
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3 Department of Pharmacology, PRES's College of Pharmacy (For Women), Chincholi, Sinnar, Nashik, Maharashtra, India.
4 Biotox Laboratories Pvt. Ltd., Nashik, Maharashtra, India.
Obstructive cholestatic liver diseases are characterized by impaired bile flow, leading to oxidative stress, inflammation, fibrosis, and progressive liver damage. Although conventional treatments are available, their effectiveness may be limited by adverse effects and high costs, creating a need for safer complementary therapies. Ginger (Zingiber officinale Roscoe) and lemon (Citrus limon L.) are rich sources of bioactive compounds with potent antioxidant and anti-inflammatory properties. Experimental studies have shown that these natural products can improve liver function, enhance antioxidant defenses, reduce inflammation, and attenuate histopathological damage in models of hepatotoxicity. This review summarizes the phytochemistry, hepatoprotective mechanisms, and experimental evidence supporting the use of ginger and lemon in bile duct obstruction-induced liver injury. It also highlights current research gaps and future prospects for their development as complementary therapeutic agents in cholestatic liver diseases
Hepatotoxicity is a major global health concern characterized by liver injury resulting from drugs, toxins, infections, metabolic disorders, or bile flow obstruction. Among these, bile duct obstruction (BDO)-induced hepatotoxicity is a severe condition associated with cholestasis, oxidative stress, inflammation, and progressive hepatic fibrosis. Obstruction of bile flow leads to the accumulation of toxic bile acids, bilirubin, and other metabolites within the liver, causing hepatocellular injury, inflammatory responses, extracellular matrix deposition, fibrosis, and ultimately cirrhosis or liver failure if left untreated [1,2]. The bile duct ligation (BDL) model is widely employed to investigate the pathophysiology of cholestatic liver injury because it closely resembles the biochemical and histopathological features observed in human cholestatic diseases. Bile duct obstruction promotes excessive production of reactive oxygen species (ROS), lipid peroxidation, mitochondrial dysfunction, and hepatocyte apoptosis, while activation of hepatic stellate cells accelerates collagen deposition and fibrotic progression [1,2]. Despite advances in treatment, currently available therapies remain limited by suboptimal efficacy, adverse effects, and high costs, creating a need for safer and more effective hepatoprotective agents.
Natural products have gained attention as alternative therapeutic approaches due to their antioxidant, anti-inflammatory, antifibrotic, and cytoprotective properties. Among them, Zingiber officinale (ginger) and Citrus limon (lemon) are rich sources of bioactive phytochemicals. Ginger contains gingerols, shogaols, paradols, and zingerone, whereas lemon is abundant in flavonoids, vitamin C, citric acid, limonene, and other phenolic compounds. These constituents exhibit potent free-radical scavenging, anti-inflammatory, and hepatoprotective activities and have demonstrated beneficial effects in experimental models of liver injury [3,4]. The combination of ginger and lemon may provide synergistic hepatoprotection by reducing oxidative stress, suppressing inflammatory cytokines, enhancing antioxidant defenses, and attenuating fibrosis. Therefore, this review critically evaluates the pathophysiological mechanisms of BDO-induced hepatotoxicity and summarizes current evidence regarding the therapeutic potential of ginger and lemon as complementary hepatoprotective agents in cholestatic liver diseases [3,4].
BACKGROUND ON HEPATOTOXICITY:
Bile Duct Obstruction-Induced Hepatotoxicity
Bile duct obstruction (BDO) causes accumulation of bile acids, bilirubin, and toxic metabolites in the liver, resulting in cholestasis, oxidative stress, inflammation, fibrosis, and eventual liver dysfunction [5,7].
Structural and Functional Liver Changes
Persistent cholestasis leads to hepatocyte necrosis, vacuolar degeneration, inflammatory cell infiltration, bile duct epithelial damage, and disruption of normal liver architecture [7,9].
Oxidative Stress and Inflammation
BDO promotes excessive production of reactive oxygen species (ROS), causing mitochondrial dysfunction, lipid peroxidation, and hepatocyte apoptosis. Neutrophil infiltration further aggravates oxidative injury [6,8].
Fibrosis and Disease Progression
Activation of hepatic stellate cells and cholangiocyte proliferation increase extracellular matrix deposition, leading to liver fibrosis and eventual cirrhosis if untreated [5,9].
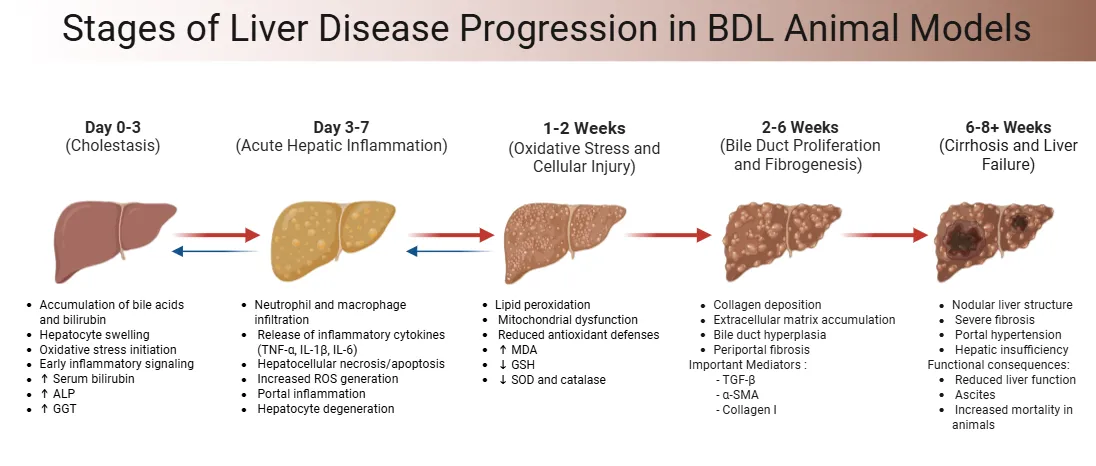
Figure 1: Progression of Cholestatic Liver Injury in Bile Duct Ligation Animal Model
Clinical and Pathological Importance of Cholestasis
Cholestasis results from impaired bile secretion or bile duct blockage, causing retention of bile acids and bilirubin. Common causes include gallstones, malignancies, surgical trauma, and congenital disorders. Clinically, it presents with jaundice, pruritus, elevated bilirubin, ALP, and GGT levels, and may progress to cholangitis, biliary cirrhosis, and hepatic failure [10,11].
Conventional Treatments and Their Limitations
Current therapies mainly focus on restoring bile flow and controlling symptoms; however, their effectiveness is often limited by adverse effects, high costs, incomplete disease reversal, and poor patient compliance. These limitations highlight the need for safer and more effective alternatives [10,11].
Rationale for Herbal Interventions
Medicinal plants rich in antioxidants and anti-inflammatory compounds have gained attention as hepatoprotective agents. Their ability to target multiple pathogenic pathways makes them promising candidates for cholestatic liver diseases [12,13].
Ginger (Zingiber officinale)
Ginger contains gingerols, shogaols, and zingerone, which exhibit strong antioxidant, anti-inflammatory, and hepatoprotective activities. These compounds reduce ROS generation, suppress inflammatory mediators and improve liver function [12,13].
Lemon (Citrus limon)
Lemon is rich in flavonoids, vitamin C, hesperidin, rutin, and eriodyctiol. These phytochemicals possess potent free-radical scavenging and anti-inflammatory properties that help protect hepatocytes from oxidative damage [12,13].
Synergistic Hepatoprotective Effects
The combination of ginger and lemon may provide synergistic benefits by reducing oxidative stress, inhibiting inflammatory cytokines, improving antioxidant defenses, lowering liver enzyme levels, and protecting liver architecture against cholestatic injury [12,13].
Table 1: Key Molecular and Cellular Processes of Bile Duct Obstruction-Induced Cholestasis Associated Hepatotoxicity
|
Mechanism |
Pathophysiological Events |
Consequences in Liver Injury |
|
Bile Acid Accumulation and Direct Hepatocyte Injury |
Hydrophobic bile acids become trapped within the cells if they are obstructed from flowing from the liver. The bile acids have detergent effects on plasma and mitochondrial membranes, which results in the disruption of membranes and the formation of reactive oxygen species (ROS). Hydrophobic bile acids induce mitochondrial permeability transition (MPT), resulting in loss of mitochondrial membrane potential and release of pro-apoptotic factors such as cytochrome c and apoptosis-inducing factor (AIF) |
Hepatocyte apoptosis and necrosis, oxidative stress, mitochondrial dysfunction, lipid peroxidation, and amplification of liver injury |
|
Pro-inflammatory signaling in Hepatocytes |
Elevated bile acid levels cause pro-inflammatory signaling specifically in hepatocytes. Cytokine and chemokine expression leads to the recruitment of neutrophils to periportal regions. Hepatic inflammatory responses and neutrophil-mediated injury are increased, |
Leading to hepatocellular damage and the progression of cholestatic liver injury, upon activation of innate immune receptors, such as Toll-like receptor-9 (TLR9). |
|
Reactive Oxygen Species (ROS) generation |
Excess Bile Acid leads to Oxidative Stress and Reactive Oxygen Species (ROS) generation by mitochondrial dysfunction and activated neutrophils. Lipid peroxidation, DNA damage, protein oxidation and endoplasmic reticulum (ER) stress pathways are activated by oxidative stress. When oxidants and antioxidants are out of balance, this exacerbates the damage to the cells. |
Dysfunction, apoptosis, oxidative damage and activation of fibrogenic pathways by hepatocytes |
|
The mechanism of injury is not known |
Pathophysiological Events: The mechanism of injury is not known. Abnormal Autophagy and Cellular Homeostasis Autophagy is a protective process that eliminates damaged mitochondria and clears up the accumulation of ROS. Accumulation of damaged organelles due to impaired autophagy, ineffective stress regulation (during prolonged cholestasis) |
increased hepatocyte apoptosis, oxidative injury, worsening cholestatic liver damage. |
|
Mitochondrial accumulation of cholesterol and altered lipid homeostasis |
Proteases like steroidogenic acute regulatory protein domain-containing protein-1 (STARD1) are responsible for the accumulation of cholesterol in the mitochondria in cholestasis. Increased mitochondrial cholesterol decreases mitochondrial glutathione and enhances susceptibility to bile acid-induced toxicity |
Increased oxidative stress, inflammation, hepatocyte injury, and fibrosis. |
|
Protective Regulatory Mechanisms and Therapeutic Targets |
Nuclear receptors and antioxidant pathways, including Farnesoid X Receptor (FXR) and Nuclear factor erythroid 2-related factor 2 (Nrf2), regulate bile acid homeostasis and antioxidant defense. Therapeutic agents such as ursodeoxycholic acid and 18β-glycyrrhetinic acid reduce bile acid toxicity and inflammatory responses. |
Promote more oxidation, inflammation, hepatocyte injury and fibrosis with bile acid induced toxicity. |
Mechanism of Cholestasis:
The characteristics of cholestasis are inability to produce bile and/or inability to secrete bile, which leads to the buildup of toxic bile acids (BAs) in the liver. This BAs retention directly damages the liver by injuring, inflaming and fibrating the liver, then cirrhosis occurs. Pathogenesis of cholestasis is multifactorial, which includes changes in the transport, synthesis, metabolism of BAs, oxidative stress, immune responses and cell signalling pathways.
OXIDATIVE STRESS, ACCUMULATION OF TOXIC BILE ACID AND HEPATOCELLULAR INJURY:
Toxic Bile Acid Accumulation and Oxidative Stress
During cholestasis, impaired bile flow causes accumulation of toxic hydrophobic bile acids within hepatocytes. These bile acids disrupt mitochondrial function, induce reactive oxygen species (ROS) generation, lipid peroxidation, DNA damage, and endoplasmic reticulum stress, ultimately resulting in hepatocyte apoptosis and necrosis [13,14].
Role of Oxidative Stress in Liver Injury
Excessive ROS activates inflammatory signaling pathways and hepatic stellate cells (HSCs), promoting inflammation and fibrosis. Neutrophils recruited during cholestasis further aggravate oxidative damage through ROS production [14].
Protective Role of Autophagy
Autophagy removes damaged mitochondria and excess ROS, thereby protecting hepatocytes from apoptosis. Activation of autophagy attenuates cholestatic liver injury, whereas inhibition worsens oxidative stress and cell death [15].
Antioxidant-Based Therapeutic Approaches
Natural antioxidants such as epigallocatechin-3-gallate (EGCG), 18β-glycyrrhetinic acid, and arbutin reduce oxidative stress, inflammation, and fibrosis by regulating antioxidant pathways and bile acid metabolism [15].
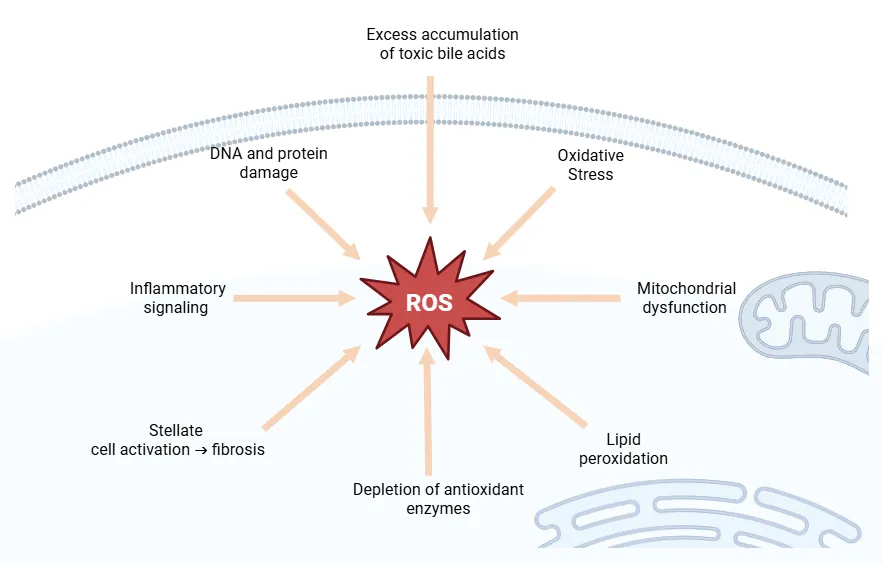
Figure 2: Reactive Oxygen Species (ROS) As Central Players in Hepatocellular Injury and Progression of Fibrosis in Cholestasis
Emerging Role of Nanozymes
Nanozyme-based antioxidants possess broad-spectrum ROS scavenging activity and have shown promise in reducing hepatocyte apoptosis, inflammation, and oxidative damage during liver injury [16].
Immune Activation and Inflammatory Response
Cholestatic hepatocytes release pro-inflammatory cytokines that recruit neutrophils and other immune cells. Key inflammatory mediators include NF-κB, CCL2 chemokines, and Toll-like receptor signaling pathways. Persistent inflammation contributes to bile duct proliferation, fibrosis, and disease progression [17].
Adaptive Response Through Nuclear Receptors
Nuclear receptors including Farnesoid X Receptor (FXR), Pregnane X Receptor (PXR), Vitamin D Receptor (VDR), and Constitutive Androstane Receptor (CAR) regulate bile acid synthesis, metabolism, detoxification, and transport. These adaptive mechanisms reduce bile acid toxicity and represent important therapeutic targets in cholestatic liver diseases [18].
Endoplasmic Reticulum Stress and Cell Death
Accumulation of toxic bile acids induces endoplasmic reticulum stress and activates inflammatory pathways such as the NLRP3 inflammasome. Protective proteins such as Sestrin2 help maintain ER homeostasis and reduce inflammatory cell death during cholestasis [18].
Fibrosis and Disease Progression
Chronic bile acid accumulation and inflammation stimulate hepatic stellate cells, leading to collagen deposition, extracellular matrix remodeling, and progressive fibrosis. Nuclear receptor-mediated signaling pathways offer additional therapeutic opportunities for limiting fibrosis and disease progression [19].
OXIDATIVE STRESS AND LIVER DAMAGE:
Oxidative stress plays a central role in cholestatic liver injury. Accumulation of toxic bile acids following bile duct obstruction causes excessive reactive oxygen species (ROS) generation, lipid peroxidation, DNA damage, mitochondrial dysfunction, and hepatocyte apoptosis. Increased malondialdehyde (MDA) levels and decreased glutathione (GSH) levels are indicators of oxidative damage [20].
Antioxidant Defense Mechanisms
Nrf2 regulates antioxidant defense by activating antioxidant response genes, while autophagy protects hepatocytes by removing damaged mitochondria and excess ROS. However, prolonged cholestasis overwhelms these protective mechanisms [20].
Antioxidant Effects of Ginger and Lemon
Zingiber officinale and Citrus limon contain potent antioxidant phytochemicals. Ginger constituents such as 6-gingerol and 6-shogaol inhibit ROS generation and enhance antioxidant enzymes including catalase, superoxide dismutase, and glutathione peroxidase. Lemon flavonoids such as hesperidin, rutin, and eriodyctiol further strengthen antioxidant protection against liver injury [21].
Inflammatory Pathways (TNF-α, NF-κB, Cytokines)
TNF-α and NF-κB are major mediators of cholestatic liver injury. NF-κB activation increases the expression of pro-inflammatory cytokines including TNF-α, IL-6, and IL-8, leading to hepatocyte apoptosis, inflammation, and fibrosis [21].
Anti-inflammatory Effects of Ginger
Ginger suppresses NF-κB activation and reduces TNF-α and IL-6 expression, thereby attenuating inflammatory responses and protecting against cholestatic liver damage [22].
Apoptosis and ER Stress
Toxic bile acids induce endoplasmic reticulum (ER) stress and mitochondrial dysfunction, resulting in CHOP-mediated apoptosis and activation of death receptor pathways such as TRAIL receptors [22].
Fibrosis and Disease Progression
Persistent inflammation activates hepatic stellate cells and cholangiocytes, promoting extracellular matrix deposition and fibrosis. TGF-β1, α-SMA, iNOS, and STARD1 are key mediators involved in fibrogenesis [23].
Anti-apoptotic and Anti-fibrotic Effects of Ginger and Lemon
Ginger and lemon exhibit anti-apoptotic and anti-fibrotic properties. Ginger decreases Bax/Bcl-2 ratio and caspase-3 activity, whereas lemon reduces lipid peroxidation and histological damage, helping preserve liver function and inhibit fibrosis [23].
INFLAMMATORY AND FIBROTIC ROLE OF TNF-Α IN THE LIVER:
TNF-α is one of the primary pro-inflammatory cytokines secreted during cholestatic liver damage, and it further damages the liver, likely through multiple mechanisms. In BDL models, up-regulated serum and tissue levels of TNF-α induce hepatocyte apoptosis through death receptor/ligand interactions and mitochondrial permeability transition. This is the induction of apoptosis which causes liver damage and affects bile acid handling by the liver, reducing bile salt uptake and worsening cholestasis. Furthermore, the sensitisation of cholangiocytes to apoptosis by the action of TNF-α weakens the integrity of bile ducts. A profibrotic contribution develops when the hepatitial stellate cells (HSCs) are stimulated by TNF- α to express tissue inhibitor of metalloproteinase-1 (TIMP-1) which inhibits the degradation of the extracellular matrix, thereby maintaining the liver fibrosis. Interestingly, although TNF-α deficiency does not decrease overall inflammation or liver damage, it has a selective profibrotic effect through TIMP-1 up-regulation, suggesting a complicated role for TNF-α.[24]
NF-κB Signaling Pathway in Cholestatic Inflammation:
The transcription factor NF-κB regulates the expression of a number of inflammatory genes, such as TNF-α, IL-6, and IL-8. Hepatic NF-κB activation due to bile duct obstruction leads to the transcription of pro-inflammatory mediators by Kupffer cells and hepatocytes. The activation of NF-κB also promotes the polarization of macrophages towards the M1 phenotype and production of ROS, which further enhances inflammation and damage. Importantly, the absence of NF-κB signalling elements (such as the IKK1 and IKK2 kinases) in hepatocytes renders these cells more susceptible to damage to the bile duct, suggesting that under normal circumstances NF-κB maintains immune homeostasis and bile duct integrity, but chronic activation leads to pathological inflammation.[25]
Anti-Inflammatory Properties of Ginger, via NF-κB Inhibition:
Ginger (Zingiber officinale) has been shown to have potent anti-inflammatory effects by inhibiting NF-κB activation and pro-inflammatory cytokines expression. In high-fat diet induced hepatic inflammation models, ginger extract reduced hepatic mRNA expressions of TNF-α and IL-6, and inhibited nuclear translocation of NF-κB and activity of the IκB kinase (IKK) effectively down regulating the liver inflammation. In addition, the active component 6-shogaol in ginger decreases NF-κB signaling in response to TNF-α in epithelial cells, which in turn lowers the production of cytokines and oxidative stress and thus preserves barrier function. The results suggest that ginger can be used as an effective medicinal herb to treat cholestatic liver diseases through its ability to regulate inflammatory pathways such as NF-κB and cytokines.[26]
Incorporating and implications of integration:
Involvement of NF-κB in the inflammatory cascade in cholestasis by cytokine production: TNF-α induces hepatocyte apoptosis, cholangiocyte injury and induces TIMP-1 in HSCs, leading to fibrogenic signaling. Importantly, NF-κB signaling functions in a dual manner, having both protective and pathological roles in maintaining bile duct. Herbal NF-κB inhibitors such as ginger can be used as potential alternative or adjunct drugs to prevent inflammation mediated hepatotoxicity in bile duct obstruction, due to their anti-inflammatory property by decreasing the pro-inflammatory cytokines, such as TNF-α.[26]
Apoptosis Mechanisms:
Cholestatic liver toxicity involves hepatocyte apoptosis mediated by toxic bile acid accumulation that leads to activation of two pathways: endoplasmic reticulum (ER) stress and mitochondrial pathway. In BDL models, there is upregulation of key mediators of ER stress-induced apoptosis including CHOP (CCAAT/enhancer-binding protein homologous protein), which promotes hepatocyte death by supporting pro-apoptotic proteins such as Bax. CHOP deficiency results in decreased apoptosis, cleaved caspase-3 expression and decreases severity of fibrosis. The death receptor pathways, which increase the expression of TRAIL-R2/DR5, sensitize hepatocytes to apoptosis. In cholestasis, autophagy is protective and prevents ROS accumulation and hepatocyte death, while its inhibition exacerbates hepatocyte death. Increasing the level of autophagy could therefore be a potential treatment for liver damage.[27]
Fibrosis Mechanisms:
Liver fibrosis in bile duct obstruction is a result of cholangiocyte proliferation (ductular reaction) and interactions with hepatic stellate cells and other cells that produce fibrous tissue, leading to deposition of extracellular matrix (ECM) that distorts tissue structure. Fibrosis markers transforming growth factor-beta1 (TGF-β1) and alpha-smooth muscle actin (α-SMA) are high after BDL, and closely matched with the severity of fibrosis. CHOP not only promotes apoptosis but also plays a role in fibrogenic signaling as CHOP deficient mice have reduced fibrosis. After bile duct ligation, inducible nitric oxide synthase (iNOS) was increased which seems to be involved in fibrotic progression; while the constitutive isoforms of NOS were not altered, this indicates NOS-related local toxicity. Additionally, STARD1-mediated mitochondrial cholesterol transport exacerbates injury and fibrosis by increasing mitochondrial oxidative stress and cell sensitivity to bile acids, unveiling a novel fibrosis pathway.[27]
Herbal Insights: Ginger and Lemon
Both ginger and lemon have bioactive components that regulate apoptosis and fibrogenesis in hepatic injuries. Ginger has anti-apoptotic properties which involve reduction in the Bax/Bcl-2 ratio, inhibition of the activity of caspase-3, and prevention of oxidative stress and mitochondrial apoptotic pathways. It has hepatoprotective and fibrosis-progression retarding effects, which seem to be mediated by its antioxidant and anti-inflammatory properties, through redox and apoptosis regulation. [24]
Lemon juice is a rich source of polyphenols which shows antioxidant activity thereby reducing the lipid peroxidation, improving histopathological changes and may interfere with the apoptotic and fibrotic pathway induced by oxidative stress, which helps to stabilize the cellular function and inhibits pro-fibrogenic signaling.[26]
Biochemical and Histopathological Alterations:
Bile duct obstruction leads to significant biochemical and histopathologic alterations in the liver that can lead to hepatotoxicity and disease progression. Ginger (Zingiber officinale) juice and lemon (Citrus limon) juice show protective properties with regard to these changes.
Biochemical Changes:
Liver enzymes are elevated, and are correlated with hepatocyte injury and bile duct damage, especially ALT, AST, ALP and GGT. When hepatocytes and bile duct cells are injured, these enzymes get into the bloodstream, indicating liver dysfunction. At the same time, there is a decrease in the activity of antioxidant enzymes such as superoxide dismutase (SOD), catalase, glutathione peroxidase (GPx), and glutathione S-transferase (GST), in support of the redox imbalance that follows bile duct ligation (BDL). Ginger (Zingiber officinale) juice and lemon (Citrus limon) juice have potent hepatoprotective activity which is able to reverse these effects. Lemon juice also decreases alcohol-induced increases in ALT, AST, hepatic triglycerides and lipid peroxidation products, and increases antioxidant enzyme activity and total antioxidant capacity (TAC) in mice, presumably due to its antioxidant activity, in various models such as carbon tetrachloride (CCl4)-induced hepatotoxicity and acetaminophen toxicity. Both juices have antioxidant properties, contributing to the balance of oxidative stress and lipid metabolism, with added hepatocyte protection against damage and steatosis.[28]
Histopathological Changes:
The histological changes of the liver brought about by bile duct obstruction are characterized by hepatocyte necrosis, inflammatory cell infiltration, proliferation of bile ducts, portal fibrosis and impairment of liver architecture. In experimental models, like CCl4 induced toxicity and alcohol induced injury, ginger and lemon juice treatment play significant role in reducing the necrosis, inflammation, fibrosis and fatty degeneration to a significant level. For instance, ginger and lemon juice reduced centrilobular necrosis and inflammatory infiltration in the CCl4 treated rats, while lemon juice was found to be beneficial in reducing degenerative and fatty changes in liver damaged by alcohol. Ginger extract or nanoparticles could serve as potential protective agents against acetaminophen-induced liver toxicity as well as other toxic conditions because of their ability to maintain liver histoarchitecture during such conditions. The attenuation of oxidative stress that leads to fibrogenesis is associated with reduced collagen deposition and fibrosis, consistent with the association of antioxidant therapies with these outcomes. [29]
Experimental Models of Bile Duct Obstruction:
COMMON ANIMAL MODELS:
Obstructive Cholestasis Models:
These are commonly used for experimental studies of obstructive cholestasis, which are primarily performed in rodents, most often rats and mice, and include Bile Duct Ligation (BDL). This causes cholestasis, hepatocyte damage and inflammation, proliferation of bile ducts, fibrosis and liver dysfunction, similar to extrahepatic cholestasis diseases in humans. It is useful for the study of liver injury, fibrogenesis and is a quick method of inducing biliary cirrhosis in comparison with chemical toxins.
Chemical-Induced Liver Injury (CCl4 Models):
Chronic exposure of the liver to CCl4 causes hepatocyte necrosis and subsequent fibrotic and cholestatic changes. This model can be used to test hepatoprotective agents such as ginger, lemon, etc., based on antioxidant and anti-fibrotic activity.
Chemotherapy-Induced Hepatotoxicity Models:
Hepatotoxicity that occurs due to the effects of certain chemotherapeutic agents such as cisplatin and doxorubicin are useful to screen phytochemicals, but cannot be used for mechanical bile duct obstruction.
Bile Duct Ligation (BDL) Model:
Obstruction of bile flow in BDL leads to the accumulation of bile acids and bilirubin which causes oxidative stress, inflammation and activation of hepatic stellate cells, thereby inducing fibrosis and cirrhosis, peaking around days 2-3 when the peak of hepatocellular injury occurs, associated with the infiltration of neutrophils, which is facilitated by adhesion molecules like ICAM-1, and proliferation of biliary epithelium. Then comes chronic inflammation, infiltration by lymphocytes and Kupffer cells, collagen deposition and fibrosis, stabilized by weeks 3-4. The use of pharmacological agents such as antioxidants, such as melatonin and metformin, help to reduce oxidative damage and improve liver histology in BDL rats, which provides further evidence for the oxidative and inflammatory mechanism of liver injury. Other compounds like chlorogenic acid are able to modulate bile acid transporters and enzymes that decrease hepatotoxicity in pathways influenced by SIRT1, showing the multifactorial mechanisms involved. Complete ligation (cBDL) results in global cholestasis while partial BDL (pBDL) leads to partial cholestasis with less morbidity in the animals, thus enhancing ethical compliance without compromising scientific rigor in BDL.
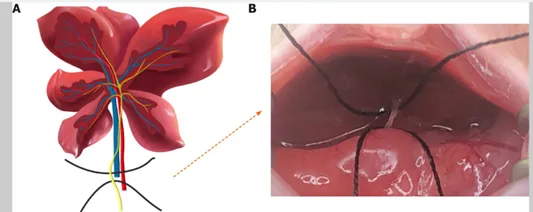
Figure 3: Schematic illustration of the process of bile duct ligation. A: Mouse liver, bile duct, portal vein and hepatic artery anatomy; B: Exposure of the bile duct
The BDL Model has been adapted into several variations:
Complete ligation (cBDL): The classical method to produce a liver injury and fibrosis is to ligate the common bile duct (full ligation (cBDL)) which leads to obstructive cholestasis of the entire liver.
Partial BDL (pBDL): Partial ligation of the hepatic bile duct in one lobe only, allowing some cholestasis and use of the other unligated lobes as internal controls. This variant minimizes morbidity of animals, and can be used to examine the differences between localized and systemic effects of bile duct obstruction.
BDL is commonly used to model the complications of chronic cholestatic liver disease such as hepatic encephalopathy, neuroinflammation, motor and cognitive dysfunction, and systemic inflammation. For instance, BDL causes hyperammonemia, activation of glial cells and blood-brain barrier disruption in mice, which are important parameters for hepatic encephalopathy studies [30].
Table 2: Major Biomarkers Associate with Bile Duct Obstruction-Induced Cholestasis Associated hepatotoxicity
|
Factors Category |
Name of Biomarkers |
Significant Role in Hepatotoxicity |
|
Liver Enzymes |
ALT, AST, ALP, GGT |
Sensitive markers of hepatocellular damage and bile duct damage. Raised levels are indicative of a liver dysfunction and cholestasis. |
|
Cholestatic Marker |
Total Bilirubin |
Increased bilirubin levels are indicative of bile duct obstruction and severity of cholestasis. |
|
Oxidative Stress Markers |
MDA, Protein Carbonyls |
Elevated levels which reflect increased lipid peroxidation and protein oxidation from exposure to Reactive Oxygen Species (ROS). |
|
Antioxidant Defense Markers |
GSH, GPx, SOD, Catalase |
Antioxidant defense systems are depleted during oxidative stress, as indicated by the lowered levels of these markers. |
|
Inflammatory Cytokines and Mediators |
TNF-α, IL-1β, IL-17A, MIP-1α, MIP-2, iNOS |
Increase in expression suggests activation of inflammatory pathways and immune-mediated liver damage. |
|
Fibrotic Markers |
α-SMA, TGF-β1, Collagen I, Fibronectin, CTGF, TIMP-1 |
These are associated with activation of the hepatic stellate cells, deposition of the extracellular matrix and progression of liver fibrosis. |
|
Apoptotic Markers |
Caspase-3, PARP, Cytochrome c, DNA Fragmentation |
More active means hepatocyte apoptosis and mitochondrial-mediated cellular injury. |
|
Cell Adhesion Molecules |
ICAM-1 |
Binds to neutrophils and increases their adherence and infiltration into the liver tissue, which exacerbates inflammation-induced liver damage. |
GINGER AND LEMON JUICE ARE EXAMPLES OF HERBS USED TO TREAT HEPATOTOXICITY
Ginger (Zingiber officinale) and lemon juice (Citrus limon) have shown significant hepatoprotective properties mainly due to their antioxidant and anti-inflammatory effects [48,49].
Ginger possesses bioactive compounds that inhibit cyclooxygenase-2 (COX-2), lipoxygenase (LOX), and NF-κB activation, thereby reducing inflammatory mediators and lipid peroxidation products such as malondialdehyde (MDA) [34].
Lemon juice contains flavonoids including eriodyctiol, rutin, hesperidin, and isorhamnetin that enhance radical scavenging activity, stimulate endogenous antioxidants, and suppress inflammatory cytokines [33,34].
The combined use of ginger and lemon promotes hepatoprotection through enhancement of antioxidant defenses, suppression of inflammatory pathways, and modulation of apoptosis and fibrosis [35].
Medicinal Plants in Liver Disorders: An Overview of Their Benefits and Risks
Although numerous herbs possess hepatoprotective activity, some herbal products can also induce hepatotoxicity, steatosis, fibrosis, cholestasis, or acute liver failure.
Plants containing pyrrolizidine alkaloids and herbs such as germander and chaparral have been associated with serious liver injury [36].
Conversely, ginger and lemon juice have demonstrated antioxidant, anti-inflammatory, and hepatoprotective activities with reductions in ALT, ALP, MDA, inflammation, and fibrosis in experimental studies.
The major advantages of phytotherapy include multitarget actions, affordability, accessibility, and synergistic effects among bioactive compounds.
Combined ginger and lemon preparations may provide superior antioxidative and hepatoprotective effects compared with individual administration [37].
PHARMACOGNOSY AND PHYTOCHEMISTRY OF GINGER (ZINGIBER OFFICINALE)
Botanical Description and Classification
Ginger (Zingiber officinale) is a herbaceous perennial plant belonging to the family Zingiberaceae and genus Zingiber. The rhizome is the principal medicinal part and contains numerous bioactive compounds responsible for its therapeutic properties .
The plant is characterized by fibrous roots, lanceolate leaves, aromatic rhizomes, and yellow-green flowers arranged in dense spikes. Proper botanical identification is essential for quality control and authentication in herbal medicine [38-42].
Phytoconstituents (Gingerols, Shogaols, Zingerone)
Ginger contains a complex mixture of secondary metabolites including gingerols, shogaols, paradols, and zingerone. Advanced analytical techniques such as HPLC and GC-MS have been employed to identify and characterize these bioactive constituents [42].
Table 3: Major Phytoconstituents, their Localization and Pharmacological Effects of Ginger
|
Phytoconstituent Category |
Major Compounds |
Pharmacological Properties |
|
Gingerols |
6-Gingerol, 8-Gingerol, 10-Gingerol |
Major pungent phenolic compounds with antioxidant, anti-inflammatory, anti-cancer and hepatoprotective activities. |
|
Shogaols |
6-Shogaol, 8-Shogaol |
Dehydrated products of gingerols formed during drying/heating; show strong antioxidant, anti-inflammatory and anti-apoptotic properties |
|
Zingerone and Paradols |
Zingerone, Paradols |
Add flavor and aroma; have antioxidant, anti-inflammatory, antimicrobial, and hepatoprotective properties. |
|
Volatile Oils |
Curcumene, Linalool, Zingiberene, β-Bisabolene |
Impart aroma properties, have antimicrobial, antioxidant, anti-inflammatory and hepatoprotective properties. |
|
Flavonoids and Phenolic Acids |
Chlorogenic Acid, Hesperidin, Quercetin |
They act as antioxidants, free-radical scavengers and reduce oxidative stress as a natural antioxidant. |
|
Phenolic Compounds |
Total Phenolics |
Phenolic Compounds have significant antioxidant potential as shown by total antioxidant capacity (TAC) and DPPH radical scavenging assay. |
Method of Extraction and Standardization
Extracts from ginger can be prepared in aqueous or organic solvents such as ethanol and essential oils can be prepared by steam distillation. The concentration of 6-gingerol and total phenolics is often used for standardisation for consistent pharmacological activity in the case of ginger preparation [43].
Pharmacological Effects of Ginger in Hepatotoxicity
Antioxidant Activity
Ginger possesses bioactive molecules that possess excellent antioxidant activity, like 4-gingerol, 6-gingediol and 6-gingerol. It boosts the endogenous antioxidants like glutathione peroxidase (GSH-Px), decreases lipid peroxidation (MDA levels) and neutralises free radicals in the liver cells, thus preventing liver damage [71,72].The activities of ginger juice extract were total antioxidant capacity, DPPH radical scavenging and ferric reducing power which prevented liver damage caused by CCl4 and increased the HDL level and decreased the LDL.
Ginger oil resulted in significant increase (31.14%) in the level of serum HDL and significant decrease in serum LDL (55.14%) without any change in serum cholesterol level and significant increase in GSH-Px level (75.06%) which protects the liver from the toxic effect of DEN.
A decrease in the amount of CCl4-induced MDA and liver enzymes [44].
Anti-inflammatory Effects
6-gingerol, 6-shogaol and zingerone are active ingredients of ginger, which inhibit enzymes (cyclooxygenase-2 or COX-2, and lipoxygenase or LOX) that decrease pro-inflammatory mediators such as prostaglandins and leukotrienes. Ginger also prevents the activation of NF-κB, which lessen the inflammation that causes liver damage [44].
A comprehensive review of these effects, coupled with experimental studies, has established that they are linked to COX-2, LOX and NF-κB inhibition.
Anti-fibrotic and Anti-apoptotic Mechanisms
The anti-fibrotic activity of ginger in hepatotoxicity models is less well described in the context provided, but it is known to affect the anti-apoptotic activity by modulating the stress signaling pathways [45].
For instance, decrease in apoptosis by inhibition of stress-activated protein kinase/JNK pathways and increase in survivin (anti-apoptotic protein) by 6-gingerol was observed in cell models, suggesting anti-apoptotic activity, which may indirectly be associated with anti-fibrotic activity by maintaining hepatocytes [45].
Evidence from BDL and Other Liver Injury Models
The hepatoprotective activity is strongly substantiated in various liver damage models. Ginger ameliorated biochemical markers, antioxidant status and histopathology in CCl4 induced hepatotoxicity model, diethylnitrosamine (DEN) induced hepatotoxicity model and ethanol induced fatty liver [46].
These have potential implications in the context of cholestatic and obstructive liver injury as well. Hepatoprotective effects validated in CCl4-induced liver damage and DEN models. Anti-toxic effect on ethanol-induced fatty liver through restoration of antioxidant enzymes and decrease of lipids [47].
PHARMACOGNOSY AND PHYTOCHEMISTRY OF LEMON (CITRUS LIMON)
Botanical Profile
Lemon belongs to Rutaceae family of citrus plants, mainly grown in the Mediterranean region and used in the cosmetic, food and medicine industry [48].
It is characterized by its fragrant rind, succulent flesh and evergreen leaves. There are many species of citrus, in which lemon differs from the others by its sour flesh, caused by the presence of a high amount of citric acid [48].
From the botanical point of view, different ecotypes (Citrus limon var. pompia) exhibit different morphological and phytochemical characteristics significant for the use of the local populations and for the industry [49].
The various parts of plant utilized and significant are fruit peel, fruit juice, seeds and leaves, which contains different phytochemicals with diversified therapeutic properties and industrial value [50].
Bioactive Compounds (Flavonoids, Vitamin C, Limonoids):
Flavonoids, Vitamin C and Limonoids in the context of Bioactive compounds. The lemon is full of bioactive components underlying the pharmacological and nutritional properties given in Table 4.
Table 4: Major Phytoconstituents, their Localization and Pharmacological Effects of Lemon
|
Phytoconstituent Category |
Major Compounds |
Pharmacological Properties |
|
Flavonoids |
Diosmin, Hesperidin, Eriocitrin, Naringin, Neoeriocitrin, Neohesperidin, Stellarin-2, Rhoifolin, Isorhamnetin Derivatives |
Flavonoids exhibit antioxidant, anti-inflammatory, antibacterial, cardioprotective and hepatoprotective activities. |
|
Vitamin C (Ascorbic Acid) |
Ascorbic Acid |
Strong natural antioxidant that neutralizes free radicals, supports the immune system, promotes collagen production and protects against oxidative stress. |
|
Limonoids and Terpenoids |
D-Limonene, β-Pinene, γ-Terpinene, α-Terpineol, Myrcene |
Have antimicrobial activity, anticancer, antioxidant, anti-inflammatory, hepatoprotective and are responsible for the characteristic aroma and essential oil activity. |
|
Phenolic Acids |
Ferulic Acid, Synapic Acid, p-Hydroxybenzoic Acid |
They have antioxidant and anti-inflammatory properties due to their ability to prevent oxidative damage and lipid peroxidation. |
|
Carotenoids |
β-Carotene and Related Pigments |
Antioxidant activity, protection of cells from oxidative damage. |
|
Alkaloids and Other Phytochemicals |
Various Bioactive Alkaloids |
Alkaloids Associated with neuroprotective, antimicrobial, anti-inflammatory, and hepatoprotective effects |
Juice Composition and Standardization
Citrus limon juice contains a matrix of: Volatile oils, Flavonoids, Sugars, Organic acids (citric), Vitamins, and water [51]. The content of bioactives such as vitamin C and flavonoids varies according to genotype, harvesting time and environmental conditions [88,89]. Research on Fino cultivar clones shows that while genetic variation affects phytochemical content, seasonal and environmental factors have more impact on the vitamin C and flavonoidal concentration, and little variation between harvest times [52]. This means that, with specific cultivation and harvesting, bioactives can be consistently produced in the industrial juice production [53]. The extraction methods for lemon peel, which is one of the by-products, impact the extraction of phenolics, flavonoids, ascorbic acid and carotenoids [52]. The best extraction process is aqueous ethanol at mild temperatures that give extracts with a high antioxidant activity and high potential for use in functional foods and cosmetic formulations [53]. This standardisation contributes to valorize the lemon peel as a functional ingredient other than lemon juice [52]. The assays employed in the quality control and standardization of lemon juice include total phenolic content, total flavonoid content, vitamin C content and antioxidant activity assays by DPPH radical scavenging and ferric reducing antioxidant power (FRAP) assays [54]. Lemon juice and products possess a special phytochemical fingerprint of marker flavonoids and limonoids that ensures uniformity and effectiveness in therapeutic and nutritional applications [55].
Pharmacological Effects of Lemon Juice in Hepatoprotection
Antioxidant Potential
The hepatoprotective activity is due to the strong antioxidant property of the lemon juice. Lemon juice significantly suppressed the elevation of serum alanine transaminase (ALT), aspartate transaminase (AST), hepatic triglyceride levels and lipid peroxidation in a mouse model of chronic alcohol-induced liver injury, suggesting a protective effect against the liver damage that occurs in these mice [56]. The antioxidant activity of lemon juice against free radicals and oxidative stress in hepatic tissue was also confirmed in vitro to substantiate its antioxidant activity [57]. This antioxidant activity could be beneficial against the bad guys (reactive oxygen species [ROS] involved in hepatocyte injury) and keep this cell in good shape [57].
Function for Detoxification and Regulation of Bile Flow
Even though no experimental evidence has been found, there are many natural products that have shown hepatoprotective effects and modulate pathways of liver detoxification and bile acid metabolism [58]. The liver plays an important role in the detoxification of xenobiotics and metabolic waste and the activity of the phase I and phase II enzymes is determined by the presence of bioactive compounds in citrus [59]. The flavonoids found in lemon juice such as eriodyctiol, rutin, hesperidin and isorhamnetin can help to express or, in the case of hesperidin, activate the enzymes that detoxify toxins in the liver [60,61]. Hence, modulation of bile acid composition/excretion is another important hepatoprotection strategy and related studies have shown that receptor mediated mechanisms have the capacity to modify the composition of bile acid towards less toxic forms that would benefit the flow of bile and reduction of cholestatic liver injury from lemon phytochemicals [62,63].
Anti-inflammatory Properties
The lemon juice is a source of polyphenolic compounds and flavonoids, which have anti-inflammatory properties, due to their ability to block the pro-inflammatory enzymes and mediators [64]. These phytochemicals inhibit the production of two enzyme systems, cyclooxygenase (COX) and lipoxygenase (LOX), that reduce the production of prostaglandins and leukotrienes that contribute to the inflammation in the liver [65]. The in vitro and in vivo evidence points to the ability of lemon extracts to reduce the production of inflammatory cytokines (TNF-α and interleukins), thus reducing hepatic inflammation and fibrosis. Lemon's antioxidant properties are further complemented by anti-inflammatory properties which offer liver protection and recovery from inflammatory liver diseases [66].
Experimental Evidence in Liver Injury
Several experimental studies using different liver injury models substantiate the hepatoprotective effect of lemon juice and its extracts [67]. The protective effects of eriodyctiol, rutin, hesperidin, isorhamnetin from lemon juice extract was observed in the liver damage induced in rats by CCl4 and the serum level of liver enzymes and antioxidants were reduced [68]. Histological examination revealed attenuation of hepatic necrosis and inflammation which demonstrates the hepatoprotective activity of lemon against chemical induced hepatotoxicity [69].
Lemon juice reduced the lipid accumulation in liver tissue (including lipid peroxidation) and the accumulation of triglycerides in liver tissue in chronically injured mice produced by alcohol consumption when given orally [70]. It was also found to have beneficial effects on biochemical markers (ALT, AST) and restoration of histopathological changes (steatosis, inflammatory cell infiltration) [71]. Lemon juice dose-dependently exhibited hepatoprotection, which was linked to increased antioxidant potential of lemon juice [72].
The oxalate, rich in polyphenolic compounds, and flavonoids, found in lemon extracts, have been shown to exert beneficial effects on parameters of oxidative stress, inflammation, and metabolic dysfunction in animal models, highlighting the potential of citrus derivatives for the treatment of liver disease and metabolic dysfunction [73].
Taken together these results highlight the potential hepatoprotective effects of lemon juice by its antioxidant, anti-inflammatory and/or detoxification-enhancing properties observed in chemically and metabolically induced liver injury models [74].
Synergistic Effects of Ginger and Lemon Juice
Mechanistic Synergy
Take advantage of herbs synergism in hepatoprotection, obtained from complementary bioactive compounds of ginger (Zingiber officinale) and lemon juice (Citrus limon), both with anti-oxidative stress and anti-inflammatory activity working on several pathways [75].
Lemon juice is also rich in flavonoids like eriodyctiol, rutin, hesperidin and isorhamnetin, compounds that have strong antioxidant and anti-inflammatory properties; ginger is also very rich in phenolic compounds such as 4-gingerol, 6-gingediol and 6-gingerol which strengthen antioxidant defenses by enhancing the activity of glutathione peroxidase (GSH-Px) and reducing serum liver enzymes (ALT and ALP) [76].
The combination of these phytochemicals gives a greater antioxidant capacity, antiradical activity and ferric reducing power compared to their individual effects, and scavenges reactive oxygen species (ROS) and prevents oxidative damage to hepatocytes [77].
Their mechanistic synergy involves regulation of key cellular signaling pathways that underlie oxidative stress and inflammation as well [78]. The components of ginger, for instance, inhibit the action of enzymes like cyclooxygenase-2 (COX-2) and lipoxygenase (LOX) while lemon flavonoids can block pro-inflammatory mediators and nuclear factor-kappa B (NF-κB) activation, both of which help reduce inflammation [78].
This double inhibition allows to inhibit the production of cytokines and infiltration of inflammatory cells in the liver tissue, preserving the liver architecture and functions [80]. These multiple effects indicate Ginger + Lemon juice has complementary and potentiated actions [81].
Combined Antioxidant and Anti-inflammatory Actions
The several bioactive compounds present in ginger and lemon juice act together to combat free radicals, thus providing them with potent antioxidant properties [82]. For instance, essential oils and dry extract of ginger increase the serum HDL and decrease LDL, in addition to increasing the enzymes that are antioxidants like GSH-Px [83]. Lemon juice and ginger both contain antioxidants, with lemon juice being high in Vitamin C and polyphenols, which together with the antioxidants found in ginger, increase the overall antioxidant activity as measured by antioxidant assays like DPPH and Ferric Reducing Antioxidant Power (FRAP) [84].
They act together to restore redox balance more effectively with a reduction in the lipid peroxidation and oxidative stress damage to the liver. The blends are more effective than the single extracts on inflammatory signaling activity. Ginger's 6-gingerol and 6-shogaol block the synthesis of inflammatory enzymes such as COX-2 and LOX and lemon juice flavonoids block the activation of NF-κB, a protein that reduces the production of tumour necrosis factor-alpha (TNF-α) and interleukins. These two blocks have been shown to cause significant decrease in inflammation, infiltration of neutrophils and fibrosis in experimental models, which are all critical steps in the progression of liver disease. The synergistic anti-inflammatory activities are important to keep liver cells healthy against the effect of toxins like CCl4.
Multiple Data Sources from Combined Therapy Studies:
The combined effect of ginger and lemon juice extract has been reported to have enhanced hepatoprotection in liver injury models induced by CCl4 in the past. The results of the combined treatment were significant for biochemical parameters: a significant reduction in serum activities of ALT, AST and alkaline phosphatase as compared to monotherapies. Histopathological results revealed a lesser degree of hepatic necrosis and infiltration of inflammatory cells with both juices combined. Importantly, the total antioxidant activity and the scavenging capacity of combined group showed a better antioxidant capacity than other groups in antioxidant assays, thus presenting clear evidence of additive or synergic effect.
Moreover, the combination of ginger and lemon juice at different concentrations was found to be more effective in preventing chronic liver damage as compared to either alone in clinical practice, which could be considered as an adjuvant or alternative hepatoprotective treatment. The effect reported in this study has not been completely delineated at a cellular and molecular level, but it suggests that this combination might constitute a natural treatment strategy to counteract oxidative stress and inflammation in the liver.[85,86]
Molecular Mechanisms of Herbal Hepatoprotection:
Ginger and lemon juice are two herbal medicines, and have been shown to have hepatoprotective activity with several molecular mechanisms.[13087] The majority of mechanisms involved are anti-hepatotoxic (due to oxidation, inflammatory, fibrogenic, apoptotic and regulation of gene and protein expression pathways mostly mediated by bile duct obstruction).[87]
Modulation of Oxidative Stress Pathways:
The mechanisms of modulation of oxidative stress pathways will be discussed. Pathways of oxidative stress will be discussed and Modulated. Liver tissues in bile duct ligated (BDL) rats have higher levels of oxidative stress parameters, such as reactive oxygen species (ROS), lipid peroxidation (malondialdehyde, MDA) and DNA oxidation (8-hydroxy-2'-deoxyguanosine, 8-OHdG).[88] This oxidative damage results in liver damage and mitochondrial dysfunction.[88]
The active ingredients of ginger such as [6]-gingerol are highly active antioxidants which neutralize ROS, and enhance the activity level of endogenous antioxidant defense enzyme such as superoxide dismutase (SOD), catalase and glutathione peroxidase.[89] These effects reduce the markers of oxidative stress, while improving mitochondrial function.[89] In addition, lemon juice is rich in Vitamin C and flavonoids — it has antioxidant activity and helps body cells and other components neutralise the free radicals, thereby preventing oxidative damage to the body.[90]
Regulation of Inflammatory Signalling:
In chronic liver injury due to bile duct obstruction, chronic inflammation occurs, which is mainly mediated by nuclear factor kappa B (NF-κB) and mitogen-activated protein kinase (MAPK) pathways leading to increased pro-inflammatory cytokines (eg. Tumor necrosis factor α (TNF-α), Interleukin (IL-1β), and IL-6).[90]
Active ingredients of ginger block NF-κB activation and downstream signaling pathways, which in turn block the production of inflammatory cytokines and infiltration of inflammatory cells.[90] Further, [6]-gingerol has been found to inhibit the Toll-like receptor 4 (TLR4)/MAPK/NF-κB pathway, which helps to reduce inflammation.[90] Lemon juice could also help to regulate inflammation by its flavonoids that help to decrease the production of cytokines and inhibit cyclooxygenase-2 (COX-2), which is another way that it helps to reduce liver inflammation.[91]
Selective activation of STAT1 has also been shown to have anti-inflammatory and anti-fibrotic effects of similar magnitude by modulators such as rilpivirine, leading to the notion that cytokine signalling is an important target for liver protection and regeneration.[91]
Effects on Fibrogenesis and Apoptosis:
The activation and proliferation of hepatic stellate cells (HSCs) causing them to produce extracellular matrix proteins, including collagen types I and III, is the source of liver fibrosis.[92] Liver fibrosis is caused by activation and proliferation of hepatic stellate cells (HSCs) which produce the proteins of the extracellular matrix (ECM), such as collagen types I and III, under the influence of transforming growth factor (TGF)-beta 1.[92] In bile duct obstruction, TGF-β1 and fibrogenic gene expression is elevated, which results in an increase in fibrogenesis and hepatotoxicity.[93]
Ginger also inhibits the activation and proliferation of HSCs, as well as the expression of TGF-β1 and collagen synthesis, thereby inhibiting fibrosis. It also helps hepatocyte survival by suppressing the ratio of Bax/Bcl-2 and activation of caspase-3 to prevent mitochondrial-mediated hepatocyte apoptosis, thereby maintaining liver tissue integrity.[94] Lemon's antioxidant properties work in a similar manner to anti-apoptotic properties, which help to prevent cell death due to oxidative stress. Furthermore, pharmacological inhibition of apoptosis (experimental using pan-caspase inhibitors) has been shown to decrease hepatocyte apoptosis and subsequent fibrosis, making control of programmed cell death pathways an important mechanism to minimise liver damage.[95]
Gene Expression and Protein Targets:
Herbal hepatoprotection can be made up of modulation of genes and proteins involved in oxidative stress, inflammation, fibrogenesis and apoptosis:[96]
• Upregulation of genes that encode antioxidant enzymes for greater ROS clearance (catalase, SOD, glutathione peroxidases).
• Fibrogenic markers: Collagen I/III gene expression is reduced and expression of the gene for TGF-β1 is reduced, which reduces the amount of extracellular matrix.
• Inflammation and fibrogenesis are inhibited by the block of NF-κB, TLR4, MAPKs (p38, ERK1/2) and STAT3 activation while the selective activation of STAT1 induces apoptosis of activated HSCs which promotes liver regeneration.
These molecular targets are affected by ginger and lemon juice, which helps restore hepatic redox balance, block profibrotic signaling and induce hepatocyte viability.
BIOCHEMICAL AND HISTOPATHOLOGICAL EVALUATION:
Liver Function Tests (ALT, AST, ALP, Bilirubin):
Liver function tests are significant to evaluate hepatocellular damage in hepatotoxicity associated with bile duct obstruction. Raised serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP) and bilirubin are indicative of hepatocyte membrane injury and cholestasis.[97]
Each of these herbal agents in studies comparing ginger and lemon juice, significantly normalized these enzymes. For instance, treatment with 6-gingerol decreased the increase in ALT, AST, and ALP levels that occurred in DEN treated rats, thus demonstrating hepatoprotection by maintenance of membrane integrity and enzymatic activity. Similarly, after giving lemon juice, ALT and AST were brought to normal levels reflecting that lemon juice has protective action against liver damage. The elevated level of ALT and AST in the acetaminophen induced toxicity model was also reduced by the ginger extract or ginger nanoparticles confirming the improved liver function.[98]
Oxidative Stress Markers (SOD, GSH, MDA):Oxidative Stress Markers (OSMs) are markers of the ratio of pro-oxidant damage/anti-oxidant defence. Common dangers in bile duct obstruction are increased lipids peroxidation and decreased antioxidant levels such as superoxide dismutase (SOD) and reduced glutathione (GSH).[99]
Ginger + lemon juice treatment enhances antioxidant enzyme activities and decreased oxidative damage. Ginger extract also showed antioxidant effect with enhancement of catalase activity and reduction in MDA in acetaminophen induced hepatotoxicity in rats and Lemon juice also reduced the level of MDA and increased the antioxidant status in alcohol induced hepatotoxicity in mice.[100] Such changes are key to restore redox balance and to prevent liver damage caused by oxidations.[100]
Inflammatory Markers (TNF-α, IL-6):
Increased levels of pro-inflammatory cytokines (such as tumour necrosis factor alpha (TNF-α) and Interleukin-6 (IL-6)) also characterize cholestatic liver injury.[100]
Using experimental liver injury model studies, it was found that 6-gingerol was highly effective in down-regulating the expression of the two pro-inflammatory cytokines, namely, IL-6 and TNF-α.[100] Ginger's wide anti-inflammatory activity comprises down-control of NF-κB signaling and downstream cytokine manufacturing, leading to decreased hepatic inflammation.[100] Comparable effects of lemon juice on the reduction of inflammatory mediators in bile duct injury models are less reported; however, the well-established antioxidant and anti-inflammatory properties of lemon juice suggest it may also have similar effects on reducing inflammatory mediators in these models.[101]
Histopathological Changes:
The degree and preservation of liver damage and healing can be confirmed histologically. The presence of hepatocyte necrosis, inflammatory infiltration, fibrosis, congestion, edema, and disturbance of liver architecture is often identified in the case of bile duct obstruction and chemically-induced liver damage by histology. These pathological changes were completely reversed by ginger and lemon juice treatment. [102]
Challenges and Limitations
One of the major challenges in evaluating the hepatoprotective effects of ginger and lemon juice is the considerable variability in herbal preparations. Differences in plant origin, cultivation conditions, harvesting practices, extraction techniques, and concentrations of bioactive constituents can significantly influence the therapeutic efficacy of herbal products. Such variability often leads to inconsistent findings within and across studies, thereby limiting the reproducibility and comparability of research outcomes. Another important limitation is the lack of robust clinical evidence. Although numerous preclinical studies have demonstrated the beneficial effects of ginger and lemon juice against bile duct obstruction (BDO)-induced hepatotoxicity, well-designed clinical trials in human subjects remain limited. This gap in clinical validation restricts the ability to draw definitive conclusions regarding their efficacy, safety, and therapeutic applicability in patients with cholestatic liver diseases. Furthermore, most available evidence is derived from animal and in vitro models, which may not accurately reflect the complexity of human liver pathophysiology. Experimental models often differ from human conditions in terms of metabolism, immune responses, disease progression, and drug dosage requirements. Therefore, caution is necessary when extrapolating preclinical findings to clinical settings [103].
Future Perspectives and Research Directions
Future research should focus on conducting large-scale, well-designed randomized controlled trials to evaluate the therapeutic efficacy, safety, optimal dosage, and pharmacokinetic properties of ginger and lemon juice in patients with cholestatic liver disorders. Clinical validation is essential for establishing evidence-based recommendations and identifying potential adverse effects or herb–drug interactions that may not be apparent in preclinical studies. Advanced molecular investigations are also needed to better understand the mechanisms underlying the hepatoprotective effects of these herbal interventions. Emerging approaches such as systems biology, network pharmacology, multi-omics technologies, and artificial intelligence-driven analyses can provide comprehensive insights into the complex molecular pathways influenced by bioactive compounds. These techniques may facilitate the discovery of novel therapeutic targets and contribute to the development of personalized treatment strategies. Another important area of future research is the standardization and quality control of herbal products. Variations in cultivation practices, environmental conditions, harvesting methods, and processing techniques can affect the composition and biological activity of herbal preparations. Therefore, implementing Good Agricultural Practices (GAP), Good Manufacturing Practices (GMP), rigorous phytochemical characterization, and contaminant screening is crucial for ensuring product consistency, efficacy, and safety. The successful integration of ginger and lemon juice into modern therapeutic approaches will require strong scientific evidence and interdisciplinary collaboration. Combining traditional medicinal knowledge with advances in pharmacology, toxicology, and clinical medicine may help establish these herbal interventions as effective complementary therapies for cholestatic liver diseases. Such efforts could support the development of standardized treatment guidelines and enhance the acceptance of evidence-based herbal medicine in mainstream healthcare [104,105].
CONCLUSION
Ginger and lemon juice exhibit significant hepatoprotective effects against bile duct obstruction (BDO)-induced liver injury through their antioxidant, anti-inflammatory, antifibrotic, and antiapoptotic properties. Preclinical studies have consistently demonstrated their ability to reduce liver damage and preserve hepatic function. However, their clinical application remains limited due to variability in herbal preparations, lack of standardization, and insufficient clinical evidence. Furthermore, differences between experimental models and human liver disease present challenges for translating preclinical findings into clinical practice. Future research should focus on well-designed clinical trials, advanced molecular investigations, and standardized quality-control measures to validate their efficacy and safety. With further scientific validation, ginger and lemon juice may serve as promising complementary therapies for the management of BDO-induced hepatotoxicity.
REFERENCES

Shubhangi Bhadane, Dr. Kiran Kotade, Sangita Bhandare, Dr. Amol More, Comprehensive Review of Herbal Interventions in Bile Duct Obstruction-Induced Hepatotoxicity: Insights from Ginger and Lemon Juice, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 4126-4151, https://doi.org/10.5281/zenodo.20729934
 10.5281/zenodo.20729934
10.5281/zenodo.20729934