
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
*Department of Pharmacy, Faculty of Medical Paramedical and Allied Health Science, Jagannath University, Jaipur, Rajasthan, 303901, India
2 Faculty of Medical Paramedical and Allied Health Science, Jagannath University, Jaipur, Rajasthan, 303901, India
One of the most serious non-communicable disease crises of the twenty-first century is type 2 diabetes mellitus (T2DM). The International Diabetes Federation (IDF) Diabetes Atlas estimates that 589 million persons worldwide—roughly one in nine adults—currently have diabetes, and by 2050, this number is expected to rise to 853 million. Conventional treatments, such as insulin, metformin, sulfonylureas, and thiazolidinediones, are still essential, but it is becoming more widely acknowledged that they are inadequate to address the complex, multi-defect pathophysiology of type 2 diabetes, which includes ?-cell exhaustion, cardiovascular risk, and the progression of chronic kidney disease. Four main developing therapy categories-GLP-1 receptor agonists (GLP-1 RAs), SGLT2 inhibitors, dual GIP/GLP-1 receptor agonists (Tirzepatide), and oral insulin delivery systems-are rigorously assessed in this study based on their molecular underpinnings, clinical trial data, and relative efficacy. Additionally, a 2025 Lancet Diabetes & Endocrinology trial found that sotagliflozin, a new dual SGLT1/SGLT2 inhibitor, reduced composite cardiovascular risk by about 30%. A critical evaluation shows that dual agonists are quickly becoming the most effective medications for combination glycemic and weight management, even if GLP-1 RAs and SGLT2 inhibitors have already established a solid position in ADA and ESC 2025 guidelines. Despite ongoing research after Phase 3 disappointments, oral insulin treatment still has scientific potential thanks to delivery techniques based on nanoparticles. In addition to advocating for a paradigm change toward tailored, cardiometabolic, and organ-protective diabetes management, this review offers an organized gap analysis.
Type 2 diabetes mellitus (T2DM) is one of the most significant non-communicable disease crises of the twenty-first century. According to the International Diabetes Federation's (IDF) Diabetes Atlas, 589 million people worldwide—roughly one in nine adults—have diabetes at the moment, and by 2050, that figure is predicted to increase to 853 million.[1,2] The worldwide health problem is made worse by the startling percentage of cases that go undetected, especially in low- and middle-income nations.
Beyond just hyperglycemia, type 2 diabetes is linked to a number of potentially fatal side effects, such as neuropathy, retinopathy, chronic kidney disease (CKD), and cardiovascular disease. Over 95% of instances of diabetes are type 2 diabetes (T2DM), which is mostly caused by increased obesity, sedentary lifestyles, urbanization, and genetic vulnerability. The illness is one of the main causes of death worldwide, accounting for about 3.4 million fatalities every year.[1]
The pathophysiological underpinnings of type 2 diabetes go well beyond insulin insufficiency. T2DM was essentially reframed as a multisystem metabolic condition by DeFronzo's conception of the "Ominous Octet"—eight concurrent organ-level abnormalities.[3] This has spurred the creation of treatments that target obesity, cardiovascular risk, renal function, and patient adherence in addition to glycemic management.
Despite being clinically successful and reasonably priced, conventional medications like insulin, metformin, and sulfonylureas have several drawbacks, including weight gain, hypoglycemia risk, progressive loss of efficacy due to β-cell failure, and little organ-protective advantages.[4,5] Over the past ten years, these flaws have prompted the creation of new therapeutic classes, radically altering clinical practice recommendations.
GLP-1 receptor agonists, SGLT2 inhibitors, dual incretin receptor agonists (Tirzepatide), and oral insulin systems are among the emerging treatments for type 2 diabetes that are thoroughly and critically examined in this review. It includes updated clinical data from 2024–2025, a structured comparative analysis, and an identification of unmet research gaps. The objective is to offer a distinctively analytical and clinically applicable viewpoint to the quickly changing field of T2DM treatments.
1.Pathophysiology Framework
According to DeFronzo (2009), the current understanding of T2DM pathophysiology revolves around a complicated interplay of eight main abnormalities.[3] The 'Ominous Octet' model emphasizes how the pancreas, liver, muscle, adipose tissue, kidney, gut, and brain are all involved in maintaining hyperglycemia. To understand why new multi-target medicines, provide better results than previous single-pathway drugs, it is crucial to comprehend this framework
1.Core Defects
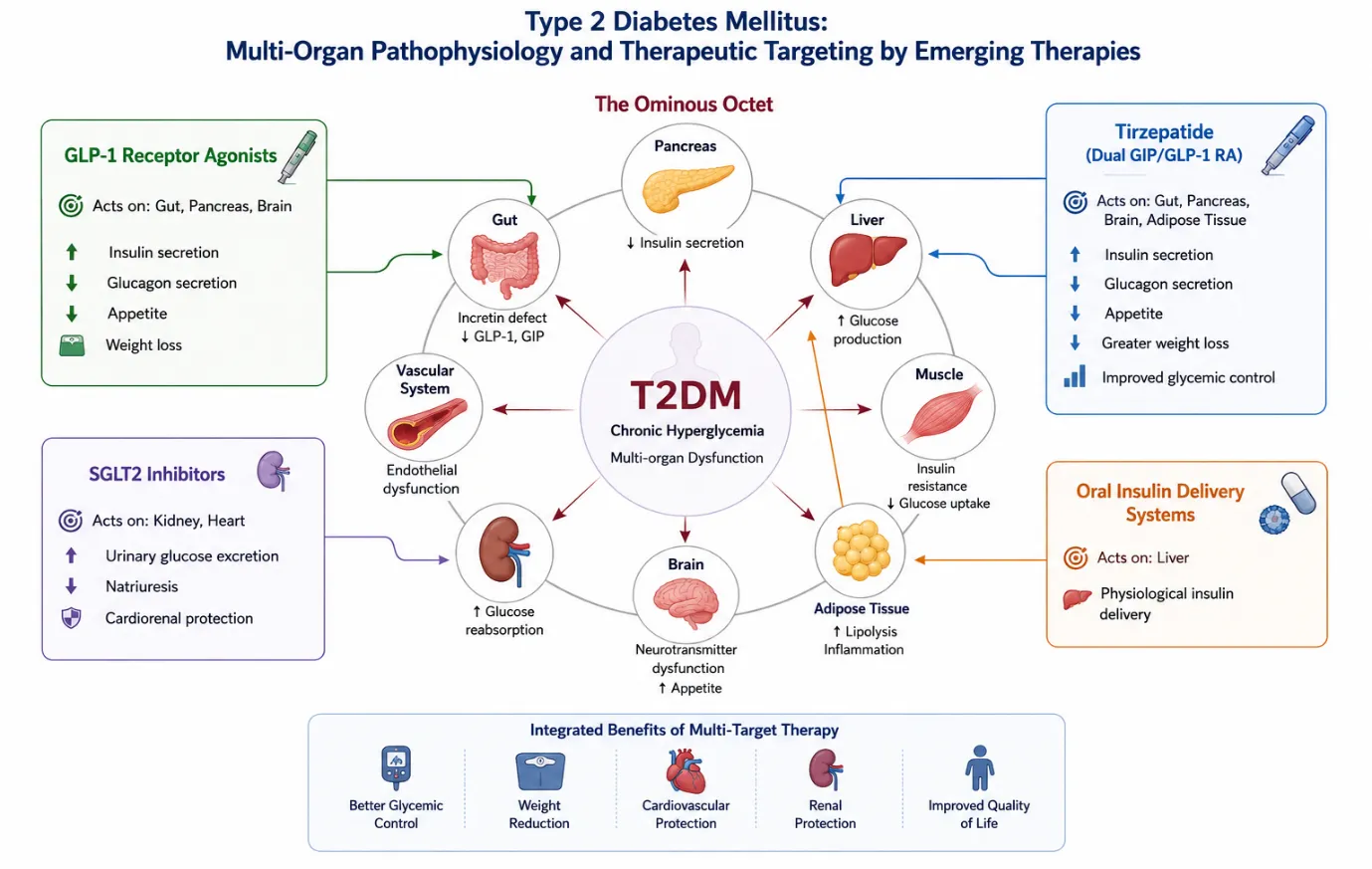
Figure 2.1: Integrated multi-organ pathophysiology of type 2 diabetes mellitus and therapeutic targeting by emerging antidiabetic therapies.
This multi-organ framework makes it abundantly evident why prolonged metabolic control is inherently difficult to achieve with traditional single-target medicines. New treatments are in a unique position to address several of this pathophysiological network's nodes at once.[3]
2.Pathophysiology Framework
According to DeFronzo (2009), the current understanding of T2DM pathophysiology revolves around a complicated interplay of eight main abnormalities.[3] The 'Ominous Octet' model emphasizes how the pancreas, liver, muscle, adipose tissue, kidney, gut, and brain are all involved in maintaining hyperglycemia. To understand why new multi-target medicines, provide better results than previous single-pathway drugs, it is crucial to comprehend this framework.
1.Core Defects
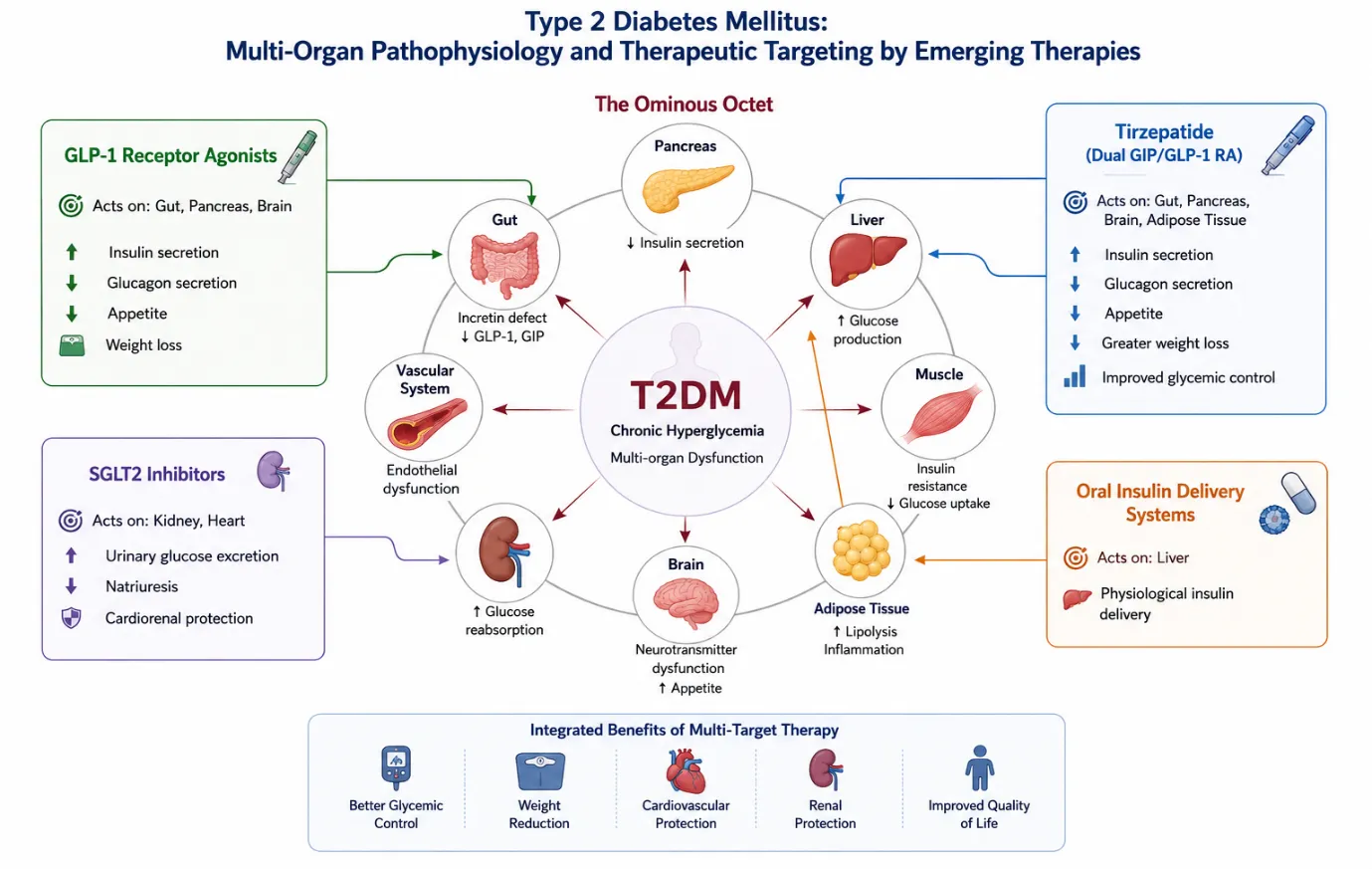
Figure 2.1: Integrated multi-organ pathophysiology of type 2 diabetes mellitus and therapeutic targeting by emerging antidiabetic therapies
This multi-organ framework makes it abundantly evident why prolonged metabolic control is inherently difficult to achieve with traditional single-target medicines. New treatments are in a unique position to address several of this pathophysiological network's nodes at once.[3]
3.Critical Appraisal of Conventional Therapies
Conventional antidiabetic medications continue to be significant, especially considering their proven effectiveness, accessibility, and low cost. A critical evaluation, however, identifies a number of clinically relevant limits that support the search for more innovative treatment approaches.
Metformin reduces hepatic gluconeogenesis and somewhat increases peripheral insulin sensitivity via activating AMP-kinase (AMPK). According to the United Kingdom Prospective Diabetes Study (UKPDS), it is the best first-line medication.[4] Its mild cardiovascular benefit, low risk of hypoglycemia, and weight neutrality are its key advantages. It is contraindicated in people with renal impairment (eGFR <30 mL/min), exclusively targets one pathway, and produces gastrointestinal discomfort in up to 30% of patients.
Sulfonylureas, such as glimepiride and glibenclamide, increase insulin secretion despite blood glucose levels, which naturally increases the risk of hypoglycemia.[5] Significantly, long-term sulfonylurea uses speeds up β-cell fatigue, which ironically exacerbates the very flaw they are meant to fix. Gaining weight exacerbates insulin resistance. Sulfonylureas are becoming less important for long-term use according to current diabetes recommendations.
The adipose tissue insulin sensitivity is enhanced by pioglitazone, a PPAR-γ agonist. Its application is complicated by severe fluid retention, risk of heart failure exacerbation, and bone fracture in women, making it inappropriate for a major portion of patients despite its effectiveness and association with decreased hepatic steatosis.
As the most effective glucose-lowering medication now on the market, insulin is essential for advanced type 2 diabetes. However, many patients experience psychological insulin resistance due to its subcutaneous administration necessity, which delays beginning. Other issues include peripheral hyperinsulinemia, weight gain, and the risk of hypoglycemia. Oral insulin administration devices have gained popularity as a result of these restrictions. [22,23]
Four general limitations of conventional therapies are identified: (1) single-pathway targeting against a multi-defect disease; (2) adverse metabolic effects, such as hypoglycemia and weight gain; (3) progressive loss of efficacy as β-cell function declines; and (4) minimal protection for the kidneys or heart.[3,4,5] These drawbacks serve as the logical foundation for newly developed multi-target treatments.
Mechanism
Endogenous GLP-1, an incretin hormone released by intestinal L-cells in response to nutrient consumption, is mimicked by GLP-1 receptor agonists. The incretin effect is significantly reduced in type 2 diabetes, which leads to inadequate insulin production after meals. Through glucose-dependent insulin secretion, concurrent glucagon suppression, delayed stomach emptying, and centrally mediated appetite reduction, GLP-1 RAs reverse this effect. Crucially, the risk of hypoglycemia is inherently minimal because insulin secretion is glucose-dependent. [6,7,8]
Clinical Evidence and Updated 2024-2025 Data
In high-risk T2DM patients, the LEADER study (Liraglutide) showed a significant cardiovascular mortality benefit and a 13% decrease in MACE.[6] Semaglutide reduced MACE by 26% in the SUSTAIN-6 trial, with a particularly notable decrease in non-fatal stroke.[7] Dulaglutide's cardiovascular benefits were extended to primary prevention populations in the REWIND study.[8]
GLP-1 RA users had a 1.1% mortality rate compared to 0.6% in the tirzepatide group, according to a seminal 2024 real-world cohort study (JAMA Network Open, August 2024) comparing 140,308 US patients with T2DM on tirzepatide versus GLP-1 RAs over a median follow-up of 10.5 months.[20] This finding highlights the potential for clinical advancement beyond traditional GLP-1 monotherapy. In head-to-head meta-analyses, GLP-1 RAs continue to show better atherothrombotic event reduction than SGLT2 inhibitors.
Regardless of HbA1c level, the ADA/EASD 2025 guidelines now prescribe GLP-1 RAs as recommended second-line treatments in individuals with high atherosclerotic risk or existing cardiovascular disease.
Critical Perspective
GLP-1 RAs have a remarkable cardiometabolic profile, but they have significant gastrointestinal tolerability problems (nausea and vomiting in about 20–40% of patients), which restrict dose escalation and adherence. The effects of long-term β-cell preservation are still not well understood. Additionally, in underdeveloped nations like India, where generic oral medications are the most commonly prescribed, cost and injectable formulation restrictions continue to be obstacles to access. [6,7,8]
4.2 SGLT2 Inhibitor
Mechanism
Through specifically inhibiting SGLT2 transporters in the renal proximal tubule, sodium-glucose cotransporter-2 (SGLT2) inhibitors increase urine glucose excretion (glycosuria) in an insulin-independent manner. Osmotic diuresis and natriuresis lower blood pressure, and the resulting caloric loss aids in weight loss. Their exceptional heart failure advantages are based on these hemodynamic effects, which include a decrease in cardiac preload and afterload. [9,10]
Clinical Evidence and Updated 2024-2025 Data
In T2DM patients with established CVD, the EMPA-REG OUTCOME study demonstrated the cardiovascular mortality benefit of empagliflozin (38% reduction in CV death). Even in populations without diabetes, the DAPA-HF trial showed that dapagliflozin was effective in lowering heart failure hospitalizations.[10] Reno protective advantages were validated by the CREDENCE and DAPA-CKD studies. [11,12]
SGLT2 inhibitors significantly decreased MACE (HR 0.89), cardiovascular death or heart failure hospitalization (HR 0.78), and slowed the progression of CKD across all eGFR and albuminuria subgroups, according to a thorough 2024 systematic review and meta-analysis of 14 randomized controlled trials involving 97,412 participants (published in Diabetes Research and Clinical Practice, November 2024).[16]
Most notably, sotagliflozin, a dual SGLT1/SGLT2 inhibitor that also prevents intestinal glucose absorption, reached clinical maturity in 2024–2025. The cardiovascular benefit of earlier SGLT2i agents was surpassed by a 2025 Lancet Diabetes & Endocrinology cardiovascular outcome trial that showed a roughly 30% reduction in the composite risk of heart attack, stroke, and cardiovascular death in T2DM patients with recent heart failure hospitalization.[13,14,15] Regardless of glycemic control status, SGLT2 inhibitors are now positioned earlier in cardio-renal-metabolic therapy algorithms according to ADA and ESC 2025 guidelines.
Clinical Perspective
Despite their advantages for the heart and kidneys, SGLT2 inhibitors increase the risk of urinary tract infections, vaginal mycotic infections, and, in rare cases, euglycemic diabetic ketoacidosis. Their ability to reduce blood sugar is quite weak (HbA1c reduction of ~0.7–1.0%). According to new research from 2025, patients with low BMI may not benefit as much from them. Cost is still a major obstacle in environments with limited resources. [9,11]
4.3 Dual GIP/GLP-1 Receptor Agonists
Mechanism
Tirzepatide, often referred to, "twincretin," is a 39-amino acid synthetic peptide that simultaneously stimulates GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. [17,18] Through a different receptor mechanism from GLP-1, the GIP component increases insulin production, encourages adipose tissue lipid metabolism, and may increase insulin sensitivity. An additive or possibly supraadditive effect on β-cell activity, appetite suppression, stomach motility, and hepatic glucose output is produced by the synergistic co-activation of both incretin pathways. Tirzepatide's extended half-life allows for once-weekly dosage due to its molecular structure, which is based on the native GIP sequence with fatty diacid modification.
Clinical Evidence and Updated 2024-2025 Data
Tirzepatide is the most effective glucose-lowering and weight-reducing medication currently approved for type 2 diabetes, with HbA1c reductions of up to 2.0–2.5% and body weight decreases of 6.2–12.9 kg across dosages (5 mg, 10 mg, and 15 mg once weekly), according to the SURPASS clinical study program (SURPASS 1–5).[17,18,19] In direct comparison trials, tirzepatide outperformed semaglutide and baseline insulin.[17]
Tirzepatide was linked to lower all-cause mortality (0.6% vs. 1.1%), lower MACE, lower major adverse kidney events (MAKE), and lower acute kidney injury risk compared to GLP-1 receptor agonists after a median follow-up of 10.5 months, according to a seminal 2024 real-world cohort study (JAMA Network Open, August 2024) using the TriNetX US Collaborative Network, which included 140,308 T2DM.[20] The most thorough real-world efficacy comparison to date, these advantages were true for subgroups stratified by eGFR, HbA1c, cardiovascular disease state, and BMI.
Tirzepatide has a favourable safety profile and significantly more weight loss than placebo in T2DM and obese individuals, according to a 2024 meta-analysis that included SURMOUNT-2.[21] In order to finalize tirzepatide's cardiovascular risk profile, detailed MACE data from the SURPASS-CVOT, a dedicated cardiovascular outcomes trial in 12,500 patients with T2DM and established ASCVD, is anticipated to be reported in 2025.
Clinical Perspective
Tirzepatide shares the gastrointestinal side-effect profile of GLP-1 RAs (nausea, vomiting, diarrhoea in the first few weeks of dose escalation), despite its remarkable metabolic results. Formal CVOT completion is pending for long-term cardiovascular endpoint data beyond the real-world study mentioned above. Tirzepatide is still not widely available in India and other low-middle-income nations, and its cost is significantly greater than that of conventional agents. Pharmaceutical development is actively exploring the possibility of triple agonists (GLP-1/GIP/Glucagon). [17,20,21]
4.4 Oral Insulin Therapy
Rational and Physiological Advantage
A considerable percentage of T2DM patients experience psychological insulin resistance, which is characterized by a patient's unwillingness to start injectable insulin therapy. This delays treatment escalation, hastening the development of problems. Oral insulin was designed to emulate the physiological portal-first delivery method of endogenous insulin and get over injection-related obstacles. [22,24] Direct hepatic glucose lowering made possible by portal delivery may lessen peripheral hyperinsulinemia and the weight gain that goes along with it.
Scientific Barriers
Gastric acid denaturation of the protein, intestinal enzyme proteolytic degradation, poor intestinal membrane permeability because of insulin's large molecular size and hydrophilicity, and highly variable bioavailability among patients are all significant pharmaceutical challenges associated with oral insulin delivery. To get around these obstacles, a variety of administration methods have been studied, including enteric-coated capsules, absorption enhancers, polymeric nanoparticles, liposomes, and mucoadhesive systems. [24,25]
Clinical Evidence: Current Status (2026)
The most clinically progressed oral insulin contender was ORMD-0801 (Oramed Pharmaceuticals). Measurable HbA1c reductions and adequate tolerability were shown in phase 2 randomized controlled trials.[22] However, the diabetes-focused effort was discontinued after following large Phase 3 trials in T2DM failed to fulfill primary efficacy targets.[23] This result highlights the ongoing difficulty in attaining comparable oral bioavailability across broad, diverse clinical groups.
Despite this obstacle, research on oral insulin platforms based on nanoparticles-using polymeric, lipid, and mucoadhesive nanocarriers-continues worldwide. [24,25] Prominent pharmaceutical companies, such as Novo Nordisk, have continued to invest in next-generation oral insulin platforms, confirming the long-term commercial and scientific justification. As of 2026, the sector is undergoing rebuilding, and no oral insulin medication has been approved as the standard of care for type 2 diabetes worldwide.
Clinical Perspective
If developed effectively, oral insulin would change the way diabetes is managed by allowing for earlier insulin introduction, enhancing adherence, and providing better physiological hepatic targeting.[24] Promising early-phase data must be read cautiously, though, as demonstrated by the Phase 3 failures of current-generation pharmaceuticals.[22,23] Rather of making small adjustments to current platforms, future development will probably rely on quantum advancements in formulation science and nanocarrier technology.[25]
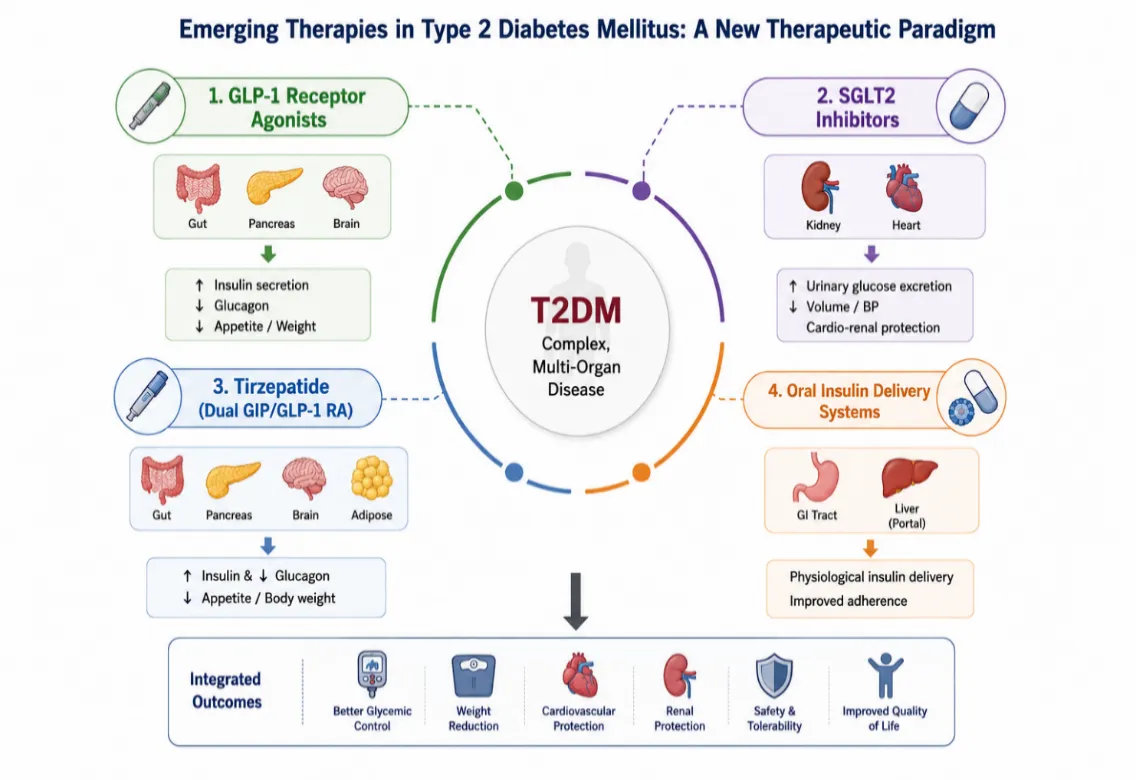
Figure 4.1 Emerging therapeutic strategies in type 2 diabetes mellitus and their integrated clinical benefits.
5.Comparative Analysis of Emerging vs. Conventional Therapies
A systematic assessment of important pharmacological and clinical factors for both established and novel treatments is shown in Table 1. Red-shaded cells show drawbacks, green-shaded cells show positive results, and yellow-shaded cells show neutral or partial benefits.
Table 1: Comparative Overview of New and Conventional T2DM Treatments
|
Parameter |
Metformin |
Sulfonylureas |
GLP-1 RAs |
SGLT2i |
Dual Agonists |
Oral Insulin* |
|
HbA1c Reduction |
~1–1.5% |
~1–1.5% |
~1–1.8% |
~0.7–1.0% |
~2.0–2.5% |
Investigational |
|
Weight Effect |
Neutral/↓ |
↑ Weight |
↓ 5–15 kg |
↓ Mild |
↓ 10–15 kg+ |
Neutral |
|
Hypoglycemia Risk |
Low |
High |
Low |
Low |
Low |
Possible |
|
CV Benefit |
Modest |
None |
Yes (MACE↓) |
HF reduction |
Emerging data |
Unknown |
|
Renal Protection |
Modest |
None |
Some evidence |
Strong |
Under study |
Unknown |
|
Route |
Oral |
Oral |
Subcutaneous / Oral |
Oral (daily) |
Subcutaneous (weekly) |
Oral (capsule) |
|
β-Cell Preservation |
Indirect |
Accelerates loss |
Possible |
Indirect |
Possible |
Unknown |
|
Guideline Position |
First-line |
Second-line |
Second-line preferred in CV risk |
Second-line preferred in CKD/HF |
Advancing |
Investigational |
5.Future Perspective
A comprehensive cardiometabolic and organ-protective approach is replacing glucose-centric control in the therapeutic paradigm for type 2 diabetes. The next ten years of diabetes care will probably be defined by a number of trajectories:
In the end, the integration of precision medicine, patient-centered care, digital health, and equitable access-a vision that is still ambitious but becoming more realistic-rather than isolated pharmaceutical innovation will be the key to managing type 2 diabetes.
CONCLUSION
A therapy strategy appropriate to the pathophysiological complexity of type 2 diabetes mellitus is necessary since it is a complicated, progressive, multiorgan metabolic disease.[3] Despite their continued therapeutic value, affordability, and necessity, conventional medicines are fundamentally restricted in their ability to address the multi-defect nature of type 2 diabetes and offer little protection against cardiovascular and renal consequences.[4,5]
The therapy approach has permanently changed with the introduction of GLP-1 receptor agonists, SGLT2 inhibitors, and dual incretin agonists. [6,7,8,9] Tirzepatide has better results than GLP-1 RAs in real-world populations across mortality, cardiovascular, and renal endpoints, according to updated data from 2024–2025.[20] With new intestinal pathways, Sotagliflozin has expanded the cardiovascular advantages of the SGLT family.[13,14,15] Oral insulin, on the other hand, continues to be an intriguing scientific but technically unsolved area.[22,23]
The systematic gap identification, organized comparison analysis, and integration of the most recent clinical trial findings are the key contributions of this study, which offers a paradigm that transcends descriptive review in Favor of analytical appraisal. Evidence-based, and customized therapy approaches are most effective in achieving the ultimate goals of T2DM management, which include prolonged metabolic control, organ protection, and enhanced quality of life. The next phase of diabetes care will be defined by ongoing innovation, translational research, and the creation of practical evidence.
REFERENCES

Arun Kumar Gulia, Rakesh Kumar Sharma, Emerging Therapies in Type 2 Diabetes Mellitus: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 392-403. https://doi.org/10.5281/zenodo.20493294
 10.5281/zenodo.20493294
10.5281/zenodo.20493294