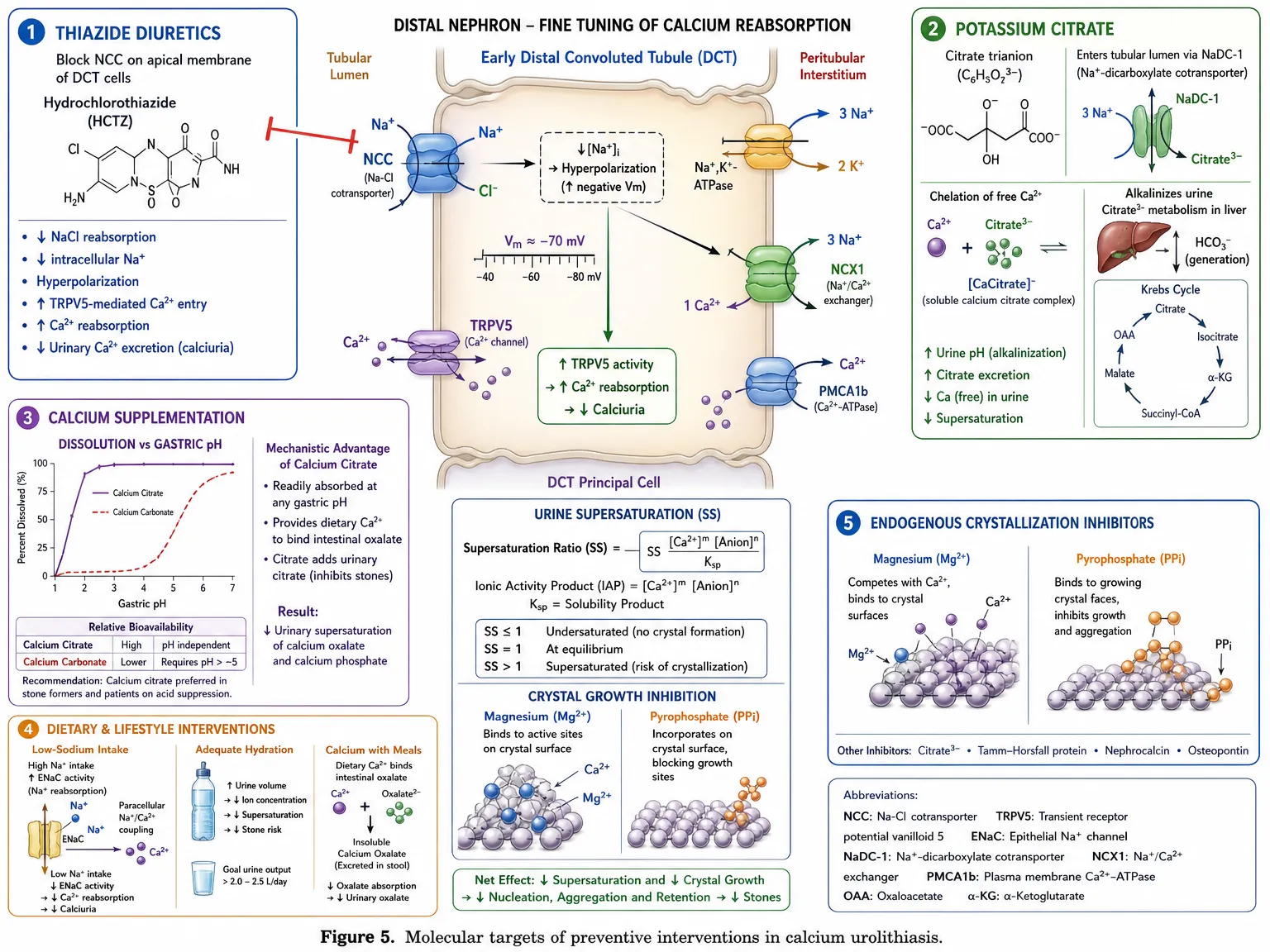
Figure 5. Molecular targets of preventive interventions in calcium urolithiasis: thiazide-mediated NCC blockade, potassium citrate chelation and alkalinization, calcium citrate bioavailability, dietary/hydration optimization, and endogenous crystal inhibitors (Mg²⁺, pyrophosphate).
The dose-response relationship between calcium supplement intake and urinary calcium excretion provides a rational basis for dose minimization as a primary risk reduction strategy. Available evidence suggests that doses above 600 mg elemental calcium per single administration produce disproportionate calciuresis relative to skeletal benefit, as the saturation of transcellular absorptive mechanisms at moderate doses means that a greater proportion of higher doses is absorbed via the paracellular route and subsequently excreted renally [27, 60]. Clinicians should therefore prescribe the minimum effective dose necessary to bridge the gap between dietary calcium intake and recommended daily targets, and should account for dietary calcium intake in dose calculations rather than prescribing supplementation as additive to an already adequate diet [88].
Where total calcium needs are 1,000–1,200 mg/day and dietary intake provides 600–800 mg/day, the supplemental dose required is only 200–600 mg/day—substantially below the 1,000–1,200 mg doses commonly prescribed or self-administered. Splitting doses into two administrations of 500 mg or less, rather than a single daily dose, further reduces peak urinary calcium excretion and is recommended as standard practice in high-risk patients [89].
8.2 Supplement Timing and Formulation Selection
The timing of calcium supplement ingestion relative to meals is the single most impactful and readily implemented behavioral modification for stone risk reduction. Multiple studies have demonstrated that calcium carbonate taken with meals reduces urinary oxalate through intestinal binding—an effect that partially offsets the calciuric effect of the absorbed calcium—whereas the same dose taken in the fasting state produces pure calciuresis without oxalate benefit [11, 90]. Patients should therefore be explicitly instructed to take calcium supplements with food rather than on an empty stomach, and this advice should be prominently embedded in prescribing information and patient education materials.
Formulation selection also influences lithogenic risk, albeit to a smaller degree than timing. In patients with reduced gastric acid secretion—including the elderly and those on chronic PPI therapy—calcium citrate is more completely absorbed than calcium carbonate and may be associated with modestly lower calciuresis [35, 36]. In individuals with a history of calcium phosphate stones or alkaline urine, the carbonate formulation's tendency to alkalinize urine must be considered, and calcium citrate, which increases urinary citrate, may be preferable. Conversely, in individuals with absorptive hypercalciuria and high urinary calcium, both formulations carry significant lithogenic potential, and aggressive dietary calcium optimization should be prioritized over supplementation [91].
8.3 Hydration and Dietary Modification
Maintaining an adequate urine output is the most universally applicable and evidence-supported strategy for reducing stone risk in all patient populations, including calcium supplement users. The dilution of urinary ions by increasing urine volume directly reduces the supersaturation of calcium oxalate and calcium phosphate, reducing the thermodynamic driving force for crystallization. Clinical guidelines from the American Urological Association and European Association of Urology consistently recommend a target urine output of at least 2.0–2.5 L/day, achievable through fluid intakes of approximately 2.5–3.0 L/day in temperate climates [92]. For patients residing in hot climates or with high physical activity levels, fluid needs are correspondingly higher.
Dietary sodium restriction is among the most evidence-supported dietary modifications for calciuric stone prevention. As noted, every 100 mmol increment in urinary sodium is associated with a 25–40 mg increase in urinary calcium through shared renal tubular handling mechanisms [76]. Reducing sodium intake to below 2,300 mg/day—and to below 1,500 mg/day in patients with hypercalciuria or recurrent stones—reduces urinary calcium through natriuresis attenuation, complementing the dose and timing optimization strategies described above. Dietary animal protein restriction reduces the acid load-mediated calcium leak, increases urinary citrate, and reduces urinary uric acid, providing a multifactorial benefit in stone prevention [77, 93].
Potassium citrate is the most widely used pharmacological intervention for urinary stone prevention and is particularly valuable as an adjunct for calcium supplement users who cannot reduce their supplemental dose due to osteoporosis severity or other compelling indications [58]. Potassium citrate supplementation at doses of 30–60 mEq/day effectively raises urinary citrate, alkalinizes urine to the target range of 6.0–7.0 for calcium oxalate prevention, reduces calcium oxalate supersaturation, and inhibits crystal growth. Several randomized trials have confirmed that potassium citrate reduces stone recurrence rates by approximately 85–90% in calcium oxalate stone formers with hypocitraturia [94]. Importantly, potassium citrate avoids the sodium-linked calciuresis of sodium citrate formulations and provides additional potassium, which is independently associated with reduced stone risk [95].
For patients who cannot tolerate potassium citrate tablets due to gastrointestinal side effects, lemon juice—a rich natural source of citric acid metabolized to citrate—provides a practical dietary alternative, though the dose required to achieve clinically significant citraturia (approximately 125 mL of reconstituted lemon juice providing 5.9 g of citric acid) is substantial [96]. Orange juice and other citrus beverages represent additional citrate sources but introduce the confounding lithogenic variable of fructose, which is independently associated with increased stone risk at high intakes.
9. Clinical Implications and Recommendations
9.1 Pre-Supplementation Assessment
Before initiating calcium supplementation, particularly in patients with one or more risk factors for nephrolithiasis, a targeted pre-assessment provides both clinically valuable baseline data and an opportunity to identify individuals in whom supplementation carries particularly high lithogenic risk [97]. A thorough dietary history—quantifying both calcium-containing food intake and typical fluid consumption—allows calculation of the true supplemental calcium requirement, which in many individuals is substantially lower than the full recommended daily intake. Serum calcium, phosphate, PTH, and 25-hydroxyvitamin D concentrations provide information about the underlying hormonal calcium regulatory status.
In patients with a prior history of kidney stones, a 24-hour urine collection including calcium, oxalate, citrate, uric acid, sodium, potassium, magnesium, phosphate, pH, and volume provides comprehensive lithogenic risk profiling before any supplemental calcium intervention [98]. Identifying pre-existing hypercalciuria, hypocitraturia, or hyperoxaluria allows targeted preventive strategies to be implemented concurrently with supplementation initiation, substantially reducing the incremental lithogenic risk. In the general population without stone history, a simpler assessment including dietary history, fluid intake habits, and spot urine calcium-to-creatinine ratio provides reasonable risk stratification without the full metabolic evaluation.
Table 4. Evidence-Based Strategies to Minimize Kidney Stone Risk in Calcium Supplement Users
|
Strategy |
Recommendation |
Rationale |
|
Dose optimization |
Limit elemental Ca from supplements to ≤500–600 mg per dose; total ≤1,000–1,200 mg/day including diet |
Reduces peak urinary Ca excretion |
|
Meal-time dosing |
Take Ca supplements with meals, never on an empty stomach |
Binds dietary oxalate; reduces free oxalate absorption |
|
Adequate hydration |
Maintain urine output ≥2 L/day; target urine specific gravity <1.010 |
Dilutes all lithogenic ions; primary prevention strategy |
|
Dietary sodium restriction |
Reduce Na intake to <2,300 mg/day (ideally <1,500 mg/day in high-risk) |
Attenuates calciuresis driven by natriuresis |
|
Moderate protein intake |
Restrict animal protein to ≤0.8–1.0 g/kg/day |
Reduces acid load and uric acid; increases urinary citrate |
|
Citrate supplementation |
Potassium citrate 20–30 mEq twice daily in stone formers |
Raises urinary citrate; alkalinizes urine; inhibits crystal growth |
|
Prefer calcium citrate |
Use calcium citrate over carbonate in patients with achlorhydria or on PPIs |
Better absorbed without gastric acid; similar oxalate binding |
|
Baseline 24-hour urine |
Obtain 24-hour urine collection before initiating supplements in high-risk patients |
Identifies pre-existing hypercalciuria, low citrate, or high oxalate |
|
Annual monitoring |
Repeat 24-hour urine or spot urine Ca:creatinine ratio annually in supplement users |
Early detection of evolving lithogenic risk |
|
Consider vitamin D co-optimization |
Target 25-OH vitamin D 30–50 ng/mL; avoid supraphysiologic doses |
Excess vitamin D amplifies intestinal Ca absorption |
|
Patient education |
Counsel patients that supplements differ from dietary calcium in stone risk |
Improves adherence to preventive behaviors |
|
Dietary calcium preference |
Encourage meeting Ca needs through food when possible |
Dietary Ca is protective; slows GI transit differently from supplements |
Ca = calcium; CKD = chronic kidney disease; PPI = proton pump inhibitor; CaSR = calcium-sensing receptor.
Post-menopausal women represent the group at highest clinical intersection of calcium supplementation need and kidney stone risk. The withdrawal of estrogen at menopause reduces renal calcium conservation, increases bone resorption-driven calcium release, and shifts the overall calcium balance in a direction that increases urinary calcium excretion [99]. When this baseline increase in calciuric tendency is compounded by supplemental calcium, the lithogenic risk is amplified. Individualized supplementation guided by dietary calcium assessment, 24-hour urine profiling, and the lowest effective dose, together with consistent meal-time administration, is particularly important in this population.
Elderly patients—particularly those over 70—present distinct pharmacological considerations for calcium supplementation and stone risk. Age-related reductions in glomerular filtration rate mean that the renal capacity to clear calcium loads is reduced; a given supplemental dose produces higher peak urinary calcium concentrations than in younger adults with the same dose [100]. Reduced gastric acid secretion favours calcium citrate over carbonate. Concurrent polypharmacy may include loop diuretics (which increase calciuresis) or thiazide diuretics (which reduce calciuresis, partially protective against calcium stones). Careful individualization of supplementation regimens in older patients, with attention to fluid intake—often inadequately low in this population—is of paramount importance.
Patients with inflammatory bowel disease (IBD), bariatric surgery recipients, and others with chronic malabsorptive conditions require careful balancing of their substantially elevated calcium supplementation needs against their also-elevated kidney stone risk. Fat malabsorption promotes oxalate hyperabsorption through saponification of luminal calcium (reducing free calcium available for oxalate binding), generating enteric hyperoxaluria that potently increases calcium oxalate supersaturation [101]. In these patients, calcium supplements taken strictly with meals serve the dual purpose of replenishing systemic calcium and binding intestinal oxalate. Low-oxalate dietary advice, adequate hydration, and potassium citrate supplementation are additional essential components of stone prevention management.
Despite the considerable progress in understanding the mechanisms and risk factors linking calcium supplementation to nephrolithiasis, several important scientific and clinical questions remain incompletely addressed. The role of the gut microbiome in modulating urinary oxalate—through the capacity of Oxalobacter formigenes and other oxalate-degrading bacteria to reduce intestinal oxalate absorption—represents a particularly promising area of investigation. Evidence suggests that colonization with O. formigenes is inversely associated with calcium oxalate stone risk, and that alterations in microbiome composition following antibiotic exposure or dietary change may influence the lithogenic risk profile of calcium supplement users through modifications in enteric oxalate handling [102, 103].
Pharmacogenomic investigation of calcium stone susceptibility genes—including VDR, CaSR, SLC26A6, SLC34A3 (encoding the sodium-phosphate cotransporter), and CLDN14 (encoding claudin-14, a tight junction protein that regulates paracellular calcium permeability in the kidney)—may eventually allow identification of individuals at heightened risk for supplement-induced nephrolithiasis before calcium is prescribed [104]. Pre-supplementation genetic screening, while not currently standard practice, could represent a future tool for personalizing supplementation strategies and monitoring intensity in high-risk genotypes.
From a clinical trial perspective, there is a notable absence of long-term, adequately powered randomized controlled trials designed with kidney stone formation as a primary endpoint in calcium supplement users. Most available RCT data derive from trials primarily designed to assess skeletal or cardiovascular outcomes, with stone events captured as secondary or adverse event endpoints. A dedicated stone prevention RCT comparing different supplementation strategies—varying dose, timing, formulation, and co-supplementation with potassium citrate—in well-characterized high-risk populations would provide the definitive evidence base currently lacking [105].
The growing availability of wearable sensors and continuous urinary monitoring devices offers exciting future possibilities for real-time tracking of urinary calcium, pH, and estimated supersaturation in supplement users, enabling personalized dynamic dosing adjustments and timely identification of evolving lithogenic risk. Telemedicine platforms integrating dietary tracking, hydration monitoring, and periodic urinary analysis into stone prevention management represent an emerging translational opportunity to reduce the population-level burden of supplement-induced nephrolithiasis [106].
Finally, the development of novel calcium salt formulations with optimized intestinal oxalate-binding properties, sustained-release kinetics designed to minimize peak calciuresis, and calcium-sensing receptor-modulating adjuncts represent promising pharmaceutical approaches to decoupling the skeletal benefits of calcium supplementation from its urinary lithogenic consequences. Research into the differential absorptive and renal effects of calcium chelated with various organic anions—beyond the currently available citrate, gluconate, and lactate salts—may yield formulations with superior safety profiles for stone-prone individuals [107].
CONCLUSION
The relationship between calcium supplementation and kidney stone disease represents a clinically significant but preventable risk that demands careful consideration in the management of patients with osteoporosis, nutritional deficiency, and other calcium-replete conditions. The mechanistic divergence between supplemental and dietary calcium—rooted principally in the differential timing of calcium delivery relative to oxalate-containing food and the resultant contrasting effects on urinary oxalate and calcium excretion—explains why supplemental calcium increases stone risk while dietary calcium is protective or neutral. This mechanistic insight is now robustly supported by large-scale epidemiological data, the findings of the Women's Health Initiative trial, and multiple meta-analyses.
The lithogenic risk of calcium supplementation is not uniform; it is shaped by dose, formulation, administration timing, vitamin D co-supplementation, genetic determinants of intestinal and renal calcium handling, concurrent dietary habits, hydration status, and the presence of underlying metabolic abnormalities including absorptive hypercalciuria, hypocitraturia, and hyperoxaluria. Each of these determinants is amenable to clinical assessment and modification, providing a robust toolkit for risk minimization that does not require abandonment of supplementation in patients with genuine skeletal need.
The cornerstone strategies—meal-time supplement administration, dose minimization to the true dietary gap, preference for calcium citrate in high-risk individuals, maintenance of urine output exceeding 2 L/day, dietary sodium and protein restriction, and potassium citrate co-administration in stone-prone patients—are individually evidence-supported and collectively capable of substantially attenuating the lithogenic impact of supplementation. Baseline 24-hour urine profiling and annual monitoring in high-risk patients complete a comprehensive preventive framework that aligns with emerging precision medicine principles.
Ultimately, the goal of balancing skeletal protection against urolithiasis prevention requires individualized clinical assessment rather than population-level prescribing patterns. As our understanding of the pharmacogenomics of calcium metabolism deepens and monitoring technologies continue to evolve, the ability to prescribe calcium supplementation with confidence in its safety profile for each individual patient will continue to improve. In the interim, the evidence reviewed herein provides a sufficiently detailed mechanistic and clinical foundation for clinicians across nephrology, endocrinology, geriatrics, and primary care to navigate this therapeutic balance with precision and confidence.


Vaibhav Rahate, Vaishnavi Mhaske, Calcium Supplementation and Kidney Stone Formation: Mechanisms, Risk Factors, and Clinical Implications A Comprehensive Narrative Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2791-2815, https://doi.org/10.5281/zenodo.21352521
 10.5281/zenodo.21352521
10.5281/zenodo.21352521