We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Doctor Of Pharmacy MET’s Institute Of Pharmacy Adgaon, Nashik.
Background:Hysterectomy is the surgical removal of the uterus which is one of the most frequently performed gynecological procedures worldwide. While it can provide relief from various pathological conditions such as fibroids, cancers, and abnormal uterine bleeding, it can also significantly affect a woman’s physical, psychological, emotional, and social well-being. This study aims to evaluate these multiple impacts using both qualitative and quantitative approaches.Objective:To assess the comprehensive impact of hysterectomy on women's lives, including physical recovery, emotional and psychological outcomes, social experiences, and quality of life.Methodology:An Observational and Retrospective study was conducted in the Nashik district over six months. A total of 150 women aged between 21 - 80 years who had undergone elective hysterectomy at least six months prior were included. Quantitative data were collected using structured questionnaires and analyzed with MS Excel and Qualitative data were obtained from in-depth interviews with 60 participants from two age groups formed and analyzed based on various factors and the responses acquired from the patient through the questionnaires.Results:Quantitative analysis revealed that women aged between 41–80 years had a significantly higher incidence of hysterectomy due to conditions such as ovarian and cervix cancer (p < 0.05) i.e. 0.02. The most common age group affected was 41–50 years. Most patients reported postoperative improvement in physical symptoms such as pain and mobility.Qualitative analysis showed that younger women (21–40 years) faced greater emotional distress, grief over loss of fertility, and marital difficulties. Social stigma and cultural expectations also played a major role in shaping women’s postoperative experiences. Older women (41–80 years), while physically benefitting from the surgery, still experienced emotional challenges and were often subject to societal judgments and negative criticism which affected them mentally and emotionally .Conclusion Hysterectomy significantly impacts women's lives across physical, emotional, social, and marital domains. The extent and nature of the impact vary with age, with younger women facing more emotional and social challenges. Comprehensive pre-operative counseling, postoperative support, and long-term follow-up are essential to address these issues holistically.
A hysterectomy is a surgical procedure involving partial or complete removal of the uterus (womb). After hysterectomy, menstruation stops and pregnancy is no longer possible.
Types
Purpose/Indications
Hysterectomy is performed when other treatments fail or are unsuitable. Common indications include:
Preoperative Preparation
Surgical Approaches
1. Vaginal Hysterectomy
2. Abdominal Hysterectomy
3. Laparoscopic Hysterectomy
Contraindications
Relative Contraindications to Vaginal Hysterectomy
General Contraindication
Complications
Intraoperative Complications
Postoperative Complications
Anatomy Involved
Important structures related to hysterectomy:
Clinical Significance
Conclusion: Hysterectomy is one of the most common gynecological surgeries used to treat benign and malignant uterine conditions. The choice of surgical route depends on the patient's condition, uterine size, surgeon expertise, available resources, and patient preference.
There is a crucial need to investigate the primary indications and causes of hysterectomy. This includes identifying the signs and symptoms leading to the surgery, such as abnormal uterine bleeding, fibroids, endometriosis, pelvic pain, and cancer. Understanding these underlying causes can help in early diagnosis and possibly avoiding unnecessary surgeries.
Postoperative complications can significantly affect patient outcomes. A study is needed to track and analyze complications such as infections, chronic pain, hemorrhage, or injury to surrounding organs. Monitoring these outcomes will aid in developing better postoperative care protocols to reduce morbidity and enhance recovery.
Hysterectomy not only affects physical health but also has emotional, psychological, and social implications. Assessing patient satisfaction and changes in quality of life post-surgery is important to evaluate the success of the treatment from the patient’s perspective. This includes understanding their experience, relief from symptoms, and return to daily activities.
Demographic variables such as age, weight, socioeconomic status, and comorbidities influence the decision and outcomes of hysterectomy. It is essential to study how these factors contribute to the rates of hysterectomy and related complications, in order to develop targeted health interventions and ensure equitable care
The long-term effects of hysterectomy on health, including hormonal changes, sexual function, and psychological well-being, require detailed evaluation. Regular follow-up studies help in identifying delayed complications and provide an opportunity for timely intervention, ensuring sustained health and well-being.
The primary objective of this study is to comprehensively assess the impact of hysterectomy on women's lives by employing both qualitative and quantitative analysis of comparative study. The study aims to explore and evaluate the physical, psychological, emotional, and social outcomes experienced by women
Plan of work
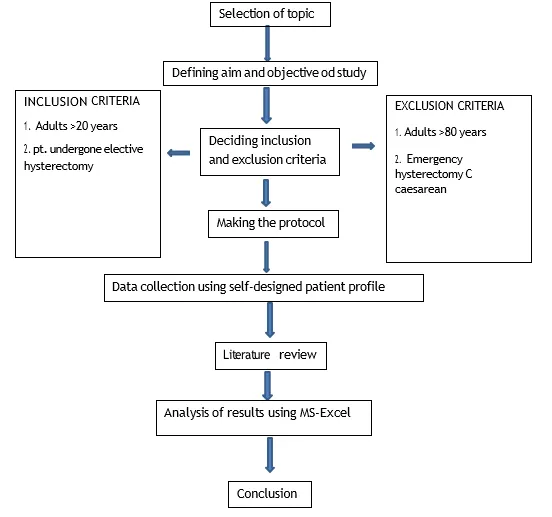
A mixed-methods cross-sectional study combining both quantitative and qualitative approaches was conducted to assess the impact of hysterectomy on women’s physical, psychological, social, and sexual health.
The study was carried out in the Gynecology Outpatient Department and follow-up clinics in Nashik district including urban and rural area , over a period of 6 months.
Women aged between 21 and 80 years who had undergone hysterectomy (total or subtotal, with or without oophorectomy) at least 6 months prior to the study were included.
A total of 150 women were included in the study using convenience sampling for quantitative analysis. For qualitative analysis, in-depth interviews were conducted on a purposive sub-sample of 20 participants, ensuring representation of different age groups and socio-economic backgrounds.
Emergency and elective hysterectomy
Participants were approached during their follow-up visits or contacted telephonically. Informed consent was obtained. The quantitative questionnaire was administered face-to-face or via phone. Qualitative interviews were conducted in a private setting.
written informed consent was taken from all participants. Confidentiality and anonymity were strictly maintained.
RESULT AND DISCUSSION
The study was performed by taking sample size of approximately 200 patients out of which 150 patients’ information was collected using the patient profile form to assess the impact of hysterectomy in the patients.
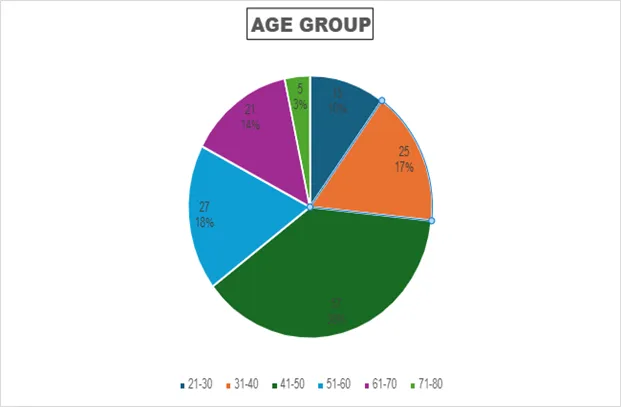
TABLE NO. 1.2 DISTRIBUTION OF AGE
|
AGE GROUP |
NO.OF PATIENTS |
PERCENTAGE |
|
21-30 |
15 |
10% |
|
31-40 |
25 |
16.66% |
|
41-50 |
57 |
38% |
|
51-60 |
27 |
18% |
|
61-70 |
21 |
14% |
|
71-80 |
5 |
3.33% |
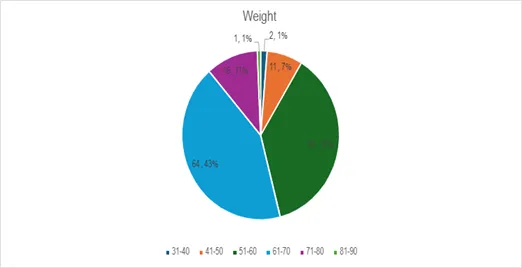
FIGURE 2.1 NO. OF PATIENTS ACCORDING TO WEIGHT GROUP
TABLE NO.2.2 DISTRIBUTION OF WEIGHT
|
NO. OF PATIENTS |
PERCENTAGE |
|
|
31-40 |
2 |
1.33% |
|
41-50 |
11 |
7.33% |
|
51-60 |
56 |
37.33% |
|
61-70 |
64 |
42.66% |
|
71-80 |
16 |
10.66% |
|
81-90 |
1 |
0.66% |
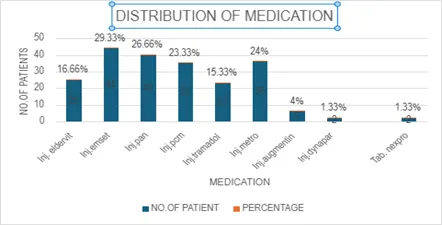
FIGURE 3.1 DISTRIBUTION OF MEDICATION
TABLE NO. 3.2 DISTRIBUTION OF MEDICATION
|
MEDICATION |
NO. OF PATIENT |
PERCENTAGE |
|
Inj. Eldervit |
25 |
16.66% |
|
Inj.emset |
44 |
29.33% |
|
Inj.pan |
40 |
26.66% |
|
Inj.pcm |
35 |
23.33% |
|
Inj.tramadol |
23 |
15.33% |
|
Inj.metro |
36 |
24% |
|
Inj.augmentin |
6 |
4% |
|
Inj.dynapar |
2 |
1.33% |
|
Tab. Nexpro |
2 |
1.33% |
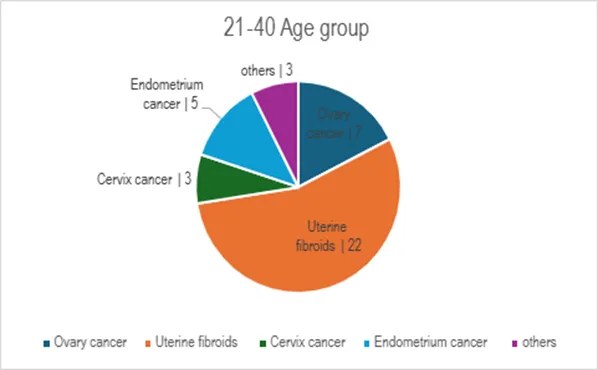
TABLE NO. 4.2 DISTRIBUTION OF DIAGNOSIS IN AGE GROUP 21-40
|
DIAGNOSIS |
NO.OF PATIENTS |
|
Ovary cancer |
7 |
|
Uterine fibroids |
22 |
|
Cervix cancer |
3 |
|
Endometrium cancer |
5 |
|
Others |
3 |
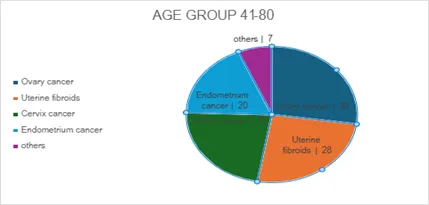
TABLE NO. 5.2 DISTRIBUTION OF DIAGNOSIS IN AGE GROUP 41-80
|
DIAGNOSIS |
NO.OF PATIENTS |
|
Ovary cancer |
30 |
|
Uterine fibroids |
28 |
|
Cervix cancer |
25 |
|
Endometrium cancer |
20 |
|
Others |
7 |
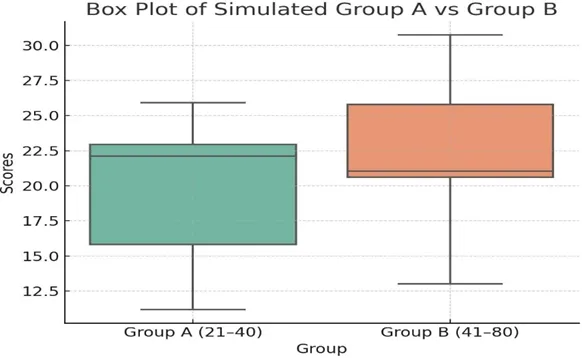
TABLE NO. 6.1 T-TEST ANALYSIS.
|
DIAGNOSIS |
GROUP A(21-40) |
GROUP B(41-80) |
|
Ovary cancer |
7 |
30 |
|
Uterine fibroid |
22 |
28 |
|
Cervix cancer |
3 |
25 |
|
Endometrium cancer |
5 |
20 |
|
Others |
3 |
7 |
|
|
|||||
|
Tests |
group A (21- 40) |
group B (41- 80) |
|
||
|
Mean |
8 |
22 |
|
||
|
Variance |
64 |
84.5 |
|
||
|
Observations |
5 |
5 |
|
||
|
Pearson Correlation |
0.48273636 |
0.48273636 |
|
||
|
Hypothesized Mean Difference |
0 |
0 |
|
||
|
Df |
4 |
4 |
|
||
|
t Stat |
-3.556003556 |
-3.556003556 |
|
||
|
P(T<=t) one-tail |
0.011835354 |
0.011835354 |
|
||
|
t Critical one-tail |
2.131846786 |
2.131846786 |
|||
|
P(T<=t) two-tail |
0.023670708 |
0.023670708 |
|||
|
t Critical two-tail |
2.776445105 |
2.776445105 |
|||
(08) and Group B (22).
|
THEME |
CODES |
QUOTES |
|
||||
|
|
|
AGE 21-40 |
AGE GROUP 41-80 |
|
|||
|
Emotional and psychological impact |
Loss of identity, Emotional emptiness. |
-15 patients said “I try to smile but don’t feel anything. |
-38 patients said, “I get irritated with |
|
|||
|
|
|
-Not being able to be a mother makes my life meaningless.” |
very small things”. - “Moods swings” |
||||
|
Social and cultural impact |
Stigma from relatives to stay quiet |
-10 patients said, “My family said you should be ashamed yourself”. - “If I talk about if people criticized me “ |
-16 patients said, “Peoples started criticizing because I have only daughters” |
||||
|
Reproductive failure |
Loss of fertility |
-20 patients said, “It hurts every time I hear someone is pregnant.” |
-10 patients said “Even if I’m older I still feel the pain and grief of losing fertility” |
||||
|
Physical health |
Pain relief Improved mobility Better sleep |
-18 patients said, “The pain is unpredictable and exhausting”. “Somedays I can’t get out of bed”. |
-40 patients said, “When i have a good day without pain I feel blessed. - “Managing pain has become my full-time job”. |
||||
|
Marital life |
Relationship with partner changes. |
-3 patients said, “We argue more since I got sick”. |
40 patients “No impact on marital life as such “. |
||||
|
|
|
- “Some time I feel like burden on him.” |
|
Women aged 41–80 underwent significantly more hysterectomies than those aged 21–40 (p = 0.02), with uterine fibroids and ovarian cancer being the most common indications.
Younger women experienced profound emotional distress and fertility grief, while older women reported physical relief from pain rarely and improved daily functioning post-hysterectomy but still complaints of emotional distress due to the social stigma .
This study shows that the patients undergoing Hysterectomy mostly shows negative impact on both the age groups A and B .
The above study is an Observational and Retrospective study which was conducted on the patients of Gynecology Department in a hospital situated in rural area who have undergone Hysterectomy. The patients were selected in the time duration of 6 months 2024-2025. Total population included was 150 patients.
Further the analysis done as follows:
Quantitative Analysis Discussion
CONCLUSION
This mixed-methods study reveals that hysterectomy significantly impacts women’s lives across multiple dimensions:
LIMITATIONS AND FUTURE SCOPE
Including the perspectives of husbands or family members may uncover deeper social and relational dynamics and improve family counselling strategies.
REFERENCES


Komal Vighne, Sakshi Bairagi, Ritamani Sahu, Anushka Shinde, Impact Of Hysterectomy on Womens Lives: A Qualitative and Quantitative Analysis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 7616-7630, https://doi.org/10.5281/zenodo.21065909
 10.5281/zenodo.21065909
10.5281/zenodo.21065909