
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Womens College of Pharmacy, Peth Vadgaon, Maharashtra, India
Using digital technologies and telecommunications, tele-pharmacy is a contemporary approach to healthcare that allows chemists to provide pharmaceutical care from a distance. It is now a crucial part of healthcare systems, particularly in underserved and rural areas with limited access to chemists. Prescription verification, drug dispensing, patient counselling, pharmaceutical treatment management, and chronic disease monitoring are all provided by tele-pharmacies. Recent advancements in internet connectivity, electronic health records, artificial intelligence, and mobile health applications have accelerated tele-pharmacy adoption worldwide. The COVID-19 pandemic promoted the use of tele-pharmacy techniques worldwide and highlighted the significance of distant healthcare services. Tele-pharmacy presents a number of advantages, including increased patient adherence, cost-effectiveness, accessibility to healthcare, and growth of clinical pharmacy services. Regulatory obstacles, cybersecurity risks, technology constraints, problems with payment, and decreased human interaction are some of the obstacles that still hinder its implementation.
The global delivery of healthcare services has been profoundly altered by digital transformation. Tele-pharmacy, which allows chemists to administer pharmacological care remotely via telecommunications technology, is one of the most significant advancements in this profession. Particularly in rural and remote areas, tele-pharmacy has proven to be a successful way to address healthcare inequities brought on by chemist shortages. Tele-pharmacy services have grown as a result of the quick development of cloud computing, smartphones, internet technologies, and electronic health data. Through tele-pharmacy, chemists can offer clinical monitoring, medication counselling, prescription evaluation, and patient education without physically visiting medical facilities.
The global adoption of Tele-Pharmacy was significantly pushed by the COVID-19 epidemic. Tele-Pharmacy reduced the risk of infection while maintaining access to medical care during lockdowns and times of social separation. Tele-Pharmacy is becoming more widely acknowledged by governments and healthcare organizations as a secure and effective way to provide pharmacological care remotely.
Tele-Pharmacy has a number of drawbacks despite its increasing significance, including regulatory restrictions, difficulties with funding, worries about cybersecurity, and problems with patient acceptance. The prospects and difficulties of Tele-Pharmacy are highlighted in this review paper, which also explores potential future paths for its effective application.
Evolution and Development of Tele-Pharmacy:-
In the late 20th century, Tele-Pharmacy emerged as a development of telemedicine. To address the shortage of chemists, early Tele-Pharmacy models were implemented in rural healthcare settings. Tele-Pharmacy services were originally introduced in rural healthcare systems in nations like the United States, Canada, Australia, and the United Kingdom.
Tele-Pharmacy procedures were greatly enhanced by technological developments such as video conferencing, electronic prescribing systems, mobile communication, and high-speed internet. Over the past 20 years, Tele-Pharmacy-related research publications have grown significantly, especially following the COVID-19 epidemic. Between 1981 and 2023, Tele-Pharmacy research significantly increased, according to a bibliometric analysis based on data.
HOW DOES TELE-PHARMACY WORK ?
Generally speaking, a tiny rural hospital, pharmacy, or clinic in a remote location is linked to a widely used service model in a bigger urban center that has more access to pharmacist staff, frequently around-the-clock. Videophone systems,(44) innovative software, and automated dispensing machines enable this connection. One Depending on whether the location is a clinic or a drugstore, the rural site is typically manned by nurses or pharmacy technicians. Patients who visit these locations may fax their prescriptions to the central facility, where a licensed chemist processes them. After reviewing the prescription, the central chemist releases the necessary supplies (such as prepackaged medication from automated dispensing devices) and the label at the rural location.(44)
After scanning the bar code to make sure the prescription and its label match, the pharmacy technician or nurse in the remote location adds the label and gives the patient the medication. To make sure that the correct prescriptions have been filled and dispensed, the pharmacist at the central end can visually watch the technician's or nurse's work(44). To make sure the patient understands how the drug is supposed to be used and administered, the central chemist offers a two-way video consultation at the conclusion of the procedure.15. This allows for effective patient counselling from a central location and answers any concerns raised by the patient.
However, tiny rural clinics or hospitals may not always be able to afford automated dispensing machines. An alternative was created by researchers in Fargo, ND, USA, where a technician prepares medication for dispensing, repackaging, and relabelling while being supervised via videoconference by a central chemist at a remote site.15. The pharmacy technician then delivers these drugs straight to the nurse or, if automated dispensing systems are available, dispenses them. In another instance, a wireless mobile technology cart has been created for use in rural hospitals to enable doctors and nurses in the patient care area to have 24-hour access to the chemist for in-person consultation and(44) conversation.15 The several Tele-Pharmacy model types are given below :-
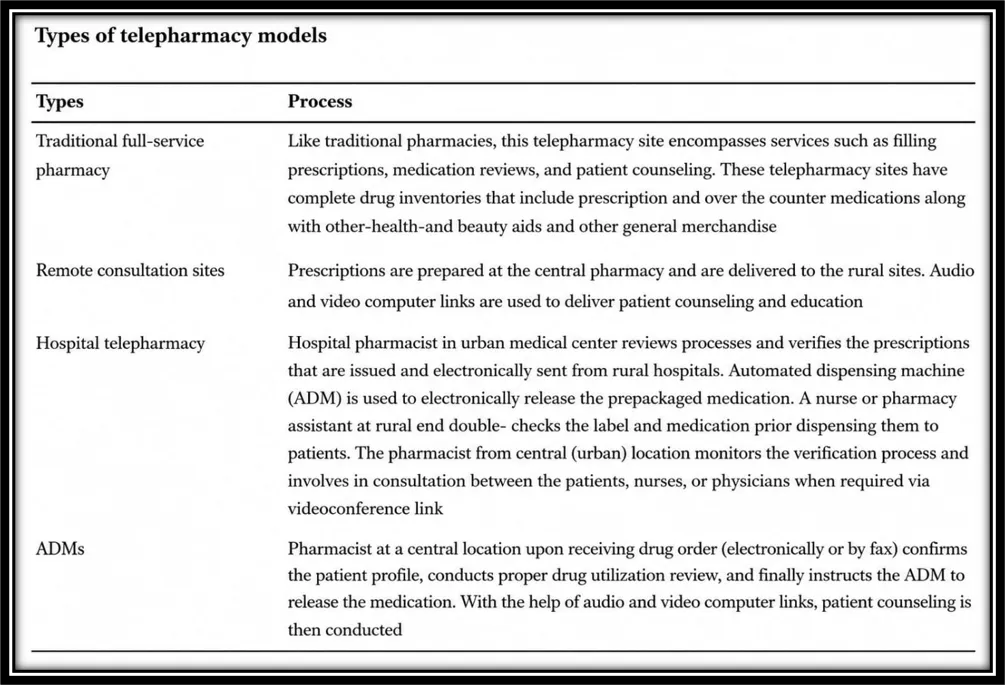
Fig no1 :-TYPES OF TELE-PHARMACY MODEL
Types of Tele Pharmacy
1. Remote Dispensing Tele-Pharmacy:
Digital communication systems are used to deliver medications at remote healthcare locations under the supervision of chemists.
2. Clinical Tele-Pharmacy :-
Clinical chemists offer remote disease monitoring, drug evaluation, and medication therapy management.
3. Hospital Tele-Pharmacy :-
Tele-Pharmacy is used by hospitals for clinical monitoring, acute care support, and drug order verification.
4. Community Tele-Pharmacy : -
Virtual counselling and prescription management services are offered by community pharmacists.
5. Home-based Tele-Pharmacy :-
Through mobile applications and telecommunication platforms, patients can access pharmaceutical care services from the comfort of their own homes.
COMPARATIVE ANALYSIS OF TELE-PHARMACY PRACTICES ACROSS COUNTRIES :-
A cross-national analysis of Tele-Pharmacy practices identified parallels and discrepancies influenced by healthcare requirements, technology developments, and regulatory frameworks.
Despite recommendations from the National Association of Boards of Pharmacy, telepharmacies in the US are subject to a thorough regulatory framework with state-level differences because of regulatory autonomy. Using cutting-edge telecommunication technologies and electronic health records (EHR) for prescription services are examples of innovations.
Regulatory disparities between states and problems with reimbursement are obstacles that affect uniform adoption.
With province-specific laws and national standards established by the Pharmacy Examining Board of Canada, the Canadian method is similar to that of the US. Tele-Pharmacy mainly provides safe online platforms for prescription management and consultation in remote places.
Connectivity problems in rural areas and their integration with provincial healthcare systems are challenges.
Under the direction of the Australian Pharmacy Board, Australia integrates Tele-Pharmacy into its larger telehealth framework. Mobile apps for medication administration and mobile health units and kiosks for remote pharmaceutical care are examples of creative solutions. Overcoming geographical limitations in remote places and guaranteeing data safety and privacy are challenges.[9] Tele-Pharmacy in the UK is managed by the General Pharmaceutical Council. In order to manage both acute and chronic care, the National Health Service has incorporated Tele-Pharmacy into digital health projects. Providing fair access and managing chemists' workloads are obstacles.With new guidelines from the Pharmacy Council of India, Tele-Pharmacy regulations are being developed in India. Tele-Pharmacy uses online consultation platforms and mobile telemedicine devices to reduce the healthcare gap between urban and rural areas.Digital literacy, infrastructure constraints, and regulatory enforcement are obstacles.According to studies, Indonesia has a favourable opinion of Tele-Pharmacy services and is prepared to employ them because of changes brought about by the epidemic.
During COVID-19, Tele-Pharmacy services in the Republic of Srpska, Bosnia, and Herzegovina grew to meet the demands of both COVID-19 and non-COVID-19 patients, demonstrating the flexibility of chemists.[8]
Despite their lack of experience, community chemists in Saudi Arabia have embraced Tele-Pharmacy's introduction during Covid-19. Positive attitudes and adoption readiness point to the possibility of wider implementation, provided that knowledge gaps are filled.
Numerous nations have adopted Tele-Pharmacy methods, customising them to fit their distinct healthcare environments. While countries like India and Indonesia are in the early phases of developing solutions to address healthcare demands, the US and Canada place a strong emphasis on technological integration. Aligning rules, building a technology infrastructure, and guaranteeing equitable access are common challenges. The positive outcomes seen in several areas during the COVID-19 crisis suggest that international collaboration and knowledge sharing could enhance telepharmacies' efficacy globally.
Equal accessibility, technology underpinnings, and regulatory standardisation are common obstacles. International collaboration could increase Tele-Pharmacy's worldwide influence, as evidenced by the favourable results observed in a variety of regions during the coronavirus epidemic.
BARRIERS TO ADOPTION OF TELE-PHARMACY IN HIGH-INCOME COUNTRIES
Even though Tele-Pharmacy has the potential to improve healthcare delivery systems, there are many barriers to its adoption in developed countries. These difficulties include financial disincentives, workforce concerns, technology barriers, and legal and regulatory constraints.
1. Regulatory and legal challenges:-
The absence of consistent regulations across regions is a significant obstacle. State-by-state variations in Tele-Pharmacy regulations in the US cause confusion and hinder the deployment of standardised services. The necessity for harmonised state-specific rules is highlighted by this diversity, which makes uniform care more difficult, especially when patients and providers are located in multiple jurisdictions.
The difficult licensing and credentialing procedures for chemists wishing to practise Tele-Pharmacy across state lines present another challenge. Pharmacists are discouraged from growing their services by these disjointed processes.
2.Technological barriers :-
Even while high-income nations typically take pride in their sophisticated technology infrastructure, problems nevertheless exist, especially with regard to data security and privacy. One major issue that can erode confidence in Tele-Pharmacy systems is protecting private health information from online threats.Furthermore, enabling seamless connectivity between Tele-Pharmacy platforms and current EHRs has technical challenges that may interfere with data integration and care continuity.
3. Workforce and professional resistance:-
Because they prefer traditional face-to-face connection, healthcare professionals may be resistant to Tele-Pharmacy. Unfamiliarity with digital platforms or worries about sustaining virtual patient interactions could be the cause of this hesitancy. Additionally, there were notable deficiencies in the abilities and training.To guarantee that chemists and allied staff are properly prepared to provide Tele-Pharmacy services, extensive educational programs are required. Improving service delivery and professional acceptance require addressing these skill gaps
4. Economic and reimbursement challenges:-
Healthcare providers face financial obstacles due to unclear reimbursement structures for Tele-Pharmacy services. Healthcare providers can be deterred from implementing Tele-Pharmacy in their practices in the absence of clear pay plans.[13,18] Additionally, the high upfront expenses of setting up Tele-Pharmacy infrastructure, including as staff training and technology purchases, might be unaffordable, particularly for smaller practices or those in remote locations.Rich countries need to improve cybersecurity, create standard legislation, and encourage professional acceptability through focused training programs in order to get past these obstacles .Additionally, for Tele-Pharmacy services to be successfully integrated into healthcare systems, legislators, healthcare providers, and technology developers must work together to solve economic issues and provide clear reimbursement schemes.
BARRIERS TO ADOPTION OF TELE-PHARMACY IN LMICS
There are many challenges in implementing Tele-Pharmacy in LMICs. The technological, financial, regulatory, labour, and cultural issues are all included in these challenges. After a thorough investigation, the following was discovered:
1. Technological infrastructure :-
Inadequate technology infrastructure, especially erratic internet availability in rural and isolated areas, is a significant barrier to Tele-Pharmacy adoption in LMICs. The regular delivery of Tele-Pharmacy services is hampered by this restriction. Due in part to limited access to technology, research conducted in Indonesia revealed that older people and those with less education have significant knowledge gaps in Tele-Pharmacy.
2. Regulatory and policy hurdles :-
The absence of thorough regulatory frameworks for Tele-Pharmacy in many LMICs leads to uncertainty and hinders the expansion of these services. Research has shown that more accommodating Tele-Pharmacy regulations can lessen pharmacy deserts, indicating that regulatory support is necessary for integration to be successful.
3. Financial limitations :-
Healthcare organisations and governments in LMICs face budgetary challenges due to the costs of setting up Tele-Pharmacy systems. The transition from traditional pharmaceutical services to digital platforms is made more difficult by the lack of funding and financial incentives.
4. Workforce constraints :-
LMICs frequently struggle with a lack of qualified medical personnel, especially chemists who are adept at providing Tele-Pharmacy services. To use telehealth technology efficiently, current employees might need additional training.
According to research, chemists' expertise and training have a big impact on how prepared they are to use Tele-Pharmacy.
5. Digital literacy :-
Tele-Pharmacy adoption may be hampered by patients' and healthcare practitioners' low levels of digital literacy. This is demonstrated by research conducted in Malaysia and Indonesia, where a lack of knowledge and comprehension of Tele-Pharmacy was common despite high levels of digital preparedness.
6. Cultural and social aspects :-
In certain LMICs, Tele-Pharmacy acceptance may be impacted by cultural preferences for face-to-face interactions and doubts about the effectiveness of distant care. Jordanian patients' opinions show that Tele-Pharmacy must be seen as a good substitute for conventional services, especially when it comes to cutting down on pointless pharmacy visits.
7. Data privacy and security issues :-
In LMICs, where strong cybersecurity safeguards are lacking, protecting patient data security and privacy is a major concern. Participation in Tele-Pharmacy services is discouraged by worries about safeguarding private health information.[8]
A holistic approach is needed to overcome these challenges, including community involvement to increase digital skills and acceptance, training for medical personnel, supportive policies, and infrastructure investment. By working together, governments, medical facilities, and international partners can get beyond these obstacles and enable LMICs to fully benefit from Tele-Pharmacy. Some countries have successfully implemented Tele-Pharmacy in settings with limited resources, demonstrating the model's potential to improve access to healthcare
Involvement of Pharmacist :-
Pharmacists can actively participate in the provision of pharmacy services in any Tele-Pharmacy paradigm. In Tele-Pharmacy models, the pharmacist guarantees the community receives high-quality treatment, especially in areas like prescription reviews and patient counselling. According to a 2013 study on the effects of Tele-Pharmacy services, fewer adverse drug events were documented when (44)chemists participated in the remote evaluation of medicine orders during hospital pharmacy closures. Every year, thousands of deaths are caused by adverse drug events and other prescription errors.
In the USA alone, avoidable adverse medication events are thought to cost US$2 billion annually. In a similar vein, a 2012 US study revealed that Tele-Pharmacy services, as prospective substitutes for round-the-clock on-site pharmacist prescription review for rural hospitals, may have reduced undesirable patient outcomes, such as extended hospital stays and possible death.
Involving chemists in Tele-Pharmacy models to enhance monitoring and promote medication compliance can lower the risk of medication errors, adverse drug events, lower medication costs, and treatment failure due to the increasing number of patients with chronic medical conditions worldwide. This means that some Tele-Pharmacy models, such as Internet pharmacies, vending machine models, mail-order pharmacies, and models that transfer pharmacists' responsibilities to other medical professionals like doctors and nurses, should be avoided since they frequently exclude active pharmacist involvement.
Tele-Pharmacy approaches incorporating the active engagement of chemists are successful in a number of US states and Australia, despite the disparities in healthcare systems among nations. About half of chemists in rural and isolated Australian regions said they would be open to conducting home medication reviews (HMR) utilising Tele-Pharmacy models in a 2005 Australian survey.
Rural and distant populations that would typically need a visiting chemist to perform this review could benefit greatly from HMR through Tele-Pharmacy. The position of a chemist as the primary healthcare provider in the provision of pharmacy services is included in and maintained by Tele-Pharmacy models in the United States, particularly in North Dakota. Other Tele-Pharmacy models that do not employ chemists frequently lack this value-added quality assurance function, which means that there is no formal drug utilisation review or patient counselling.
According to an American study, chemists' participation in Tele-Pharmacy models has helped monitor and reduce drug mistake rates. The models indicated a tendency toward better prescription documentation, lower drug risk, and an achievable minimal standard of pharmaceutical review, and they proved to be a useful tool at sites that had no pharmacy inputs before. The number of orders that a remote pharmacist evaluated, changed, terminated, or cancelled, the time it took to process orders, and the money saved were further indicators of the effect of pharmacist engagement.
Clinical benefits and challenges of Tele-Pharmacy :-
ADVANTAGES :-
1. Access to healthcare services :-
The ease of access to medical treatments in isolated and rural areas is the main benefit of Tele-Pharmacy. In remote and rural areas, regular access to prescription drugs and chemists are acknowledged as essential components of patient-centered healthcare delivery.2 Pharmacists can offer advanced pharmaceutical care services in isolated locations when access to medical care is either nonexistent or rapidly diminishing.
Ninety percent of the 410 small rural hospitals in the United States stated that nurses were in charge of dispensing and administering medications, and around half of the hospitals reported having a chemist on site (less than five hours per week).21, 22 In order to address this situation, a number of Tele-Pharmacy models were developed. These models enable full-service operation, which includes drug utilisation evaluation, patient counselling, patient education, and the active engagement of central and remote chemists utilising a variety of technologies.
2.Economic benefits :-
Tele-Pharmacy offers a number of financial advantages. According to reports, opening a new pharmacy is far more expensive than purchasing equipment and hiring pharmacy technicians for Tele-Pharmacy. Multiple locations can be served by a single competent chemist. Therefore, expenditures are kept to a minimum by taking into account the growing pay scale for chemists and the additional costs associated with recruiting more chemists for rural locations. More than 60% of patients would have had trouble paying for their prescription drugs in the absence of a Tele-Pharmacy strategy aimed at the low-income population.14 Garrelts et al.'s study of Tele-Pharmacy's effects in a multihospital health system revealed a net anticipated annual savings of US$1,132,144.
Conversely, Tele-Pharmacy reduces travel time and costs, which are significant obstacles for elderly and disabled veterans living in remote areas.24 In Connecticut, USA, a Tele-Pharmacy program that provided pharmaceutical therapy management services to 96 senior patients managed to save ₹S$300,000.25. When chemists are not on site, Tele-Pharmacy is a great way for healthcare practitioners to avoid treatment delays. When patients are not directed to other locations, travel time and other related expenses are avoided.
3. Patient satisfaction :-
Patient satisfaction is a benefit of telemedicine medication availability and information in rural places. The elderly patients' refusal to leave their homes for their checkups used to be one of the main obstacles in the clinic. Pharmacists can now check patients' prescriptions remotely without needing to travel.
Patient satisfaction and trust have grown as a result of this.25. Rural community patients prefer receiving pharmacy services locally via Tele-Pharmacy services rather than having to travel outside of their community, according to a US study to determine the underlying factors determining patient satisfaction depending on healthcare delivery mode or community-specific factors.27. More than 75% of the patients in a similar research conducted in the USA to assess the Tele-Pharmacy program expressed satisfaction with the videoconference service and communication with the chemist.14. According to a study on patient surveys conducted in Queensland, Australia, patients are rather pleased with the Tele-Pharmacy services they received.
4.Effective patient counseling :-
Patients are more satisfied with Tele-Pharmacy when it comes to pharmacist counselling and the time it takes to get medicine..Pharmacists advise adopting webcam-enabled Tele-Pharmacy services because they offer greater privacy and lengthier counselling sessions, according to a study on Tele-Pharmacy-related services and outcomes in the USA. Another study demonstrated the efficacy of Tele-Pharmacy counselling by explaining metered-dose inhaler techniques through compressed video rather than typical package insert training.
Skoy et al. investigated how well students could counsel patients using Tele-Pharmacy and looked at any discrepancies between Tele-Pharmacy and in-person consultation. According to their findings, students who have never used Tele-Pharmacy technology before may effectively consult with patients.31. Nevertheless, the study also showed that students performed better during the in-person consultation, indicating the need for more Tele-Pharmacy consultation training and practice.
5.Minimal scarcity of pharmacists :-
The lack of local pharmacy services, which provide medications without a chemist's involvement, is currently a problem for several hospitals, clinics, and medical facilities in remote areas.32, 33 The majority of pharmacy services are transferred to nurses, physicians, and other healthcare professionals who might not have received training in proper medication administration when chemists are unavailable in rural and isolated locations. This situation may have produced an unsatisfactory system that does not adhere to government regulations for the supply of high-quality pharmaceutical services to all individuals. These problems may be resolved using Tele-Pharmacy.
The pharmacy profession will soon play a significant role in Tele-Pharmacy trials. One practical solution to these transfers from the pharmacy profession to other professions is a remote Tele-Pharmacy service. Therefore, Tele-Pharmacy enhances patient access to medications and pharmacy services while addressing the shortage of pharmacists in remote locations.
A study conducted in Queensland, Australia, in 2010 revealed that Tele-Pharmacy models may be successfully implemented to give patients in rural hospitals pharmacist medication reviews.19. Later in 2013, clinical pharmacy services could be provided in isolated and rural areas of Queensland thanks to government financing. Hospital Tele-Pharmacy networks offer a cost-effective, practical, and adaptable answer to the staffing demands of chemists at tiny rural hospitals. Tele-Pharmacy facilitates staff coverage for after-hours, weekend, vacation and emergency situations, as well as challenging scheduling times when pharmacist substitutes and relief assistance might not be easily accessible.
DISADVANTAGES :-
1.Pharmacy regulation laws :-
Despite the widespread potential of Tele-Pharmacy, the laws and policies governing pharmacy operations do not sufficiently address the expanding industry. A number of policy issues need to be addressed, including the physical location of pharmacists who provide Tele-Pharmacy services, the minimum amount of time that pharmacists must be on site, the types of technology used, and the roles of pharmacists, pharmacy technicians, nurses, or other healthcare providers in medication distribution systems.
Despite the utilisation of professional and technological improvements, Tele-Pharmacy is still a relatively new idea, and new legislation are being implemented slowly. There is a lack of consistency across different jurisdictions in areas with Tele-Pharmacy laws. It is currently difficult to execute and apply a complete and standard Tele-Pharmacy law.
2.Operational difficulties :-
Unquestionably, Tele-Pharmacy is a fantastic idea, but it can be difficult to implement at times. Rural clinics and hospitals that offer Tele-Pharmacy services have resource and operational difficulties. There are resource and operational issues with Tele-Pharmacy services. Only more advanced and sophisticated equipment with high-speed digital connections (such as an Integrated Service Digital Network)—which are frequently scarce in rural areas—may be able to provide Tele-Pharmacy services.
Incorporating and integrating Tele-Pharmacy technologies into current healthcare systems can also be significantly hampered by organisational cultures.2 Both patients and healthcare practitioners may find face-to-face vs virtual workflow to be overwhelming and less impromptu. According to a study on tele healthcare normalisation (the regular integration of programs in daily practice), the development of a supportive organisational structure, the expansion of new procedures by professionals, the involvement of organised, cohesive groups, and a positive relationship with a policy level sponsor are all necessary for the successful normalisation of telehealthcare services.
Even while Tele-Pharmacy is effectively incorporated into standard healthcare in the United States, complications at these levels are typically underestimated, which prevents telehealth programs from becoming mainstream health services.
For rural and isolated hospitals, Tele-Pharmacy necessitates considerable changes to the current process, which may be difficult for some facilities to implement.11 When a single pharmacist manages multiple distant pharmacy locations, there is a problem with increased workload. Additionally, if the pharmacy law calls for a monthly on-site visit, this may entail time-consuming travel obligations to the remote locations.
3.More time, effort, and money :-
It takes a lot of time, money, and effort to start up a Tele-Pharmacy (technology, software, connectivity, and operating costs). The anticipated approximate cost of the North Dakota Tele-Pharmacy project is $20,000 for drug store furnishings, between $60,000 and $80,000 for medicine inventory, and $20,000 for digital subscriber lines. US$800 per month, hardware: US$2,000, pharmacy operation software: US$5,000–7,000, videoconference setup: US$6,500, videoconference equipment: US$3,500–15,000, transmission/connectivity: US$250 per month, firewall security systems: US$1,200, and other various expenses) for the successful Tele-Pharmacy model.1 However, this cost estimate is based on a study conducted in 2004.
It is anticipated that the actual cost will rise several times. Furthermore, in nations that use Tele-Pharmacy services, Tele-Pharmacy systems have not been integrated with traditional healthcare systems. Because of this, government and private healthcare systems are hesitant to pay for Tele-Pharmacy expenses. For instance, people who presently pay for their health insurance will only receive funding for standard medical expenses; Tele-Pharmacy costs will not be reimbursed. The global expansion of Tele-Pharmacy services necessitates the integration of new healthcare systems. Reviewing the legislation and establishing guidelines for Tele-Pharmacy operations in the upcoming years will be necessary for this integration, which will be a difficult and time-consuming effort.
Furthermore, even though Tele-Pharmacy services have a bright future, chief executive officers in on-site hospitals and remote clinics struggle to pay for Tele-Pharmacy expenses. On the other side, chemists think they can get beyond technological and legal obstacles, but they are unsure if they will be able to pay for this service in the long run. In the end, the cost issue seems to be one of the main obstacles to Tele-Pharmacy services for rural hospitals with fewer patients.
OTHERS :-
Security
Transmitting private and medical information via the Internet is known as Tele-Pharmacy. Information security becomes a worry since controlling this massive data movement is crucial. Only research that respects patient privacy and human rights may use patient data.
Reluctance to use technology :-
Reluctance or incapacity to use the technology is another drawback of Tele-Pharmacy. This is more common among older adults who have misgivings about technology. The chemist may find it more difficult to properly understand the patient's condition in the absence of face-to-face discussion.
Continuity of care :-
When in-person interactions are not feasible, the chemist should offer an ethical indirect supply service that complies with the rules governing the proper use of medications. On remote locations, maintaining continuity of treatment and adhering to proper dispensing practices becomes more difficult. In every facet of pharmacy practice, pharmacy technicians must rely on the pharmacist.Even while chemists oversee or monitor pharmacy technicians from a central location, it is challenging to prevent regulatory violations. Unlike traditional pharmacies, it is difficult to supervise the use of illegal drugs or the delivery of drugs without a valid prescription.
The Future of Tele-Pharmacy :-
Tele-Pharmacy is likely to become a permanent fixture in the pharmacy industry due to the advantages of its use and the usually positive attitude that patients have toward it. The general consensus is that instead than taking the place of in-person care, telemedicine should be used as an auxiliary.
There are still a lot of unanswered concerns about the application and efficacy of Tele-Pharmacy and telemedicine, as well as how these technologies should be used in healthcare.32. One uncertainty is if a significant number of states will participate in a multistate licensing program, as was previously mentioned.65 Other queries include: How will this technology affect trust and the patient-clinician relationship? Will the lack of therapeutic touch and nonverbal communication harm this relationship?
Will certain appointments be replaced by patient-focused mobile applications, as prescription digital therapies are starting to do? Could patient counselling be aided by an AI format such as ChatGPT?. Could a chemist or prescriber take over to finish the encounter, for instance, once an artificial intelligence program initiates an appointment? Will the technician have additional AI capabilities that a chemist may review in a remote Tele-Pharmacy, saving time for discussions?
REFERENCES

Sakshi Powar, Mahek Shikalgar, Siddhi Karande, Pooja Koli, Dr. Dhanraj Jadge, Challenges and Opportunities in Tele Pharmacy, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 56-70. https://doi.org/10.5281/zenodo.20483190
 10.5281/zenodo.20483190
10.5281/zenodo.20483190