
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
(Laureate Institute of Pharmacy), Kathog, Himachal Pradesh India (176031)
Dermatophytosis is a common superficial fungal infection affecting keratinized tissues such as skin, hair, and nails, with a growing global burden exacerbated by the rapid emergence of antifungal resistance. Conventional antifungal therapies, including azoles, allyl amines, and griseofulvin, though effective, are often associated with adverse effects, high treatment costs, prolonged therapy, and increasing rates of treatment failure due to resistant dermatophyte strains such as Trichophyton indotineae. These limitations necessitate the exploration of safer and more effective alternative therapeutic approaches. Medicinal plants have long been recognized as rich sources of bioactive compounds with antifungal potential and fewer side effects. This review comprehensively discusses the classification, pathophysiology, and current treatment strategies for dermatophytosis, with a special emphasis on antifungal resistance mechanisms. Furthermore, it highlights the anti-dermatophytic efficacy of various herbal compounds and phytochemicals, including turmeric (Curcuma longa), aloe vera (Aloe barbadensis), garlic (Allium sativum), neem (Azadirachta indica), black pepper (Piper nigrum), and henna (Lawsonia inermis). These natural agents exhibit antifungal activity through diverse mechanisms such as disruption of fungal cell membranes, inhibition of ergosterol biosynthesis, induction of oxidative stress, and immunomodulatory effects. Owing to their safety, accessibility, affordability, and broad-spectrum activity, herbal therapies represent promising alternatives or adjuncts to conventional antifungal treatments. Further preclinical and clinical studies are essential to validate their efficacy and facilitate their integration into modern antifungal management.
Dermatophytosis refers to a widespread superficial fungal infection caused by a specific group of fungi collectively known as dermatophytes. Clinically, it manifests in multiple forms, including tinea corporis, tinea pedis, and tinea capitis (1). Dermatophytes were among the earliest microorganisms identified as human pathogens and are characterized by their unique ability to invade keratinized tissues of humans and animals, resulting in dermatophytic infections. Taxonomically, all dermatophyte species are classified under the family Arthrodermataceae, which comprises nine genera. Among these, Trichophyton, Microsporum, and Epidermophyton are most frequently associated with infections in humans. Globally, Trichophyton rubrum remains the predominant anthropophilic species responsible for the majority of dermatophytic infections. Nevertheless, notable geographical and population-based variations have been observed, with a recent rise in infections caused by zoophilic species such as Microsporum canis and Trichophyton mentagrophytes, potentially linked to increased contact between humans and animals (3). Dermatophytosis contributes substantially to healthcare expenditure at both community and hospital levels, particularly in resource-limited and developing regions where fungal infections are highly prevalent. Furthermore, the increasing incidence of resistance to commonly used antifungal agents has made management more challenging. Conventional antifungal therapies are often associated with adverse effects, prompting a growing interest in alternative therapeutic options. In recent years, considerable attention has been directed toward natural products possessing antifungal activity. Medicinal plants have long served as valuable therapeutic resources and are known to contain a wide range of biologically active constituents (4).
Based on disease severity, dermatophytosis is managed using topical and systemic antifungal agents, administered either individually or in combination. Commonly prescribed topical therapies include allyl amines such as terbinafine and naftifine, along with azole derivatives including clotrimazole, bifonazole, sulconazole, miconazole, sertaconazole, eberconazole, econazole, oxiconazole, and luliconazole, all of which are considered effective in treating dermatophytic infections (11). Among these, topical allyl amines—particularly terbinafine—have demonstrated superior cure rates and reduced treatment duration compared to azole formulations. In clinical practice, fixed-dose combinations (FDCs) containing corticosteroids and antifungal agents are frequently prescribed. Although corticosteroids offer rapid symptomatic relief by suppressing inflammation, their inappropriate use may promote self-medication. Excessive or irrational use of FDCs and topical antifungals has been implicated in the increasing prevalence of drug-resistant dermatophytosis (5). Several first-line antifungal agents, including meglumine antimoniate and sodium stibogluconate, suffer from limitations such as prolonged treatment courses, toxicity concerns, and the emergence of resistant fungal strains. These challenges emphasize the urgent need for safer, more effective, and economically feasible therapeutic alternatives. Berberis vulgaris (family Berberidaceae), commonly known as barberry, is widely distributed across Asia and Europe and is referred to as “Zereshk” in Persian. Native to south-eastern Iran, various parts of this plant—including the roots, bark, leaves, and fruits—have been traditionally employed for the management of numerous ailments, including cardiovascular, gastrointestinal, respiratory, dermatological, urinary tract, and infectious disorders. Scientific studies have demonstrated that B. vulgaris and its principal bioactive constituent, berberine, exhibit notable antifungal activity against Candida species. Furthermore, different extracts of B. vulgaris and berberine have shown promising efficacy against pathogenic dermatophytes such as Trichophyton mentagrophytes, Trichophyton rubrum, Microsporum canis, and Microsporum gypseum (1).
Classification of Dermatophytes
Dermatophytic infections are predominantly caused by three major genera, namely Trichophyton, Microsporum, and Epidermophyton. In addition to these, certain provocations and non-dermatophyte filamentous fungi (NDFF) may also be involved in superficial fungal infections. The classification and nomenclature of dermatophytes are traditionally based on their sexual (teleomorphic) stages (6). At present, the asexual (anamorphic) forms of dermatophytes belonging to the genera Epidermophyton, Microsporum, and Trichophyton are placed under the class Hyphomycetes within the phylum Deuteromycota. In contrast, the sexual forms—primarily associated with zoophilic and geophilic species of Microsporum and Trichophyton—are classified under the genus Arthroderma, order Onygenales, phylum Ascomycota (7). Tinea corporis is most frequently associated with Trichophyton rubrum, Trichophyton tonsurans, and Microsporum canis. Among these, T. rubrum is recognized as the most prevalent etiological agent of dermatophytosis worldwide and represents the leading cause of tinea corporis in North America. Infections of tinea corporis arising secondary to tinea capitis are commonly attributed to T. tonsurans (8). Based on their ecological niche and primary source of infection, dermatophytes are broadly classified into anthropophilic, zoophilic, and geophilic species (9).
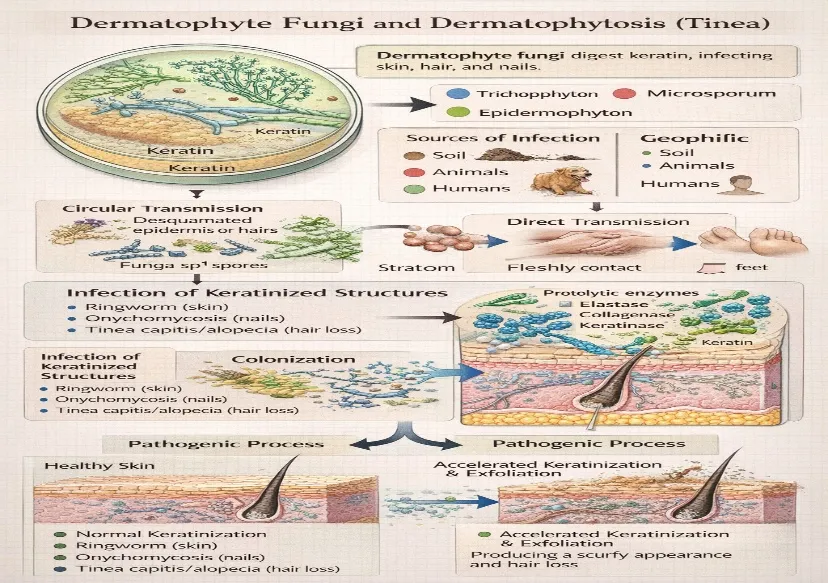
Pathophysiology of Ringworm
the genera Trichophyton, Microsporum, and Epidermophyton. They are further grouped according to their natural reservoirs into geophilic species originating from soil, zoophilic species associated with animals, and anthropophilic species adapted to human hosts. Infection is transmitted either indirectly through contact with contaminated skin scales or hair fragments, or directly via close skin-to-skin contact. Dermatophytosis, commonly referred to as tinea, affects the skin and other keratinized tissues such as hair and nails. Cutaneous lesions typically present as annular plaques with central clearing, giving rise to the characteristic “ringworm” appearance. Inflammatory responses observed during infection may be enhanced by the release of fungal proteolytic enzymes, including keratinases, collagenases, and elastases, particularly in severe cases (10). The persistence of dermatophytes within the keratinized layer has been linked to restricted iron availability, which may also explain the tendency for spontaneous resolution through host inflammatory mechanisms involving iron-binding proteins and enzymatic defense barriers. The infection process begins with fungal colonization of the stratum corneum, usually provoking minimal initial host response. Progressive infection may result in hyperkeratosis, increased desquamation, scaling, and alopecia due to excessive keratin production and shedding (11).
Current Antifungal Therapies
Griseofulvin was the earliest orally administered drug introduced for the management of dermatophytic infections. It was discovered in 1958 by Professor Jimmy Gentles, who reported that an antibiotic derived from Penicillium griseofulvum exhibited antifungal activity against dermatophytes. Despite the later introduction of azole antifungals and terbinafine, griseofulvin continues to be used in combination with these agents. A wide range of antifungal therapies is currently available for the treatment of tinea infections. Management of tinea corporis, tinea cruris, tinea pedis, and tinea manuum primarily involves topical therapy. Numerous topical dosage forms are available, including creams, gels, ointments, and medicated soaps. Commonly prescribed topical agents include azole antifungals such as clotrimazole, miconazole, econazole, and oxiconazole. Allylamine antifungals, including terbinafine and naftifine, are also widely utilized. Systemic antifungal therapy is generally reserved for cases of onychomycosis and tinea capitis. However, available evidence indicates that topical treatments such as ciclopirox and amorolfine may be beneficial in mild cases of onychomycosis. Frequently used topical agents for tinea pedis and tinea manuum include terbinafine, butenafine, miconazole, econazole, ketoconazole, clotrimazole, oxiconazole, and ciclopirox. In cases where infection persists or fails to respond adequately, oral antifungal therapy may be required. Terbinafine, butenafine, econazole, miconazole, ketoconazole, clotrimazole, and ciclopirox are commonly employed topical options for tinea corporis and tinea cruris (12). Treatment of Candida infections in otherwise healthy individuals typically involves topical azole agents or polyene antifungals such as nystatin and amphotericin B. In more severe infections, systemic therapy with oral fluconazole or itraconazole may be necessary; however, potential drug interactions—particularly with agents like cyclosporine and rifampicin—should be carefully evaluated. Tinea capitis is commonly managed using griseofulvin, terbinafine, or itraconazole. Terbinafine demonstrates greater efficacy against Trichophyton species, whereas griseofulvin and itraconazole are generally more effective in infections caused by Microsporum species (13).
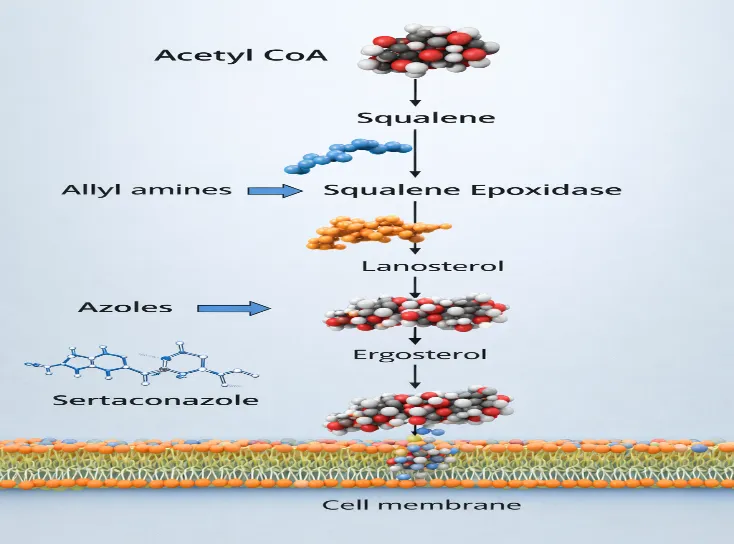
Mechanism of Action
Antifungal agents exert their therapeutic effects by inhibiting key enzymes involved in fungal sterol biosynthesis. One such critical enzyme is squalene epoxidase, which catalyzes the conversion of squalene to squalene epoxide. Many antifungal drugs selectively target pathways unique to fungal cells. Azole antifungals, including miconazole, fluconazole, and ketoconazole, inhibit the enzyme lanosterol 14α-demethylase. This enzyme plays an essential role in the conversion of lanosterol to ergosterol, a vital structural component of the fungal cell membrane. Interference with ergosterol synthesis disrupts membrane integrity, ultimately resulting in growth inhibition or fungal cell death (fungistatic or fungicidal effect) (15).
Limitations and Side effects of Antifungal Therapy (14)
Antifungal Resistance
Overall, clinical antifungal resistance, which is characterized by persistence of infection or signs in malignancy of treatment with applicable antimicrobial agents, causes failure to rule out fungal infection Cellular stress due to reaction to an antifungal medicine causes mechanisms that facilitate dermatophyte survival. Dermatophytes are activated by exposure to an antifungal medicine, levee age to their cell wall, alterations in the osmolarity of the terrain and emergence of reactive oxygen forms are stimulants that can activate signalling pathways to counteract the effects of unexpected cellular stress (16) Fungi possess the ability to sense and respond in a coordinated manner to environmental alterations in order to survive various cellular stresses, including those triggered by exposure to antifungal agents. To cope with these stresses, fungi have evolved alternative adaptive mechanisms involving complex regulatory networks that integrate cellular signaling pathways, stress response systems, and antifungal defense strategies (17). One of the major consequences of these adaptive processes is the increasing occurrence of dermatophyte infections associated with antifungal resistance. In recent years, a notable rise in antifungal-resistant dermatophytic infections has been documented worldwide.
Antifungal resistance was initially reported in India and has subsequently been identified in the United States as well as across several European countries. Among dermatophytes, Trichophyton mentagrophytes genotype VIII, also referred to as T. indotineae, has emerged as the predominant causative organism. Over the past decade, increasing resistance has been observed against one of the most frequently prescribed antifungal drugs, terbinafine. Terbinafine is considered a first-line therapy for dermatophytosis and exerts its antifungal action by inhibiting the enzyme squalene epoxidase. This enzyme plays a crucial role in ergosterol biosynthesis, which is an essential structural component of the fungal cell membrane (18). Resistance to antifungal agents may occur naturally (primary resistance), even in the absence of prior drug exposure, or may be acquired (secondary resistance) following repeated or prolonged exposure to antifungal therapy. The underlying microbiological mechanisms responsible for resistance are primarily associated with genetic mutations or variations in target genes. These alterations may lead to reduced drug uptake, structural changes at the drug-binding site, increased drug efflux, or enhanced elimination of the antifungal agent from the fungal cell. In particular, azole antifungals such as itraconazole disrupt ergosterol synthesis, a critical regulator of fungal cell membrane integrity. Resistance to azoles among dermatophytes has been linked to amino acid substitutions within the squalene epoxidase gene, which reduce terbinafine binding affinity. Additionally, decreased intracellular drug accumulation and increased efflux pump expression have also been reported as contributing resistance mechanisms (19).
Mechanism of Antifungal Resistance
In the clinical side, antifungal resistance has been determined as the persistence of infection/symptoms despite proper antifungal treatment that will ultimately result in the failure of killing fungal infection (20). The most popular mechanisms suggested in the dermatophyte resistance to antifungal drugs are:
Mechanism of Drug Efflux Fungi develop resistance via overexpression of efflux membrane transporters especially the ATP-binding cassette (ABC) transporters that are involved in an active elimination of antifungal drugs in the cell. This will reduce the concentration of the drug within the cell and will reduce its functionality. ABC transporters have a conserved nucleotide binding domain and an un-conserved transmembrane domain which enables them to secrete a wide range of dissimilar substances. The genomes of dermatophytes exhibit high similarity of the abundance of APB transporter genes in all the species. These genes tend to be complimentary and to compensate each other. In Trichophyton interdigitale (previously T. rubrum), the antifungal drugs increase the expression of mdr1, mdr2, and mdr4. Speaking of which, deletion of mdr2 enhances sensitivity to terbinafine, which indicates its particular implication. Nevertheless, aggregate efflux activity is caused by the synergic effect of multiple transporters, which causes diffuse and slow resistance (21).
2. Drug Target Gene Mutations
Another important mechanism contributing to antifungal resistance involves alterations in genes encoding drug-target enzymes, which ultimately reduce drug–target binding. This phenomenon has been well documented in yeast species, where ERG11 gene mutations are associated with azole resistance (Candida albicans), and mutations in the FKS1 gene are linked to echinocandin resistance. Although fewer confirmed target-gene mutations have been identified in dermatophytes, recent investigations suggest that genetic alterations may disrupt the interaction between azole antifungals and their target enzyme, lanosterol 14-α-demethylase, particularly affecting short-tailed triazoles. These genetic changes contribute to the development of azole resistance and a decrease in drug affinity (22).
Need for Alternative Therapies
The global incidence of dermatophyte infections continues to rise, affecting approximately 20–25% of the world’s population. The widespread and often indiscriminate use of antifungal agents has created a substantial challenge in the management of fungal diseases, particularly due to the emergence of resistant strains. This growing resistance problem has highlighted the urgent need to explore alternative and non-conventional therapeutic strategies to identify new and effective antifungal treatments (23). Currently, several synthetic agents, including azole derivatives, are commonly employed in therapy. These antifungal agents are frequently prescribed for the treatment of various skin infections. However, the increasing occurrence of treatment-related adverse effects underscores the need to reconsider safer therapeutic options (24). With the growing prevalence of antifungal drug-resistant strains, dermatophytosis cases have escalated considerably, emphasizing the demand for novel and effective treatment approaches. As a result, there has been increasing interest in natural products with antifungal activity, as they are generally considered safe, cost-effective, readily available, and possess a broad range of medicinal properties that may help prevent disease progression and improve patient outcomes (25). Furthermore, innovative therapeutic approaches derived from diverse sources—including natural products, synthetic compounds, and polymer-based systems—are being recognized as promising alternatives (26).
Herbal Compounds and Phytochemicals with Anti-Dermatophytic Action
Conventional therapies currently used for the management of fungal infections are associated with several limitations, including the development of antifungal resistance and the risk of serious adverse effects (27). In an effort to enhance treatment efficacy, prolonged use of systemic antifungal medications is often required; however, this may lead to complications such as hepatotoxicity. Preliminary reports suggest that some conventional remedies may also contribute to antibiotic resistance and cause unfavorable or adverse reactions in certain cases (28). Medicinal stores have sold another set of biologically effective substances centuries and have been widely used as either crude accoutrements or finished mixtures to cure colorful ailments(29). Although allopathy developed greatly throughout the 19 th century, stores remain a major source of medicinals in both ultramodern and traditional medicine across the world (30). Herbal shops have gained a significant amount of interest in recent times due to the numerous benefits of their operations such as reduced costs and reduced side goods. It is also commented that a good strategy is to use factory grounded products in the treatment of bacterial, fungal, and sponger ails. Also, certain behaviors could be done to create details by identifying the active constituents in the factory. Some of the stores have been proven to maintain antifungal percentages against fungi. These Include, Myrtus communis, Ginger, black sap, liquorice, Narcissustazetta, aloe vera, thyme, dill, cilantro, onions, cilantro, henna and garlic. Such stores have a number of microbially active chemicals, such as, alkaloids, flavonoids, citronellol, tannins, geraniol, thymoquinone, and phenolic composites (31).
The principal curcuminoid present in the widely used Indian spice turmeric, which belongs to the ginger family (Zingiberaceae), is curcumin. In addition to curcumin, bis-desmethoxycurcumin and desmethoxycurcumin constitute the remaining two major curcuminoids (32). Turmeric has been traditionally utilized in the management of various dermatological conditions, including skin infections, pruritus, tinea, and ringworm. The rhizomes are commonly employed in medicinal practice due to their carminative and antifungal properties, as well as their antioxidant and anti-inflammatory activities, largely attributed to curcuminoids and volatile oils. In the present investigation, topical formulations such as cream preparations containing turmeric, including formulations with 6% and 10% w/w turmeric oil, were developed and evaluated. One of the key bioactive components of turmeric oil, ar-turmerone, has been reported to exhibit significant anti-dermatophytic activity (33). This study focuses on the potential application of aqueous and alcoholic extracts of turmeric rhizomes, along with a composite system formulated using silver nanoparticles (Ag-NPs) derived from turmeric extracts. These formulations demonstrated enhanced antifungal activity, particularly when used in combination with silver nanoparticles and conventional antifungal agents. Current evidence suggests that these nanoparticles interact with fungal cells at the molecular level, leading to disruption of the cell membrane, interference with DNA replication, protein degradation, and ultimately fungal cell death (34). A plant tissue culture-based study further demonstrated the fungistatic activity of curcumin at a concentration of 0.8 g/L. Curcumin exerts its antifungal action by inhibiting C-5 sterol desaturase and ergosterol biosynthesis, thereby increasing the production of reactive oxygen species within fungal cells. Additionally, curcumin has been shown to alter ATPase activity, resulting in reduced protease secretion and contributing to its overall antifungal efficacy (35). In veterinary applications, dermatophytosis—particularly in dogs—has emerged as a significant concern. A clinical study conducted on dogs diagnosed with dermatophytosis at the Veterinary Clinical Complex (VCRC), Orathanadu, reported symptoms such as pruritus, focal and circular alopecia, scaling, crust formation, erythematous margins, hyperpigmentation, and epidermal thickening. Topical ketoconazole served as the positive control in Group I, while poly-herbal formulations were administered to Groups II, III, and IV. Notably, a poly-herbal combination consisting of Acalypha indica, Curcuma longa, and sodium chloride in a 7:2:1 ratio demonstrated significant reduction in fungal infection following a 10-day treatment regimen in companion animals (36).

Aloe vera is a succulent species belonging to the Asphodelaceae family and has long been recognized for its extensive medicinal value, with documented therapeutic applications across diverse cultures for several centuries. Commonly referred to as the “wonder plant,” it is widely known for its broad spectrum of pharmacological activities (37). Among the various bioactive constituents identified in Aloe vera, aloe-emodin, a naturally occurring hydroxyanthraquinone derivative, plays a significant role in its antifungal action. Aloe-emodin has demonstrated notable antifungal activity against a wide range of fungal organisms, including Candida species and dermatophytes. Its mechanism of action involves interference with ergosterol biosynthesis, a critical component of fungal cell membranes. Since ergosterol is essential for maintaining membrane integrity and fluidity, its inhibition results in compromised membrane structure and impaired fungal cell viability (38). Another important phytoconstituent present in Aloe vera is aloin, which exhibits pronounced immunomodulatory properties. Aloin has been reported to stimulate immune responses by activating macrophages, leading to increased secretion of inflammatory mediators such as interleukins and tumor necrosis factor-α. Macrophages play a pivotal role in host defense against fungal pathogens by engulfing invading organisms and initiating inflammatory responses (39). In addition, specific polysaccharides found in Aloe vera have been shown to enhance immune function by stimulating T-lymphocytes and natural killer cells, thereby strengthening the body’s defense mechanisms against fungal invasion (40). Experimental investigations employing techniques such as minimum inhibitory concentration (MIC) assays and time-kill studies have consistently confirmed the antifungal potential of Aloe vera by demonstrating inhibition of fungal growth and replication (38). Moreover, in vivo studies have produced favorable outcomes, including reduced fungal burden and improved therapeutic responses in fungal infections (41).

3.Garlic (Allium sativum)
Garlic, well known by its strong odor and distinct flavor, has been used throughout history as a component of traditional medicine because of the many health benefits it has (42). Allicin is the most significant bioactive component of garlic with its high concentration being the primary reason behind its potent antifungal effects against yeast and mold (43). It has antifungal activity that works in a number of ways, mainly by acting on the ergosterol production pathway in fungi (plays a significant role in maintaining membrane fluidity and stability (45). Allicin inhibits important enzymes of ergosterol synthesis including squalene epoxidase and 14-alpha-demethylase that are products of the ERG1- and ERG11-genes, respectively (46).

4.Neem (Azadirachta indica)
The antifungal effects of neem can be attributed to a vast range of biologicalactive composites, plus limonoids, nimbin, nimbidin, & azadirachtin, that are reportedly linked with the antifungal effects of the plant(48).Neem isolates have been targeted at several pathogenic fungal species, including Aspergillus fumigatus and Candida species, as a result of their antifungal effects(49).The antifungal effect of neem is an activity that is directed to the sterol b Azadirachtin is a specific inhibitor of the enzyme 24-methylenedihydrolanosterol acetyltransferase (24-MDT), which is required in converting lanosterol to 24-methylenedihydrolanosterol (50,51,52,53).

5.Black Pepper (Piper nigrum)
The black pepper ethereal oil painting possesses high antifungal rate. It has been proved that the n- hexane extract of black pepper essential oil painting has significant antifungal effects (54).Also antifungal effects against Candida spp. have been evidenced, and the effect of its actions on acridity factors and antifungal resistant clinical isolates considered (55).

6.Henna (Lawsonia inermis)
The major component of henna leaves, which was fraxetin, exerted high antifungal effects in ethanol excerpt of leaves and acetone against dermatophyte species. It is possible to develop these excerpts as a cover to treat dermatophytosis (56). Studies have shown that henna paste contains antifungal parcels on dermatophytes species and dermatophytes isolates of Candida. The leaves of this factory contain antibacterial-, seditious-, antipyretic-packs (57).

CONCLUSION
Dermatophytosis is a serious health concern of the world which has been complicated by the rising cases of antifungal resistance and drawbacks of traditional treatment options such as side-effects, high cost and lack of efficacy. This review shows the increasing danger of the problem of resistant species of dermatophytes and the necessity to find other methods of therapy. Plant-based phytochemicals including the herbal compounds and turmeric, aloe vera, garlic, neem, black pepper, and henna show a promising anti-dermatophytic effect, which includes the interference with fungal cell membrane, inhibition of ergosterol production. Herbal therapies are a promising and viable alternative or a supplement to current antifungal therapy due to their safety, low cost, and wide biological activity. More preclinical and clinical research is justified to support their effectiveness and help to incorporate them in contemporary antifungal treatment options.
REFERENCES


Divya*, Aryan Jamwal, Dimple Kumari, Akshay Thakur, Vinay Pandit, M. S. Ashawat, Dermatophytes and the Rising Threat of Antifungal Resistance: Exploring Herbal Compounds as Alternative Therapies, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 458-471. https://doi.org/10.5281/zenodo.20501749
 10.5281/zenodo.20501749
10.5281/zenodo.20501749