
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Womens college of pharmacy, peth vadgaon, Maharashtra, India
Stem cell therapy has emerged as one of the most promising frontiers in regenerative medicine, offering potential treatment strategies for a wide range of degenerative, genetic, inflammatory, and traumatic diseases. The unique properties of stem cells, including self-renewal, differentiation capacity, and paracrine signaling, enable tissue repair and functional restoration beyond the capabilities of conventional therapies. Over the past two decades, extensive preclinical studies and clinical trials have investigated the safety, feasibility, and therapeutic efficacy of various stem cell types, including hematopoietic stem cells, mesenchymal stem cells, embryonic stem cells, and induced pluripotent stem cells. Despite significant advancements, challenges such as immune rejection, tumorigenicity, ethical concerns, variability in clinical outcomes, and regulatory limitations continue to restrict widespread clinical translation. This review provides a comprehensive overview of the current status of clinical trials in stem cell therapy across major disease areas, including cardiovascular disorders, neurological conditions, musculoskeletal injuries, autoimmune diseases, and metabolic disorders. Furthermore, it highlights recent technological innovations and discusses future perspectives focusing on gene-edited stem cells, organoid technology, tissue engineering, and personalized regenerative medicine.
Stem cell therapy has emerged as a revolutionary approach in regenerative medicine due to its unique ability to repair, regenerate, and replace damaged tissues and organs. Stem cells possess two defining biological characteristics: self-renewal and differentiation into specialized cell lineages, making them highly valuable for therapeutic interventions in various degenerative and chronic diseases. Over the past few decades, stem cell–based strategies have gained increasing scientific and clinical attention as potential alternatives to conventional pharmacological and surgical treatments, particularly for diseases where tissue regeneration is limited or irreversible damage occurs [1,2]. The concept of stem cell therapy originated from the successful application of hematopoietic stem cell transplantation for hematological malignancies and inherited blood disorders. Since then, advancements in cellular biology and regenerative medicine have significantly broadened the therapeutic scope of stem cells, extending their applications to neurological disorders, cardiovascular diseases, musculoskeletal degeneration, diabetes, autoimmune conditions, and tissue engineering. Different categories of stem cells, including embryonic stem cells (ESCs), adult stem cells, mesenchymal stem cells (MSCs), hematopoietic stem cells (HSCs), and induced pluripotent stem cells (iPSCs), have been investigated for their regenerative potential and clinical utility [3,4]. Clinical translation of stem cell research has accelerated rapidly, with thousands of clinical trials being conducted worldwide to assess the safety, efficacy, dosing, and long-term outcomes of stem cell–based therapies. Mesenchymal stem cells have attracted particular interest because of their immunomodulatory effects, anti-inflammatory properties, and low immunogenicity, allowing their application in diverse inflammatory and degenerative conditions. Similarly, induced pluripotent stem cells have opened new possibilities in personalized medicine, as they can be generated from adult somatic cells and differentiated into patient-specific tissues, thereby minimizing immune rejection and ethical concerns associated with embryonic stem cells [5,6]. Despite considerable therapeutic promise, stem cell therapy continues to face multiple scientific and translational challenges. Issues related to tumorigenicity, immune incompatibility, ethical concerns, inconsistent clinical outcomes, scalability of manufacturing, and regulatory barriers have limited widespread clinical implementation. Moreover, heterogeneity in stem cell sources, isolation techniques, and administration protocols often contributes to variations in therapeutic effectiveness across clinical studies [7,8]. Recent technological advancements, including gene editing, tissue engineering, biomaterials, artificial intelligence–assisted cell optimization, and organoid technology, are transforming the future landscape of regenerative medicine. These innovations are expected to improve treatment precision, enhance safety profiles, and overcome current limitations in stem cell therapy. Therefore, a comprehensive evaluation of clinical trials and future perspectives of stem cell therapy is essential to understand its current achievements, existing challenges, and emerging opportunities in modern healthcare [9,10].
Classification And Types Of Stem Cells Used In Clinical Therapy
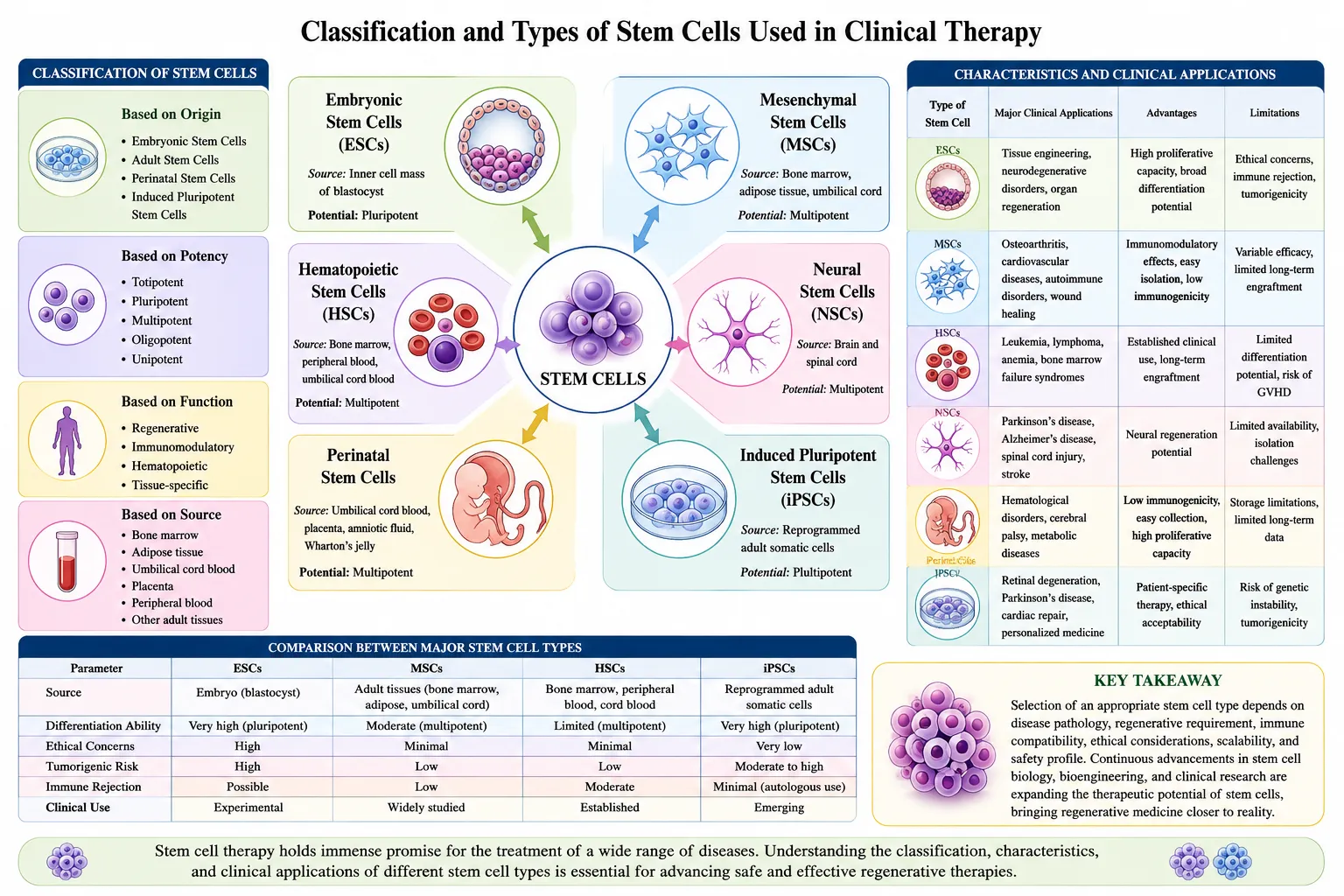
Fig 1.classification and types of stem cell
Stem cells are broadly classified based on their origin, differentiation capacity, and therapeutic applications. Their regenerative potential varies according to their ability to self-renew and differentiate into specialized tissues. Selection of an appropriate stem cell source is a critical factor influencing clinical outcomes, safety, ethical acceptability, and long-term therapeutic efficacy. Stem cells used in clinical trials are generally categorized into embryonic stem cells, adult stem cells, perinatal stem cells, and induced pluripotent stem cells [11,12]. Embryonic stem cells (ESCs) are pluripotent stem cells derived from the inner cell mass of blastocysts and possess the ability to differentiate into almost all cell types of the human body. Due to their unlimited proliferative capacity and broad differentiation potential, ESCs are considered highly promising for regenerative medicine and tissue replacement therapies. However, ethical controversies regarding embryo destruction, immune rejection risks, and tumorigenicity concerns have restricted their widespread clinical application [13]. Adult stem cells, also referred to as somatic stem cells, are multipotent cells found in mature tissues such as bone marrow, adipose tissue, skin, liver, and dental pulp. These cells play an essential role in tissue repair and maintenance. Mesenchymal stem cells (MSCs) and hematopoietic stem cells (HSCs) are among the most extensively studied adult stem cells in clinical trials. MSCs exhibit anti-inflammatory, immunomodulatory, and tissue regenerative capabilities, making them suitable for orthopedic, cardiovascular, and autoimmune disorders. Hematopoietic stem cells remain the gold standard for treating hematological malignancies and bone marrow failure syndromes [14,15]. Perinatal stem cells obtained from umbilical cord blood, placenta, amniotic fluid, and Wharton’s jelly have attracted increasing scientific attention due to their ease of collection, reduced ethical concerns, lower immunogenicity, and higher proliferative potential compared to adult stem cells. Umbilical cord blood stem cells have been successfully used in hematopoietic transplantation and are currently being explored for neurological and metabolic disorders [16]. Induced pluripotent stem cells (iPSCs) represent one of the most significant breakthroughs in regenerative medicine. These cells are generated by reprogramming adult somatic cells into a pluripotent state through transcription factors. iPSCs overcome ethical concerns associated with embryonic stem cells and provide opportunities for personalized medicine, disease modeling, and patient-specific regenerative therapies. Their application in clinical trials involving retinal degeneration, Parkinson’s disease, and cardiac regeneration has shown encouraging outcomes; however, genomic instability and tumorigenic risks remain challenges requiring further investigation [17,18]. The choice of stem cell source in clinical therapy depends on factors such as disease pathology, regenerative requirement, immune compatibility, ethical considerations, scalability, and safety profile. Continuous research is focused on improving cell isolation, differentiation efficiency, and therapeutic targeting to maximize clinical success and minimize adverse outcomes [19,20].
Table 1. Classification and Characteristics of Stem Cells Used in Clinical Therapy
|
Type of Stem Cell |
Source |
Differentiation Potential |
Major Clinical Applications |
Advantages |
Limitations |
Ref. |
|
Embryonic Stem Cells (ESCs) |
Inner cell mass of blastocyst |
Pluripotent |
Tissue engineering, neurodegenerative disorders |
High proliferative capacity |
Ethical concerns, tumorigenicity |
[13] |
|
Hematopoietic Stem Cells (HSCs) |
Bone marrow, peripheral blood, cord blood |
Multipotent |
Leukemia, lymphoma, anemia |
Established clinical use |
Limited differentiation potential |
[15] |
|
Mesenchymal Stem Cells (MSCs) |
Bone marrow, adipose tissue, umbilical cord |
Multipotent |
Osteoarthritis, cardiovascular diseases, autoimmune disorders |
Immunomodulatory effects |
Variable efficacy |
[14,19] |
|
Neural Stem Cells (NSCs) |
Brain and spinal cord |
Multipotent |
Neurodegenerative diseases |
Neural regeneration |
Limited availability |
[12] |
|
Perinatal Stem Cells |
Placenta, umbilical cord blood |
Multipotent |
Hematological and neurological disorders |
Low immunogenicity |
Storage limitations |
[11,16] |
|
Induced Pluripotent Stem Cells (iPSCs) |
Reprogrammed somatic cells |
Pluripotent |
Personalized medicine, retinal repair |
Patient-specific therapy |
Risk of genetic instability |
[17,18] |
Clinical Trials Of Stem Cell Therapy In Major Diseases
Stem cell therapy has rapidly progressed from experimental laboratory investigations to clinical evaluation in multiple therapeutic areas. Clinical trials are primarily designed to assess the safety, efficacy, dosage optimization, and long-term therapeutic outcomes of stem cell–based interventions. The increasing number of registered clinical studies reflects growing confidence in regenerative medicine as a promising treatment modality for chronic, degenerative, and currently incurable diseases. Different stem cell populations, particularly mesenchymal stem cells, hematopoietic stem cells, and induced pluripotent stem cells, have demonstrated encouraging therapeutic potential in various clinical settings [21,22]. In hematological disorders, stem cell transplantation remains one of the most successful and clinically established therapeutic strategies. Hematopoietic stem cell transplantation (HSCT) has become a standard treatment for leukemia, lymphoma, aplastic anemia, multiple myeloma, and inherited immunological disorders. Clinical evidence demonstrates that transplantation of healthy hematopoietic stem cells can restore normal blood cell production and immune function, significantly improving survival rates among patients with hematological malignancies. Autologous and allogeneic stem cell transplantation approaches have both shown effectiveness, although graft-versus-host disease remains a significant complication in allogeneic transplantation [23,24]. Cardiovascular diseases constitute another major focus of stem cell clinical research. Myocardial infarction and heart failure are characterized by irreversible cardiomyocyte loss and limited regenerative capacity of cardiac tissue. Several clinical trials have investigated the administration of mesenchymal stem cells, bone marrow–derived stem cells, and cardiac progenitor cells to improve cardiac repair and vascular regeneration. Early clinical findings suggest modest improvements in cardiac function, reduction in scar tissue formation, and enhanced myocardial perfusion; however, inconsistencies in clinical outcomes and variations in cell delivery techniques continue to challenge therapeutic standardization [25,26]. Neurological disorders represent one of the most promising yet complex areas of stem cell therapy research. Neurodegenerative diseases such as Parkinson’s disease, Alzheimer’s disease, amyotrophic lateral sclerosis, and spinal cord injury are characterized by irreversible neuronal damage and limited regenerative potential. Clinical trials involving neural stem cells, mesenchymal stem cells, and induced pluripotent stem cell–derived neurons have shown encouraging outcomes in terms of neuroprotection, reduction in inflammation, and functional improvement. Particularly, iPSC-derived dopaminergic neurons have demonstrated potential for restoring neuronal function in Parkinson’s disease, although long-term safety and tumorigenicity concerns remain under investigation [27,28]. Stem cell therapy has also shown substantial promise in orthopedic and musculoskeletal disorders, especially in cartilage repair, bone regeneration, and degenerative joint diseases. Osteoarthritis, osteoporosis, and tendon injuries are commonly investigated conditions in regenerative medicine. Mesenchymal stem cells derived from bone marrow or adipose tissue have demonstrated regenerative capabilities through anti-inflammatory effects and promotion of extracellular matrix repair. Clinical trials suggest improvement in pain management, mobility, and tissue regeneration, although standardized treatment protocols are still lacking [29]. Autoimmune and inflammatory diseases have become increasingly important targets for stem cell therapy due to the immunomodulatory properties of mesenchymal stem cells. Conditions such as multiple sclerosis, rheumatoid arthritis, Crohn’s disease, and systemic lupus erythematosus involve abnormal immune activation leading to chronic inflammation and tissue destruction. Stem cell–based interventions have shown the ability to regulate immune responses, suppress inflammation, and improve clinical symptoms in several early-stage clinical trials. However, larger randomized controlled trials are required to validate long-term therapeutic efficacy and safety [30]. Diabetes mellitus, particularly type 1 diabetes, has emerged as another major therapeutic target for stem cell research. The destruction of insulin-producing pancreatic β-cells creates a need for lifelong insulin therapy and continuous disease management. Clinical studies are increasingly exploring the differentiation of stem cells into functional pancreatic β-cells to restore endogenous insulin production. Although preliminary findings are promising, challenges including immune-mediated destruction, graft survival, and long-term metabolic control remain significant barriers to clinical translation [31,32]. The application of stem cells in ophthalmological disorders has generated considerable attention due to the accessibility of ocular tissues and the limited regenerative capacity of retinal structures. Clinical trials involving retinal pigment epithelial cells derived from induced pluripotent stem cells or embryonic stem cells have demonstrated promising outcomes in age-related macular degeneration and retinal dystrophies. These approaches may eventually provide restorative treatment options for vision loss that were previously considered irreversible [33]. Despite encouraging progress across multiple disease areas, the translation of stem cell therapy into routine clinical practice remains constrained by concerns regarding treatment standardization, ethical considerations, regulatory approval, cell survival, and long-term safety outcomes. Consequently, ongoing clinical trials continue to focus not only on therapeutic effectiveness but also on optimizing administration routes, dosing regimens, and patient selection criteria to maximize treatment success [34,35].
Challenges And Limitations In Clinical Translation Of Stem Cell Therapy
Despite remarkable progress in stem cell research and encouraging findings from clinical trials, the widespread clinical implementation of stem cell therapy continues to face numerous scientific, ethical, technical, and regulatory barriers. Although stem cells possess enormous regenerative potential, translating laboratory discoveries into safe, effective, and standardized therapeutic products remains a significant challenge. Variability in clinical outcomes, inconsistent treatment protocols, and concerns regarding long-term safety have slowed the transition of stem cell therapy into routine medical practice [36,37]. One of the primary challenges associated with stem cell therapy is immune rejection and host incompatibility. Although autologous stem cells reduce the risk of immune-mediated rejection, allogeneic transplantation may trigger immune responses leading to graft failure or graft-versus-host disease (GVHD). Mesenchymal stem cells exhibit relatively low immunogenicity; however, immune-related complications can still occur depending on the transplantation environment and disease condition. Researchers continue to explore immune suppression strategies and gene editing technologies to overcome compatibility barriers [38]. Tumorigenicity remains another major safety concern, particularly in therapies involving pluripotent stem cells such as embryonic stem cells and induced pluripotent stem cells. Incomplete differentiation or contamination with undifferentiated cells can result in teratoma formation after transplantation. Genetic instability occurring during cell expansion and reprogramming further increases oncogenic risks. Therefore, strict quality control measures, genomic screening, and controlled differentiation protocols are necessary to ensure therapeutic safety [39,40]. Standardization and reproducibility of stem cell products represent major limitations in clinical translation. Stem cells derived from different tissues or donors often display significant heterogeneity in biological activity, differentiation potential, and therapeutic performance. Differences in isolation methods, culture conditions, storage procedures, and administration routes contribute to inconsistent clinical outcomes across studies. The absence of universally accepted manufacturing guidelines further complicates comparison between clinical trials [41]. Ethical concerns surrounding stem cell use continue to influence public perception and regulatory approval. Embryonic stem cell research remains controversial because of ethical debates regarding embryo destruction. Although induced pluripotent stem cells have minimized some ethical limitations, concerns regarding consent, ownership of biological materials, and genetic manipulation persist. Ethical frameworks must balance scientific innovation with social and moral responsibilities [42]. The scalability and commercialization of stem cell therapies also present considerable obstacles. Large-scale production of stem cells requires sophisticated infrastructure, controlled manufacturing environments, and stringent quality assurance systems. The cost of cell expansion, cryopreservation, transportation, and personalized manufacturing significantly increases treatment expenses, limiting accessibility for patients, particularly in low- and middle-income countries [43]. Another critical issue is the limited survival, migration, and integration of transplanted stem cells after administration. Many transplanted cells fail to survive in hostile microenvironments characterized by inflammation, oxidative stress, hypoxia, and immune activation. Poor engraftment efficiency reduces therapeutic effectiveness and may require repeated administration, increasing treatment complexity and cost [44]. Regulatory uncertainty also remains a major challenge in stem cell therapy development. Different countries follow varying approval pathways and clinical standards, resulting in inconsistent regulatory oversight. Furthermore, the rise of unregulated stem cell clinics offering unproven therapies has raised concerns regarding patient safety, misleading claims, and ethical malpractice. Stronger international guidelines and evidence-based regulatory systems are essential to ensure safe clinical implementation [45].
Table 2: Major Challenges in Clinical Translation of Stem Cell Therapy
|
Challenge |
Description |
Impact on Clinical Application |
Reference |
|
Immune Rejection |
Host immune response against transplanted cells |
Reduced graft survival and therapeutic efficacy |
[38] |
|
Tumorigenicity |
Risk of teratoma or tumor formation |
Safety concerns and delayed approval |
[39,40] |
|
Cell Heterogeneity |
Variability among stem cell populations |
Inconsistent therapeutic outcomes |
[41] |
|
Ethical Issues |
Concerns regarding embryonic stem cells |
Public and regulatory limitations |
[42] |
|
High Treatment Cost |
Expensive manufacturing and storage |
Limited accessibility |
[43] |
|
Poor Cell Survival |
Low engraftment after transplantation |
Reduced treatment effectiveness |
[44] |
|
Regulatory Complexity |
Lack of harmonized guidelines |
Delayed clinical approval |
[45] |
Table 3: Limitations of Different Stem Cell Types in Clinical Therapy
|
Stem Cell Type |
Major Limitation |
Clinical Concern |
Reference |
|
Embryonic Stem Cells (ESCs) |
Ethical controversy, tumorigenicity |
Restricted clinical use |
[39,42] |
|
Mesenchymal Stem Cells (MSCs) |
Variable efficacy |
Inconsistent regeneration |
[41] |
|
Hematopoietic Stem Cells (HSCs) |
Risk of GVHD |
Immune complications |
[38] |
|
Induced Pluripotent Stem Cells (iPSCs) |
Genetic instability |
Tumor risk |
[40] |
|
Neural Stem Cells |
Limited availability |
Restricted scalability |
[44] |
Although these challenges are substantial, continuous advancements in biotechnology, gene editing, biomaterials, tissue engineering, and artificial intelligence are gradually improving the safety and efficiency of stem cell therapies. Addressing these limitations through standardized manufacturing, robust clinical evidence, and improved regulatory oversight will be critical for the successful integration of stem cell therapy into mainstream healthcare systems [36,45].
Future Perspectives And Emerging Innovations In Stem Cell Therapy
The future of stem cell therapy is expected to be shaped by advances in regenerative medicine, gene engineering, biomaterials, and computational technologies. Although current stem cell–based interventions have shown encouraging therapeutic outcomes, emerging innovations are focused on improving efficacy, precision, safety, and accessibility. Future clinical applications are likely to transition from generalized regenerative strategies toward highly personalized and disease-specific therapeutic approaches [46,47]. One of the most promising future directions in stem cell therapy is the integration of gene editing technologies, particularly clustered regularly interspaced short palindromic repeats (CRISPR-Cas9). Gene editing enables correction of disease-causing genetic mutations in stem cells before transplantation, thereby improving therapeutic effectiveness and reducing disease recurrence. This strategy has generated substantial interest for inherited disorders such as sickle cell anemia, β-thalassemia, cystic fibrosis, and muscular dystrophy. The combination of gene-edited stem cells with regenerative medicine may revolutionize treatment for genetic diseases previously considered incurable [48,49]. Personalized regenerative medicine using induced pluripotent stem cells (iPSCs) is another rapidly emerging area. Patient-specific iPSCs generated from somatic cells provide individualized therapeutic opportunities with minimal immune rejection risk. These cells can be differentiated into disease-relevant tissues for transplantation, disease modeling, and drug toxicity screening. Personalized stem cell therapies are expected to improve treatment outcomes by accounting for genetic variability and patient-specific biological characteristics [50]. Organoid technology represents a transformative innovation in stem cell research. Stem cell-derived organoids are miniature three-dimensional tissue structures that closely mimic human organs in terms of cellular architecture and function. Organoids are increasingly used for studying disease mechanisms, personalized drug screening, cancer research, and regenerative medicine applications. In the future, organoid transplantation may provide alternatives for organ replacement and reduce dependency on donor organ transplantation [51,52]. Stem cell–derived extracellular vesicles and exosomes are emerging as promising cell-free therapeutic alternatives. Exosomes contain bioactive molecules such as proteins, RNA, growth factors, and cytokines that mediate regenerative and immunomodulatory effects. Compared with whole-cell transplantation, exosome-based therapy offers advantages including lower immunogenicity, reduced tumorigenicity, easier storage, and improved safety profiles. Clinical interest in exosome therapeutics is increasing for cardiovascular, neurological, and inflammatory diseases [53]. The integration of tissue engineering and three-dimensional bioprinting is also expected to redefine the future of regenerative medicine. Bioprinting technologies enable the fabrication of artificial tissues and scaffolds capable of supporting stem cell growth and differentiation. These engineered constructs may eventually allow regeneration of complex tissues such as cartilage, bone, skin, blood vessels, and even whole organs. Such developments may substantially reduce organ transplantation shortages and improve patient outcomes [54,55]. Artificial intelligence (AI) and machine learning are increasingly contributing to stem cell research by improving data analysis, predictive modeling, and treatment optimization. AI-based systems can analyze complex biological datasets to predict stem cell differentiation patterns, identify therapeutic biomarkers, and optimize manufacturing conditions. Furthermore, computational approaches may enhance clinical trial design and patient selection, ultimately improving therapeutic success rates [56]. Another important future direction involves the development of universal donor stem cells through genetic engineering. Immune-compatible “off-the-shelf” stem cell products may overcome limitations associated with donor availability, immune rejection, and high treatment costs. Such universal stem cell banks could improve accessibility and enable rapid therapeutic intervention for various diseases [57].
Table 4 : Emerging Innovations in Stem Cell Therapy
|
Emerging Technology |
Principle |
Potential Clinical Application |
Major Advantage |
Reference |
|
CRISPR-Cas9 Gene Editing |
Correction of genetic mutations |
Genetic disorders, inherited diseases |
Precision therapy |
[48,49] |
|
Induced Pluripotent Stem Cells (iPSCs) |
Patient-specific stem cell generation |
Personalized medicine |
Reduced immune rejection |
[50] |
|
Organoid Technology |
Miniature organ development |
Disease modeling, transplantation |
Mimics human physiology |
[51,52] |
|
Exosome Therapy |
Cell-free regenerative signaling |
Cardiovascular and neurological diseases |
Reduced tumor risk |
[53] |
|
3D Bioprinting |
Fabrication of tissue scaffolds |
Organ regeneration |
Customized tissue repair |
[54,55] |
|
Artificial Intelligence |
Predictive biological modeling |
Clinical trial optimization |
Improved precision |
[56] |
|
Universal Donor Stem Cells |
Immune-compatible engineered cells |
Large-scale therapy |
Enhanced accessibility |
[57] |
Table 5: Comparison Between Current and Future Stem Cell Therapeutic Approaches
|
Parameter |
Current Stem Cell Therapy |
Future Stem Cell Therapy |
Reference |
|
Treatment Approach |
Generalized cell transplantation |
Personalized regenerative medicine |
[50] |
|
Cell Source |
Donor-dependent |
Patient-specific or universal donor cells |
[57] |
|
Safety Profile |
Tumorigenicity concerns |
Improved genomic control |
[48] |
|
Therapeutic Precision |
Moderate |
High precision using AI and gene editing |
[56] |
|
Organ Regeneration |
Limited |
Advanced bioprinting and organoids |
[51,54] |
|
Cost and Accessibility |
High cost |
Potentially scalable |
[55,57] |
Despite considerable optimism, several barriers remain before these futuristic approaches can become standard clinical practice. Ethical considerations, regulatory approval, long-term safety assessment, manufacturing scalability, and cost-effectiveness continue to require careful evaluation. Nevertheless, continuous technological advancements suggest that stem cell therapy may eventually transition from experimental interventions to mainstream curative treatments for numerous chronic and degenerative diseases [46,47].
Ethical And Regulatory Considerations In Stem Cell Therapy
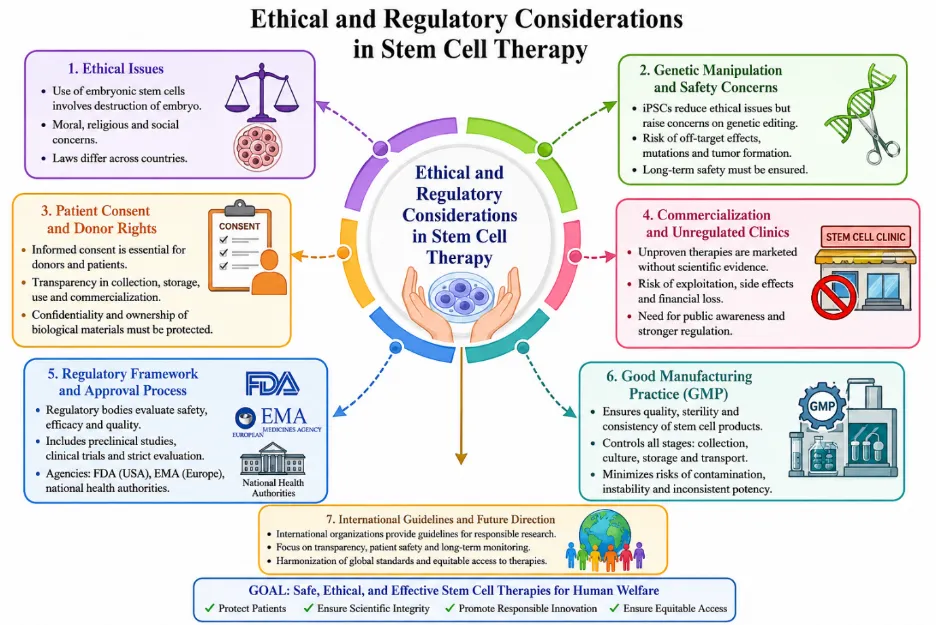
Figure 2. Ethical and Regulatory Considerations in Stem Cell Therapy: Key Challenges, Regulatory Frameworks, and Future Directions
The rapid advancement of stem cell research has introduced several ethical, legal, and regulatory concerns that significantly influence the development and clinical implementation of stem cell–based therapies. Although stem cell therapy offers promising therapeutic opportunities for numerous chronic and degenerative diseases, ethical controversies and regulatory inconsistencies continue to shape public acceptance and scientific progress. Addressing these concerns is essential to ensure patient safety, scientific integrity, and equitable access to regenerative treatments [58,59]. One of the most debated ethical issues in stem cell research relates to the use of embryonic stem cells (ESCs). Embryonic stem cells are derived from the inner cell mass of blastocysts, a process that involves destruction of the embryo. This has raised moral objections among various religious, ethical, and social groups regarding the moral status of human embryos. Ethical debates have led to differences in legislation across countries, with some nations permitting embryonic stem cell research under strict supervision while others impose significant restrictions or complete bans [60]. The development of induced pluripotent stem cells (iPSCs) has helped alleviate some ethical concerns because these cells are generated through reprogramming adult somatic cells without embryo destruction. Despite this advantage, ethical questions remain regarding genetic manipulation, genomic editing, and long-term biological consequences. The possibility of unintended genetic mutations, off-target effects, and germline modifications has generated concern regarding the responsible application of these technologies in clinical medicine [61]. Patient consent and donor rights represent another critical ethical dimension in stem cell therapy. Stem cells are frequently obtained from biological tissues such as bone marrow, adipose tissue, umbilical cord blood, and embryos. Proper informed consent procedures must ensure that donors understand how their biological materials will be collected, stored, used, and potentially commercialized. Transparency regarding risks, benefits, confidentiality, and ownership of biological samples is necessary to maintain ethical standards in biomedical research [62]. The commercialization of stem cell therapies has also generated ethical concerns, particularly due to the emergence of unregulated clinics offering unproven treatments. Many private clinics market stem cell interventions for disorders lacking scientific evidence or regulatory approval, potentially exposing patients to severe health risks and financial exploitation. Reports of adverse effects, infections, tumor formation, and treatment failures emphasize the urgent need for stronger regulation and public awareness regarding evidence-based stem cell therapies [63]. Regulatory frameworks for stem cell therapy vary substantially among countries, creating challenges in global standardization and clinical translation. Regulatory agencies such as the United States Food and Drug Administration, the European Medicines Agency, and national health authorities play essential roles in evaluating stem cell products for safety, efficacy, manufacturing quality, and clinical benefit. Stem cell products typically undergo extensive preclinical studies, phased clinical trials, and manufacturing compliance requirements before receiving market approval [64]. Good Manufacturing Practice (GMP) guidelines are particularly important for stem cell production because they ensure consistency, sterility, quality control, and reproducibility of cellular products. Since stem cells are living biological entities, even minor variations in culture conditions, storage, or transportation may significantly affect therapeutic performance and patient outcomes. Therefore, regulatory agencies emphasize strict monitoring of manufacturing protocols to minimize risks associated with contamination, instability, and inconsistent potency [65]. International organizations have also contributed to ethical governance through the development of guidelines for stem cell research and clinical application. Scientific communities advocate responsible innovation, transparency, patient-centered care, and long-term monitoring of treated individuals to maintain trust and improve therapeutic outcomes. Future regulatory efforts are expected to focus on harmonizing international standards, strengthening oversight of experimental therapies, and ensuring equitable access to advanced regenerative medicine technologies [66]. Although ethical and regulatory barriers may initially slow scientific advancement, they are essential for protecting patients from harm and maintaining public confidence in stem cell medicine. A balanced approach that promotes scientific innovation while ensuring ethical accountability and regulatory rigor will be critical for the safe integration of stem cell therapy into mainstream healthcare systems [67].
CONCLUSION
Stem cell therapy has emerged as a promising and rapidly advancing field in regenerative medicine with the potential to transform the treatment of various chronic, degenerative, and life-threatening diseases. Clinical trials have demonstrated encouraging outcomes in conditions such as hematological disorders, cardiovascular diseases, neurodegenerative conditions, autoimmune disorders, and diabetes, highlighting the regenerative and immunomodulatory potential of stem cells. Despite significant progress, challenges including immune rejection, tumorigenicity, ethical concerns, high treatment costs, and regulatory limitations continue to hinder widespread clinical application. Nevertheless, advancements in gene editing, induced pluripotent stem cells, organoid technology, exosome therapy, and tissue engineering are expected to improve the safety, efficacy, and accessibility of stem cell–based treatments. Overall, stem cell therapy represents a promising frontier in modern medicine. Continued clinical research, technological innovation, and robust regulatory oversight are essential to ensure safe and effective translation of stem cell therapies into routine healthcare practice.
REFERENCES




Ankita Kadam*, Sadiya Jamdar, Sanika Charne, Ravina Kamble, Dhanraj Jadge, Clinical Trials and Future Perspectives of Stem Cell Therapy: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 81-96. https://doi.org/10.5281/zenodo.20483337
 10.5281/zenodo.20483337
10.5281/zenodo.20483337