
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Womens College of Pharmacy, Peth Vadgaon, Maharashtra, India
Encephalitis is a severe neurological disorder characterized by inflammation of the brain parenchyma, commonly caused by viral infections, autoimmune responses, and, less frequently, bacterial, fungal, or parasitic infections. The condition can result in significant morbidity and mortality if not diagnosed and treated promptly. Viral pathogens such as herpes simplex virus (HSV), arboviruses, enteroviruses, and varicella-zoster virus are major contributors to infectious encephalitis, whereas autoimmune encephalitis results from antibodies attacking neuronal receptors in the central nervous system. Clinical manifestations range from mild fever and headache to seizures, altered consciousness, psychiatric abnormalities, and neurological deficits. Diagnosis involves a combination of clinical evaluation, cerebrospinal fluid (CSF) analysis, neuroimaging, electroencephalography (EEG), serological testing, and molecular diagnostic tools such as polymerase chain reaction (PCR). Treatment strategies depend on etiology and include antiviral agents, corticosteroids, immunotherapy, supportive management, and rehabilitation. Recent advances in molecular diagnostics, immunotherapy, and vaccine development have significantly improved disease outcomes. This review highlights the etiology, epidemiology, pathophysiology, diagnosis, therapeutic interventions, complications, preventive strategies, and future perspectives of encephalitis disease.
Encephalitis is a severe neurological disorder characterized by inflammation of the brain parenchyma, which can result from infectious or non-infectious causes. The condition is considered a medical emergency due to its rapid progression and potential to cause permanent neurological damage, cognitive impairment, seizures, coma, and even death if left untreated. Encephalitis may occur in individuals of all age groups, although children, elderly individuals, and immunocompromised patients are generally at a higher risk of developing severe complications. The disease can present with a wide spectrum of clinical manifestations ranging from mild flu-like symptoms to severe neurological deficits, making early diagnosis and intervention essential for patient survival and recovery [1].
The etiology of encephalitis is highly diverse, with viral infections being the most common causative factor worldwide. Viruses such as herpes simplex virus (HSV), varicella-zoster virus (VZV), enteroviruses, arboviruses, and rabies virus are frequently implicated in infectious encephalitis. In recent years, autoimmune encephalitis has gained increasing clinical attention due to its association with antibodies targeting neuronal cell surface antigens, including N-methyl-D-aspartate receptor (NMDAR). Autoimmune encephalitis may mimic psychiatric or infectious disorders, often creating diagnostic challenges for clinicians and delaying appropriate treatment [2].
The global burden of encephalitis remains substantial despite advances in vaccination and antiviral therapies. Epidemiological studies indicate that the incidence of encephalitis varies according to geographical location, age, environmental exposure, and seasonal prevalence of infectious vectors. In developing countries, vector-borne encephalitis such as Japanese encephalitis continues to pose significant public health concerns, whereas in developed nations, viral and autoimmune etiologies are increasingly recognized. Mortality and morbidity rates remain high, particularly among untreated patients or those diagnosed at advanced disease stages [3].
The pathophysiology of encephalitis involves inflammatory processes within the central nervous system (CNS), leading to neuronal injury and cerebral dysfunction. Infectious agents invade the brain either through hematogenous spread or retrograde neuronal transmission, initiating immune-mediated inflammatory responses that damage neuronal tissues. In autoimmune encephalitis, the immune system erroneously attacks neuronal receptors and synaptic proteins, disrupting normal neurotransmission and resulting in neurological and psychiatric manifestations [4].
Clinically, encephalitis is associated with symptoms such as fever, headache, altered mental status, seizures, confusion, memory deficits, behavioral disturbances, and focal neurological abnormalities. The severity of symptoms varies depending on the underlying etiology, affected brain regions, and host immune status. Due to overlapping clinical features with meningitis and other neurological disorders, comprehensive diagnostic evaluation involving neuroimaging, cerebrospinal fluid (CSF) analysis, electroencephalography (EEG), and molecular diagnostic techniques is often required to confirm the diagnosis [5].
Early recognition and prompt treatment of encephalitis are essential for minimizing neurological complications and improving long-term outcomes. Antiviral agents such as acyclovir remain the cornerstone therapy for suspected viral encephalitis, particularly HSV encephalitis, while immunomodulatory therapies including corticosteroids, intravenous immunoglobulin (IVIG), and plasmapheresis are frequently employed in autoimmune cases. Preventive strategies, including vaccination, vector control measures, and public health surveillance, continue to play a vital role in reducing the burden of encephalitis globally [6].
2. Epidemiology of Encephalitis
Encephalitis is recognized as a significant global public health concern due to its high morbidity, mortality, and long-term neurological consequences. The incidence of encephalitis varies considerably across regions and populations, generally ranging from 3.5 to 12 cases per 100,000 individuals annually. Variability in incidence is influenced by geographical distribution, age, seasonal patterns, causative pathogens, vaccination coverage, and healthcare accessibility. Although encephalitis affects all age groups, infants, children, elderly individuals, and immunocompromised patients are disproportionately affected due to their increased susceptibility to severe infections and weakened immune responses [7].
Globally, infectious encephalitis remains predominantly caused by viral agents, with herpes simplex virus (HSV) identified as one of the most frequent causes of sporadic fatal encephalitis in many developed countries. Arboviral encephalitis, transmitted by mosquitoes and ticks, demonstrates significant geographical variation. For example, West Nile virus encephalitis is more prevalent in North America, whereas Japanese encephalitis remains endemic in many Asian countries, including India, China, Nepal, and Southeast Asian nations. Climate change, urbanization, migration, and vector habitat expansion have contributed to the changing epidemiological trends of vector-borne encephalitis worldwide [8].
In India, encephalitis continues to represent a major healthcare burden, particularly in rural and endemic regions. Acute encephalitis syndrome (AES) is commonly reported in states such as Uttar Pradesh, Bihar, Assam, and West Bengal, often affecting pediatric populations. Japanese encephalitis virus (JEV) has historically been one of the leading infectious causes of encephalitis outbreaks in India. However, several non-viral etiologies, including scrub typhus, enteroviruses, dengue virus, and bacterial infections, have also been implicated in AES cases. Limited healthcare infrastructure, delayed diagnosis, poor sanitation, and inadequate vaccination coverage further contribute to disease prevalence in resource-limited settings [9].
Seasonal fluctuations play a crucial role in encephalitis epidemiology, especially for vector-borne infections. Cases of mosquito-borne encephalitis often increase during monsoon and post-monsoon seasons due to favorable breeding conditions for vectors. Similarly, tick-borne encephalitis tends to occur more frequently in warmer months when outdoor activities increase human exposure to infected ticks. Such seasonal patterns assist healthcare systems in predicting outbreaks and implementing preventive public health interventions [10].
The epidemiology of autoimmune encephalitis has become increasingly important due to advancements in diagnostic technologies and growing clinical recognition. Previously considered rare, autoimmune encephalitis is now understood to occur at frequencies comparable to infectious encephalitis in some populations. Anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis is among the most commonly identified autoimmune forms, especially in young adults and females. Earlier underdiagnosis resulted from limited antibody testing and poor awareness among clinicians regarding psychiatric and neurological symptom overlap [11].
Despite medical advancements, encephalitis continues to cause substantial mortality and long-term disability. Survivors often experience persistent neurological complications such as cognitive impairment, epilepsy, speech disturbances, behavioral abnormalities, and motor dysfunction. Studies have reported mortality rates ranging from 5% to 30%, depending on disease etiology, timeliness of diagnosis, patient age, and treatment availability. Consequently, enhanced epidemiological surveillance, vaccination campaigns, early disease recognition, and improved healthcare infrastructure are essential for reducing the global disease burden of encephalitis [12].
3. Etiology and Risk Factors of Encephalitis
Encephalitis is a multifactorial neurological disorder caused by infectious and non-infectious agents that lead to inflammation of the brain parenchyma. The etiology of encephalitis can broadly be categorized into infectious encephalitis, primarily caused by viruses, bacteria, fungi, and parasites, and autoimmune encephalitis, where immune-mediated mechanisms attack neuronal tissues. Despite advances in diagnostic technologies, approximately 30–60% of encephalitis cases remain of unknown etiology, emphasizing the complexity of disease identification and pathogen detection [13].
Among infectious causes, viral infections are responsible for the majority of encephalitis cases worldwide. Viral pathogens possess neurotropic properties that enable them to invade the central nervous system (CNS) through hematogenous dissemination or retrograde neuronal transmission. Herpes simplex virus type 1 (HSV-1) is considered the leading cause of sporadic fatal encephalitis in adults due to its predilection for the temporal lobe. Other important viral agents include varicella-zoster virus (VZV), enteroviruses, arboviruses, rabies virus, cytomegalovirus (CMV), and Epstein–Barr virus (EBV). The prevalence of these infections varies depending on geographic region, climate, and vector exposure [14].
Autoimmune encephalitis has emerged as a significant cause of non-infectious encephalitis, particularly among younger individuals and females. This form of encephalitis results from antibodies directed against neuronal cell surface receptors or intracellular antigens. Anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis is among the most frequently diagnosed autoimmune encephalitis syndromes and often presents with psychiatric manifestations, seizures, cognitive dysfunction, and autonomic instability. Other autoimmune variants include anti-LGI1, anti-CASPR2, and anti-GABA receptor encephalitis [15].
Bacterial, fungal, and parasitic infections can also cause encephalitis, although they are relatively less common than viral etiologies. Organisms such as Mycoplasma pneumoniae, Listeria monocytogenes, Cryptococcus neoformans, Toxoplasma gondii, and Naegleria fowleri have been associated with encephalitic presentations, particularly in immunocompromised individuals. Opportunistic infections frequently occur in patients with HIV/AIDS, malignancies, organ transplantation, or immunosuppressive therapy, increasing the severity and complexity of clinical management [16].
Several host-related and environmental risk factors contribute to susceptibility to encephalitis. Age plays a crucial role, with neonates, children, and elderly individuals being at higher risk due to immature or weakened immune defenses. Immunocompromised states, poor vaccination status, vector exposure, travel to endemic regions, seasonal climatic conditions, and pre-existing neurological disorders further increase disease susceptibility. Genetic predisposition and altered immune responses may additionally influence disease severity and patient prognosis [17].
Table 1. Major Infectious Causes of Encephalitis
|
Causative Agent |
Type |
Mode of Transmission |
Clinical Features |
Common Geographic Distribution |
Citation |
|
Herpes Simplex Virus (HSV-1) |
Virus |
Reactivation/ Direct infection |
Fever, seizures, temporal lobe involvement |
Worldwide |
[14] |
|
Varicella-Zoster Virus (VZV) |
Virus |
Reactivation of latent infection |
Rash, headache, confusion |
Worldwide |
[14] |
|
Japanese Encephalitis Virus (JEV) |
Arbovirus |
Mosquito bite (Culex species) |
Fever, movement disorders, paralysis |
Asia, including India |
[18] |
|
West Nile Virus |
Arbovirus |
Mosquito bite |
Fever, meningitis, neurological deficits |
North America, Europe |
[19] |
|
Rabies Virus |
Virus |
Animal bite |
Hydrophobia, paralysis, fatal encephalitis |
Asia, Africa |
[20] |
|
Listeria monocytogenes |
Bacteria |
Contaminated food |
Brainstem encephalitis, fever |
Worldwide |
[16] |
|
Cryptococcus neoformans |
Fungus |
Inhalation |
Headache, altered consciousness |
Immuno-compromised patients |
[16] |
|
Toxoplasma gondii |
Parasite |
Foodborne/ Congenital |
Focal neurological symptoms |
Global |
[16] |
Table 2. Autoimmune Types of Encephalitis
|
Type of Autoimmune Encephalitis |
Target Antigen |
Major Symptoms |
High-Risk Population |
Citation |
|
Anti-NMDAR Encephalitis |
NMDA receptor |
Psychiatric symptoms, seizures |
Young adults, females |
[15] |
|
Anti-LGI1 Encephalitis |
LGI1 protein |
Memory loss, faciobrachial dystonic seizures |
Older adults |
[21] |
|
Anti-CASPR2 Encephalitis |
CASPR2 protein |
Neuromyotonia, confusion |
Elderly males |
[21] |
|
Anti-GABA Receptor Encephalitis |
GABA receptors |
Severe seizures, cognitive dysfunction |
Adults |
[15] |
Table 3. Major Risk Factors Associated with Encephalitis
|
Risk Factor |
Mechanism Increasing Risk |
Examples |
Citation |
|
Age Extremes |
Weak or immature immune response |
Children and elderly |
[17] |
|
Immunocompromised State |
Reduced host defense |
HIV/AIDS, chemotherapy |
[16] |
|
Geographic Exposure |
Exposure to endemic pathogens |
Rural areas with mosquitoes |
[18] |
|
Seasonal Variation |
Increased vector population |
Monsoon/post-monsoon seasons |
[10] |
|
Lack of Vaccination |
Increased susceptibility |
Japanese encephalitis outbreaks |
[22] |
|
Animal Exposure |
Transmission through bites |
Rabies infection |
[20] |
4. Pathophysiology of Encephalitis
The pathophysiology of encephalitis involves inflammation of the brain parenchyma resulting from direct invasion of infectious pathogens or abnormal immune-mediated responses. This inflammatory process disrupts normal neuronal functioning, leading to cerebral edema, neuronal destruction, altered neurotransmission, and neurological impairment. The severity of pathological damage depends on the causative agent, host immune response, duration of infection, and timeliness of therapeutic intervention. Brain inflammation can affect multiple regions including the cerebral cortex, temporal lobes, limbic system, and brainstem, thereby producing diverse neurological manifestations [23].
In infectious encephalitis, pathogens generally gain access to the central nervous system (CNS) through two principal mechanisms: hematogenous dissemination and retrograde neuronal transmission. In hematogenous spread, microorganisms enter systemic circulation and cross the blood–brain barrier (BBB), subsequently infecting neural tissues. Alternatively, certain neurotropic viruses, such as rabies virus and herpes simplex virus, migrate along peripheral nerves through retrograde axonal transport to reach the brain. Following CNS invasion, pathogens initiate inflammatory cascades that trigger neuronal injury and glial activation [24].
The blood–brain barrier serves as a protective physiological structure that restricts entry of harmful pathogens and toxins into neural tissues. However, during encephalitis, inflammatory mediators such as cytokines, chemokines, and adhesion molecules increase BBB permeability, allowing infiltration of immune cells into the brain. This heightened inflammatory response contributes to vasogenic edema, increased intracranial pressure, and neuronal dysfunction. Excessive inflammation may paradoxically worsen tissue injury despite its protective role in pathogen elimination [25].
Neuroinflammation plays a central role in disease progression and involves activation of microglia, astrocytes, macrophages, and infiltrating lymphocytes. Activated immune cells release pro-inflammatory cytokines including interleukin-1 (IL-1), tumor necrosis factor-alpha (TNF-α), and interleukin-6 (IL-6), which contribute to neuronal apoptosis and synaptic dysfunction. Persistent neuroinflammation can result in long-term neurological complications such as epilepsy, memory deficits, and cognitive dysfunction among survivors of encephalitis [26].
Herpes simplex virus encephalitis (HSVE), one of the most extensively studied forms of encephalitis, predominantly affects the temporal and frontal lobes of the brain. HSV causes necrotizing inflammation, hemorrhage, and edema, which frequently manifest as behavioral abnormalities, confusion, seizures, and memory disturbances. Delayed antiviral treatment in HSV encephalitis is strongly associated with poor neurological outcomes and irreversible brain damage due to extensive neuronal necrosis [27].
In autoimmune encephalitis, the underlying mechanism differs substantially from infectious causes, as brain inflammation results from immune-mediated targeting of neuronal receptors and synaptic proteins. Autoantibodies against receptors such as NMDAR interfere with synaptic transmission and neuronal signaling rather than directly destroying neural tissue. This disruption frequently manifests as psychiatric symptoms, cognitive decline, movement abnormalities, autonomic dysfunction, and refractory seizures. Unlike infectious encephalitis, autoimmune forms often respond favorably to immunotherapy when diagnosed promptly [28].
Brain edema and elevated intracranial pressure are critical pathological consequences observed in severe encephalitis cases. Inflammatory swelling may compromise cerebral blood flow and oxygen delivery, increasing the risk of ischemia, brain herniation, and death. Severe inflammation can additionally disturb neurotransmitter balance, contributing to altered consciousness, delirium, and seizure activity. These complications highlight the importance of rapid diagnosis and aggressive therapeutic management to prevent irreversible neurological injury [29].
The recovery phase of encephalitis is often influenced by the extent of neuronal damage and regenerative capacity of the nervous system. Although some patients achieve complete neurological recovery, others may develop long-term sequelae including motor dysfunction, behavioral disorders, epilepsy, speech impairment, and reduced quality of life. Chronic neuroinflammatory changes and neuronal loss may persist for months or years, emphasizing the importance of rehabilitation and long-term neurological monitoring in affected individuals [30].
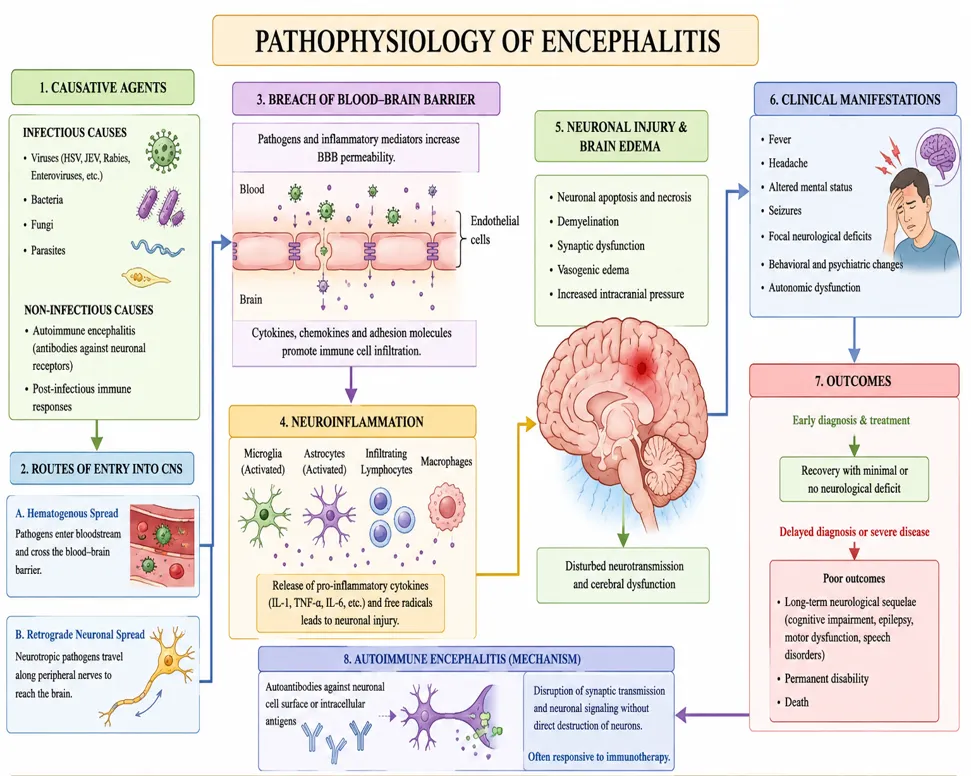
Figure 1. Pathophysiology of Encephalitis: Mechanisms of Brain Inflammation, Neuroinvasion, and Clinical Outcomes
5. Types of Encephalitis
Encephalitis is classified into different types based on etiology, mode of pathogenesis, causative organisms, and immune involvement. Broadly, encephalitis is categorized into infectious encephalitis and autoimmune encephalitis. Infectious encephalitis results from direct invasion of pathogens into the brain tissue, whereas autoimmune encephalitis occurs due to abnormal immune responses targeting neuronal structures. Accurate classification of encephalitis is crucial for diagnosis, treatment selection, and prediction of clinical outcomes because therapeutic strategies differ significantly depending on the underlying cause [31].
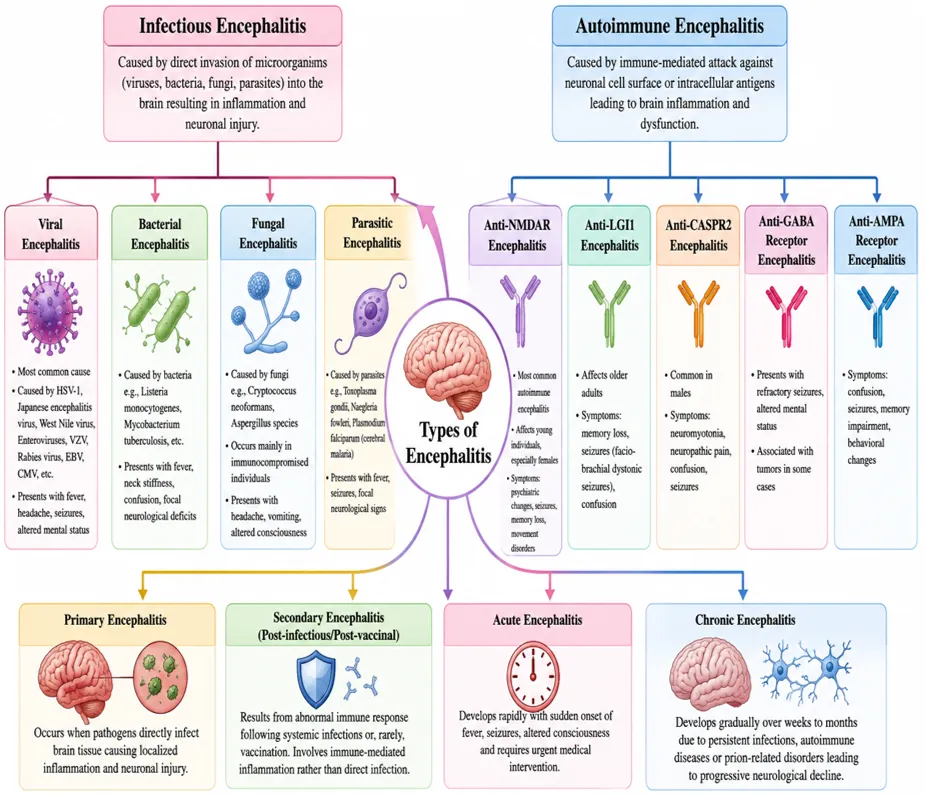
Figure 2: Classification and Types of Encephalitis
5.1 Infectious Encephalitis
Infectious encephalitis occurs when microorganisms directly infect and inflame brain tissues. Viral infections are the predominant cause of infectious encephalitis worldwide, accounting for the majority of reported cases. However, bacterial, fungal, and parasitic organisms may also contribute to disease development, particularly in immunocompromised individuals. The severity of infection depends on pathogen virulence, host immunity, and speed of clinical intervention [32].
5.1.1 Viral Encephalitis
Viral encephalitis is the most common form of encephalitis and is primarily caused by neurotropic viruses capable of invading the central nervous system. Herpes simplex virus type 1 (HSV-1) is the leading cause of sporadic fatal viral encephalitis in adults and often affects the temporal lobes, resulting in seizures, confusion, and behavioral abnormalities. Arboviruses such as Japanese encephalitis virus, West Nile virus, and tick-borne encephalitis virus are transmitted by arthropod vectors and contribute significantly to disease burden in endemic regions [33].
Enteroviruses, varicella-zoster virus, Epstein–Barr virus, cytomegalovirus, and rabies virus are also important viral causes of encephalitis. Rabies encephalitis is particularly severe because it is nearly always fatal after symptom onset if post-exposure prophylaxis is not administered promptly. Viral encephalitis may present acutely with fever, headache, altered mental status, and seizures, necessitating urgent antiviral therapy and supportive care [34].
5.1.2 Bacterial Encephalitis
Although less common than viral forms, bacterial encephalitis can occur due to direct invasion of bacteria into neural tissues or secondary complications of systemic infection. Listeria monocytogenes is a notable bacterial cause, particularly among elderly individuals, pregnant women, and immunocompromised patients. Bacterial encephalitis may present with fever, neck stiffness, confusion, and focal neurological deficits, often overlapping clinically with meningitis and meningoencephalitis [35].
5.1.3 Fungal and Parasitic Encephalitis
Fungal and parasitic encephalitis are relatively uncommon but can be life-threatening in immunocompromised patients. Opportunistic fungi such as Cryptococcus neoformans frequently affect patients with HIV/AIDS and organ transplantation. Parasitic infections including toxoplasmosis, cerebral malaria, and amoebic encephalitis caused by Naegleria fowleri may result in severe brain inflammation, cerebral edema, and high mortality rates. Early diagnosis is often difficult due to nonspecific clinical presentations [36].
5.2 Autoimmune Encephalitis
Autoimmune encephalitis represents a group of inflammatory neurological disorders caused by immune-mediated attacks against neuronal antigens. Unlike infectious encephalitis, there is no direct microbial invasion; instead, antibodies disrupt normal neuronal signaling and synaptic function. Anti-NMDAR encephalitis is among the most recognized forms and often presents with psychiatric symptoms, seizures, memory impairment, autonomic dysfunction, and abnormal movements. Many cases are associated with tumors such as ovarian teratomas, particularly in young females [37].
Other forms of autoimmune encephalitis include anti-LGI1, anti-CASPR2, anti-GABA receptor, and anti-AMPA receptor encephalitis. Each subtype presents unique neurological and psychiatric manifestations depending on the neuronal target involved. Increasing awareness and availability of antibody testing have significantly improved diagnosis and treatment outcomes in recent years. Immunotherapies including corticosteroids, intravenous immunoglobulin (IVIG), rituximab, and plasmapheresis are frequently used for management [38].
5.3 Primary and Secondary Encephalitis
Encephalitis may also be classified as primary or secondary based on disease origin. Primary encephalitis occurs when pathogens directly infect brain tissue, resulting in localized inflammation and neuronal injury. In contrast, secondary encephalitis, also known as post-infectious or post-vaccinal encephalitis, develops as a result of abnormal immune reactions following systemic infections or, rarely, vaccination. Secondary encephalitis may involve widespread demyelination and autoimmune inflammatory responses rather than direct pathogen invasion [39].
5.4 Acute and Chronic Encephalitis
Acute encephalitis develops rapidly and typically presents with sudden onset of fever, altered consciousness, seizures, and neurological dysfunction requiring emergency medical intervention. Chronic encephalitis, although less common, develops progressively over time and may result from persistent infections, autoimmune diseases, or prion-related neurodegeneration. Chronic forms often produce gradual cognitive decline, behavioral abnormalities, and movement disorders, leading to long-term disability [40].
6. Clinical Manifestations of Encephalitis
The clinical manifestations of encephalitis are highly variable and depend on factors such as the causative agent, brain region involved, patient age, immune status, and disease severity. Encephalitis often begins with non-specific prodromal symptoms resembling viral infections, followed by progressive neurological impairment. The hallmark feature distinguishing encephalitis from other infectious neurological disorders is altered mental status, which may include confusion, personality changes, irritability, or reduced consciousness. Clinical presentations may range from mild illness to life-threatening neurological emergencies requiring intensive care management [41].
In the early stages of encephalitis, patients frequently experience constitutional symptoms such as fever, headache, malaise, nausea, vomiting, and generalized weakness. These symptoms are often associated with systemic inflammatory responses and may precede neurological abnormalities by several days. Headache occurs due to inflammatory irritation of the meninges and elevated intracranial pressure, whereas fever results from immune-mediated pyrogenic responses to infection or inflammation. Because these symptoms are non-specific, early diagnosis is often difficult, potentially delaying appropriate treatment [42].
Altered mental status is considered one of the cardinal clinical features of encephalitis and may present as confusion, delirium, agitation, hallucinations, disorientation, or decreased responsiveness. In severe cases, patients may progress to stupor or coma due to extensive cerebral inflammation and neuronal dysfunction. Behavioral and psychiatric abnormalities are particularly prominent in autoimmune encephalitis and temporal lobe involvement, where patients may exhibit anxiety, psychosis, paranoia, emotional instability, and memory disturbances [43].
Seizures are common neurological manifestations of encephalitis and may occur as focal or generalized episodes depending on the affected brain region. Viral encephalitis, especially herpes simplex encephalitis, frequently involves temporal lobe inflammation, increasing seizure susceptibility. Persistent seizures or status epilepticus can lead to additional neuronal injury and poor neurological outcomes if not managed promptly. Children are particularly vulnerable to seizure-related complications due to increased neuronal excitability during brain development [44].
Neurological deficits such as weakness, paralysis, speech disturbances, movement abnormalities, and sensory impairment are frequently observed in encephalitis patients. Focal neurological signs may reflect localized inflammation within specific brain regions. For instance, cerebellar involvement may cause impaired coordination and ataxia, whereas frontal lobe inflammation may alter behavior and executive functioning. Cranial nerve abnormalities, tremors, and involuntary movements may also occur depending on disease progression and etiology [45].
Cognitive dysfunction is another significant manifestation, particularly among survivors of severe encephalitis. Patients often experience difficulties with memory, concentration, learning, language processing, and executive functioning even after apparent clinical recovery. Long-term neuropsychological complications can significantly affect education, employment, and quality of life. Cognitive impairment is especially common in patients with delayed diagnosis, severe inflammation, or prolonged intensive care hospitalization [46].
Autonomic nervous system dysfunction may develop in severe encephalitis cases, particularly autoimmune encephalitis. Patients may experience abnormalities such as fluctuating blood pressure, irregular heart rate, breathing difficulties, excessive sweating, urinary retention, and gastrointestinal disturbances. Such complications may require intensive monitoring because autonomic instability can contribute significantly to morbidity and mortality [47].
Clinical presentation often differs between children and adults. Pediatric patients commonly present with irritability, lethargy, poor feeding, seizures, and altered consciousness, while adults more frequently exhibit confusion, memory impairment, and psychiatric manifestations. Elderly individuals may present atypically with subtle cognitive changes or delirium, often complicating diagnosis and delaying treatment initiation. These age-related variations highlight the importance of individualized clinical assessment in encephalitis management [48].
Delayed recognition of clinical symptoms can significantly worsen prognosis and increase the risk of irreversible neurological damage. Therefore, healthcare professionals must maintain a high index of suspicion when patients present with fever, altered mental status, seizures, or focal neurological deficits. Prompt clinical evaluation combined with neuroimaging, cerebrospinal fluid analysis, and laboratory investigations remains essential for early diagnosis and improved therapeutic outcomes [49].
7. Diagnosis of Encephalitis
The diagnosis of encephalitis is often challenging because its clinical manifestations overlap with several neurological disorders, including meningitis, brain abscess, metabolic encephalopathy, stroke, and psychiatric illnesses. Early diagnosis is crucial because delayed intervention can lead to irreversible neurological damage, prolonged hospitalization, and increased mortality. A comprehensive diagnostic approach generally includes clinical evaluation, neurological examination, laboratory investigations, cerebrospinal fluid (CSF) analysis, neuroimaging, electroencephalography (EEG), and molecular diagnostic methods to identify the underlying cause of inflammation [50].
Clinical diagnosis begins with careful assessment of symptoms such as fever, headache, altered mental status, seizures, focal neurological deficits, and behavioral abnormalities. A detailed patient history involving recent infections, travel to endemic areas, vaccination status, exposure to insects or animals, and immunocompromised conditions can help identify possible etiological factors. Because encephalitis can rapidly progress, clinicians often initiate empirical treatment while confirmatory investigations are underway [51].
Cerebrospinal fluid (CSF) analysis remains one of the most important investigations for diagnosing encephalitis. Lumbar puncture is commonly performed to evaluate inflammatory changes within the CNS. Typical findings include elevated white blood cell count (pleocytosis), mildly increased protein concentration, and normal glucose levels in viral encephalitis. In autoimmune encephalitis, antibody testing in CSF may reveal disease-specific neuronal antibodies that assist in confirming diagnosis [52].
Neuroimaging techniques, particularly magnetic resonance imaging (MRI), play an essential role in detecting brain inflammation and identifying affected regions. MRI is generally more sensitive than computed tomography (CT) for diagnosing encephalitis and frequently reveals abnormalities involving the temporal lobe in herpes simplex encephalitis. Imaging findings may also help differentiate encephalitis from tumors, ischemic stroke, and other structural brain disorders [53].
Electroencephalography (EEG) is frequently used to detect abnormal electrical activity within the brain, especially in patients presenting with seizures or altered mental status. EEG findings in encephalitis may include generalized slowing, epileptiform discharges, or periodic lateralized epileptiform discharges (PLEDs), which are commonly associated with herpes simplex encephalitis. Although EEG findings are not disease-specific, they provide valuable supportive evidence for diagnosis [54].
Molecular diagnostic methods such as polymerase chain reaction (PCR) have revolutionized encephalitis diagnosis by enabling rapid identification of infectious pathogens from CSF samples. PCR testing is particularly valuable in herpes simplex encephalitis because early antiviral treatment significantly improves survival and neurological outcomes. Serological tests and antibody assays additionally assist in diagnosing arboviral and autoimmune forms of encephalitis [55].
Table 4. Diagnostic Methods Used in Encephalitis
|
Diagnostic Method |
Purpose |
Typical Findings |
Advantages |
Limitations |
Citation |
|
Clinical Examination |
Initial assessment of symptoms and neurological signs |
Fever, confusion, seizures, altered mental status |
Rapid, non-invasive |
Non-specific findings |
[51] |
|
Cerebrospinal Fluid (CSF) Analysis |
Detect CNS inflammation |
Pleocytosis, elevated protein, antibodies |
Essential for confirmation |
Invasive procedure |
[52] |
|
Magnetic Resonance Imaging (MRI) |
Detect brain inflammation and structural changes |
Temporal lobe abnormalities, edema |
High sensitivity |
Expensive, less accessible |
[53] |
|
Computed Tomography (CT) Scan |
Rule out structural lesions |
Brain swelling or hemorrhage |
Quick imaging |
Less sensitive than MRI |
[53] |
|
Electro-encephalography (EEG) |
Evaluate brain electrical activity |
Slowing, epileptiform discharges |
Useful for seizure detection |
Non-specific changes |
[54] |
|
Polymerase Chain Reaction (PCR) |
Identify infectious pathogens |
Viral DNA/RNA detection |
Highly sensitive and specific |
Limited pathogen range |
[55] |
|
Autoantibody Testing |
Diagnose autoimmune encephalitis |
NMDA, LGI1, CASPR2 antibodies |
Accurate for autoimmune forms |
Costly testing |
[56] |
Table 5. Differential Diagnosis of Encephalitis
|
Disease Condition |
Similar Symptoms |
Distinguishing Feature |
Citation |
|
Meningitis |
Fever, headache, altered consciousness |
Predominant meningeal irritation and neck stiffness |
[57] |
|
Brain Tumor |
Seizures, cognitive changes |
Progressive onset and imaging evidence |
[58] |
|
Stroke |
Sudden neurological deficits |
Vascular abnormalities on imaging |
[58] |
|
Metabolic Encephalopathy |
Altered mental status |
Metabolic imbalance without CNS inflammation |
[59] |
|
Psychiatric Disorders |
Behavioral changes, psychosis |
Absence of inflammatory neurological findings |
[56] |
Prompt and accurate diagnosis is essential for improving clinical outcomes in encephalitis. Because laboratory confirmation may take time, clinicians often initiate empirical antiviral therapy, especially acyclovir, when herpes simplex encephalitis is suspected. Combining clinical suspicion with advanced diagnostic tools substantially increases diagnostic accuracy and facilitates timely therapeutic interventions [60].
8. Treatment and Management of Encephalitis
The treatment and management of encephalitis primarily depend on the underlying cause, disease severity, and timing of intervention. Since encephalitis can progress rapidly and lead to irreversible neurological damage, immediate medical attention is essential. Initial management typically involves hospitalization, neurological monitoring, stabilization of vital functions, and empirical therapy while diagnostic confirmation is pending. Early initiation of treatment has been shown to significantly improve prognosis and reduce mortality, especially in infectious encephalitis [61].
Supportive care remains a fundamental component of encephalitis management regardless of etiology. Patients with severe disease often require admission to intensive care units (ICUs) for monitoring of respiratory function, cardiovascular stability, hydration, electrolyte balance, and neurological status. Supportive measures include oxygen therapy, intravenous fluids, nutritional support, fever control, and management of elevated intracranial pressure. In critically ill patients, mechanical ventilation may be necessary to maintain adequate oxygenation and prevent complications [62].
Antiviral therapy represents the cornerstone of treatment for viral encephalitis, particularly herpes simplex encephalitis (HSE). Intravenous acyclovir is the preferred first-line antiviral agent and should be initiated immediately when HSE is suspected, even before laboratory confirmation, because delayed treatment is strongly associated with poor neurological outcomes. Acyclovir acts by inhibiting viral DNA replication, thereby reducing viral proliferation and limiting neuronal damage. Other antiviral medications may be considered depending on the causative organism, including ganciclovir for cytomegalovirus infections [63].
Antibacterial and antifungal therapies are indicated when bacterial or fungal encephalitis is suspected or confirmed. Broad-spectrum antibiotics may initially be administered empirically in patients presenting with encephalitic symptoms accompanied by signs of bacterial infection. Antifungal agents such as amphotericin B and fluconazole are frequently used for fungal encephalitis, particularly in immunocompromised individuals. Selection of antimicrobial agents depends on pathogen sensitivity, patient condition, and severity of infection [64].
Management of autoimmune encephalitis differs substantially from infectious encephalitis and primarily focuses on immunotherapy. First-line treatments commonly include corticosteroids, intravenous immunoglobulin (IVIG), and plasmapheresis to suppress abnormal immune responses and reduce antibody-mediated neuronal damage. In cases resistant to initial therapy, second-line immunosuppressive agents such as rituximab or cyclophosphamide may be used. Prompt immunotherapy significantly improves neurological recovery and functional outcomes in autoimmune encephalitis patients [65].
Seizure management is an important aspect of encephalitis treatment because seizures frequently occur due to neuronal inflammation and cortical irritation. Antiepileptic drugs (AEDs) such as levetiracetam, valproate, and phenytoin are commonly administered to control acute seizures and prevent recurrent episodes. Patients experiencing status epilepticus require urgent intensive care intervention due to increased risk of brain injury, respiratory compromise, and mortality [66].
Management of raised intracranial pressure (ICP) is critical in severe encephalitis cases because cerebral edema can compromise cerebral perfusion and increase mortality risk. Therapeutic interventions may include osmotic agents such as mannitol, hypertonic saline, controlled ventilation, head elevation, and corticosteroid administration in selected cases. Continuous neurological monitoring is essential to detect worsening intracranial hypertension and prevent life-threatening complications such as brain herniation [67].
Rehabilitation and long-term supportive care are essential components of post-encephalitis recovery, particularly among survivors with neurological sequelae. Many patients experience persistent deficits including cognitive dysfunction, motor impairment, behavioral disturbances, epilepsy, speech difficulties, and memory loss. Multidisciplinary rehabilitation involving physiotherapy, occupational therapy, speech therapy, neuropsychological counseling, and psychiatric support helps improve functional independence and quality of life [68].
Table 6. Pharmacological Management of Encephalitis
|
Drug/ Therapy |
Indication |
Mechanism of Action |
Common Examples |
Citation |
|
Antiviral Therapy |
Viral encephalitis |
Inhibits viral replication |
Acyclovir, Ganciclovir |
[63] |
|
Antibiotics |
Bacterial encephalitis |
Eliminates bacterial pathogens |
Ceftriaxone, Vancomycin |
[64] |
|
Antifungal Drugs |
Fungal encephalitis |
Disrupt fungal cell integrity |
Amphotericin B, Fluconazole |
[64] |
|
Corticosteroids |
Autoimmune encephalitis |
Reduces inflammation and immune response |
Methylprednisolone |
[65] |
|
Intravenous Immunoglobulin (IVIG) |
Autoimmune encephalitis |
Modulates abnormal immunity |
Human immunoglobulin |
[65] |
|
Plasmapheresis |
Severe autoimmune encephalitis |
Removes pathogenic antibodies |
Therapeutic plasma exchange |
[65] |
|
Antiepileptic Drugs |
Seizure control |
Stabilizes neuronal activity |
Levetiracetam, Phenytoin |
[66] |
|
Osmotic Agents |
Raised intracranial pressure |
Reduces cerebral edema |
Mannitol, Hypertonic saline |
[67] |
Table 7. Supportive and Rehabilitation Strategies in Encephalitis
|
Supportive Strategy |
Purpose |
Clinical Importance |
Citation |
|
Intensive Care Monitoring |
Stabilize critical patients |
Prevent respiratory and neurological deterioration |
[62] |
|
Oxygen Therapy |
Maintain oxygenation |
Prevent hypoxia-related brain injury |
[62] |
|
Nutritional Support |
Improve recovery |
Prevent malnutrition during hospitalization |
[68] |
|
Physiotherapy |
Restore motor function |
Improve muscle strength and mobility |
[68] |
|
Speech Therapy |
Improve communication deficits |
Enhance language recovery |
[68] |
|
Neuropsychological Counseling |
Manage behavioral and cognitive problems |
Improve quality of life |
[68] |
Although significant advancements have been made in encephalitis treatment, prognosis remains dependent on early diagnosis and timely intervention. Delays in antiviral administration, particularly in herpes simplex encephalitis, are associated with severe neurological complications and increased mortality. Therefore, prompt multidisciplinary management involving neurologists, infectious disease specialists, intensivists, and rehabilitation teams is essential for improving patient outcomes [69].
9. Prevention Strategies and Prognosis of Encephalitis
Prevention of encephalitis primarily focuses on reducing exposure to causative pathogens, improving vaccination coverage, strengthening public health measures, and promoting early medical intervention. Since many encephalitis cases are associated with infectious agents, preventive strategies are particularly important in limiting disease transmission and reducing morbidity and mortality. Prevention approaches differ according to the type of encephalitis, geographical distribution, and specific risk factors associated with disease outbreaks [70].
Vaccination remains one of the most effective methods for preventing several forms of viral encephalitis. Vaccines against diseases such as Japanese encephalitis, measles, mumps, rubella (MMR), varicella, rabies, and tick-borne encephalitis have significantly reduced disease incidence in many regions. In endemic countries, mass immunization programs targeting children have substantially decreased Japanese encephalitis-related hospitalizations and mortality. Timely immunization according to national vaccination schedules is therefore critical for preventing encephalitic complications arising from vaccine-preventable infections [71].
Vector control measures are essential for preventing mosquito-borne and tick-borne encephalitis. Arboviral encephalitis, including Japanese encephalitis and West Nile virus encephalitis, is commonly transmitted through infected mosquito bites. Preventive strategies include eliminating stagnant water, using insect repellents, wearing protective clothing, installing mosquito nets, and implementing environmental sanitation programs. Public health awareness campaigns play a major role in educating communities regarding vector avoidance and disease prevention, particularly during seasonal outbreaks [72].
Animal bite prevention and prompt post-exposure management are critical for reducing rabies-associated encephalitis. Rabies remains a fatal neurological disease once clinical symptoms develop; however, immediate wound cleansing, rabies immunoglobulin administration, and post-exposure vaccination are highly effective in preventing disease progression. Public education regarding stray animal avoidance and vaccination of domestic pets further contributes to rabies prevention efforts [73].
Healthcare-associated preventive measures, including infection surveillance, early case identification, and rapid treatment initiation, are important for reducing complications associated with encephalitis. Patients presenting with fever, altered mental status, and seizures should receive prompt neurological assessment and empirical antiviral treatment when herpes simplex encephalitis is suspected. Early intervention can significantly reduce neuronal damage and improve survival outcomes, emphasizing the importance of clinician awareness and rapid diagnostic evaluation [74].
For autoimmune encephalitis, prevention strategies are more limited because the condition results from abnormal immune responses rather than infectious transmission. However, early recognition of symptoms, prompt antibody testing, and rapid initiation of immunotherapy can prevent severe neurological deterioration. In certain cases associated with tumors, especially ovarian teratomas, early tumor detection and removal contribute substantially to disease control and prevention of relapse [75].
The prognosis of encephalitis varies widely depending on the causative agent, patient age, severity of inflammation, speed of diagnosis, and treatment effectiveness. Viral encephalitis caused by herpes simplex virus can result in severe neurological disability or death if untreated; however, early acyclovir administration markedly improves survival. Autoimmune encephalitis generally demonstrates favorable outcomes when diagnosed early and treated aggressively with immunotherapy. Nevertheless, delayed diagnosis often leads to prolonged hospitalization and persistent neurological impairment [76].
Long-term complications are frequently observed among encephalitis survivors and may significantly affect quality of life. Persistent sequelae include epilepsy, cognitive deficits, behavioral disturbances, memory impairment, motor dysfunction, speech disorders, and psychiatric symptoms. Children recovering from encephalitis may additionally experience developmental delays and academic difficulties. Consequently, long-term follow-up and rehabilitation programs are essential for optimizing neurological recovery and psychosocial functioning [77].
Despite improvements in diagnostics, antiviral therapy, immunotherapy, and supportive care, encephalitis continues to remain a major cause of neurological morbidity worldwide. Future efforts should focus on expanding vaccination programs, improving public health surveillance, developing novel therapeutic approaches, and enhancing awareness regarding early clinical recognition. Strengthening healthcare infrastructure and access to timely medical intervention can significantly improve patient outcomes and reduce the overall burden of encephalitis [78].
10. Recent Advances and Future Perspectives in Encephalitis Research
Recent advances in encephalitis research have significantly improved understanding of disease mechanisms, diagnostic approaches, and therapeutic interventions. The emergence of advanced molecular techniques, immunological testing, and neuroimaging technologies has transformed the diagnosis and management of encephalitis. Improved recognition of autoimmune encephalitis, rapid pathogen detection methods, and personalized treatment strategies have collectively enhanced patient survival and neurological outcomes. Despite these advancements, encephalitis remains a major neurological challenge due to diagnostic complexity, variable clinical presentations, and limited treatment options for several etiologies [79].
One of the most important developments in encephalitis research is the advancement of molecular diagnostic technologies, particularly multiplex polymerase chain reaction (PCR), metagenomic next-generation sequencing (mNGS), and genomic profiling. These techniques enable rapid identification of infectious pathogens from cerebrospinal fluid samples, even when conventional microbiological tests fail to detect causative organisms. Metagenomic sequencing has shown particular promise in identifying rare, emerging, and previously undiagnosed pathogens, thereby reducing delays in treatment and improving diagnostic accuracy [80].
The increasing recognition of autoimmune encephalitis represents another major breakthrough in neurology and neuroimmunology. Advances in antibody testing have facilitated earlier diagnosis of disorders involving antibodies against neuronal surface proteins such as NMDA receptors, LGI1, CASPR2, and GABA receptors. Improved awareness among neurologists and psychiatrists has reduced misdiagnosis of autoimmune encephalitis as psychiatric illness, allowing earlier initiation of immunotherapy and better functional recovery among affected individuals [81].
Artificial intelligence (AI) and machine learning are emerging as valuable tools in encephalitis diagnosis and prognosis prediction. AI-assisted analysis of neuroimaging data, electroencephalography (EEG) signals, and clinical biomarkers has demonstrated potential in identifying disease patterns and differentiating encephalitis subtypes. Predictive models may assist clinicians in recognizing severe disease early, optimizing therapeutic decisions, and forecasting long-term neurological outcomes. Although still under development, AI-based diagnostic support systems may play a substantial role in future neurological practice [82].
Novel therapeutic strategies are also being explored to improve encephalitis treatment outcomes. Researchers are investigating targeted immunotherapies, monoclonal antibodies, antiviral drug optimization, stem cell therapies, and neuroprotective interventions aimed at minimizing neuronal injury. For autoimmune encephalitis, biologic therapies such as rituximab and tocilizumab have demonstrated promising results in refractory cases resistant to first-line immunotherapy. Similarly, development of broad-spectrum antiviral agents may improve treatment options for emerging viral encephalitis pathogens [83].
Vaccine development and global surveillance systems have further contributed to prevention and outbreak control of encephalitis-causing pathogens. Enhanced vaccination strategies for arboviral infections, improved rabies prevention programs, and international infectious disease monitoring systems have strengthened public health preparedness. Climate change and globalization, however, continue to increase the risk of emerging vector-borne encephalitis outbreaks, emphasizing the need for continuous epidemiological surveillance and adaptive prevention strategies [84].
Biomarker discovery has become an important area of research for improving early diagnosis and monitoring treatment responses in encephalitis. Investigators are studying cerebrospinal fluid proteins, inflammatory cytokines, neuronal autoantibodies, and neurodegenerative markers to predict disease severity and prognosis. Reliable biomarkers could help clinicians differentiate infectious from autoimmune encephalitis and tailor treatment plans more effectively [85].
Future perspectives in encephalitis research emphasize multidisciplinary collaboration between neurologists, infectious disease specialists, immunologists, psychiatrists, and molecular scientists. Development of rapid diagnostic platforms, personalized immunotherapy, advanced neurorehabilitation methods, and novel antiviral compounds may substantially improve patient outcomes in the coming decades. Greater awareness, healthcare accessibility, and research funding are also necessary to reduce the global burden of encephalitis and its associated neurological disabilities [86].
CONCLUSION
Encephalitis is a serious and potentially life-threatening neurological disorder characterized by inflammation of the brain tissue resulting from infectious and non-infectious causes. Viral infections, particularly herpes simplex virus, remain the most common etiological factors, while autoimmune encephalitis has gained increasing recognition due to advances in immunological diagnostics. The disease affects individuals across all age groups and presents with a broad spectrum of clinical manifestations, ranging from mild flu-like symptoms to severe neurological complications such as seizures, altered consciousness, cognitive dysfunction, and coma.
The diagnosis of encephalitis remains clinically challenging because of overlapping symptoms with other neurological and psychiatric disorders. However, advances in neuroimaging, cerebrospinal fluid analysis, electroencephalography, molecular diagnostic techniques, and antibody testing have considerably improved diagnostic accuracy. Early recognition and rapid diagnosis are essential to prevent irreversible neuronal damage and improve patient prognosis.
Treatment strategies vary depending on the underlying etiology of encephalitis. Antiviral medications, especially acyclovir, are highly effective in treating viral encephalitis when administered promptly. Autoimmune encephalitis requires immunotherapeutic interventions including corticosteroids, intravenous immunoglobulin, plasmapheresis, and biologic therapies. Supportive care, intensive monitoring, seizure management, and long-term rehabilitation also play essential roles in improving patient recovery and minimizing neurological sequelae.
Preventive approaches such as vaccination, vector control, public awareness, and rapid medical intervention remain important in reducing disease burden globally. Despite substantial advancements in diagnostics and treatment, encephalitis continues to pose a major challenge due to delayed diagnosis, emerging pathogens, and long-term neurological complications among survivors.
Future research focusing on advanced diagnostics, personalized therapeutics, artificial intelligence-based clinical prediction, biomarker discovery, and innovative neuroprotective strategies may further improve disease outcomes. Strengthening healthcare systems, increasing awareness, and expanding access to timely medical care will be critical in reducing morbidity, mortality, and disability associated with encephalitis worldwide.
REFERENCES

Shruti Bongale, Srushti Barwade, Sushilkumar Sarvagod, Dhanraj Jadge, Encephalitis Disease: Pathophysiology, Clinical Manifestations, Diagnosis, Treatment, and Recent Advances, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 97-118. https://doi.org/10.5281/zenodo.20483906
 10.5281/zenodo.20483906
10.5281/zenodo.20483906