
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Shri Dhaneshwari Manav Vikas Mandal’s DR. Vedprakash Patil Pharmacy College, Georai Tanda, Chh. Sambhajinagar 431003
Topical delivery systems remain a foundational approach in managing dermatological conditions, preventing sepsis, and accelerating wound healing. Antiseptic creams are specialized semisolid emulsions designed to safely apply antimicrobial agents to living tissue. This review provides a comprehensive analysis of the formulation, manufacturing methodologies, and multi-parametric evaluation protocols for both synthetic and herbal antiseptic creams.We systematically detail the classification systems of topical emulsions and classify active antimicrobial agents according to their chemical structure and mechanisms of action. This paper outlines the functional roles of essential excipients—including aqueous phases, oil phases, emulsifying agents, humectants, and stabilizers. It describes standard preparation methods, such as the fusion and cold emulsification methods.Furthermore, this review explores key evaluation parameters, detailing physicochemical tests (pH, rheology, spreadability), physical stability tracking (phase separation, thermal stress testing), and in vitro microbiological assays (agar well diffusion, minimum inhibitory concentration). This comprehensive review serves as a technical reference for designing, optimizing, and quality-assuring stable, effective, and non-irritating topical antiseptic preparations.
Topical creams represent a fundamental class of semisolid dosage forms within pharmaceutical science, defined pharmacopeially as viscous, liquid, or semisolid biphasic emulsions engineered specifically for external application to either the skin or accessible mucous membranes. Structurally, these systems are characterized by a heterogeneous distribution of two mutually immiscible liquid phases: a lipophilic (oil) phase and a hydrophilic (aqueous) phase. [4] One phase is physically fragmented into microscopic droplets—referred to as the internal or dispersed phase—and distributed uniformly throughout the continuous or external phase. This structural architecture is thermodynamically unstable due to the high interfacial tension between the oil and water molecules. To prevent natural degradation processes such as coalescence, flocculation, and phase separation, the system requires the addition of amphiphilic emulsifying agents. These agents line the interfacial boundaries, lowering surface tension and forming a mechanical or electrostatic barrier that keeps the droplets suspended.[8]
From a functional perspective, creams serve as vital vehicles within modern topical drug delivery frameworks. Their primary purpose is to evenly distribute active pharmaceutical ingredients (APIs) across human skin, ensuring that therapeutic agents are spread consistently over the target surface. The physical structure of a cream is carefully optimized to control how the encapsulated drug is released. When applied, the continuous phase of the cream interacts with the skin’s surface, while the dispersed droplets act as micro-reservoirs that gradually release the API. By altering the balance of the oil and water phases, formulation scientists can tailor the cream's properties. For instance, oil-in-water (O/W) systems offer a non-greasy feel and wash off easily with water, making them ideal for acute conditions. Conversely, water-in-oil (W/O) systems provide an emollient, protective barrier that slows down drug release, which is highly beneficial for treating chronic, dry skin conditions.[10]
The Biological Barrier of Human Skin and Microbial Threats
The human skin is the body's largest organ, serving as a complex, multi-layered biological barrier that shields internal physiological systems from a wide range of environmental threats. This vital barrier protects against mechanical trauma, ultraviolet radiation, and pathogenic invasion. Structurally, this protective function is driven by the outermost layer of the epidermis, known as the stratum corneum. Often described using a "brick-and-mortar" model, the stratum corneum consists of flattened, protein-rich dead cells (corneocytes, the "bricks") tightly embedded within a highly organized extracellular matrix of lipids (ceramides, cholesterol, and free fatty acids, the "mortar"). This unique architecture creates a highly effective waterproof seal that prevents transepidermal water loss and blocks harmful external pathogens from entering the body. [11]
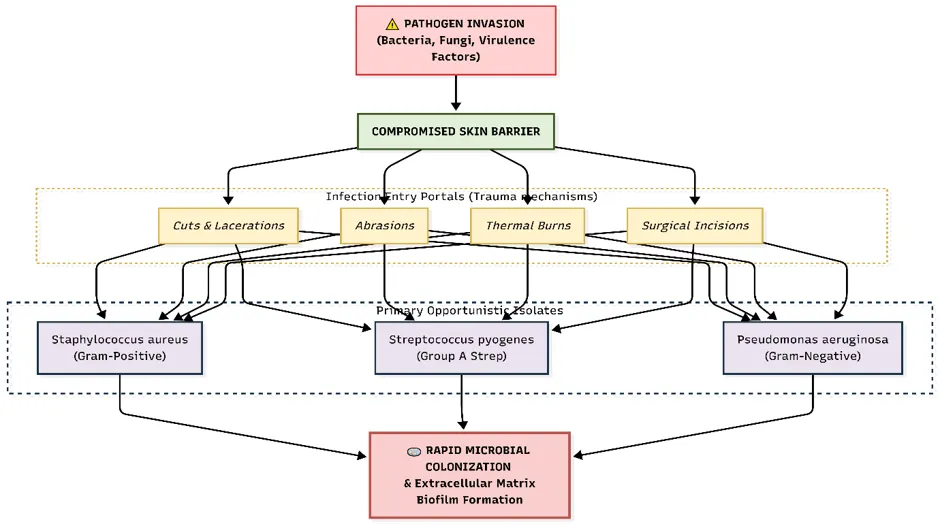
Fig: The Biological Barrier of Human Skin and Microbial Threats
2. CLASSIFICATION OF TOPICAL CREAMS
Topical creams are categorized primarily by the spatial configuration of their immiscible phases and their specific therapeutic or cosmetic functions.
2.1 Physicochemical Classification (Phase Structure)
Emulsions are thermodynamically unstable systems consisting of at least two immiscible liquid phases [6]. One phase is dispersed as droplets (the internal or dispersed phase) throughout the other (the external or continuous phase), stabilized by an emulsifying agent.
2.2 Functional Classification
3. APPLICATIONS, ADVANTAGES, AND DISADVANTAGES
3.1 Therapeutic Applications
3.2 Advantages of Antiseptic Creams
3.3 Disadvantages and Limitations
4. MATERIALS USED IN FORMULATING ANTISEPTIC CREAMS
4.1 Active Antiseptic Agents (APIs)
Active agents are selected based on their antimicrobial spectrum, skin compatibility, and structural stability within the emulsion framework.
4.1.1 Synthetic Antiseptics
4.1.2 Natural/Herbal Antiseptics
4.2 Structural Excipients and Additives
|
Material Classification |
Common Examples |
Functional Role in Formulation |
|
Aqueous Vehicle |
Purified Water, Deionized Water |
Forms the continuous phase in O/W systems; acts as a solvent for hydrophilic active ingredients, preservatives, and water-soluble additives. |
|
Oil Phase / Emollients |
Liquid Paraffin, Stearic Acid, Cetyl Alcohol, Beeswax, Isopropyl Myristate |
Forms the lipophilic matrix; dictates viscosity, establishes an occlusive barrier to prevent moisture loss, and modifies emollient properties [12]. |
|
Emulsifying Agents |
Anionic: Sodium Lauryl Sulfate Cationic: Cetrimide Non-ionic: Tween 60, Span 80, Cetomacrogol 1000 |
Lowers interfacial tension between oil and water phases; forms a mechanical or electrostatic barrier at the droplet interface to prevent coalescence. |
|
Humectants |
Glycerol, Propylene Glycol, Sorbitol |
Retains water within the vehicle to prevent the cream from drying out; promotes hydration of the stratum corneum upon application [4]. |
|
Preservatives |
Methylparaben, Propylparaben, Sodium Benzoate, Phenoxyethanol |
Prevents microbial proliferation within the high-water environment; ensures product safety throughout its shelf life [5]. |
|
Antioxidants |
Tocopherol (Vitamin E), Butylated Hydroxytoluene (BHT), Ascorbyl Palmitate |
Prevents oxidative rancidity of the unsaturated lipid components within the oil phase. |
|
Buffering/ Neutralizing |
Citric Acid, Triethanolamine, Sodium Phosphate buffers |
Adjusts and maintains the formulation pH within the skin-compatible range ($5.0\text{to} 7.0$) to ensure stability and reduce irritation [12]. |
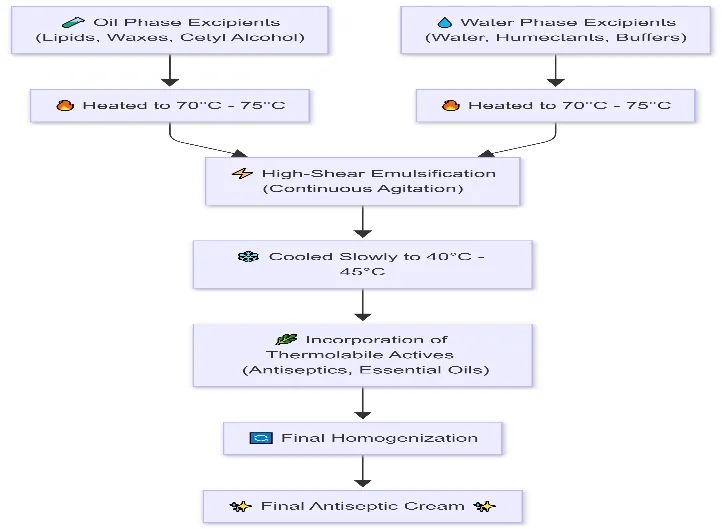
Formulation Of Antiseptic Creams
Evaluation Tests for Antiseptic Creams
To ensure therapeutic efficacy, physical uniformity, consumer acceptability, and long-term stability, formulated antiseptic creams must undergo rigorous, multi-parametric quality control testing.
6.1 Physical and Physicochemical Evaluation
A. Appearance and Organoleptic Properties
The cream is visually inspected under standardized lighting conditions against a white background to evaluate basic sensory parameters:
B. pH Determination
Because human skin maintains a slightly acidic surface pH (4.5 text to 6.0) to support its protective acid mantle, topical formulations must be carefully balanced. The pH is measured using a calibrated digital pH meter. A 10% w/v aqueous dispersion of the cream is prepared by dispersing 10 g of the formulation in 90 mL of distilled water under mild agitation. The glass electrode is immersed into the dispersion, and the reading is allowed to stabilize. The ideal target pH range for an antiseptic cream is 5.0 text to 7.0 to ensure compatibility with the skin barrier and minimize the risk of tissue irritation or chemical dermatitis [7, 12].
C. Viscosity and Rheological Profile
Viscosity is quantified using a rotational viscometer (e.g., Brookfield viscometer) with a suitable spindle (such as T-bar spindles) at varying rotational speeds at 25°C. Viscosity data are critical because they directly impact several product characteristics:
D. Spreadability
Spreadability measures the ease with which a cream applies to skin or affected tissues. It is quantified using a parallel-plate apparatus. A designated volume of cream is placed between two ground glass slides. A specified weight is applied to the upper slide, compressing the cream into a uniform circle. The upper slide is then pulled along a fixed distance by a suspended weight. The time taken for the slides to separate completely is recorded.
[3]. A higher spreadability value indicates that the product spreads easily with minimal mechanical pressure, which is ideal when treating painful or tender wound sites.
E. Extrudability Test
This test measures the ease with which the cream is expelled from its final packaging. Standard collapsible aluminum or plastic tubes are filled with the formulation and sealed. A constant weight or uniform mechanical force is applied to the crimped base of the tube. The weight of the cream extruded through the nozzle over a set period is quantified. Optimal extrudability ensures that the consumer can smoothly remove the product from the packaging without requiring excessive force..
F. Washability
Washability evaluates how easily the product can be removed from the skin after use, which directly affects patient compliance. A small amount of cream is applied to a designated area of the forearm. It is then washed under a gentle stream of tap water at 25text °C without vigorous scrubbing. O/W formulations should wash away cleanly without leaving a greasy, water-resistant residue.
7. Microbiological Evaluation Protocols
Topical antiseptic creams must demonstrate clear antimicrobial efficacy against standard target pathogens. Agar well diffusion method is The assay provides a qualitative and semi-quantitative measure of antimicrobial activity against a standard panel of pathogens:
7.3 Determination of Minimum Inhibitory Concentration (MIC)
The MIC represents the lowest concentration of the active formulation that completely prevents visible microbial growth. To determine the MIC of a semisolid cream, a standard weight of the product is extracted into an appropriate solvent system (such as PBS containing 0.1% Tween 80). This stock extract undergoes serial two-fold dilutions in sterile nutrient broths within a 96-well microtiter plate.
Each well is inoculated with a standardized bacterial culture and incubated at 37°C for 24 hours. The wells are then inspected visually for turbidity or analyzed spectrophotometrically at 600 nm. A lower MIC value indicates higher antimicrobial potency, allowing the formulation to remain effective even when diluted by wound exudates.
7.5 In Vitro Antimicrobial Activity via Direct Inoculation
This test simulates real-world use by evaluating antimicrobial performance directly within the cream matrix. The formulation itself is inoculated with a known concentration of test organisms The inoculated product is stored at 22°C. Samples are taken at designated intervals (such as Day 1, 7, 14, and 28), neutralized, and plated for viable counts. This protocol helps verify that the active antiseptic remains available and functional within the complex lipid matrix over time, rather than becoming trapped or inactivated by the emulsifying agents.
8. Stability Studies and Stress Testing
Topical creams must maintain their chemical composition and physical structure throughout their designated shelf life. Stability studies are conducted in compliance with International Council for Harmonisation (ICH) Q1A(R2) guidelines [14].
8.1 Environmental Testing Conditions
Formulated creams are stored in final commercial packaging inside environmental stability chambers under two primary stress conditions:
8.2 Evaluated Parameters
Samples are withdrawn at specific intervals (0, 1, 2, 3, and 6 months) and evaluated across several parameters to detect early signs of degradation:
9. Future Trends in Antiseptic Cream Formulations
Recent advances in topical drug delivery focus on improving stability and control over active ingredient release.
10. CONCLUSION
The successful design of an antiseptic cream depends on carefully selecting active antimicrobial agents and balancing them within a stable, non-irritating emulsion base. Oil-in-Water (O/W) systems remain preferred for most acute applications due to their high patient acceptability, cooling properties, and ease of washing. This review highlights that incorporating rigorous physicochemical, thermal, and microbiological evaluations into early-stage development is essential for producing topical formulations that meet modern clinical standards.
REFERENCES



Mayur Narode, Vaishnavi Pawar, Dipali Hamde, Comprehensive Review on the Formulation and Evaluation of Antiseptic Creams, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 7539-7548. https://doi.org/10.5281/zenodo.21054614
 10.5281/zenodo.21054614
10.5281/zenodo.21054614