
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3,4 Pataldhamal Wadhwani College of Pharmacy, Yavatmal, Maharashtra, India.
5 Brix Biopharma private limited Karad, Satara, Maharashtra, India
This study focused on the formulation and evaluation of a gastro-retentive dosage form of Diclofenac Sodium with the aim of prolonging gastric residence time and achieving sustained drug release. Gastro-retentive capsules were prepared using HPMC, Acrypol 971P, and Acrypol 912G by the wet granulation method followed by capsule filling. Prior to formulation development, Preformulation studies including organoleptic evaluation, melting point determination, solubility studies, UV spectroscopic analysis, and FTIR compatibility studies were carried out. The prepared formulations were evaluated for micromeritic properties, weight variation, drug content, swelling index, mucoadhesive strength, and in vitro drug release. All formulations showed satisfactory flow properties, acceptable drug content, and sustained release characteristics. Among the different batches, formulation F6 was identified as the optimized batch based on its overall performance. It exhibited satisfactory mucoadhesive strength and a controlled drug release pattern, releasing 96.25% of the drug within 12 hours and 98.07% within 24 hours. FTIR studies confirmed the compatibility of Diclofenac Sodium with the selected excipients, while release kinetic analysis indicated that the optimized formulation followed the Higuchi model. The findings of this study suggest that the developed gastro-retentive dosage form can effectively prolong gastric retention and provide sustained drug release, making it a promising approach for improving the therapeutic performance of Diclofenac Sodium.
Oral drug delivery is the most preferred route of drug administration due to its convenience, ease of administration, and improved patient compliance. However, the bioavailability of orally administered drugs is influenced by several physiological factors, among which gastric residence time (GRT) plays a significant role.[1] Dosage forms that are designed to remain in the stomach for an extended period are known as gastro-retentive drug delivery systems (GRDDS).[2] These systems can remain in the gastric region for several hours, thereby significantly prolonging the gastric residence time of drugs.[3]
Prolonged gastric retention can improve drug bioavailability, reduce drug wastage, and enhance the solubility of drugs that are less soluble at higher pH values. GRDDS are also useful for local drug delivery in the stomach and the proximal part of the small intestine. By increasing the residence time of the dosage form in the stomach, these systems provide improved therapeutic efficacy and enhanced patient benefits. Gastro-retentive dosage forms have also been investigated for the treatment of local gastric disorders such as Helicobacter pylori infection, a major cause of peptic ulcer disease.[4,5]
Conventional oral drug delivery systems often fail to overcome the limitations imposed by the gastrointestinal tract, including incomplete drug release, reduced therapeutic effectiveness, and the need for frequent dosing. As a result, drugs may pass rapidly through the stomach, leading to reduced absorption and lower bioavailability. These limitations have encouraged the development of gastro-retentive drug delivery systems capable of retaining the dosage form in the stomach for a prolonged period.[6]
Recent studies have reported increasing interest in the development of novel drug delivery systems capable of remaining in the stomach for an extended duration while providing a predetermined drug release profile. GRDDS are particularly beneficial for drugs that are absorbed mainly in the upper gastrointestinal tract and for drugs requiring prolonged gastric retention. Various approaches have been employed for the development of GRDDS, including floating systems, bioadhesive systems, raft-forming systems, expandable systems, ion-exchange systems, superporous hydrogels, magnetic systems, and low- and high-density systems.[7]
Among these approaches, mucoadhesive drug delivery systems have gained considerable importance. These systems contain mucoadhesive polymers that adhere to the gastric mucosal surface and thereby prolong gastric residence time. The ability of these polymers to interact with the mucus layer makes them highly suitable for gastro-retentive formulations. Mucoadhesive polymers may be natural, such as sodium alginate, gelatin, and guar gum, or semi-synthetic polymers such as Hydroxypropyl Methylcellulose (HPMC), Carbopol, and sodium carboxymethyl cellulose.[12-13]
Mucoadhesive systems increase gastric residence time by enhancing the intimacy and duration of contact between the dosage form and the biological membrane. Increased adhesion to the gastric mucosa allows the dosage form to remain at the site of absorption for a longer period, thereby improving drug bioavailability.[12-13] However, gastric mucoadhesion alone may not always be sufficient to withstand the strong propulsive forces generated by gastric motility. Continuous mucus turnover and dilution of gastric contents may also limit the effectiveness of mucoadhesion as the sole mechanism for gastric retention. Nevertheless, bioadhesive drug delivery systems remain a promising approach for site-specific drug delivery and improved therapeutic performance.[12-13]
Diclofenac Sodium is a widely used non-steroidal anti-inflammatory drug (NSAID) indicated for the treatment of pain, inflammation, rheumatoid arthritis, osteoarthritis, and other inflammatory conditions.[9,10] Although the drug is therapeutically effective, conventional dosage forms may require repeated administration to maintain therapeutic drug levels. Development of a gastro-retentive dosage form may help prolong gastric residence time and provide sustained drug release, thereby improving therapeutic efficacy and patient compliance.[8,11] Therefore, the present study was undertaken to formulate and evaluate a gastro-retentive dosage form of Diclofenac Sodium using HPMC, Acrypol 971P, and Acrypol 912G as release-retarding and mucoadhesive polymers. The prepared formulations were evaluated for their physicochemical properties, swelling behaviour, mucoadhesive strength, drug content, and in vitro drug release characteristics.
MATERIALS AND METHODS
Material
Diclofenac Sodium was procure from Swastik pharmaceuticals, Acrypol971P and Acrypol912G was received from corel pharma Chem, Sodium Benzoate BP V. N. Pharma V. N. Chemical,PVP K-30 IP/BP was received from Pharma Infotech International. Microcrystalline Cellulose 101 IP /BP and Microcrystalline Cellulose 102 IP /BP was received from Archk Pharma Co. Magnesium Stearate IP/ BP received from Pharma Infotech International. Purified Talc IP/BP was received from V. N. Pharma V. N. Chemical, Colloidal Silicon Di -Oxide IP was received from V. N. Pharma V. N. Chemical.
Preformulation Studies
Physical characterization[15]
The drug sample was evaluated for physical appearance, colour, odour, and texture. The observations were recorded and compared with official specifications to confirm the identity and purity of the drug.[15]
Solubility Study
The solubility behaviour of Diclofenac Sodium was investigated in various solvents to identify a suitable dissolution medium and analytical solvent system. Excess quantity of drug was added to different solvents and shaken continuously until equilibrium was achieved. The solutions were filtered and analysed spectrophotometrically. [15,16]
Standard Calibration Curve
A standard stock solution of Diclofenac Sodium was prepared in phosphate buffer pH 6.8. Appropriate aliquots were withdrawn and diluted to obtain concentrations ranging from 5–25 μg/ml. The absorbance of each solution was measured at 276 nm using a UV-visible spectrophotometer. A calibration curve was constructed by plotting absorbance against concentration, and the regression equation was determined. [16]
Fourier Transform Infrared Spectroscopy (FTIR)
Drug-excipient compatibility studies were performed using FTIR spectroscopy. Infrared spectra of pure Diclofenac Sodium and physical mixtures containing drug and polymers were recorded over the range of 4000–400 cm?¹. The obtained spectra were analysed for any significant changes in characteristic absorption peaks that might indicate incompatibility or interaction between formulation components. [17]
Formulation of Gastro-retentive Capsules
Gastro-retentive capsules were prepared by the wet granulation method. [18] Accurately weighed quantities of Diclofenac Sodium, HPMC, Acrypol 971P, Acrypol 912G, and other excipients were passed through a suitable sieve and blended thoroughly to obtain a uniform powder mixture. The dry blend was granulated using an appropriate quantity of PVP K30 binder solution. The wet mass was passed through a sieve to obtain granules of uniform size and subsequently dried at controlled temperature until optimum moisture content was achieved. The dried granules were screened, lubricated with magnesium stearate and talc, and finally filled into hard gelatin capsules. Eight different formulations (F1–F8) were prepared by varying the concentration of release-retarding and mucoadhesive polymers in order to optimize gastric retention and sustained drug release characteristics.
Table 1 : Formulation composition for Mucoadhesive Diclofenac capsule.
|
Sr No |
Material |
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
|
1 |
Diclofenac Sodium IP |
50 |
50 |
50 |
50 |
50 |
50 |
50 |
50 |
|
2 |
HPMC |
20 |
30 |
40 |
60 |
70 |
60 |
50 |
60 |
|
3 |
Acrypol971P |
5 |
7 |
10 |
12 |
15 |
18 |
12 |
10 |
|
4 |
Acrypol912G |
5 |
8 |
10 |
13 |
15 |
17 |
13 |
10 |
|
5 |
Lactose |
51 |
56 |
46 |
28 |
23 |
28 |
44 |
36 |
|
6 |
Sodium Benzoate BP |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
|
7 |
PVP K-30 IP/BP |
6 |
6 |
6 |
6 |
6 |
6 |
6 |
6 |
|
8 |
Microcrystalline Cellulose 101 IP /BP |
60 |
50 |
55 |
45 |
40 |
40 |
50 |
55 |
|
9 |
Microcrystalline Cellulose 102 IP /BP |
50 |
50 |
50 |
45 |
40 |
35 |
45 |
45 |
|
10 |
Magnesium Stearate IP/ BP |
2 |
2 |
2 |
2 |
2 |
2 |
2 |
2 |
|
11 |
Purified Talc IP/BP |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
|
12 |
Colloidal Silicon Di -Oxide IP |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
|
13 |
Purified Water |
qs |
qs |
qs |
qs |
qs |
qs |
qs |
qs |
Evaluation of Prepared Formulations
Micromeritic Properties[14]
The prepared granules were evaluated for flow characteristics before capsule filling.
Bulk Density
Bulk density was determined by carefully pouring a known quantity of granules into a graduated cylinder and measuring the bulk volume.
Bulk Density = Weight of Powder / Bulk Volume
Tapped Density
Tapped density was determined after mechanically tapping the graduated cylinder containing the granules until constant volume was obtained.
Tapped Density = Weight of Powder / Tapped Volume
Carr’s Compressibility Index
Carr’s index was calculated to evaluate followability and compressibility characteristics.
Carr’s Index (%) = [(Tapped Density – Bulk Density) / Tapped Density] × 100
Hausner’s Ratio
Hausner’s ratio was calculated using the relationship between tapped density and bulk density.
Hausner’s Ratio = Tapped Density / Bulk Density
Angle of Repose
The angle of repose was determined using the fixed funnel method. The angle formed by the powder cone was measured and calculated using the appropriate mathematical relationship.
Weight Variation Test
Twenty capsules from each batch were selected randomly and individually weighed. The average weight was calculated and compared with pharmacopeial limits to determine uniformity of dosage units.
Swelling Index
The swelling behaviour of the prepared formulations was evaluated by placing capsules in simulated gastric fluid and measuring the increase in weight at predetermined time intervals.
Swelling Index (%) = [(Wt – Wo) / Wo] × 100
Where:
Wo = Initial weight of capsule
Wt = Weight of swollen capsule at time t
Drug Content Determination
Drug content analysis was performed to ensure uniform distribution of Diclofenac Sodium within the formulations. Capsules were opened, accurately weighed quantities were dissolved in phosphate buffer pH 6.8, filtered, and analysed spectrophotometrically at 276 nm.
Mucoadhesive Strength Study
Mucoadhesive strength was determined using freshly excised gastric mucosa. The force required to detach the formulation from the mucosal surface was recorded and expressed as mucoadhesive strength. The test was performed in triplicate and mean values were calculated.
In Vitro Drug Release Study
Dissolution test was carried out using USP type I (Basket)dissolution test apparatus and the stirring rate was 50 rpm. The 0.1N Hcl (pH 1.2) was for the first 2 h and pH 6.8 phosphate buffer was used for remaining 24 hr as dissolution medium (900 mL) and was maintained at temperature 37±0.5 °C. Samples of 5 mL were withdrawn at predetermined time intervals with syringe fitted with a pre filter and immediately replaced with 5 mL of fresh medium maintained at temperature 37±0.5 °C. The collected samples were Diluted suitably with dissolution medium, wherever necessary and were analyzed for the diclofenac sodium content spectrophotometric method at 276 nm. C
Drug Release Kinetics
To understand the mechanism of drug release, dissolution data were fitted to various mathematical models including:
The correlation coefficient (R²) obtained from each model was used to identify the release mechanism governing drug release from the gastro-retentive formulations.
RESULTS AND DISCUSSION
Preformulation Studies
Table 2: Physical characterization
|
Sr. No. |
Parameter |
Observation |
|
1 |
Colour |
white or slightly yellowish, |
|
2 |
Odour |
Odourless |
|
3 |
Taste |
Bitter |
|
4 |
Melting point |
280 ? c |
Table 3 : Solubility of Diclofenac Sodium
|
Sr. No |
Solvent |
Solubility of Diclofenac Sodium |
|
1 |
Methanol |
Soluble |
|
2 |
Ethanol |
Freely soluble |
|
3 |
Water |
Sparingly soluble |
|
4 |
Acetone |
Slightly soluble |
Table 4: Standard Calibration of diclofenac sodium
|
Sr. No. |
Volume of stock solution |
Concentration (ug/ml) |
Absorbance |
|
1. |
1 ml |
5 |
0.140 |
|
2. |
2ml |
10 |
0.287 |
|
3. |
3ml |
15 |
0.478 |
|
4. |
4ml |
20 |
0.615 |
|
5. |
5ml |
25 |
0.806 |
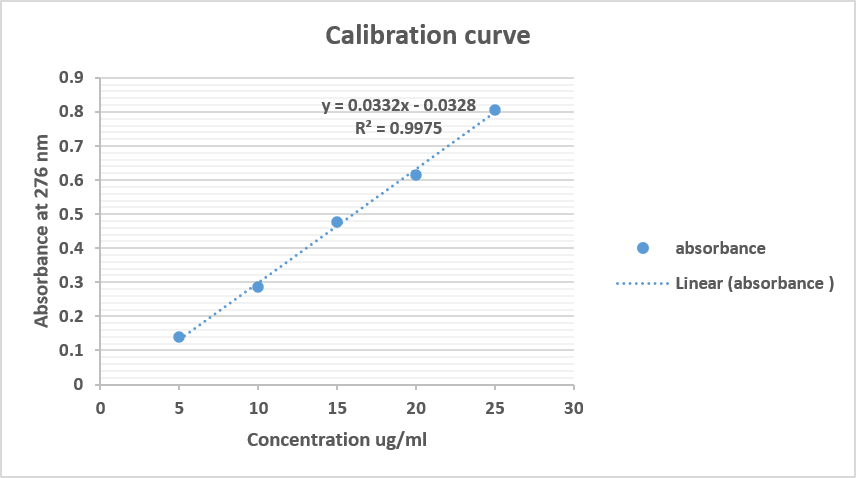
Figure 1 : Calibration curve of Diclofenac Sodium in 6.8 pH phosphate buffer.
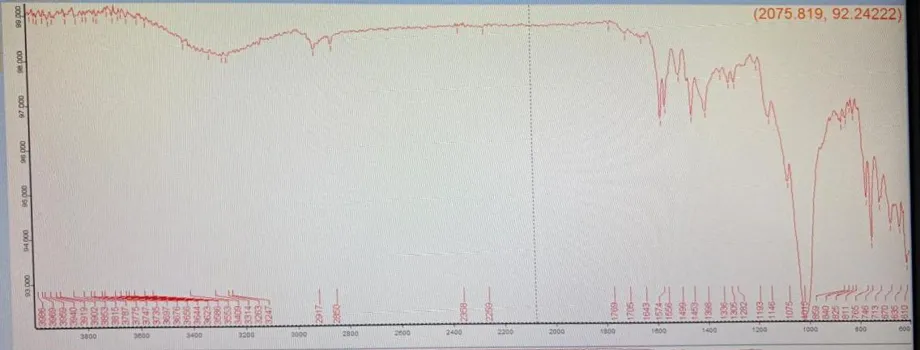
Figure 2 : FTIR of Diclofenac Sodium
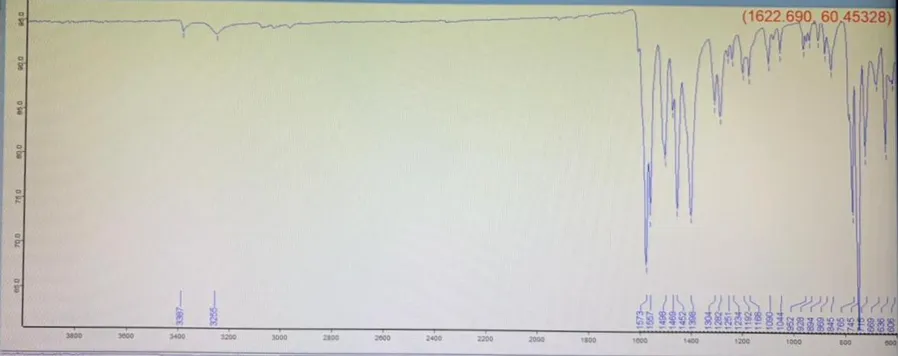
Figure 3 : FTIR of Diclofenac Sodium + Excipient
Evaluation of Prepared Formulations
Micromeritic Properties
Table 5: Evaluation Of Micromeritical properties
|
Formulation |
Bulk density (g/cm3) |
Tapped density (g/cm3) |
Carr’s index (%) |
Hausner’s ratio |
Angle of repose (θ) |
|
F1 |
0.50 ± 0.01 |
0.58 ±0.01 |
13.79 ± 0.40 |
1.16 ± 0.02 |
29 ? ±0.5 |
|
F2 |
0.49 ± 0.02 |
0.57 ± 0.01 |
14.03 ± 0.50 |
1.163±0.02 |
31.3 ? ±0.6 |
|
F3 |
0.50 ± 0.02 |
0.62 ± 0.02 |
19.35 ± 0.60 |
1.24 ±0.03 |
30.3 ? ±0.5 |
|
F4 |
0.48 ± 0.01 |
0.58 ± 0.01 |
17.24 ± 50 |
1.21± 0.02 |
32.2 ? ±0.6 |
|
F5 |
0.50 ± 0.01 |
0.59 ±0.01 |
15.25 ± 50 |
1.18 ± 0.02 |
31.9 ? ± 0.5 |
|
F6 |
0.47 ± 0.02 |
0.58 ± 0.01 |
18.96 ± 60 |
1.23 ± 0.02 |
31.3 ? ± 0.6 |
|
F7 |
0.48 ± 0.02 |
0.59 ± 0.01 |
18.64 ± 0.50 |
1.229±0.02 |
32.6 ?± 0.6 |
|
F8 |
0.46 ± 0.01 |
0.51± 0.01 |
9.80 ± 0.40 |
1.10 ± 0.02 |
31.7 ? ± 0.5 |
All batches showed good flow properties, with angle of repose values below 33°, along with acceptable Carr’s Index and Hausner’s ratio. This indicates satisfactory granule formation and followability, making the granules suitable for further processing such as capsules filling.
Weight variation, lock length and Drug content.
Table 6 : Weight variation, lock length and Drug content
|
Formulation code |
Average Weight (mg) |
Lock length (mm) |
Drug content (%) |
|
F1 |
329.8±1.2 |
180.00 ± 0.2 |
97.5±0.7 |
|
F2 |
330.5±1.1 |
179.50 ± 0.3 |
97.8±0.6 |
|
F3 |
328.9±1.3 |
180.00 ± 0.2 |
96.6±0.8 |
|
F4 |
331.2±1.0 |
180.00 ± 0.2 |
95.9±0.8 |
|
F5 |
332.0±1.2 |
179.56 ± 0.3 |
95.8±0.7 |
|
F6 |
330.8±1.0 |
180.00 ± 0.2 |
97.3±0.9 |
|
F7 |
329.5±1.3 |
180.1 ± 0.2 |
96.8±0.7 |
|
F8 |
329.0±1.2 |
179.8 ± 0.3 |
96.6±0.6 |
All formulations (F1–F8) showed uniform average weight, lock length, and drug content, indicating successful capsule filling and good content uniformity.
Average Weight: 328.9–332.0 mg, Lock Length: 179.50–180.10 mm, Drug Content: 95.8–97.8% (within acceptable limits).
Swelling index
Table 7 : Swelling index
|
Time (Min) |
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
|
1 |
18.22±0.6 |
20.61±0.7 |
22.20±0.7 |
25.63±0.6 |
19.65±0.8 |
21.2±0.7 |
23.32±0.6 |
20.31±0.7 |
|
2 |
25.30±0.8 |
28.33±0.9 |
32.91±0.1 |
34.53±0.9 |
16.32±1.1 |
30.60±0.9 |
34.40±0.8 |
28.16±0.9 |
|
4 |
30.52±1.0 |
35.74±1.1 |
40.24±1.2 |
45.19±1.0 |
32.13±1.1 |
38.32±0.1 |
42.21±1.0 |
35.27±1.1 |
The swelling index increased with time for all formulations, indicating effective hydration of the mucoadhesive polymers. The optimized formulation F6 showed good swelling behavior in 4 hour, which may contribute to improved mucoadhesion and sustained drug release.
Mucoadhesive strength
Table 8: Evaluation of mucoadhesive strength of diclofenac sodium capsule .
|
Formulation code |
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
F9 |
|
Mucoadhesive strength |
8.0±1.6 |
9±1.5 |
8.9±1.7 |
9±1.8 |
10±1.7 |
12±1.8 |
9.7±1.5 |
8.5±1.6 |
10±1.6 |
The mucoadhesive strength of all formulations ranged from 8.0 ± 1.6 g to 12.0 ± 1.8 g, indicating effective mucoadhesive properties. The optimized formulation F6 showed the highest mucoadhesive strength (12.0 ± 1.8 g), suggesting stronger adhesion to the mucosal surface and improved gastric retention.
Cumulative % drug release of Diclofenac sodium Mucoadhesive capsule.
Table 9 : cumulative % drug release of diclofenac sodium Mucoadhesive capsule
|
Time (hrs.) |
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
|
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
2 |
30.32±1.2 |
27.80±1.3 |
24.01±1.4 |
25.47±1.3 |
22.68±1.5 |
20.23±1.6 |
25.2±1.3 |
26.2±1.2 |
|
4 |
50.14±1.5 |
49.97±1.4 |
45.79±1.6 |
55.88±1.3 |
49.99±1.4 |
40.12±1.7 |
48.79±1.5 |
49.45±1.4 |
|
6 |
70.45±1.8 |
60.68±1.7 |
57.89±1.6 |
65.47±1.5 |
62.87±1.6 |
60.56±1.7 |
66.85±1.5 |
67.21±1.6 |
|
8 |
85.04±1.6 |
83.36±1.5 |
80.70±1.7 |
78.04±1.8 |
77.98±1.7 |
76.60±1.8 |
86.99±1.5 |
83.41±1.6 |
|
10 |
92.36±1.3 |
89.65±1.4 |
83.21±1.6 |
88.1±1.5 |
93.07±1.3 |
86.45±1.5 |
88.63±1.4 |
85.89±1.5 |
|
12 |
90.27±1.3 |
90.98±1.3 |
87.43±1.5 |
93.21±1.2 |
95.83±1.1 |
96.25±1.1 |
92.21±1.3 |
86.91±1.5 |
|
24 |
95.42±1.2 |
93.59±1.3 |
93.58±1.3 |
96.6±1.1 |
97.83±1.0 |
98.07±1.0 |
93.72±1.2 |
91.36±1.4 |
The in-vitro drug release study indicated that all formulations were able to sustain the release of Diclofenac Sodium over a period of 24 h. A gradual increase in drug release was observed with increasing dissolution time. Among all the formulations, F6 showed the highest drug release (98.07 ± 1.0%) at 24 h, followed by F5 (97.83 ± 1.0%) and F4 (96.60 ± 1.1%). Based on the dissolution results, F6 was considered the optimized formulation as it provided the most effective and prolonged drug release profile throughout the study period.
Kinetics of drug Release:
Table 10: Drug release kinetics of formulations F1 to F8.
|
Formulation code |
First order plot (R2) |
Zero order plot (R2) |
Higuchi plots (R2) |
Hixon-Crowel cube root plot (R2) |
Korsmeyer-peppas plots |
Best fit model |
|
|
N |
R2 |
||||||
|
F1 |
0.9284 |
0.8919 |
0.9505 |
0.9320 |
0.529 |
0.9245 |
Higuchi plot |
|
F2 |
0.9628 |
0.9282 |
0.9662 |
0.9608 |
0.599 |
0.9430 |
Higuchi plot |
|
F3 |
0.9646 |
0.9240 |
0.9649 |
0.9580 |
0.627 |
0.9415 |
Higuchi plot |
|
F4 |
0.9855 |
0.9240 |
0.9724 |
0.9914 |
0.487 |
0.9916 |
Korsmeyer-peppas plots |
|
F5 |
0.9562 |
95256 |
0.9864 |
0.9834 |
0.629 |
0.9855 |
Higuchi plot |
|
F6 |
0.9322 |
0.9744 |
0.9959 |
0.9873 |
0.795 |
0.9825 |
Higuchi plots |
|
F7 |
0.9397 |
0.8862 |
0.9450 |
0.9302 |
0.585 |
0.9136 |
Higuchi plots |
|
F8 |
0.9422 |
0.8784 |
0.9425 |
0.9282 |
0.532 |
0.9146 |
Higuchi plots |
For formulations F1 to F3,F5,F6,F7,F8 the Higuchi Mode showed the best fit with the highest R² values. Formulation F4 showed the best fit with the Korsmeyer peppas Model (R² = 0.9916).In most formulations, drug release followed diffusion-controlled mechanisms indicated by Higuchi and Korsmeyer-Peppas models.
CONCLUSION
The present study successfully developed and evaluated mucoadhesive gastroretentive capsules of Diclofenac Sodium for sustained drug delivery. FTIR studies confirmed the compatibility of Diclofenac Sodium with the selected excipients, while all formulations exhibited satisfactory micromeritic properties and acceptable capsule characteristics. Among the prepared formulations, batch F6 demonstrated the most promising performance, showing drug content of 97.3 ± 0.9%, mucoadhesive strength of 12 ± 1.8 g, and cumulative drug release of 96.25 ± 1.1% at 12 h and 98.07 ± 1.0% at 24 h. Drug release from F6 followed the Higuchi model (R² = 0.9959) with a release exponent (n = 0.795), indicating a non-Fickian diffusion mechanism involving both diffusion and polymer swelling. The findings suggest that the developed mucoadhesive gastroretentive capsule system is capable of prolonging gastric residence and providing controlled drug release, making formulation F6 a promising candidate for the effective oral delivery of Diclofenac Sodium.
REFERENCES

Rutika Bawankule, Akshada Fursule, Aasawari Rajgure, Shilpa Gawande, Mahesh Rao, Formulation and Evaluation of a Gastro-Retentive Dosage Form to Prolong Gastric Retention, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6558-6567. https://doi.org/10.5281/zenodo.20909343
 10.5281/zenodo.20909343
10.5281/zenodo.20909343