
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
SGMSPM’s Sharadchandra Pawar College of Pharmacy, Otur
Levofloxacin, the active S-(-) isomer of ofloxacin, is a broad-spectrum fluoroquinolone antibiotic effective against Gram-positive, Gram-negative, and atypical pathogens by inhibiting bacterial DNA gyrase and topoisomerase IV. This review details its chemical structure as a pyridone carboxylic acid derivative (molecular weight 361, pKa 5.70-6.05 and 7.90-8.22), physicochemical properties including pH-dependent solubility (30–300 mg/mL between pH 1-8), and pharmacokinetic profile featuring high bioavailability (>95%), extensive tissue distribution, minimal metabolism (<5%), and primary renal excretion (60-80% unchanged). Various analytical techniques for its quantification—such as UV spectrophotometry (?=292-331 nm), HPLC (isocratic mobile phases at 294 nm), HPTLC (silica gel plates at 298 nm), and LC-MS/MS—are evaluated for precision, accuracy, and stability-indicating capabilities in pharmaceuticals, plasma, and tissues. Clinical applications include urinary tract infections, prostatitis, and post-exposure prophylaxis for anthrax, underscoring its bactericidal efficacy and favourable tolerability
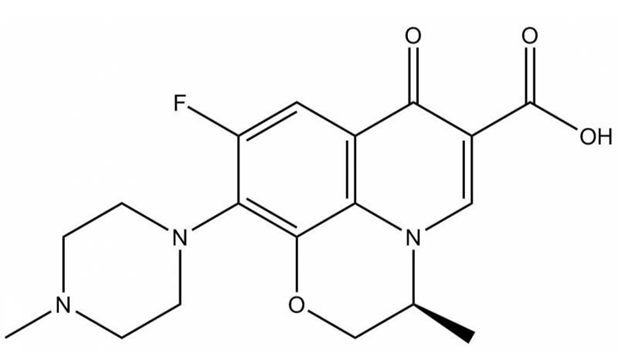
Levofloxacin { (2s)_7fluoro-2-methyl-6-) 4-methylpiperazine-1-yl)-10-0-1azatricyclo-11-carboxylic acid}. Levofloxacin is another name for the fluoroquinolone antibiotic.It is a broad-spectrum antibiotic. It is a second-generation antibacterial drug that works very well against both gram-positive and gram-negative bacteria. It promotes bacterial lysis by blocking bacterial DNA gyrase, which is necessary for DNA replication. Here is a review of several analytical techniques that have been described for levofloxacin measurement. There have been reports of UV spectrophotometric, HPLC, HPTLC, fluorimetric, bioanalytical, and UPLC procedures. In addition to these bioanalytical techniques, stability-indicating analytical methods and visual spectrometric approaches have also been published for the measurement of levofloxacin in blood.[1]Levofloxacin, a later-generation antibacterial drug belonging to the fluoroquinolone class, exhibits exceptional efficacy against both Gram-positive and Gram-negative bacteria, in addition to atypical respiratory and urogenital tract pathogens. Levofloxacin has typically been used as a second- or third-line treatment for H. pylori, however some studies have shown that levofloxacin-containing regimens are beneficial as a first-line treatment.[2]Similar to other fluoroquinolones, levofloxacin actively enters phagocytic cells in vitro, which has important consequences for its ability to combat intracellular infections. The substantial V d observed is a result of significant levofloxacin accumulation in phagocytic cells and other organs.[3]* The active isomer of ofloxacin, levofloxacin (LVLXDR-3355), is a fluoroquinolone medication that was created in Japan in 1986. Because it is more effective than ofloxacin and has superior tissue distribution and fewer side effects, it is frequently utilized in clinical practice. Levofloxacin, which often has analgesic and anti-inflammatory properties, is the recommended medication for treating osteoarthritis induced by viral causes.However, levo-floxacin does not yet have an effective therapeutic impact because the majority of osteoarthritis is a condition caused by degenerative changes in the joints. One of the most prevalent musculoskeletal conditions in the world today is osteoarthritis (OA).[4]Levofloxacin’s tolerability profile is comparable to that of other oral fluoroquinolones, with the most often reported side effects being in the gastrointestinal and central neurological systems. Patients using concurrent levofloxacin do not seem to require a change in theophylline dosage.Levofloxacin absorption is decreased when it is used with antacids or other medications that include divalent or trivalent cations.[5] In plasma or urine, levofloxacin is stereochemically stable and does not change back into its less active isomer, D-ofloxacin. 24- Levo-floxacin has a mean renal clearance of 7.14 L/h per 1.73 m 2 and a total body clearance of about 8.5 L/h per 1.73 m 2, indicating low extrarenal clearance.[6]
Chemistry of Levofloxacin:
Levofloxacin is a pyridone carboxylic acid derivative that shares structural similarities with nalidixic acid and more recent fluorinated quinolone antibacterial medicines (fig. I). The parent molecule, ofloxacin, is a racemic combination of S-(-) and R-(+) isomers due to the presence of a methyl group at the oxazine ring’s 3-carbon position. Since levofloxacin is the pure S-(-) isomer of ofloxacin, it differs from ofloxacin. The commercially available substance, levofloxacin hemihydrate, has a molecular weight of 370.380.Levofloxacin is sparingly soluble in water and readily soluble in glacial acetic acid and chloroform. Pharmacokinetic investigations have been carried out on both oral tablets and intravenous preparations.[3]LVFX has a melting point of 228.6°C and is an odorless, white to yellow, crystalline powder when it is solid. 361 is its molecular weight. With an octanol:water partition coefficient (log P) of 0.6, LVFX is essentially insoluble in water but soluble in ethanol, chloroform, and ethanol–water mixtures. Two ionizable functional groups are present in LVFX: a basic piperanyzyl group (pKa2=8.22 and 7.90) and a carboxylic group (pKa1=6.05 and 5.70). Between pH 1 and pH 8, LVFX has a pH-dependent solubility range of roughly 30–300 mg/mL.[7]
Properties of Levofloxacin:
Pharmacokinetic Properties:
Non-compartment analysis was used to determine the PK parameters of levofloxacin in plasma, lung, and bronchial mucosa. Cmax, peak time (Tmax), area under the time-concentration curve from time zero to infinity (AUC0–24), half life (T1/2), mean residence time until 24 hours (MRT0–24), total apparent clearance (CLt/F), apparent volume of distribution (Vd/F), the ratio of Cmax in tissue vs. plasma (RCmax), the ratio of levofloxacin AUC0–24 in tissue vs. plasma (RAUC_0–24), and the latter three parameters indicate the permeability of levofloxacin in lung or bronchial mucosa.[8]
Absorption:
The duodenum and jejunum absorb the more recent quinolones, like levofloxacin and sparfloxacin, which easily dissolve in the gastrointestinal (GI) tract.However, the various drugs have varied tmax and bioavailability. The bioavailability of all the more recent fluoroquinolones is either equivalent to or higher than that of ciprofloxacin, which ranges from 55 to 88%.Excellent bioavailability is exhibited by levofloxacin and gatifloxacin (>95%), followed by sparfloxacin (92%) and moxifloxacin (86%).Notably, the duodenum and colon appear to absorb sparfloxacin through both carrier-mediated and passive processes. Because of the lower absorption, bioavailability decreases with larger doses.[9]
Distribution:
When designing the LVX dosage regimen to achieve AUC/MIC and Cmax/MIC values with higher probabilities of clinical success and avoidance of resistance, the apparent volume of distribution value demonstrated a statistically significant correlation with the severity of illness on the Simplified Acute Physiology Score II.36 CrCl, as well as total bodyweight and severity of illness.[10]
Metabolism:
In rats, dogs, monkeys, and/or humans, three levofloxacin metabolites have been found in trace amounts. Levofloxacin-~-D-glucuronide (M1), desmethy 1-levofloxacin (M2), and levofloxacin-N-oxide (M3) are these metabolites.In humans, only the M2 and M3 metabolites have been identified. In humans, levofloxacin has a restricted metabolism and is mostly eliminated unaltered in the urine. Less than 5% of levofloxacin was eliminated in the urine as metabolites in 24 hours after a single oral dose (M2 and M3 accounted for roughly 1.75 and 1.63% of the dose, respectively), while roughly 79.6% of the dose was recovered in the urine as unaltered drug in the next 24 hours.[3]
Excretion:
When compared to ciprofloxacin, all of the more recent agents have longer elimination half-lives (t1 −2β), which helps explain why they can all be administered as a single daily dose (tables I and II). However, dose frequency is also predicted by the target species’ susceptibility. Levofloxacin is mostly eliminated by the kidneys, and between 60 and 80 percent of the dosage is recovered unaltered in the urine. Levofloxacin’s final clearance is around 60% higher than creatinine clearance, indicating that it is eliminated by both tubular secretion and glomerular filtration.[9]
Pharmacodynamics:
Optimal regimens and dosages can be determined with the help of PD evaluation, integration of pharmacokinetic (PK) parameters with MICs, and correlation of such results with clinical or bacteriologic outcomes (so-called PK/PD modeling). Nonetheless, gram-negative infections were the source of many of the recognized serum concentration-dependent breakpoint parameters. For S pneumoniae, clinical effectiveness is equivalent to a maximal plasma concentration:MIC ratio of around 12 for levofloxacin.[9]
Solubility of Levofloxacin:
The gastrointestinal tract condition was represented by the solubility value of LFCA (2:1) In water and phosphate buffer solution pH 6.8 and 7.4, which were then compared to LFs. 6.8 g of dihydrogen potassium phosphate (KH2PO4) and 1 g of sodium hydroxide (NaOH) were combined and dissolved in 1L of distilled water to create a buffer solution with a pH of 6.8. A pH meter was used to measure the final pH after a few drops of 0.05 N NaOH solution were added. Next, 1.179 g of dihydrogen potassium phosphate (KH2PO4), 4.303 g of disodium hydrogen phosphate (Na2HPO4), and 9 g of sodium chloride were dissolved in 500 mL of distilled water to create a buffer phosphate solution with a pH of 7.4 The samples were put into 10 mL Erlenmeyer tubes, filled with each medium (water and buffer phosphate pH 6.8 and 7.4, respectively, approximated the gastric and ileum environments), sealed, and shaken at room temperature at 25 rpm. The solid sample was added until a saturated state was indicated by some granules remaining undissolved. Next, using a Beckman DU640 UV/Vis Spectrophotometer (Indiana, USA) and validated UV spectrophotometry under λ = 331 nm, the LF solubility was ascertained using the same manner as the stability test.[10]
Analytical Methods of Levofloxacin:
HPLC Method of Levofloxacin:
A Shimadzuw LC-10AD HPLC system with a UV-vis detector model SPD-10A was used to carry out the HPLC procedure. Shimadzuw Class-VP software was used for data integration. A reversed phase Phenomenexw Synergi Fusion-RP (150 4.60 mm i.d., 4 mm particle size) served as the analytical column. Every analysis was carried out under isocratic conditions at room temperature (24 + 28C). A combination of water, acetonitrile, and phosphoric acid 0.025 M was used as the mobile phase. Triethylamine (60:20:20, v/v/v) was used to adjust the pH to 3.0. The injection volume was 20 mL, and the flow rate was 1.0 mL/min. At 294 nm, the UV was detected.Using 1.0 cm quartz cells and a UV-vis Genesys 2 Spectronic at 292 nm, the spectrophotometric technique was carried out.20 mg of precisely weighed levofloxacin reference standards (99.97%) were moved to 20 mL volumetric flasks and diluted in mobile phase (final concentration 1000 mg/mL). After 10 minutes of sonication, the resultant solution was diluted to reach a final concentration of 10 mg/mL. Every day, fresh solutions were made.[11]
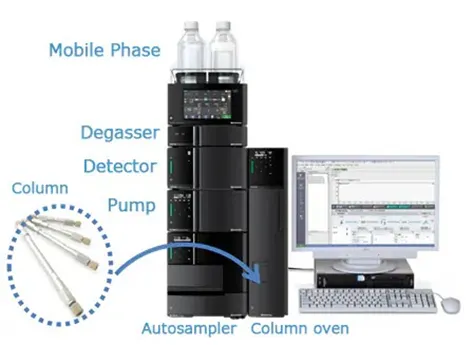
Fig.2 HPLC
UV of Levofloxacin:
Levofloxacin is an antibiotic classified as a fluoroquinolone.It has two pka values, 5.59 and 7.94, and is soluble in water (PH 6.7).Because it dissolves in water, water can be employed as a solvent in UV spectrophotometry. As a result, water was used as a solvent in several of the described techniques.However, one approach uses a solvent of 0.1M hydrochloric acid.It might be because Levofloxacin’s Pka values are 5.59 and 7.94, and it’s best to keep Pka values two units apart from Pkavalue. Levofloxacin is present in both ionized and unionized forms when water is utilized as asolvent. The solvent has been a mixture of acetonitrile, methanol, and water. The response’s linearity in the given procedures is suitable for 2–12 µ/ml.There have also been reports of a visible spectrophotometric approach based on the condensation product produced when 2,4-dinitrophenylhydrazine reacts with Levofloxacin’s carbonyl group.[1]

Fig.3 Ultra-Violet Spectroscopy
HPLC/MS of Levofloxacin:
Different combinations of mobile phases, such as methanol-aqueous ammonium formate solution (10 mM), formic acid methanol solution-water, and formic acid methanol solution-aqueous formic acid solution with different ratios, were tested and optimized to produce symmetric peak shapes and a short analysis time.Using eluent A and eluent B (79:21, v/v) as the mobile phase produced the best peak morphologies, separation, resolution, and analysis time. Within 3.5 minutes, LVF, CPR, and IS were eluted with symmetric peak morphologies; their respective retention durations were 1.9, 2.5, and 2.8 minutes. To prevent possible sample.A needle wash protocol was developed for carryover in isocratic elution mode. Tests were conducted on washing solutions made of water, methanol, acetonitrile, and isopropyl alcohol, as well as their combinations in different ratios. After applying a needle wash with 50% aqueous methanol supplemented with 0.1% formic acid in between injections, the complete removal of sample carry-over was recorded. A mixture of standard solutions containing each fluoroquinolone at a concentration of 0.1 g/ml was injected in order to optimize the MS/MS conditions.[12]
LC MS/MS of Levofloxacin
To guarantee the dependability and repeatability of the analytical measurements, the LC-MS method’s precision and accuracy were thoroughly assessed. FPSE was used to extract LEV samples spiked into plasma at four distinct concentration levels (0.005, 0.015, 0.048, and 0.727 μg mL−1), including the LLOQ value. A set of replicate samples (n = 6) of the same matrix with known quantities of the target analytes were analyzed to assess intraday and interday precisions. By comparing the measured concentrations to the known concentrations of the spiked samples, intraday and interday accuracy were evaluated. The data are shown in the Supporting Information File, where recovery values exceed 97.2% and the RSD% ranges from 1.0 to 8.6%.[13]
HPTLC of Levofloxacin:
Aluminum-backed silica gel 60 F254 TLC plates that had been previously cleaned with methanol were used for chromatography; the plates were prepared in a Camag twin-trough chamber using a water-methanol-n-butanol-ammonia solution (25%), 5 + 5 + 5 + 0.4 (v/v).Levofloxacin standard solutions were moved to various 10-mL volumetric flasks and diluted to volume with methanol, resulting in final levofloxacin concentrations of 0.8–3.0 lg lL–1, each containing 0.3 lg lamotrigine (IS). A Camag Linomat IV sample applicator was used to apply standards and samples (2.0 lL levofloxacin containing 0.3 lg lamotrigine) in 6-mm bands to the plates.Following plate development and drying, both medications were assessed by scanning densitometry at k = 298 nm using a Camag TLC Scanner III under the control of CATS.V.4.06 software (Camag). For every peak, peak areas were noted. The following formula was used to calculate the amount of levofloxacin from the peak area: Amount of levofloxacin = (Rspl 6 C 6 D 6 Average wt)/(Rstd 6 W), where Rspl is the area of the levofloxacin sample peak, Rstd is the area of the levofloxacin standard peak, C is the concentration of standard solution [mg mL–1], D is the dilution factor, and W is the weight of the tablet [mg].[14]

Fig.no.4 HPTLC
Application of Levofloxacin
CONCLUSION
Levofloxacin stands out as a versatile second-generation fluoroquinolone with superior tissue penetration, once-daily dosing potential due to its prolonged half-life, and robust activity across diverse infections via concentration-dependent pharmacodynamics (e.g., Cmax/MIC ≥12 for Streptococcus pneumoniae). Analytical methods like HPLC, UV, HPTLC, and LC-MS/MS offer reliable, validated tools for quality control, bioavailability assessment, and therapeutic monitoring, supporting its widespread pharmaceutical use despite interactions with cations and minor side effects in gastrointestinal and CNS systems. Future research could explore novel formulations to enhance solubility and mitigate resistance risks, reinforcing levofloxacin's role in clinical practice.
REFERENCES





Yadav Abhishek, Tembhekar Swaraj, Thorat Om, Tekale Mandar, Levofloxcin: Chemistry, Analytical Methods, Pharmacokinetics, And Clinical Applications - A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 8075-8082, https://doi.org/10.5281/zenodo.20465196
 10.5281/zenodo.20465196
10.5281/zenodo.20465196