
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
SVPM college of pharmacy Malegaon, Baramati
Lymphatic filariasis (LF) is a parasitic disease caused by filarial nematodes — primarily Wuchereria bancrofti, Brugia malayi, and Brugia timori — transmitted to humans through the bites of infected mosquitoes. (NCBI) Infection is typically acquired in childhood, where it silently damages the lymphatic system, and later in life manifests as painful and profoundly disfiguring conditions including lymphoedema, elephantiasis, and scrotal swelling. ((CDC) Recurrent secondary bacterial infections of the affected extremity, characterized by severe pain, fever, and chills, hasten the progression of lymphedema to its advanced stage, known as elephantiasis. An additional complication is tropical pulmonary eosinophilia (TPE) syndrome, a potentially serious, progressive lung disease characterized by fever and nocturnal cough. (CDC) Diagnosis is typically made using blood smears and serologic tests, including antigen assays. (CDC) Lymphatic filariasis is endemic in 72 countries worldwide, and the resulting disfigurement and disability can lead to physical impairment, social stigmatization, and loss of employment. (medrxiv) Since 2000, more than 9 billion treatments of antifilarial medicines — combinations of albendazole, diethylcarbamazine, and/or ivermectin — have been distributed through mass drug administration (MDA) programmes in 72 endemic countries, and 17 countries have reached elimination as a public health problem. (PLOS) The WHO's Global Programme to Eliminate Lymphatic Filariasis (GPELF) aims to stop transmission through MDA and to alleviate suffering through morbidity management and disability prevention.
INTRODUCTION
History Of Filariasis
Ancient medical records indicate that Lymphatic Filariasis (LF), particularly elephantiasis, has been recognized for thousands of years. Around 600 B.C., the Indian text Sushruta Samhita described Shleepada, a condition characterized by severe swelling of the limbs, closely resembling modern bancroftian filariasis [8,9]. Persian physicians of the same era also documented similar symptoms, suggesting early recognition of the disease [11,15].
Evidence from artifacts and historical depictions indicates that LF may have existed as early as 1500 B.C. In ancient Egypt, reliefs from the funeral temple of Hatshepsut at Thebes—now displayed in the Egyptian Museum—depict individuals with swollen limbs consistent with elephantiasis [11,15]. These findings demonstrate that LF affected early civilizations and was interpreted according to prevailing medical theories of bodily fluid imbalances.
Overall, historical descriptions from India, Persia, and Egypt confirm the long-standing presence and recognition of LF in ancient societies [8–15].

Figure 2.Ancient illustrations depicting cases of elephantiasis adapted. (a) The statue of Pharaoh Mentuhotep depicting a swollen limb, (b) the princess of Punt with elephantiasis.
|
Stage
|
Signs & Symptoms |
Description |
||
|
Asymptomatic Stage |
No visible symptoms |
Many infected individuals show no external signs but have microscopic microfilariae in blood and lymphatic damage. |
||
|
|
Lymphatic vessel dilation |
Silent damage to lymphatic system detectable through imaging. |
||
|
Acute Stage (Acute Adenolymphangitis – ADL) |
Fever |
Recurrent episodes of high fever. |
||
|
|
Painful lymph nodes |
Tender, swollen lymph nodes (lymphadenitis). |
||
|
|
Red, inflamed skin |
Inflammation along affected lymph vessels. |
||
|
|
Limb pain and swelling
|
Temporary swelling of arms, legs, or scrotum. |
||
|
Chronic Stage |
Lymphedema
|
Persistent swelling of limbs due to lymph blockage. |
||
|
|
Elephantiasis |
Thickened skin and massive enlargement of limbs. |
||
|
|
Hydrocele |
Swelling of the scrotum in males due to fluid accumulation. |
||
|
|
Skin changes |
Hardening, darkening, thickening, fissures, and nodules. |
||
|
|
Reduced mobility |
Difficulty walking or using affected limb. |
||
|
Complications |
Secondary bacterial infections |
Recurrent infections worsen swelling. |
||
|
|
Psychological distress |
Social stigma, depression, disability. |
Cause and transmission
Lymphatic Filariasis is caused by infection with parasites classified as nematodes (roundworms) of the family Filarioidea.
There are three types of these thread-like filarial worms:
Adult worms reside in the lymphatic vessels and disrupt the normal function of the lymphatic system. The worms can live for approximately 6–8 years and, during their lifetime, produce millions of microfilariae (immature larvae) that circulate in the blood [17-18].
Mosquitoes are infected with microfilariae by ingesting blood when biting an infected host. Microfilariae mature into infective larvae within the mosquito. When infected mosquitoes bite people, mature parasite larvae are deposited on the skin, from where they can enter the body. The larvae then migrate to the lymphatic vessels where they develop into adult worms, thus continuing a cycle of transmission.
Lymphatic filariasis is transmitted by different types of mosquitoes, for example by the Culex mosquito, widespread across urban and semi-urban areas, Anopheles, mainly found in rural areas, and Aedes, mainly in endemic islands in the Pacific
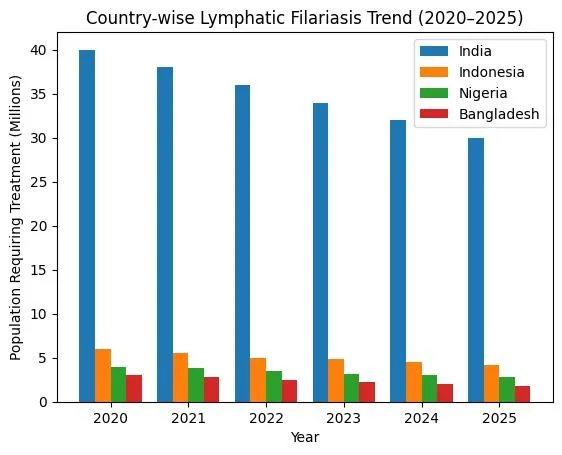
Global epidemiology of LF
Lymphatic filariasis (LF) affects approximately 120 million people across 72 countries globally [19]. In Southeast Asia and India alone, about 45.5 million people are infected [19]. LF is endemic in parts of Africa, Asia, the Pacific and the Americas, including Haiti, the Dominican Republic, Guyana, and Brazil [20].
The disease is mainly caused by Wuchereria bancrofti (widely distributed in tropical and subtropical regions) and Brugia malayi (primarily in South and Southeast Asia) [21–23]. Transmission occurs through mosquito vectors such as Anopheles, Culex, Aedes, and Mansonia species, which thrive in warm, humid climates [24].
LF is classified as a Neglected Tropical Disease (NTD) under the London Declaration (2012) [25]. Control strategies include Mass Drug Administration (MDA), vector control, improved sanitation, and community collaboration to eliminate LF as a public health problem [26–28].
Pathophysiology
Lymphatic Filarisis
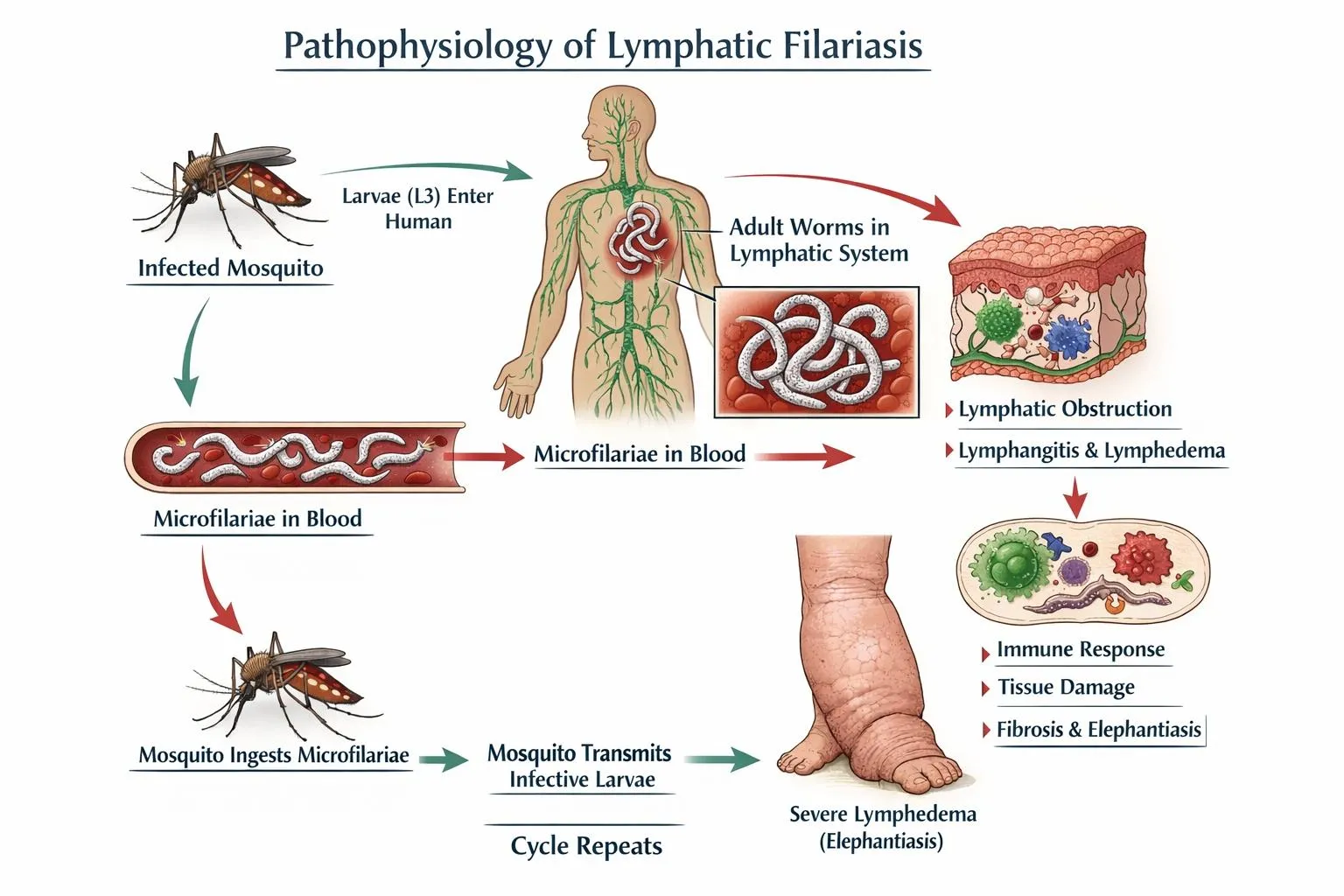
Humans are the only definitive hosts for Wuchereria bancrofti, while Brugia malayi and Brugia timori can also infect domestic and wild animals [29,30]. When an infected mosquito bites a human, it deposits third-stage larvae into the skin. These larvae migrate to the lymphatic system, mature into adults, and reproduce [31]. Female worms release microfilariae with nocturnal periodicity, which circulate in the blood [32]. A mosquito ingests the microfilariae during a subsequent blood meal. Inside the mosquito, microfilariae develop into infectious third-stage larvae, which are transmitted to another human during the mosquito's next feeding [33]. This cycle takes approximately 12 months, with adult worms living up to 15 years and producing microfilariae [34].
Life cycle of LF
The life cycle of lymphatic filariasis (LF) involves a complex interaction between humans and mosquito vectors, facilitating the transmission of the parasitic worms Wuchereria bancrofti, Brugia malayi, and Brugia timori [35,36]. The cycle begins when an infected mosquito bites a human and ingests microfilariae, the immature larvae, present in the person’s bloodstream [35]. These microfilariae are typically active during the night, aligning with the nocturnal feeding habits of mosquito species such as Anopheles, Culex, Aedes, and Mansonia [37].
Within the mosquito, the microfilariae migrate to the midgut, penetrate the midgut wall, and then move to the thoracic muscles, where they develop into first-stage (L1) and second-stage (L2) larvae. Over 10–14 days, these L2 larvae transform into third-stage larvae (L3), the infective form of the parasite, which then migrate to the mosquito’s proboscis [35,38]. When the mosquito bites another human, it deposits the L3 larvae onto the skin, where they enter the body through the bite wound and migrate to the lymphatic system [38].
Inside the lymphatic system, the larvae develop into fourth-stage larvae (L4) and eventually mature into adult worms over several months [35,39]. These adult worms, which can live for 6–8 years, reside in the lymphatic vessels and nodes, causing significant damage and leading to chronic conditions such as lymphedema and hydrocele [39,40]. The adult worms mate and produce thousands of microfilariae daily, which are released into the bloodstream and circulate during the night, ready to be ingested by another mosquito, thereby continuing the cycle [37,40].
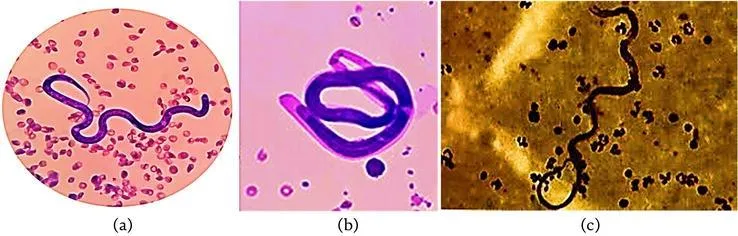
A. W. bancrofti B. B. malayi C. B. timori.
Figure 5. Worms known to cause lymphedema.
Clinical Manifestations of Lymphatic Filarisis
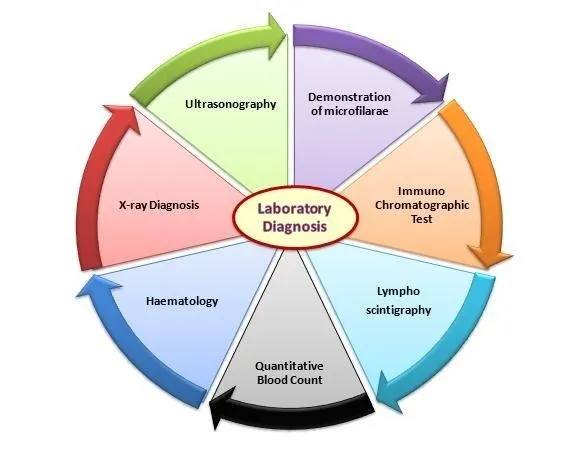
Diagnosis of Lymphatic Filarisis
TREATMENT OF LYMPHATIC FILARIASIS
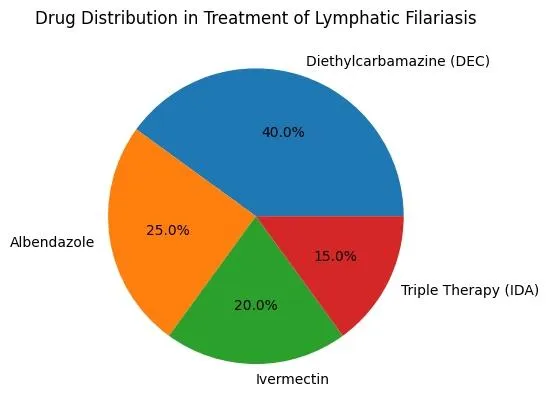
3. Management of Acute Attacks (ADLA)
|
Drug Name |
Dose |
Duration |
Route |
|
Diethylcarbamazine (DEC) |
6 mg/kg/day in 3 divided doses |
12 days |
Oral |
|
Albendazole |
400 mg single dose |
Single dose (with DEC) |
Oral |
|
Ivermectin |
150–200 mcg/kg single dose |
Single dose |
Oral |
|
DEC + Albendazole |
DEC 6 mg/kg + Albendazole 400 mg |
Single annual dose (MDA program) |
Oral |
Prevention And Control Of Lymphatic Filariasis
2. Vector Control (Mosquito Control)
3. Personal Protective Measures
4. Morbidity Management & Disability Prevention (MMDP)
Nationwide MDA Campaign for lymphatic Filarisis Elimination:
The second phase of the Bi-annual Nationwide Mass Drug Administration (MDA) campaign for Lymphatic Filariasis elimination has recently been launched. This phase targets 63 endemic districts in Bihar, Jharkhand, Karnataka, Odisha, Telangana, and Uttar Pradesh. It involves a door-to-door administration of preventive medications in these areas, pushing India closer to achieving its goal of eliminating Lymphatic Filariasis ahead of the global target.
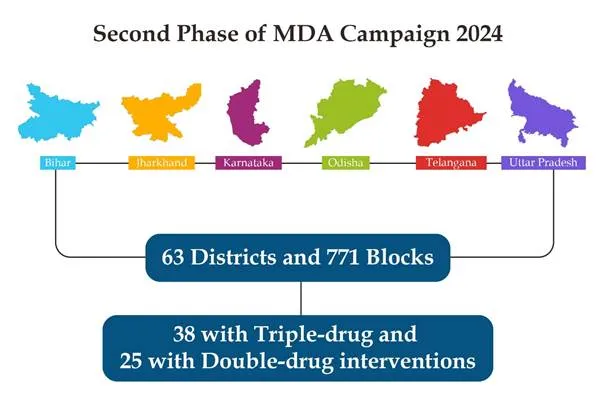
As part of the second phase of the MDA campaign, preventive measures are being implemented across 63 districts (comprising 38 triple-drug and 25 double-drug areas) and 771 blocks in 6 states.
This phase emphasizes not only the distribution of medications but also ensuring their consumption to maximize the campaign's effectiveness and achieve its goals.
Notably, the first phase of the Bi-annual MDA campaign 2024, which covered 96 districts across 11 states, achieved a national coverage rate of 95% of the eligible population.
MDA Campaign
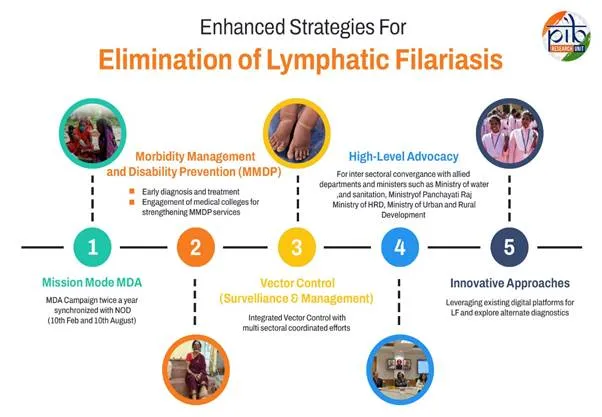
India's efforts to eliminate Lymphatic Filariasis (LF) have made substantial strides with the introduction of the Enhanced Strategy for LF Elimination by 2027. This strategy incorporates a mission-mode Annual Mass Drug Administration (MDA) campaign, held biannually on February 10 and August 10, alongside National Deworming Day (NDD).
India has implemented a comprehensive five-pronged strategy to combat LF, which includes Mission Mode Mass Drug Administration (MDA), Morbidity Management and Disability Prevention (MMDP), Vector Control (Surveillance and Management), High-Level Advocacy, and Innovative Approaches.
Significant Progress in MDA Campaign
LF Elimination by 2027: An ambitious target
I In 2023, India’s then Union Minister for Health and Family Welfare, Mansukh Mandaviya, stated that lymphatic filariasis (LF) is not a neglected disease in India but a priority disease targeted for elimination in a time-bound manner (41). The ministry committed to eliminating LF by 2027 through a nationwide Sarva Dawa Sevan (Mass Drug Administration, MDA) campaign, which is three years ahead of the global target set by the World Health Organization (42). During the launch of this initiative, the Additional Secretary and Mission Director (National Health Mission), Roli Singh, highlighted that despite 10–15 rounds of MDA in the past, LF elimination could not be achieved due to suboptimal coverage (43).
The 2027 elimination goal follows a series of missed and extended deadlines, with earlier national targets initially set for 2015 and later extended to 2017 (44,45). At the global level, WHO’s Global Programme to Eliminate Lymphatic Filariasis initially targeted elimination by 2020; however, ongoing challenges have led to a revised global timeline of 2030 (46).
The second phase of the bi-annual nationwide MDA campaign was launched in August, targeting 63 high-risk districts across six states, including Bihar, Jharkhand, Karnataka, Odisha, Telangana, and Uttar Pradesh (47). This included both triple-drug and double-drug districts covering a total of 771 blocks. According to the Ministry of Health and Family Welfare, MDA campaigns achieved 82% national coverage across 170 districts in 2023, while the first phase of 2024 reached a 95% coverage rate in 96 districts across 11 states (47).
Epidemiologically, at least 65% of the total population must receive preventive chemotherapy for effective control of LF. However, even when adult worms are eliminated, complications may persist due to the lack of a fully effective microfilaricidal or adulticidal drug. Ongoing studies are therefore focused on identifying adulticidal agents, which are crucial both for reducing transmission and alleviating disease symptoms in affected patients (46).
India’s familiar challenges and the way ahead
India has over 23 million patients suffering from lifelong disability as a result of lymphatic filariasis (LF) (48), and it inflicts an annual economic loss of about $1 billion in India (49). According to the World Health Organization, indirect losses due to diminished productivity act as a severe drain on local and national economies (50). Acute attacks are estimated to be responsible for losses of $60–85 million per year in India (50).
Earlier, a dedicated budget for filariasis control was not available, and limited human resources resulted in District Malaria Officers managing multiple responsibilities across rural and urban populations. Operational challenges, delayed funding, and interruptions in research activities were also reported, indicating systemic programmatic limitations (51). Previous national plans acknowledged that earlier control efforts had limited impact due to low commitment, implementation gaps, and operational constraints (51).
Experts have emphasized that adequate drug administration coverage and compliance are essential to achieve LF elimination targets. However, lack of awareness among communities regarding the importance of mass drug administration (MDA) leads to gaps in both distribution and consumption (52). Evidence suggests that successful implementation of MDA at the primary healthcare level depends on patient adherence as well as active involvement of healthcare workers in monitoring and motivation (52).
Furthermore, LF is often under-recognized due to its non-fatal nature, leading to low community-level urgency until advanced stages develop. Misconceptions regarding government-provided medication further affect compliance. Programmatic experiences highlight that improvements such as shifting from loose tablets to strip-packaged formulations helped enhance acceptance and adherence within communities (53).”

As part of a branding attempt, a logo and tagline have been developed for the national Filaria Eradication Campaign. The tagline reads “Safe drug, assurance for better health”.
REFERENCES


Rutuja Shete*, Sharmila Shah, Lymphatic Filariasis: Current Status, Pathogenesis, And Global Elimination Strategies, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 5417-5430. https://doi.org/10.5281/zenodo.20774173
 10.5281/zenodo.20774173
10.5281/zenodo.20774173