
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Matoshri College of Pharmacy, Eklahare, Nashik -422105.
Epilepsy is a long-term neurological condition characterized by recurrent seizures resulting from abnormal electrical discharges in the brain. It affects millions of individuals worldwide and poses significant clinical, psychological, and social challenges. This review summaries the current understanding of epilepsy, including its pathophysiology, classification, causes, clinical features, and diagnostic methods. Modern classification systems categories epilepsy by structural, genetic, infectious, metabolic, immune, and unknown etiologies. Diagnostic techniques such as electroencephalography, magnetic resonance imaging, and other neuroimaging tools play an important role in identifying seizure types and their origin. Pharmacological therapy using anti-seizure medications remains the primary treatment; however, a considerable number of patients develop drug-resistant epilepsy. In such cases, alternative approaches such as surgical intervention, neurostimulation devices, and dietary therapies like the ketogenic diet are considered. Recent advances including gene therapy, precision medicine, and artificial intelligence-based monitoring systems are contributing to more personalized treatment strategies. Despite these developments, challenges such as treatment gaps and social stigma continue to affect patient care. Continued research and improved healthcare access are essential to enhance the quality of life of individuals with epilepsy.
Epilepsy
Epilepsy is a long-term neurological condition characterized by recurrent seizures caused by abnormal brain activity, impacting around 50 million individuals globally. These frequent "attacks" are caused by abnormal electrical activity in the brain, which disturbs behavior, consciousness, and sensory perception. Because people with this condition frequently experience stigma, discrimination, and human rights violations, it affects their social position in addition to their health. In low-income countries, over 75% of people are deprived of accessible, safe, and effective antiseizure medications necessary to manage their seizures [1]. "Convulsions" refer to intermittent disturbances in brain function caused by an overactive synchronisation of neurons. The phrase "epileptic seizures" is specifically designated for seizures resulting from atypical neuronal firing, distinguishing them from non-epileptic incidents such as psychogenic seizures. When seizures occur repeatedly and without provocation, the diagnosis typically made is epilepsy. There are numerous triggers for epilepsy, all associated with fundamental brain dysfunction [2]. Epileptic seizures are marked by excessive or hypersynchronous abnormal neuronal activities in the cerebral cortex, which is the brain's outer layer. Epilepsy is described as a long-term brain disorder characterised by a consistent tendency to produce spontaneous seizures that have no immediate triggers like a central nervous system injury [3]. An epilepsy syndrome denotes a collection of typical clinical characteristics that appear together, including distinct seizure types, EEG results, and triggers. These syndromes can indicate the progression of the disorder and the potential effectiveness of antiepileptic drugs (AEDs). The phrase "epilepsy syndrome" acts as a general term for seizures that exhibit these traits.
History
The Greek words "epilambanein," which means "to take hold of," and "epilepsia," which means "to grasp upon," are the source of the English word "epilepsy." Indications of epilepsy can be found in the oldest medical records, indicating that people have been aware of the ailment for a long time. In the past, it was thought that epilepsy had a spiritual origin. Epilepsy was frequently linked in ancient societies to religious convictions or demonic possession [4]. In the past, epilepsy was often seen as a condition affected by demonic spirits or divine visions, and it was believed to have spiritual importance. In some Hmong communities that practiced animism, it was thought to be an attack by a demonic entity, but the affected person might also become a shaman as a result of their experiences [5]. The earliest known description of an epileptic seizure, written in Akkadian around 2000 BC, links the condition to a moon god and suggests exorcism as a treatment. The Code of Hammurabi, which dates to approximately 1790 BC, states that a slave with epilepsy may be returned for a refund. Cases of epileptic seizures are also documented in the Edwin Smith Papyrus, which dates to around 1700 BC [6]. The Sakikku, a Babylonian medical text composed between 1067 and 1046 BC, has the earliest thorough account of epilepsy, including its signs, symptoms, and treatments. It describes several sorts of seizures and attributes their source to demonic spirits, promoting spiritual remedies above medical ones because to the lack of a biological explanation of the ailment [4]. The Ayurvedic classic Charaka Samhita, written circa 400 BC, accepted Punarvasu Atreya's description of epilepsy as a loss of consciousness approximately 900 BC [7]. Jean-Martin Charcot asserted that epileptic patients were always mentally retarded at the Salpetriere, which is regarded as the foundation of modern neurology. He attributed this condition to either criminal insanity or chronic syphilis [8]. In the fifth century BC, Hippocrates rejected the belief that epilepsy was caused by spirits in his writings on the Sacred Disease. He said that epilepsy developed medically in the brain and called anyone who associated it with supernatural causes foolish. Hippocrates addressed the physical characteristics and social humiliation associated with the illness, emphasized inheritance as an important factor, and acknowledged worse outcomes when the disorder appears early. His description of epilepsy as the "great disease" gave rise to the phrase "grand mal" for tonic-clonic seizures. Hippocrates insisted that epilepsy is not a divine disease and may be quickly cured, but his beliefs about its physical roots were ignored in his day, and evil spirits were blamed for it until at least the 17th century [4, 6]. In the past, people with epilepsy have faced stigma and incarceration. In Tanzania and other African countries, epilepsy is still commonly believed to be caused by witchcraft, poisoning, or evil spirits. The Romans called it Morbus comitialis, meaning "disease of the assembly hall," because they believed it was a divine scourge. Although stigma persists, it is gradually decreasing, particularly in wealthy nations [8, 9]. Bromide, the first successful anti-seizure drug, was developed in the middle of the 19th century [10]. Phenytoin was initially used in 1938 after phenobarbital, the first modern therapy, was created in 1912 [11].
Types of Epilepsy
Table No.1- Types of Epilepsy
|
Type |
Description |
|
Generalised seizures |
|
|
Generalised tonic-clonic seizures (GTCS, major epilepsy, grand mal) [12] |
The most typical lasts between one and two minutes. Aura, sobbing, unconsciousness, tonic and clonic convulsions of all bodily muscles, extended slumber, and paralysis of all central nervous system functions are typical occurrences. |
|
Absence seizures (minor epilepsy, petit mal) [13] |
It lasts roughly thirty seconds and is common among children. The patient freezes and looks in one direction; there is no obvious muscle spasm, slight bilateral jerking, or momentary loss of consciousness. Three cycles per second is a typical EEG wave and spike pattern. |
|
Atonic seizures (Akinetic epilepsy) [14] |
It also called epileptic attacks characterized by a sudden loss or diminution of muscle tone. This last under 15 min. unconsciousness due to excessive inhibitory secretions causing relaxation of all muscles. |
|
Myoclonic seizures [12] |
A sudden shock-like contraction of the muscles of a limb or body. Infantile arrhythmia or convulsions observed in infants. Probably not the epileptic type. Muscle spasms that come and go and a steady decline in mental capacity. Diffuse changes are noticeable in the EEG between seizures. |
|
Partial seizures [Focal Seizure] |
|
|
Simple partial seizures (SPS, cortical focal epilepsy, focal aware seizures) [15] |
lasts fifty to one minute. Often by accident. Depending on the part of the cortex involved in the seizure, originate from a specific brain area without impairing consciousness or awareness. |
|
Complex partial seizures (CPS, temporal lobe epilepsy, psychomotor) [15] |
Seizures characterized by strange and irregular behaviour, purposeful movements and emotional changes lasting 1-2 minutes with loss of consciousness. Plows often come first. The temporal lobe is the home of the grasping target. |
|
Simple partial or complex partial seizures secondarily generalized [16] |
A partial seizure is followed by loss of consciousness and generalized tonic-clonic seizures. |
Causes of Epilepsy
The cause of epilepsy is unknown in 60% of occurrences. In other instances, it could be linked to brain abnormalities caused by severe brain injuries, strokes, infections such as meningitis or encephalitis, congenital malformations, brain tumours, or metabolic issues.
The International League Against Epilepsy (ILAE) classifies the six causes of epilepsy as structural, genetic, infectious, metabolic, immunological, and unknown. A single individual may be impacted by multiple causes because these categories may overlap [17].
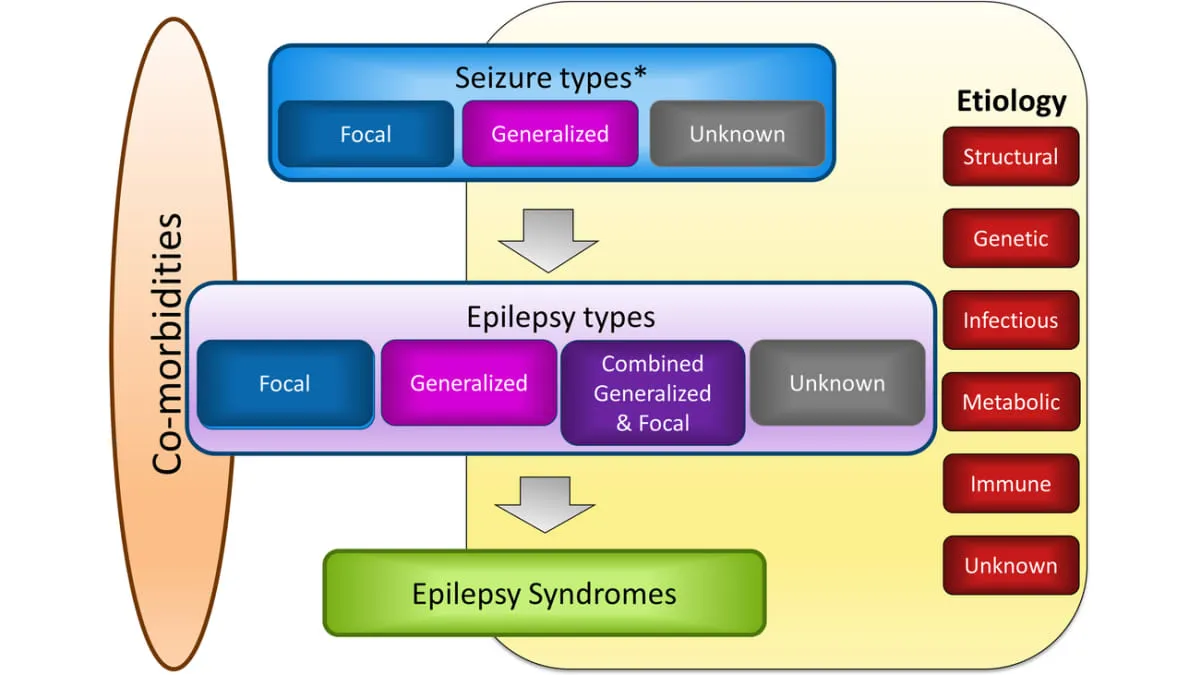
Figure No 1: Type and Causes of Epilepsy
Structural causes of epilepsy include developmental or genetic issues like focal cortical dysplasia and mesial temporal sclerosis, as well as acquired factors like stroke, traumatic brain injury (TBI), brain tumors, or infections that increase the risk of seizures [18]. Traumatic brain injury (TBI) accounts for 6–20% of epilepsy occurrences, with severity impacting risk; strokes induce seizures in 6–10% of older persons, especially following severe cortical events. Brain tumors account for about 4% of cases [19]. Neuroimaging methods like MRI are crucial for identifying structural epilepsy through abnormalities that correspond with seizure activity. Additionally, prenatal issues and recurring infections can raise the chance of epilepsy. For patients whose medication-resistant seizures are linked to specific lesions, surgical alternatives may be considered.
Epilepsy often has a genetic component; some persons are predisposed to seizures from birth. DNA differences can alter brain proteins and increase the likelihood of seizures, according to scientific research. These differences can either emerge naturally or be inherited by a child. Moreover, epilepsy may result from a combination of hereditary and environmental causes [20]. Numerous gene mutations that control brain activity are among the many genetic causes of epilepsy, which frequently result in aberrant electrical signalling and seizures. Both common and unusual types of epilepsy are significantly influenced by these genetic variables, which can be inherited or develop on their own [21]. The majority of them are brought on by interactions between many genes and environmental elements [22]. The choice of genetic testing is influenced by a number of variables. These are the most widely used genetic testing for epilepsy: [20,23,24]
Epilepsy gene panels assess a range of genes associated with epilepsy, ranging from fewer than 20 to several hundred. However, they often produce ambiguous results and may overlook freshly discovered genes when compared to entire genome or exome sequencing [25].
The primary symptom of autoimmune epilepsy (AE), which is brought on by alterations in immune function, is seizures. AE was recently categorized as epilepsy by the International League Against Epilepsy (ILAE). The immune system, which consists of cells including macrophages, B cells, T cells, and antibodies, is mostly responsible for the body's defence. AE is often underestimated, and its true incidence is unknown. Cases with an autoimmune etiology must be identified since these individuals may benefit from immunotherapy but not react to traditional antiseizure medications [26].
Rasmussen's disease, anti-NMDA receptor encephalitis, limbic encephalitis (associated with LG1, CASPR2, and other antibodies), and GAD65 antibody-related epilepsy are specific forms of autoimmune epilepsies.
The primary reason of metabolic causes of epilepsy is disorders affecting the body's metabolism, typically caused by hereditary enzyme shortages or biochemical imbalances. These disruptions can affect brain function and raise the risk of seizures by depriving the brain of energy sources, accumulating toxins, or altering osmolality. Metabolic epilepsy develops when these diseases produce epilepsy, and traditional antiepileptic medications often fail to treat the underlying metabolic issues [27].
Common metabolic causes- [28]
Unknown causes of epilepsy highlight the limitations of scientific understanding and diagnostic techniques because they cannot be definitively recognized despite extensive study. This group includes a large number of epilepsy cases, especially in areas with limited access to advanced testing [17].
Symptoms [29]
Symptoms during seizure-
Table No.2- Symptoms of Epilepsy
|
Type of Epilepsy |
Symptoms |
|
Generalised tonic-clonic |
Loss of consciousness with collapse; tonic phase: generalised body stiffening; clonic phase: violent jerking; post-ictal state: deep sleep; other symptoms: tongue biting and urinary incontinence |
|
Absence |
Loss of consciousness for a few seconds, staring blankly, subjective loss of time |
|
Myoclonic |
Brief sporadic electrical shock-like jerking movements |
|
Clonic |
Violent rhythmic jerking movements |
|
Tonic |
Rigidity and stiffening |
|
Atonic |
Loss of muscle tone leading to a fall |
|
Focal aware seizure |
Awareness maintained; four subcategories: motor – jerking, stiffening and others; sensory – the five senses affected (if the patient experiences sensory symptoms only, the term aura is used); autonomic; psychological – memory, emotions or other phenomena |
|
Focal impaired awareness seizure |
Awareness impaired, automatisms |
Post Seizure symptoms [30]
The postictal state is the period of time following an epileptic seizure that is characterized by behavioural, motor, and cognitive alterations until normal neurological function is restored. According to a comprehensive review, symptoms might vary widely in terms of nature, intensity, and duration, ranging from three seconds to around 12.3 days. A 2019 meta-analysis identified up to 31 postictal symptoms, the most common of which were headaches, migraines, psychosis, Todd's paresis, aphasia, cognitive impairments, and automatisms.
Prevention
It is predicted that 25% of occurrences of epilepsy might be avoided.
Diagnosis
In order to diagnose epilepsy, medical professionals evaluate symptoms and medical history. They note that epilepsy is often underdiagnosed in paediatric patients, which can have negative consequences like intellectual disability and school dropout. For diagnosis, standard EEG recordings are typically utilized. Antiepileptic drugs can control about 60% of seizures; nevertheless, certain individuals may require surgical excision of epileptogenic foci for improved care. Successful treatment depends on the precise identification of the seizure-generating region, which calls for advanced imaging techniques as CT, MRI, PET/SPECT, MEG, and MRS [31]. Tests that can be performed to diagnose epilepsy include a neurological examination, blood tests, and genetic testing to identify the underlying cause of seizures.
The human electroencephalogram (EEG), which records electrical activity in the brain using scalp electrodes, was created in 1929 by psychiatrist Hans Berger. By identifying abnormal patterns that indicate epilepsy and identifying interictal epileptiform discharges even in the absence of seizures, it aids in diagnosis and classification [32].
An improved variant of the traditional EEG test, high-density EEG places electrodes closer together on the scalp to increase the accuracy of detecting the brain areas associated with seizure activity [33].
The computed tomography (CT) scan, which creates precise cross-sectional images of the brain using X-rays, is the main imaging technique used to diagnose epilepsy by identifying acute structural abnormalities. The word "tomography" comes from the Greek word "tomo," which meaning section, highlighting its focus on sectional radiology [31, 34].
MRI is regarded as the gold standard for structural imaging in epilepsy because of its superior soft tissue contrast, multi-plane imaging capability, and absence of ionizing radiation. Compared to CT scans, it provides more thorough insights into brain structure, which helps identify the causes of seizures [35].
A tiny amount of radioactive tracer is administered intravenously during PET scans in order to map brain metabolic activity and spot anomalies. Seizure onset zones frequently coincide with areas with hypometabolism.
Single-photon emission computed tomography (SPECT) is a nuclear medicine technique that creates three-dimensional images of tissue and organ function. Unlike conventional imaging, SPECT evaluates physiological processes by measuring the uptake and distribution of an administered radioactive tracer. Because it is crucial for the diagnosis of skeletal, neurological, and cardiac problems, this capability has been extensively employed in clinical practice and research since the late 20th century [36].
These assessments evaluate speech, memory, and cognitive abilities. The test results aid in identifying the parts of the brain that are impacted by seizures.
Treatment
The treatment for epileptic seizure includes first aid, therapeutics, gene therapy, ketogenic diet and surgery [30].
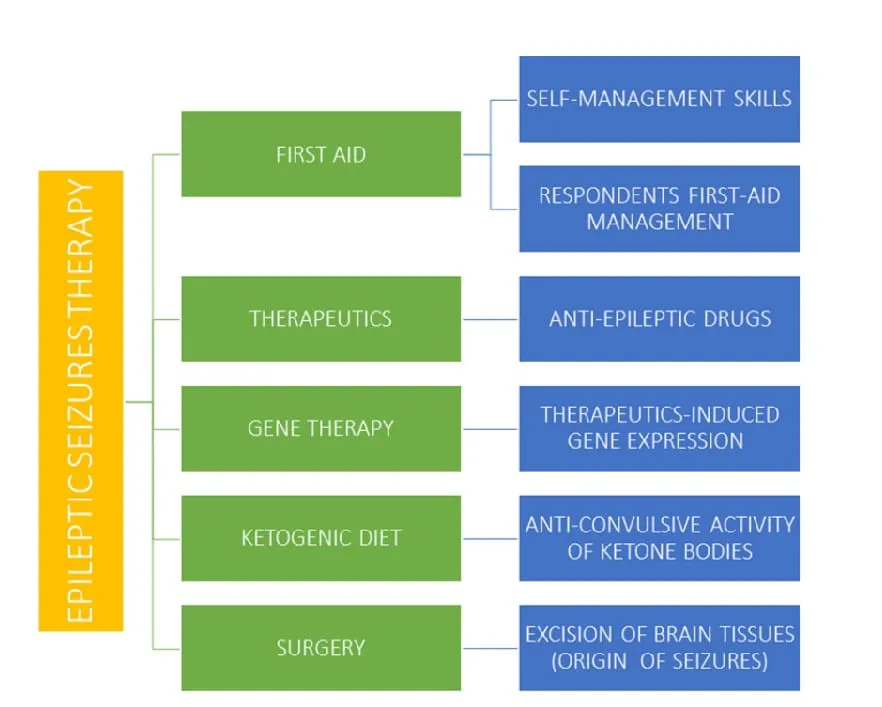
Figure No.2 – Treatment of Epilepsy
The cornerstone of treating epilepsy is anti-seizure drugs (ASMs), although those with drug-resistant epilepsy have other choices, including surgery, neurostimulation, and therapeutic diets. By 2026, precision medicine and AI monitoring systems will be used more frequently in clinical practice.
In order to administer first aid for epileptic seizures, bystanders must move swiftly, emphasizing the significance of remaining calm and supportive. Because stigma and misunderstandings can increase dread during a seizure, appropriate responses are essential. Important actions include keeping an eye on how long the seizure lasts and assessing the patient's blood sugar, pulse, and respiration. Transient cyanosis may result from acute respiratory muscle paralysis, although it usually disappears after the seizure, which typically lasts two to three minutes without having any potentially lethal effects. If a seizure lasts more than five minutes or happens again without recovering consciousness, emergency services must be called. After the seizure is over, the patient should be soothed and given time to rest because post-ictal tiredness may result in prolonged sleep for several hours or even a day.
For most patients, anti-epileptic or anticonvulsant medications are the first-line therapy and the primary means of managing epileptic seizures. Approximately 70% of patients can control their seizures with the correct medicine.
Many persons with epilepsy can effectively manage their disease with a single anti-seizure medication, however some may need a combination for greater control. Children who are symptom-free may discontinue treatment, and many people who have been seizure-free for two years may stop taking medication with a doctor's consent. When choosing the right medication and dose, medical experts must take into account variables like age, the kind and frequency of seizures, and any drug interactions [38]. Numerous adverse side effects are possible with anti-seizure medications. Typical mild side effects include fatigue, light-headedness, weight gain, decreased bone density, skin rashes, poor coordination, difficulty speaking, and cognitive issues. More serious but rare adverse effects include depression, suicidal thoughts or behaviours, severe skin responses, and organ inflammation, especially the liver.
When medicine is ineffective (drug-resistant epilepsy) and the seizures come from a particular, safely detachable area of the brain, surgery is a possibility.
For focal epilepsy that does not respond to medicine, a successful treatment is resective surgery, which includes removing the part of the brain that causes seizures. The objective is to cease seizure activity, but even tiny resections can significantly change brain networks. It is essential to understand these alterations in order to improve surgical results. The treatment is appropriate for non-eloquent areas in order to preserve essential capabilities such as speech or movement.
MRI-guided lasers are used in minimally invasive ablation, particularly in laser interstitial thermal treatment (LITT), which uses tiny skull incisions to remove brain tissue that causes seizures. Compared to surgical resection, this method offers a less intrusive way to treat drug-resistant focal epilepsy. Despite its proven usage for incurable tumors, its applicability in adult focal epilepsy has not been thoroughly investigated.
Increased health hazards are linked to medically refractory epilepsy. Patients with focal epilepsy who have detectable imaging abnormalities can benefit from open surgical resection, but it may cause neurological and cognitive problems [41]. A less invasive option is MR-guided laser interstitial thermal treatment (MRgLITT), which uses a tiny cannula and real-time temperature monitoring to precisely kill specific brain tissue. This approach is appropriate for treating seizures from deep brain regions like the hippocampus and amygdala because it minimizes harm to neighbouring areas, lowers surgical risks, and shortens hospital stays [42].
Using high-intensity sound waves to ablate or modify seizure-causing brain tissue while being directed by real-time MRI for improved precision, MR-guided focused ultrasound (MRgFUS) is a revolutionary, incisionless treatment for drug-resistant epilepsy. Recent technological developments and the continuous trend toward less invasive neurosurgery techniques are reflected in this strategy [43, 44].
The isolation procedure, sometimes referred to as disconnection surgery, is being researched as a substitute for resective surgery in the treatment of seizures. This method aims to functionally isolate important, vascularized brain tissue from the healthy hemisphere; it was initially used in functional hemispherectomy [45]. Disconnected treatments target the neuronal circuits that cause seizures in people with medication-resistant epilepsy, whereas resective surgeries maintain the integrity of brain tissue.
When medicine and reconstructive surgery are ineffective for treating drug-resistant epilepsy, neurostimulation devices can be used as a palliative measure by delivering electrical pulses that alter brain activity and lessen seizures.
Vagus nerve stimulation (VNS) is a surgical neuromodulator treatment that involves implanting a device to stimulate the vagus nerve, which connects many organs to the brainstem. The apparatus is made up of a pulse generator that is placed under the skin of the chest and attached to a lead that surrounds the neck's left vagus nerve. In around half of the patients, VNS reduced seizures by more than 50% within two years after FDA approval in 1997 [46]. Patients with drug-resistant epilepsy experience fewer and milder seizures as a result of VNS's continuous electrical impulses to the vagus nerve [47]. Recent advancements include closed-loop VNS devices that employ EEG monitoring to detect seizure activity and automatically start stimulation [48].
Responsive neurostimulation (RNS) is an FDA-approved treatment for individuals with drug-resistant focal epilepsy. It employs focused electrical pulses to halt seizures and electrocorticography (ECoG) to detect abnormal brain activity. Electrodes monitor ECoG signals, and the neurostimulator generates biphasic pulses when specific patterns are identified. In addition to long-lasting benefits in quality of life, research shows a 75% median reduction in seizures over a nine-year period, with a 73% responder rate and more than one-third of patients achieving ≥90% improvement. Patients with multifocal or eloquent-area epilepsy who are not candidates for surgery can benefit greatly from RNS because of its low rate of complications, notably infection [49,50].
There are multiple steps in the RNS system's mechanism of action:[51]
Deep-brain stimulation (DBS) is a safe and effective neurosurgical method for treating movement disorders and drug-resistant epilepsy. Electrodes are implanted, typically in the anterior nucleus of the thalamus (ANT), and linked to a chest-mounted pulse generator that continuously stimulates the brain at high frequencies in order to control seizure networks [52]. High-frequency stimulation (>100 Hz) influences hypersynchronous neuronal firing, raises seizure thresholds, and may promote neuroplasticity through a number of methods. Since FDA clearance in 2018, DBS has shown median seizure reductions of 41–68% in 1-3 years, surpassing sham stimulation by about 29%. Over 50% long-term seizure reduction has been attained by nearly half of the patients. Patients who have not benefited from reconstructive surgery and have low rates of complications—such as infection in roughly 3% of cases—should consider DBS. Over time, both focal and generalized epilepsies usually see improved clinical improvements [53].
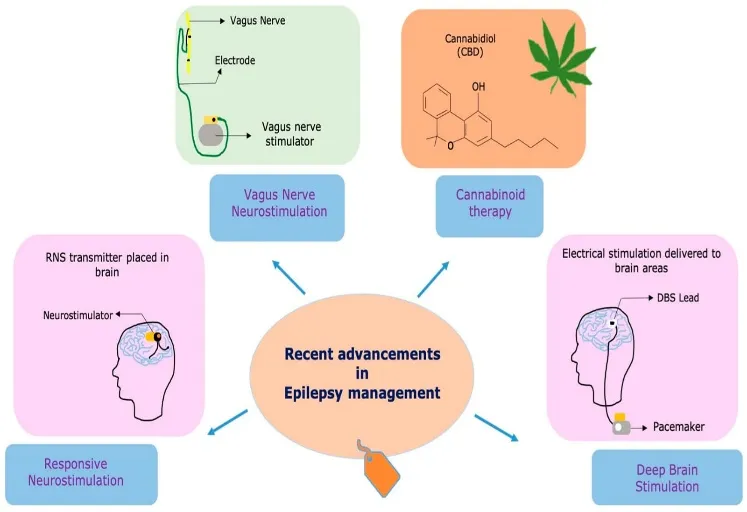
Figure No.3 – Recent technologies and therapies for management of epilepsy
The ketogenic diet aims to mimic the metabolic consequences of fasting by eating a high-fat, low-carb diet. As a result, energy metabolism shifts from using carbs to fats, producing ketone bodies as the brain's alternative fuel. Since the 1920s, it has been used medicinally to treat drug-resistant epilepsy, especially in youngsters [55]. The ketogenic diet (KD) enhances GABA-mediated inhibition and mitochondrial efficiency while reducing neuronal excitability by raising circulating ketone bodies. It comprises versions like the classic KD (4:1 fat to carbohydrate protein), the modified Atkins diet (MAD), and low-glycemic index therapy. After three to six months of KD therapy, 50–60% of children with drug-resistant epilepsy obtain seizure independence; in other cases, significant decreases are observed. Improvements in EEG activity and long-term benefits are observed at 24 months, especially in individuals with structural brain abnormalities [56].
Gene therapy, which was first developed to repair damaged genes, now includes more extensive gene-based treatments that transfer genetic material or change gene expression. When it comes to neurological problems, this is particularly crucial. One novel method is to alter mRNA transcription using RNA interference or antisense oligonucleotides [57]. Recent advances in gene editing, especially with CRISPR-Cas9, make it possible to precisely alter DNA sequences, which helps researchers modify genes associated with epilepsy and investigate their effects on seizure susceptibility.
[58].
CONCLUSION
Epilepsy continues to be a complex, multidimensional neurological disorder that significantly affects global health. This review focuses on its diverse pathophysiology, classification, etiological factors, and wide variety of clinical manifestations. Advances in diagnostic techniques, including as EEG, MRI, and functional imaging, have greatly improved the accuracy of seizure detection and localization. Although anti-seizure medications remain the cornerstone of epilepsy treatment, a sizable portion of patients still suffer drug-resistant epilepsy, necessitating alternative approaches such surgery, neurostimulation devices, and nutritional therapy. New innovations like gene therapy, precision medicine, and artificial intelligence-based monitoring systems are revolutionizing the way epilepsy is managed in the future by enabling more customized and effective treatment regimens. But problems including treatment gaps, social stigma, and limited access to healthcare services persist, particularly in low- and middle-income countries. Therefore, more research, improved healthcare facilities, and greater public awareness are essential to improving patient outcomes and the quality of life for those with epilepsy.
ACKNOWLEDGEMENT
The Department of Pharmaceutics at Matoshri College of Pharmacy in Eklahare, Nashik, is greatly appreciated by the writers for giving the resources and assistance needed to complete this review. Additionally, the authors would like to express their gratitude to faculty members and colleagues for their essential advice and support during the writing of this work. We would especially want to thank all the authors and researchers whose work has contributed to this review.
REFERENCES


Ashwini Wagh*, Prashant Malpure, Geetanjali Patil, Ujjawala Jadhav, Dhiraj Chavan, Epilepsy: A Comprehensive Review of Pathophysiology, Classification, Diagnosis, and Emerging Therapeutic Strategies, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 6618-6634. https://doi.org/10.5281/zenodo.20390125
 10.5281/zenodo.20390125
10.5281/zenodo.20390125