
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacology,Acharya & BM Reddy College of Pharmacy,Acharya Dr. Sarvepalli Radhakrishna Road,Achit Nagar (Post), Soldevanahalli,Bengaluru, India.
Characterized by an imbalance of localized and systemic bone loss from long-term inflammation secondary to RA treatments, osteoporosis is one of the major comorbidities of RA. This review examines the puzzling role of inflammatory cytokines like TNF-? and IL-6 also bone metabolism concerning their roles in osteoclastogenesis and bone resorption. It also addresses the possible effects in younger and male RA patients and their hormonal effects on postmenopausal women. Autoimmune-related bone loss and glucocorticoid-induced osteoporosis (GIOP) are the risk factors that focus on the diagnosis and management protocols that warrant detailed diagnosis and treatment strategies.While DXA represents the microporosity-a direct measure of bone mass-density structure, it is a big deal; new technologies, such as radiofrequency echographic multispectrometry (REMS) and quantitative computed tomography (QCT), are then needed since their diagnostic sensitivity is limited. A diagnostic marker should improve individual risk stratification, and provide an early alert. The management of RA involves the utilization of biologics and DMARDs to arrest bone loss. The combination of this therapeutic strategy with contemporary anti-osteoporotic drugs like denosumab and bisphosphonates creates a previously ignored approach to treatment.With prevention still being important, the emphasis lies on special dietary and lifestyle regimes that include sufficient calcium and vitamin D supplementation, together with physical activity and weight-bearing ones.
Osteoporosis is a disorder of the skeletal system that causes bone structure to weaken and bone density to decrease. This results in greater fragility and an increased risk of fractures. This condition's weakened bone structure is reflected in the term porous bone [1]. As they happen with little to no trauma fragility fractures are a major sign of osteoporosis [2]. Historically, “osteoporosis” comes from 19th-century French & German medical language, which defined the condition as the appearance of aged bone tissue having pores [3]. The incidence of osteoporosis is diverse around the world, affecting 9% to 38% of women and 1% to 8% of men [2]. Primary osteoporosis tends to occur in postmenopausal women and older patients, whereas secondary osteoporosis occurs due to some specific medical conditions, such as thyrotoxicosis or hyperadrenocorticism [4].
Osteoporosis diagnosis is challenging. Fracture-based definitions miss potential candidates for treatment, whereas the classic 1994 WHO definition only of BMD has a T-score of ≤–2.5 or 2.5 standard deviations below the young adult female average and does not consider other risks [5]. Low BMD or osteoporosis is defined as an increased risk for fractures, and such risk varies with age and gender. A primary care physician can make a clinical diagnosis for a patient aged 50 years or older who has experienced a low-trauma fracture (for example, a hip, vertebral, humeral, or pelvic fracture) after age 40 or has an absolute risk of 20 percent for a major fracture in the next 10 years, according to instruments like Fracture Risk Assessment Tool (FRAX) [6]. Biophosphates like alendronate, risedronate, and zoledronic acid have been shown through RCTs to be effective in reducing the risk of fractures in elderly postmenopausal women with osteoporosis. However, treatment with bisphosphonates is not devoid of adverse effects. Common complaints of patients who were placed on oral bisphosphonates include gastrointestinally mediated disorders including acid reflux and irritation of the esophagus. Patients suffering from these side effects find that their quality of life becomes affected [7].
Osteoporosis cannot be diagnosed using BMD measurements taken from sites other than the lumbar spine, total hip, femoral neck, or 33% radius, nor can it be estimated by methods other than DXA, except for T-scores of the total hip and femoral neck derived from 2D projections of QCT data. Diagnosis relies on proper collection, analysis, interpretation, and reporting of data, as well as proper maintenance and calibration of DXA devices, all of which yield reliable results for use in clinical decisions. Patients with persistent fragility fractures can be diagnosed with osteoporosis by physical examination in addition to BMD results, provided that the possible causes of skeletal fragility, such as multiple myeloma or osteomalacia, have been excluded [8].
Rheumatoid arthritis (RA) is a chronic inflammatory condition that leads to joint destruction, affecting 0.5-1% of the global population and potentially causing significant disability and reduced quality of life. It was observed the disease manifestations occur two to three times more frequently in women than in men, regardless of age. However, it was noted that the onset typically happen most often between the fourth and sixth decades of life [9]. RA is characterized by symmetrical inflammation of multiple small joints, which causes considerable damage to cartilage and bone. Persistent synovitis and progressive joint destruction are the hallmarks of the disease [10].
Due to several reasons including the disease’s severity and duration, patients suffering from RA have experienced greater bone mass loss compared to the general population as well as the effects of severe physical disability and treatments containing large amounts of corticosteroids. Such individuals with RA suffer almost double the chances of osteoporotic fractures. The bone erosions occurring in RA occur from enhanced osteoclastic activity, associated with inflammation [11]. In RA, bone erosions predict subsequent bone loss and decrease in bone mass. It is intriguing that peri-articular bone loss, which defines RA, occurs prior to the development of symptoms of synovitis and is both a feature of systemic loss and local joint damage [12]. This article aims at reviewing the pathophysiology of osteoporosis it was mentioned that in patients with rheumatoid arthritis, there are various risk factors that contribute to an increased risk of osteoporosis, diagnose and follow problems specific to RA-associated osteoporosis, and review pharmacological and non-pharmacological current options for treating osteoporosis.
2. Pathophysiology of Osteoporosis in RA
In bone tissue there are four cell types; osteoblasts and osteocytes, for bone formation and maintenance; osteoclasts that aid in bone resorption; and bone lining cells that contribute to overall bone health by responding to signals from RANKL receptor activators and MCSF, are important for the continuous processes of bone formation and resorption, which are necessary to keep bones healthy (figure no:1). When bone resorption takes place with osteoclasts, at work in the body osteoblasts step to create bone by forming a matrix to make up the resorbed bone [13]. Osteocytes are thought to regulate the bone cells and to keep the bone tissue healthy and firm [14].
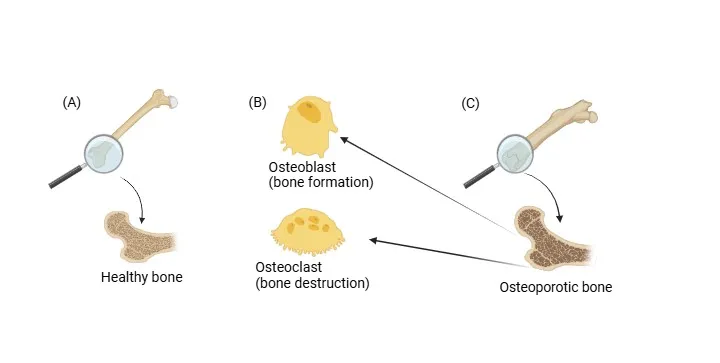
Figure 1: The diagram illustrates bone (labelled as C) depicting osteoblasts and osteoclasts (labelled as B) the cell types engaged in the bone remodelling process alongside a representation of healthy bone (labelled as A).
This figure was created using the site (https://app.bio render.com/).
Osteoporosis is a severe disease associated with rheumatoid arthritis (RA) and characterized by local and systemic bone loss measurements. To produce effective treatments, it is important to understand the pathophysiological factors promoting osteoporosis in RA. Traditional risk factors for osteoporosis continue to be useful clues in predicting osteoporosis in persons afflicted with RA. Generally speaking, very few studies cited report a greater frequency of spinal or femoral osteoporosis in women than in men [15], older age, history of low trauma fractures, a lower body mass index, longer periods of corticosteroid therapy, high Larsen score, and higher HAQ score [16,17,18]. Compared with postmenopausal controls, RA women have greater bone loss; hormone replacement therapy suppresses bone resorption in postmenopausal RA women regardless of glucocorticoid therapy [19].
The risk of developing osteoporosis is higher in rheumatoid arthritis patients than in the general population [20,21]. The prevalence of osteoporosis among RA patients has been described from 7% to 26% at the hip and from 19% to 32% at the spine [20,22,23]. The inflammatory cytokines can cause overexpression of RANKL in rheumatoid arthritis patients and activate osteoclastogenesis [24]. A reduced blood concentration level of OPG and elevated concentrations of the RANKL were found in osteoporosis and RA [21].
2.1 Role of cytokine (IL-6, TNF-α) on osteoclast activation
IL-6 is a major important immune system cytokine and it’s released chiefly by monocytes, neutrophils, T cells and macrophages [25]. Both membrane-bound and soluble IL-6 receptos (sIL-6R) drive its biological activity [26]. The example of IL-6 and IL-11 being pro-inflammatory cytokines is seen with their altering of osteoclast differentiation and skeletal homeostasis. The combined result of binding soluble IL-6 to membrane-bound receptors of pre-osteoclasts is increased levels of bone resorption, which leads to the promotion of osteoclastogenesis [27]. And bone remodeling is also affected by IL-6, principally osteoclastogenesis. In osteoblasts, IL-6 signals through the JAK/STAT3 signaling system to release PGE2, RANK, IL-1 and PTHrP for pro-osteoclastic effects [28,29,30]. PGE2 and PTHrP, which activate osteoblast RANKL production and IL-6 [31,32]. The signalling networks for PTH and 1,25(OH)2D3 also depend on sIL-6R for their activity [33]. The circulating sIL-6R results from cleavage or alternative splicing of IL-6R, which can free the receptor from cells existing in trace amount in the circulation, such as CD4T-primarily [34]. To initiate the signaling pathways via IL-6, IL-6 must be able to associate with the sIL-6R that exists in the circulating pool before associating with the osteoblastic membrane (figure no:2). Greater amounts of IL-6 and sIL-6 are hence an indication of the osteolytic diseases, for example, rheumatoid arthritis [35].
Besides the catabolic activity of bone, TNF-α is important regarding intracellular regulation of bone metabolism and inflammatory bone diseases [36]. It is important in tissue regeneration and modulation of the immune system for response against infections. To be more specific, tumor necrosis factor-α (TNF-α) induces bone loss by the way of decreased osteoclast activation [37, 38]. To be precise, if an excessive amount of TNF-α releases into the chronic inflamed tissue, it may lead to the loss of the bone and a decline in bone density due to the fact that it can destruct the osteoblast's ability of bone formation. In autoimmune diseases or chronic inflammatory conditions, TNF-α in high quantity is likely to have detrimental effects on bone health maintenance and making the risk of osteoporotic [39]. The effect of the cytokine is to specifically induce uncoupling of M-CSF from RANKL together with nontargeted on TRAP+ OC precursors. The additional TNF-α regulation of RANK in the OC precursors remains to be discovered. Besides being activated by quite a number of the molecules in the osteoclastogenic pathway, also I've RANKL. TNF-α can be partly responsible for the speeding up of RANKL-induced osteoclast differentiation through the processes of TRAF2/5 and MAPKs in TNFR1-mediated signal which activates NF-κB and AP-1 [40-43]. Autophagosomes degrade TRAF3 during RANKL activation, enhancing TNF-induced osteoclanomics in TAF6/ osteoclast precursors. The evidence suggests that RANKL can function as an independent signal for osteoclastogenesis, rather than being dependent on TRAF6 [44]. TNF- promotes osteoclastogenesis by stimulating stromal cells, osteoblasts, and T cells to generate M-CSF and RANKL [45]. RA patients often benefit from golimumab, certolizumag, adalimUMaB, and infliximac, as synovial cells control JNK signaling and regulate NF-B by using TNF-4 [46, 47]. These results highlight the importance of TNF- in osteoclastogenesis, as both direct and indirect mechanisms are involved.
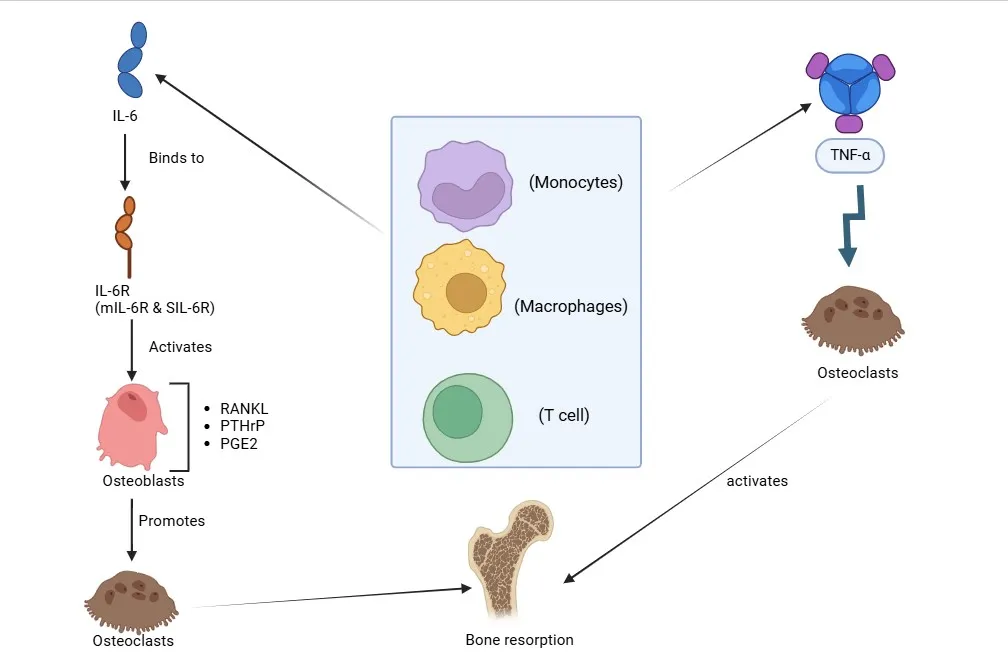
Figure 2: The figure illustrates the role of IL-6 and TNF-α Pathways in Osteoclastogenesis and Bone Resorption. It depicts how IL-6, through its receptor (IL-6R), and TNF-α contributes to osteoclastogenesis.
2.2 Hormonal Influence in Postmenopausal Women.
Many changes in hormones, of which a strong drop in the level of estrogen, are involved particularly in the transition to menopause. This deficiency of hormones has far-reaching effects on the skeletal system among other body systems. It is also responsible for low bone density found in women after menopause, along with a high stake of developing osteoporosis.
Hypogonadism is a hormonal imbalance between the hormones produced by the ovaries, mostly estrogen, in which estrogen production drops sharply after menopause. The simultaneous increase of FSH and LH levels following the reduction of estrogen, creates a disturbance in the normal hormonal process, regulating bone metabolism and affecting general health [48,49]. Due to its effect on different bone cells, estrogen is vital for maintaining bone density. Estrogen stimulates osteoblast activity and differentiation, which are essential for bone formation. It also has a tendency to decrease osteoblast apoptosis, resulting in an enhanced potential for new bone formation [50,51]. The role of estrogen in inducing the apoptosis of osteoclasts and inhibition of osteoclastogenesis was also noted. This further slows down the catabolism of bone or bone resorption [48,50].
Three kinds of bone destruction are generalized osteoporosis, periarticular osteoporosis, and bone erosions, indicating rheumatoid arthritis. Osteoporosis is noted to occur in almost half of postmenopausal RA patients, with various studies showing lower BMD and accompanied by an increase in the risk of fracture [52,53]. Inflammation and menopause are known to cause bone loss through a lack of estrogen [54]. pro-inflammatory cytokines like TNF-α and IL-1, produced by macrophages, stimulate osteoclast activity to assist in bone healing. Additionally, it is noted that terminally differentiated osteoclasts, originating from the monocyte/macrophage lineage, are responsible for resorbing the bone matrix The inhibition of RANKL binding to Yin-1 hinders the differentiation of precursor cells into mature osteoclasts and prevents further differentiation from NF-B signaling [55]. In rheumatoid arthritis, Th 17 cells release pro-inflammatory cytokines and activate osteoclast precursors by activating their IL-17 prodction and release RANKL expression. RANKL might therefore be expressed on the membrane of Th17 cells to promote osteoclastogenesis [54-56] subsequently. Other factors in the same vein are steroid treatment, lower body mass, and decreased physical exertion, which amplify the incidence of fractures and diminished bone mineral density among RA patients [53].
So, over the last several years, some authors suggested that estrogen replacement could prevent osteoporosis and the degeneration of joints in menopausal RA patients [53,57]. In animal model experiments, the administration of physiological doses of estrogens has consistently been shown to be protective against osteoporosis and arthritis [57]. Hormone-replacement therapy was beneficial for raising BMD in postmenopausal RA [58,59]. However, recent restrictions on the use of HRT in general for women have come in response to the adverse effects seen with prolonged treatments. There were two major trials that were done among healthy postmenopausal women, and these showed a higher incidence of breast cancer, CHD, stroke, and pulmonary embolism among HRT-treated candidates [60,61]. Systemic osteoporosis in RA patients should no longer be treated with HRT due to its elevated cardiovascular risks specifically attributed to the condition itself [62].
Women with osteoporosis (Rha) should also consider alternative therapies as anti-TNF drugs have been shown to reduce inflammation and improve bone density. The treatment with a TNF blocker boosts bone metabolism by increasing plasma markers of bone formation and decreasing indicators of osteoporosis [63-65]. Bisphosphonates have had a beneficial effect on bone mineral density (BMD) in RA patients, particularly on steroids; this effect was less pronounced in comparison with normal menopausal women with osteoporosis [66,67].
2.3 Bone Loss in Younger Patients
Chronic inflammatory disease, systemic inflammation, RA negatively affects bone health. Complicated processes causing osteoporosis in younger people include rather inflammatory cytokines, dysregulation of Immunity, and other systemic variables. Thus, RA leads to chronic inflammation resulting in osteoblast differentiation and function impairment. This autoantibody aggravates this situation. This is done by some other disorders in the normal remodeling of bone processes such as RF and ACPAs. Other inflammatory cytokines, such as DKKI, and sclerostin, interfere with the Wnt signaling pathway, a pathway crucial for osteoblastogenesis, and further inhibit bone formation and skeletal health [68]
Bone metabolism is substantially influenced by the autoantibodies associated with RA. Neither these factors induce the process of osteoclast activation and systemic bone loss, nor can rheumatoid factor and ACPA be identified before the clinical manifestations of the disease. In RA patients, a poorer bone MBD is correlated to higher ACPA titers. Besides that, autoantibodies against osteoprotegerin (OPG) have similarly been shown in some studies to be enhancers of bone resorption by balancing resorption with production [69]. Various other systemic insults also favor the onset of osteoporosis in RA patients. Physical inactivity induced by joint pain and disability is another major cause of muscle wasting and diminished mechanical loading on bones, which ordinarily helps maintain bone mineral density. Long-term corticosteroid therapy, a common treatment in RA, severely impaired bone health by inhibiting osteoblast function while stimulating osteoclast activity. Inadequate nutrition, particularly insufficient calcium and vitamin D intake, is linked to a higher risk of osteopenia and osteoporosis in RA patients [70].
RA-related inflammatory processes cause significant joint destruction, including boning erosions and cartilage destruction. Due to joint instability and malalignment from cartilage destruction, bones frequently rub against each other, further enhancing injuries and pain. The chronic inflammation can cause periarticular erosions that may lead to structural instability in bones, and ultimately increase skeletal fragility [71]. RA progression can go beyond the joints. Restrictions to activity imposed by pain and disability result in the underlying occurrence of muscle atrophy or weakness from disuse and, thus, inadequate mechanical loading, or perhaps neither in support of bone density. On top of that, finding an acceptable diet may be a little bit out of the question for those with untreated RA due to pain and other physical restrictions. Such mineral deficiency conditions seem to carry an elevated risk of developing osteoporosis [72]. With all these acting together, the condition itself gives rise to a pattern of increased fracture risk. As has been documented, between 30 and 50 % of RA patients suffer from idiopathic osteoporosis: it increases the- chances of sustaining a hip fracture and other serious injuries, especially in younger patients who are untreated compared to their older peers [73].
3. Risk Factors for Osteoporosis in RA
3.1 Age-specific factors
With major hormonal changes taking place, postmenopausal women experience a steep drop in estrogen hormone levels essential to bone and muscle health. The decreased production of estrogen compounds the risk of osteoporosis while inciting enhanced muscle catabolism [74,75]. Compared to men, muscle strength declines more pronouncedly in women after menopause (1.5-3% yearly) while muscle mass decreases (1-2% yearly) [76]. Osteoporosis arises from higher rates of bone resorption induced by osteotropic cytokines siding with lost estrogen levels. Such bone loss, more than 2% annually, appears most pronounced during the initial start of menopause, a fairly high turnover period, in sites such as the spine [77,78]. Menopause-related hormonal alterations typically bring about inflammatory responses, with most proinflammatory cytokines acting to accelerate the muscle and bone degradation process [79,80]. Preventive treatments like hormone therapy (HT) appear promising in attenuating these adverse effects by maintaining muscle strength and lowering fracture risk, making them a feasible strategy for osteoporosis [81].
Early onset RA has numerous long-term dangers to skeletal health, manifesting between the ages of 30 and 50. In certain instances, chronic inflammation resulting from the inflammatory response in RA harms already functioning skeletal functions by pre-empting symptoms. In RA, a combination of elevated auto-antibodies, including rheumatoid factor (RF) and ACPA, cause systemic bone loss through the activation of osteoclasts. Joint pains and disabilities from RA lead to decreased physical activity that lowers mechanical loading on bones and insidiously contributes to muscle wasting which may further compromise the preservation of BMD. A sedentary lifestyle predisposes to osteoporosis. By the prolonged use of corticosteroids, there is likely to be enhanced osteoclast activity and inhibition of osteoblast function, which further aggravates some of the bone health issues caused by RA. These factors complicate the risk posed by patients who suffer from RA as regards osteoporosis and fragility fractures earlier in life. Higher ACPA titers have been associated with reduced BMD, which stresses early diagnosis and intervention to prevent these effects [82].
3.2 Medication Impact
In treating autoimmune and inflammatory diseases, GCs are widely used, and for this reason, the deficit of bone tissue may occur as a result of the use of the mentioned drug, causing Glucocorticoid-Induced Osteoporosis (GIOP). This disorder stems from multiple processes, including increased osteoblast apoptosis and a decrease in osteoblast proliferation, which affect critical pathways such as Wnt signaling in reducing bone formation. GCs induce bone resorption through stimulation of osteoclastic activity by increasing RANKL expression and repressing OPG [83,84]. Simultaneously, they disturb calcium homeostasis through suppression of intestinal and renal calcium absorption and reabsorption, which enhances bone loss and incites secondary hyperparathyroidism [84,85].
The risk for osteoporosis appears significantly linked to the length of glucocorticoid therapy and the amount used. Higher dosages and longer durations increase the risk of loss of bone density; even moderate doses such as 2.5 mg daily of prednisolone can produce measurable trabecular bone loss within a few months [84,86]. Also independent of prior or current bone mineral density status exposure to glucocorticoids can increase the risk for osteoporosis by total cumulative bone loss and inducing susceptibility to fracture [85].
The other factors also include age and gender, since postmenopausal women are especially at risk due to hormonal changes that worsen bone density loss [85,87]. Age-associated hormone therapy and bone loss are even more felt in older people, who also show a tendency to develop comorbidities that require treatment with glucocorticoids [84]. Sedentary behavior tends to lessen mechanical pressure on bones, while inadequate calcium and vitamin D intake also diminish bone mineralization. A lifestyle that is marked by sedentary behavior and inadequate diet adds to these considerations. GIOP has to be prevented long while treating patients on long-term glucocorticoid therapy, with such multifactorial associations being addressed [83,84,87].
For patients with rheumatoid arthritis (RA), biologics and disease-modifying antirheumatic agents (DMARDs) contribute to a significant improvement in bone density, addressing direct inflammation as the reason for loss of bone integrity. The mechanisms by which these medicines achieve this are based on certain inflammatory cytokines, such as TNF and IL-6, which contribute to systemic inflammation, an important cause of bone loss. By inhibiting these cytokines, biologics precede a bone-erecting effect by increasing osteoblast activity and down-regulating osteoclast activity, which creates a net positive impact on bone resorption [88,89]. RA patients have complained of long-term biologic treatments being responsible for the decrease in osteoporosis and the number of osteoporotic fractures. Likewise, bone loss is hindered by biologics as they also render the RANKL, the main source of bone resorption, ineffective [90,91].
In addition, when RA symptoms are effectively controlled by biologics, patients experience improved quality of life and improved mobility. Active bone mechanical loading requires physical activity to maintain bone strength, and improved mobility enables this. Psychological and physical benefits from less pain and improved function encourage further lifestyle changes promoting bone health [88,89,91].
3.3 Lifestyle and Nutritional factors
Factors that can impact on bone mass during adolescence are genetic, dietary, and behavioral (exercise) factors. The primary factors influencing age-related bone loss in adults and older adults are gonadal status, the effects of certain nutrients, and levels of physical activity [92]. Calcium and Vitamin D are one of the two minerals required for healthy bones. When osteoporosis occurs or bones have been weakened by low calcium, a possible vitamin D deficiency can be the first step to address. This includes not only prolonged and acute vitamin D deficiency but also metabolic bone diseases with reduced bone matrix mineralization or elevated osteoid accumulation. Serum 25(OH)D levels, which are the main form of vitamin D in the body that is present in the biological fluid, are a reliable indicator of a deficit [93-95].
Calcium intake in different age groups has a strong effect on bone mass. Calcium supplementation reduces the rate of age-related bone loss in adults [96]. Typically, calcium supplements reportedly minimize bone loss by 1% per year, while they also prevent bone loss in the elderly, where lower dietary consumption of calcium results in better bone response [97]. Here, serum PTH appears to be the key mechanism through which calcium supplementation attenuates skeletal loss. The effects on parathyroid are summoned by combined weaknesses of low calcium intake and absorption to Vitamin D deficiency, which increase the PTH and turnover of minerals in the bones as people age [98,99]. Vitamin D is synthesized in the skin following exposure to UV radiation and steroid precursors; the main sources of vitamin D are limited to some foods, and dietary sources are crucial when there is limited exposure to sunlight. Vitamin D is in many respects a steroid prohormone, biologically inert until it has undergone metabolic activation [100]. Initiate with the less soluble calcium salts: calcium carbonate must be taken with meals, which helps to dissolve the salt in the stomach by the action of gastric acid. However, such constituent issues with more soluble calcium salts, in which calcium might not be absorbed from the carbonate salt, are included in phosphate, oxalate, and phytate [101]. A special role for vitamin K has been invoked about osteoporosis and, specifically, the risk of hip fracture. Clinical trials have shown that people who experience hip fractures have lower levels of vitamins K1 and K2. The gamma-carboxylated glutamyl residues of osteocalcin (OC), which are associated with the skeleton and affect bone metabolism, are formed only in the presence of vitamin K [102].
Table No. 1: The impact of various risk factors on bone health.
|
Risk Factor |
Description |
Impact on Bone Health |
|
Postmenopausal Hormonal Changes |
The decline in estrogen levels after menopause. |
Increased risk of osteoporosis, muscle catabolism, and bone resorption. |
|
Rheumatoid Arthritis (RA) |
High levels of auto-antibodies (RF and ACPA) cause chronic inflammation. |
Increased osteoclast activity, decreased physical activity, joint pain, and systemic bone loss. |
|
Glucocorticoids Use (GCs) |
Corticosteroid treatment over an extended period. |
The risk of glucocorticoid-induced Osteoporosis (GIOP), secondary hyperparathyroidism, bone remodeling imbalance. |
|
Biologics and DMARDs |
Medications used to manage RA |
Reduce glucocorticoid dependence, enhance bone density, lower osteoclast activity, and lessen inflammation. |
|
Calcium and Vitamin D Deficiency |
Inadequate intake or absorption of nutrients from the diet. |
A higher risk of osteoporosis, secondary hyperparathyroidism, and decreased bone mineralization. |
|
Sedentary lifestyle |
Lack of physical activity |
Decreased mechanical stress on bones, which leads to muscle atrophy and bone loss. |
|
Aging |
Bone density naturally decreases with age |
Comorbidities requiring glucocorticoids exacerbate an increased risk of osteoporosis and fractures. |
|
Vit K Deficiency |
Low levels of Vit K1 & K2 are indicative of a Vit K deficiency. |
Reduced bone metabolism and a higher chance of hip fractures. |
|
Gender (Female) |
Women who have gone through menopause are more vulnerable because of hormonal changes. |
Accelerated bone loss especially after menopause, in comparison to men. |
|
Nutritional Factors |
A poor diet & low calcium intake. |
Contribute to accelerated bone loss & low peak bone mass. |
4. Diagnostic and Monitoring Challenges
4.1 Limitations of current diagnostic tools
Dual-energy X-ray absorptiometry (DXA) is a diagnostic radiographic technique used for estimating bone mineral density (BMD) and diagnosing osteoporosis, more particularly in rheumatoid arthritis (RA) patients. Glucocorticoids, a common prescription in RA therapy, are responsible for causing bone loss. They are often prescribed in rheumatology and therefore their role in diseases such as arthritis is significant [103,104]. However, the DXA involves significant problems. In order to be recognized, it needs generally at least 30% bone mass loss, which has rendered it not so very sensitive for detecting early bone loss. In this way, diagnosis and therapy cannot get underway rapidly [105]. Moreover, DXA assesses the total bone mineral density (BMD) but does not differentiate between local bone loss affecting regions involved in RA and systemic bone loss affecting overall skeletal health. In essence, this lack of clarity may result in localized damage being underestimated, which has a bearing on effective management [104,106]. Added to that, DXA may not take into account the possible differences in administration routes and dosages of glucocorticoid medications; such variability may be particularly important in determining fracture risk [103,104]. Alternative means of getting a diagnosis are being explored in view of these shortcomings. QCT basically gives a three-dimensional evaluation of bone density, which can inform better on localized changes appearing. New ultrasound methodologies that employ non-ionizing measurements of BMD include REMS, which may be more sensitive to localized changes in the RA-affected areas. DXA will still remain an important tool for the assessment of osteoporosis among RA patients [104,106,107]. What follows is a discussion of its shortcomings, and it's time to draw attention to the need for other diagnostic instruments to give a broader understanding of both local and systemic bone health-such is essential for optimizing patient care and avoiding RA-induced bone loss-related issues. Diagnosing rheumatoid arthritis (RA), especially if it becomes difficult to treat (D2T), can be done with great difficulty. All current diagnostic tools, such as biomarkers and conventional imaging methods, cannot adequately assign disease diagnosis or management. With varied and frequently inadequate diagnostic criteria, a number of studies assessing those tools show some moderate to high risk of bias [108, 109]).
However, said new imaging methods represent promising alternatives. The ultrasound method becomes effective in evaluating inflammatory activity in RA patients with aggravating comorbidities like obesity or fibromyalgia after visualizing synovitis and other inflammatory changes [108,109]. MRI, in addition to providing a full view of soft tissues, identifies early inflammatory changes, such as bone marrow edema and synovitis, which is a very important pointer as the RA progresses [108]. Technological developments in AI provide faster diagnostics. The advanced machine learning and deep learning algorithms very precisely and efficiently carry out analysis on medical images, hence using the clinical parameters to boost detection accuracy over the traditional methods [110].
Also, the development of the research on biomarkers is notable. In the current diagnostic stage is also the testing for anti-citrullinated protein antibodies; however, research is continuing to find other more clinically valuable biomarkers providing prognostic and active disease-related suggestions. Genomic studies are, in quest of finding promising candidates, assessing genetic markers for their association with rheumatoid arthritis in order to improve early diagnosis and therapy stratification. Such biomarkers may, in some cases, be of great service in the differential diagnosis of RA from related disorders [110]. Even with the promise that these emerging imaging techniques and investigations of serological markers for diagnosing RA better will have great potential in the enhancement of disease care and the monitoring of the disease, faultiness in current diagnostic techniques for RA warrant the construction of novel and modified techniques for better diagnosis and monitoring, especially in D2T cases. The need for continuous research and validation in those areas to promote rheumatologic practice is accentuated.
4.2 Fracture risk assessment in RA
The World Health Organization's FRAX tool takes some clinical risk factors into account, including RA, to estimate 10-year probabilities for osteoporotic fractures. Although FRAX has been validated and shown to predict fracture risk quite accurately, it has severe limitations when it comes to taking bone mineral density (BMD) into account. FRAX is claimed to be poorly calibrated and may overestimate the fracture risk in patients who are already considered high-risk; estimates for RA patients are less accurate than those for non-RA populations [111, 112]. Furthermore, in the case of rheumatoid arthritis, FRAX ignores inflammation and disease activity-both of which severely limit bone loss in RA. The effectiveness varies in different populations, and may underestimate risk both in younger RA patients and those not taking glucocorticoids. To enhance the assessment of fracture risk [113], the following practices, including the use of additional biomarkers associated with inflammation and the metabolites of the bones as well as the utilization of advanced imaging techniques such as quantitative computed tomography (QCT) and the development of personalized risk assessment models, would all be beneficial. While FRAX is regarded as reliable, its use in combination with the current methods might bring an care optimization.
5. Prevention and Management Strategies
5.1 Pharmacological Interventions
In Rheumatoids, osteoporosis and fractures are more common as compared to the application of glucocorticoids and chronic inflammation. Anti-osteoporotic treatments like denosumab and bisphosphonates are usually suggested to achieve the same outcome. Bisphosphonates have been shown to maintain bone mineral density (BMD) in RA patients by inhibiting bone resorption. In some studies, the monoclonal antibody denosumab has even been shown to perform better than bisphosphonates in improving BMD and slowing joint damage in RA [114].
Combining techniques for maintaining bone health with RA-specific therapies, particularly bDMARDs, furthers a comprehensive method of controlling both bone loss and joint inflammation. Retaining bone health, in addition to regulating disease activity, is the desired aim of biologics by reducing inflammatory cytokines. Interleukin 6 inhibitors are shown to be beneficial in localized bone loss, and anti-TNF medications have developed a neural link with enhanced dual-site BMD [115].
It can be hypothesized that implementing bDMARDs together with anti-osteoporotic drugs may yield some synergistic benefits. Research indicates that people with RA receiving long-term biologic therapy along with anti-osteoporosis treatment are better protected against bone loss than those receiving only anti-TNF inhibitors or traditional synthetic DMARDs [116]. Anti-osteoporotic drugs such as denosumab and bisphosphonates together with RA-specific therapies such as biologics are key to optimizing bone health in RA patients. This comprehensive approach aims to improve overall patient outcomes while decreasing fracture incidence.
5.2 Non-Pharmacological Interventions
Related conditions such as osteoporosis and rheumatoid arthritis (RA) require a holistic approach to their treatment, involving dietary and activity plans tailored specifically to the needs of the patient. Exercise aids in maintaining the health of the bones, adds to one's physical performance, and ultimately counteracts its associated effects with osteoporosis and RA. High-intensity progressive resistance training (PRT) is able to improve physical function, ameliorate rheumatoid cachexia, and gradually increase muscle strength without aggravating disease activity, as shown by the report [117]. The RAPIT trial has shown that long-term high-intensity weight-bearing exercise decreases BMD loss at the hip and shows further that weight-bearing exercises are especially useful in maintaining bone mineral density (BMD) [118]. Walking, cycling, and swimming form the basis for regular aerobic exercise that promotes cardiovascular health. This is particularly important for RA patients, who face an enhanced cardiovascular risk, therefore being chiefly dependent on such workouts [119].
Aquatic exercises promote a resistance workout that is joint-friendly in patients with severe pain or mobility issues while flexibility and range of motion exercises-yoga and tai chi-are anti-rheumatic due to their ability to relieve joint stiffness [120, 121]. Nutritional strategies are another complementary solution since calcium is key for bone health, and so is vitamin D, which can be sourced from dairy, leafy greens, fatty fish, and fortified food [122]. An anti-inflammatory diet rich in fruits, vegetables, whole grains, nuts, and omega-3 fatty acids promotes both joint and bone health, reducing inflammation. To promote bone health, however, one should limit alcohol and caffeine intake, which impair calcium absorption. A combination of individualized exercise regimens with the same array of nutritionally balancing therapies allows physicians to approach these twin problems with efficacy: osteoporosis and RA on the enhancement of bone health and improved patient outcomes [123,124].
5.3 Age-Specific Preventive Approaches
Hormonal changes, heightening symptoms and comorbidities risk, especially osteoporosis, one other challenge already grappled with by post-menopausal women suffering from rheumatoid arthritis (RA). In fact, post-menopausal women are 35% more susceptible to RA when compared with pre-menopausal women, supporting the idea that RA activity is heightened by changes in post-menopausal estrogen levels. This risk is aggravated following the onset of early menopause [125]. Besides, low estrogen levels therefore hasten the loss of bone, rendering individuals much more susceptible to osteoporosis and fractures. In this group, assessing BMD and fracture risk will require routine bone health monitoring via DEXA images. Although hormone replacement therapy (HRT) is generally not given because of associated cardiovascular risks with RA, pharmacologic therapies such as denosumab and bisphosphonates are often employed to prevent bone loss [126,127]. Complementary approaches may involve tailored weight-bearing exercise programs and dietary interventions that ensure adequate calcium and vitamin D consumption for the maintenance of bone health [128,129].
Long-term care for younger RA patients differs from older ones in the fact that an assessment of both acute and future implications needs to be accounted for. Early intervention using biologics or DMARDs to control disease progression and minimize joint damage can be associated with better long-term outcomes [130,131]. Aspects of the treatment may extend past medical necessity to include a multidisciplinary team of rheumatologists, physical therapists, dietitians, and counselor-psychologists deliberating over physical, nutritional, and psychological needs toward a positive outcome with complete care. Various anti-inflammatory diets, rich in omega-3 fatty acids, antioxidants, and key micronutrients, are important in maintaining good health, while, on the side, regular exercise, low-impact aerobic exercise, strength training, and flexibility exercises help maintain mobility and relieve fatigue [132,133]. Constant evaluation of joint function, disease activity, and general health is critical for adjusting treatment regimens and preventing long-term RA consequences, such as osteoporosis or cardiovascular problems. For all RA patients, including those who have gone through menopause, individualized approaches that optimize results and improve the quality of life are a boon [134,135].
CONCLUSION
Osteoporosis is often seen as a comorbidity with rheumatoid arthritis (RA) presents a significant challenge due to its complex etiology, which involves inflammatory cytokines, hormonal factors, and adverse drug reactions. Although quite a bit has been learned about the mechanisms behind bone loss in RA, there are still ample gaps in age- and gender-specific therapies, personalized treatment plans, and early identification. A multidisciplinary approach with the participation of rheumatology, endocrinology, and orthopedics must be adopted because of osteoporosis complexity due to RA.
Selective research is needed since large variances exist between postmenopausal women and men or younger ages regarding osteoporosis's representation. State-of-the-art diagnostic technologies like QCT and REMS could potentially revolutionize risk stratification and early detection, coupled with the development of new biomarkers. Biologics in treatment hold promise not only to stabilize bone density but also to alleviate the inflammation involved. However, optimizing combination treatments and reducing adverse effects of previously available drugs are still the hottest targets.
Prevention measures, such as protecting the general public through customized dietary and other lifestyle interventions, are crucial for lightening the load of osteoporosis. Fundamental to enhancing bone health at all ages are promoting weight-bearing activities and ensuring sufficient calcium and vitamin D intake. Moreover, aggressive and early management of RA with DMARDs and biologics shall not only prevent systemic bone loss but also help improve long-term results.
These areas of investigation and understanding will continue to promote comprehensive care by teamwork and creativity in research. With these programs targeting the twin issues of osteoporosis and the quality of life of people with RA, we look forward to improvements in the lives of both populations.
REFERENCES


Sushma M, Dr. Manjunatha PM, Gayathri S V, Nikhil H R, Uday R, Inflammation Meets Hormonal Deficiency: Osteoporosis in Postmenopausal Women with Rheumatoid Arthritis., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, https://doi.org/10.5281/zenodo.21393565
 10.5281/zenodo.21393565
10.5281/zenodo.21393565