
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
SVB’s College of Pharmacy, Dombivli (E), Maharashtra 421204.
This review uniquely integrates formulation science, stakeholder perspectives, and market analysis. The non-adherence of young people to medications for diabetes is a problem that continues to be of great concern. The primary reasons young people do not take their medications for diabetes are related to how they are made, including: poor taste; large tablets; and difficulty swallowing medications. Even when pediatric patients are prescribed Metformin — which is the most commonly prescribed medication for youth with type 2 diabetes mellitus ? they frequently do not take the medication because of the bitter taste and the high dosage of Metformin required to achieve therapeutic benefit. In addition, it is estimated that between 31 and 94 people per 100,000 pediatric patients annually have recently been diagnosed with type 2 diabetes worldwide. Furthermore, 8-12% of adolescents in urban India are considered obese, thereby increasing the prevalence of type 2 diabetes drug use within the pediatric population. The worldwide market for Metformin is expected to grow at an annual compound rate of 5-7% and the market for diabetes medications is rapidly expanding, so it is a small and highly specialized area of the market. Therefore, Metformin lozenges differ from the currently available Metformin because they target non-therapeutic uses (i.e. enhance the therapeutic value of Metformin by changing its formulation).
Patient-centric dosage forms like lozenges aim to tackle key adherence issues associated with traditional oral antidiabetic therapy (1,2). These include unpleasant taste and difficulty swallowing (1,2). Diabetes mellitus is a long-lasting metabolic disorder marked by high blood sugar levels caused by poor insulin secretion, insulin action, or both (3). Type 1 diabetes mainly affects younger children, while the rise of type 2 diabetes in adolescents has increased the use of oral antidiabetic agents in pediatric care (4). Worldwide, the incidence of pediatric type 2 diabetes is between 31 and 94 cases per 100,000 each year (5). Prevalence can reach 5,300 cases per 100,000 in high-risk groups (5,6). In India, adolescent obesity rates are between 8 and 12% in urban areas (7).
Metformin hydrochloride, a biguanide, is the recommended first-line treatment for type 2 diabetes. It remains widely prescribed due to its proven effectiveness, safety, and low cost (8,9). However, its clinical use often faces limitations due to poor taste and large tablet size (10,11). These factors can make swallowing difficult, leading to lower patient compliance, especially among younger individuals (1,10). Evidence from the TODAY trial indicates that only about 50% of youth maintained good blood sugar control on metformin alone after four years (12). This highlights the challenges of adherence. Caregivers often resort to splitting or crushing tablets, which can affect dosing accuracy and treatment results (13).At the same time, the global market for metformin is expected to grow at about 5 to 7% annually (14). Pediatric diabetes treatments are also seeing rapid growth, underlining their commercial importance (5). Lozenges and orally disintegrating tablets provide practical benefits by dissolving in the mouth without needing water (15,16). They make administration easier and can mask bitterness with sweetened and flavored bases (10,15). Together, these aspects position taste-masked metformin lozenges as a formulation-level approach to improve acceptance and adherence among certain pediatric and adolescent groups. They complement existing solid oral therapies instead of replacing them.
Medication adherence in children poses a unique clinical challenge, especially for chronic metabolic conditions like Type 2 Diabetes Mellitus (T2DM), where ongoing long-term therapy is crucial for maintaining blood sugar levels (17). Pediatric T2D is more aggressive than adult cases, showing rapid decline in β-cells and early onset of microvascular complications (18). This emphasizes the need for consistent adherence. Current treatment guidelines suggest metformin as the first-choice medication for youth aged 10 and older with stable blood sugar levels, typically alongside lifestyle changes (8). Despite its proven effectiveness and low cost, metformin hydrochloride has formulation-related issues. Its strong bitterness and large tablet size often lead to refusal or difficulty swallowing, which creates a challenge for adherence (10,17). Evidence from the TODAY trial showed that about 50% of youth could not maintain stable blood sugar levels on metformin alone after four years, indicating the shortcomings of current formulations (12). Registry data from the Pediatric Diabetes Consortium further indicates that lower HbA1c at diagnosis leads to better outcomes and highlights the need for early and consistent adherence (19). Developmental changes add to these challenges; younger children prefer liquids while teenagers like portable solid forms (1). When available products do not match their developmental needs, caregivers often make unprescribed adjustments, such as crushing or splitting tablets. This happens in 30 to 40% of cases and can lead to dosing errors and reduced effectiveness (13,21). Addressing these issues through patient-focused design, like taste-masked lozenges, can improve acceptability, reduce improvised administration methods, and ensure safe and effective medication delivery for children.
In the area of pharmaceuticals there is no such thing as a single best method for masking the taste of an active pharmaceutical ingredient (10). For those active pharmaceutical ingredients that are high in solubility and have a bitter taste at therapeutic doses can be very challenging to develop paediatric oral formulations (10,23). An excellent example of this would be Metformin hydrochloride. Due to its bitter taste and large doses sometimes required to achieve therapeutic levels (500–2000 mg/day) children sometimes refuse to take it or vomit it back after ingestion (10,23). Simple additives, such as sweeteners or flavouring agents, typically are not sufficient to mask the taste of very bitter ingredients (10). Hence, the use of more sophisticated technologies that will delay the rate at which Metformin dissolves in the mouth. The physicochemical properties of metformin, along with the interaction between drug and excipient, dictate the effectiveness of multiple strategies used to mask the taste of metformin formulations. The solubility of metformin hydrochloride is very high due to its interaction with bitter receptors on the tongue. Therefore, the rapidly dissolving metformin in saliva introduces it very quickly to the taste receptors, resulting in poor palatability.
Various taste masking techniques, such as micro-encapsulation, ion-exchange resins, and cyclodextrin inclusion complexes, reduce the amount of free drug available in the oral cavity. Microencapsulation provides a polymeric coating that slows the dissolution of metformin in saliva and permits its eventual release from the coating in the stomach. Ion-exchange resins create reversible complexes with metformin and remain stable at neutral pH but dissociate at low pH, so they can release metformin. Cyclodextrins can limit the interaction of metformin with taste receptors and, therefore, enhance palatability by forming inclusion complexes.
The slow dissolution of lozenges will assist in the control of how metformin is released and will help improve the masking effect of the taste. However, the above-mentioned strategies do not have a substantial impact on the pharmacokinetics of metformin because metformin is absorbed primarily in the small intestine and not through the buccal mucosa.Microencapsulating a drug using a polymer coating achieves a very good taste mask, but costs to manufacture are significantly higher than for other methods mentioned (10,24). Ion-exchange resin formulation will produce a taste-masking drug-resin complex but with limitations in drug-loading. Cyclodextrins do improve solubility and taste, and they also must be justified as safe excipients (25,26). Clinical studies demonstrate that liquid preparations of metformin are more acceptable than crushed tablets, further demonstrating the need to produce taste-masked formulations to assist with adherence (27). Lozenges present their own unique considerations regarding practicality; their drug-loading capacity (~200–400 mg/unit) provides little flexibility with dosing (15). As a result of this, sugar-free, non-cariogenic bases must be used for all excipients in compliance with EMA/FDA requirements for safety with children (29). Lozenges are easier to carry than liquids and have greater stability than tablets; from the standpoint of palatability and swallowability, may offer advantages in specific pediatric subgroups (15). Furthermore, there are specific manufacturing techniques available that would enable cost-effective methods to produce lozenges on a large scale compared to lyophilization methods (30).
Caregivers often struggle to give oral medications to children (31). To help with swallowing, many use unapproved methods like splitting or crushing tablets (13,21). Research shows that bad taste, especially bitterness, is a major reason children refuse or do not finish their treatment (2,31). Young children naturally prefer sweet flavors and often reject bitter medicines (2). More than half of kids under six have trouble swallowing standard oral medications (31).
Preferences for medication forms change as children grow. Studies suggest that liquid medicines are most popular among younger kids (around 1 to 6 years old), but this preference decreases sharply in teenagers, who generally prefer solid forms (1,31). Parents also show a strong interest in medications that dissolve quickly in the mouth, like orally disintegrating tablets, because they reduce the risk of choking (15,31). Flavored lozenges are usually well accepted by school-aged children and are seen as easier and more pleasant to take (15,31).
For chronic conditions like diabetes, children often dislike metformin due to its bitter taste and large tablet size (10,17). These findings point to the need for more child-friendly medication forms, with taste-masked lozenges potentially offering a simpler and more acceptable option for some pediatric patients.
To show how consumer preferences affect pediatric medication design, the following chart summarizes trends in caregiver and patient preferences for common oral formulations (31). The distribution reflects the relative acceptability reported across various pediatric adherence and acceptability studies, rather than primary survey data (31). This overview emphasizes how ease of administration and pleasant taste influence formulation choices in real-world pediatric care.
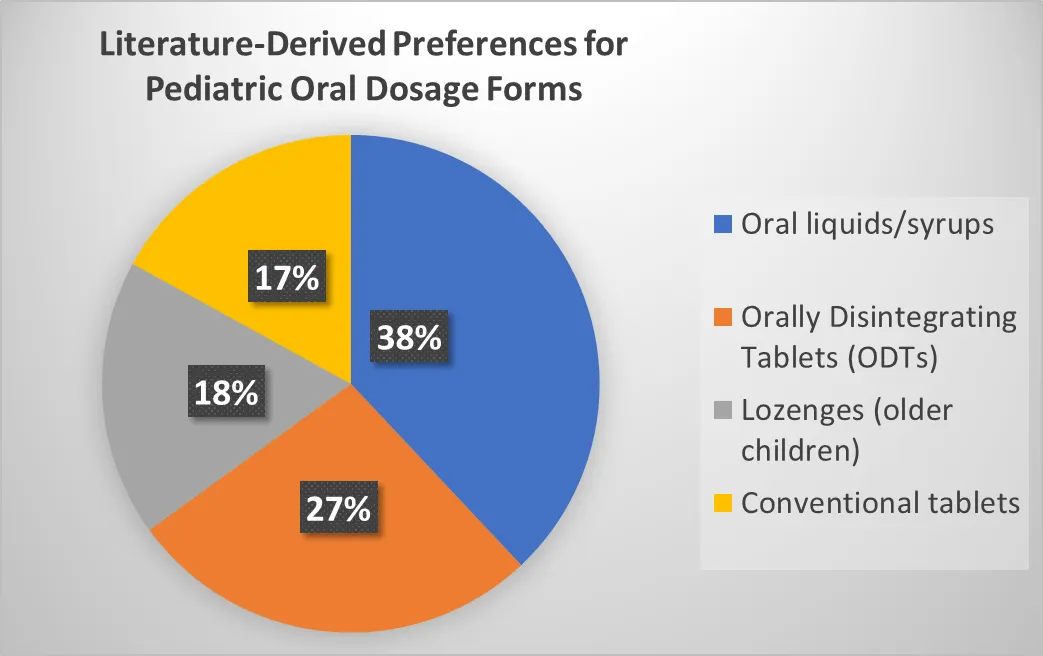
Fig 1. Reported pediatric dosage-form preferences across age groups, synthesized from secondary literature sources (31). Percentages represent values extracted from independent published studies and are presented for illustrative comparison rather than statistical aggregation (1,10,15,17,31).
While the preceding chart outlines literature-derived preferences for pediatric oral dosage forms, preference alone doesn't fully explain why some formulations are favored in practice. To provide more context, the following graph highlights the practical challenges caregivers report when giving oral medications to children (31). Together, these figures show how formulation preferences are shaped by everyday administration difficulties, linking consumer choice with real-world usability issues.
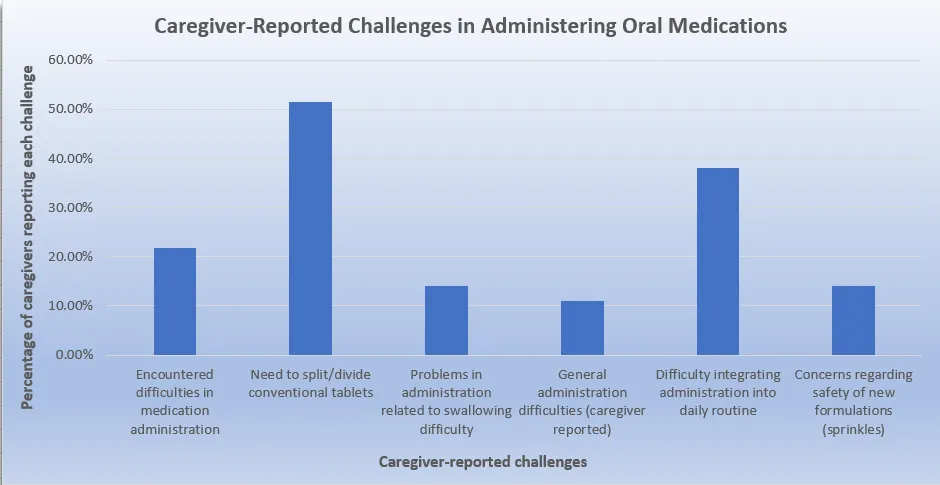
Figure 2. Caregiver-reported challenges in administering oral medicines to pediatric patients, aggregated from independent published studies and shown for comparative, non-inferential purposes.(1,2,10,17,31)
The challenges caregivers face, as shown above, highlight the barriers encountered when administering pediatric medications. Issues like taste aversion, swallowing difficulty, and the need for tablet adjustments are major concerns (2,13,31). These challenges increase the burden on caregivers and directly impact the acceptability of different oral dosage forms among various pediatric age groups. To illustrate how these administration difficulties affect formulation preferences, the following figure examines the acceptability rankings of oral dosage forms among older pediatric populations, where developmental ability allows for more flexibility in medication choice (31).
Effective management of pediatric diabetes requires not just effective medication but also agreement among patients, caregivers, and healthcare professionals on how acceptable the treatment is (31,32). These three groups have distinct but connected roles in determining adherence and long-term results.
Pediatric patients are the main users, and their physical and emotional sensitivities greatly impact treatment success (2,31). Children are very sensitive to bitter tastes, and the taste of metformin often leads to refusal, spitting, or vomiting (10,17). Research shows that over 50% of children under 12 struggle to swallow or accept bitter oral medications, and even one bad experience can cause long-term resistance (31,32). In contrast, adolescents prefer discreet solid forms of medication that fit their social and developmental needs (1,31). Lozenges and orally disintegrating tablets (ODTs) directly meet these preferences by hiding bitterness and easing the anxiety of swallowing (15,22).
Caregivers serve as caregivers for daily dosing. When medications are not made for children, caregivers often crush tablets or mix them with food, a practice seen in 40% of pediatric prescriptions for solid oral medications (13,21). These adjustments can lead to dosing errors and changes in how the body processes the drugs, especially with extended-release products (21). Surveys show that 60–70% of parents regularly face challenges in giving bitter medicines, highlighting the need for formats that are easy to administer, provide consistent dosing, and are convenient to carry (31,32). Lozenges dissolve slowly and offer familiar taste experiences, which help lessen daily conflicts and reduce the burden on caregivers (15).
Healthcare professionals stress that adherence is key to controlling blood sugar levels, noting that poor compliance causes 30–40% of the suboptimal outcomes in pediatric diabetes (32,33). Doctors worry about patients stopping medication because of bad taste or gastrointestinal issues, while pharmacists point out problems with dosing errors and counseling challenges related to liquid forms (31,33). Regulatory bodies like the EMA and FDA are increasingly backing age-appropriate solid forms that enhance dosing accuracy and lessen caregiver manipulation (29). From an industry point of view, the demand for tasty, patient-friendly formats presents a chance for differentiation in a crowded metformin market (14).
By bringing together the views of patients, caregivers, and healthcare professionals, taste-masked lozenges stand out not as a new therapy but as a formulation innovation aimed at addressing stakeholder priorities. This agreement enhances both clinical adherence and commercial viability.
While the preceding discussion highlights the qualitative perspectives of key stakeholders involved in pediatric medication use, these viewpoints differ in the specific attributes they prioritize during treatment decision-making. To synthesize these stakeholder-specific concerns in a comparative manner, the following stacked bar chart summarizes the relative importance of palatability, ease of administration, adherence outcomes, and dosing accuracy across patients, caregivers, clinicians, and pharmacists. This visualization provides an integrated overview of how formulation acceptability is shaped by multiple, sometimes competing, stakeholder priorities
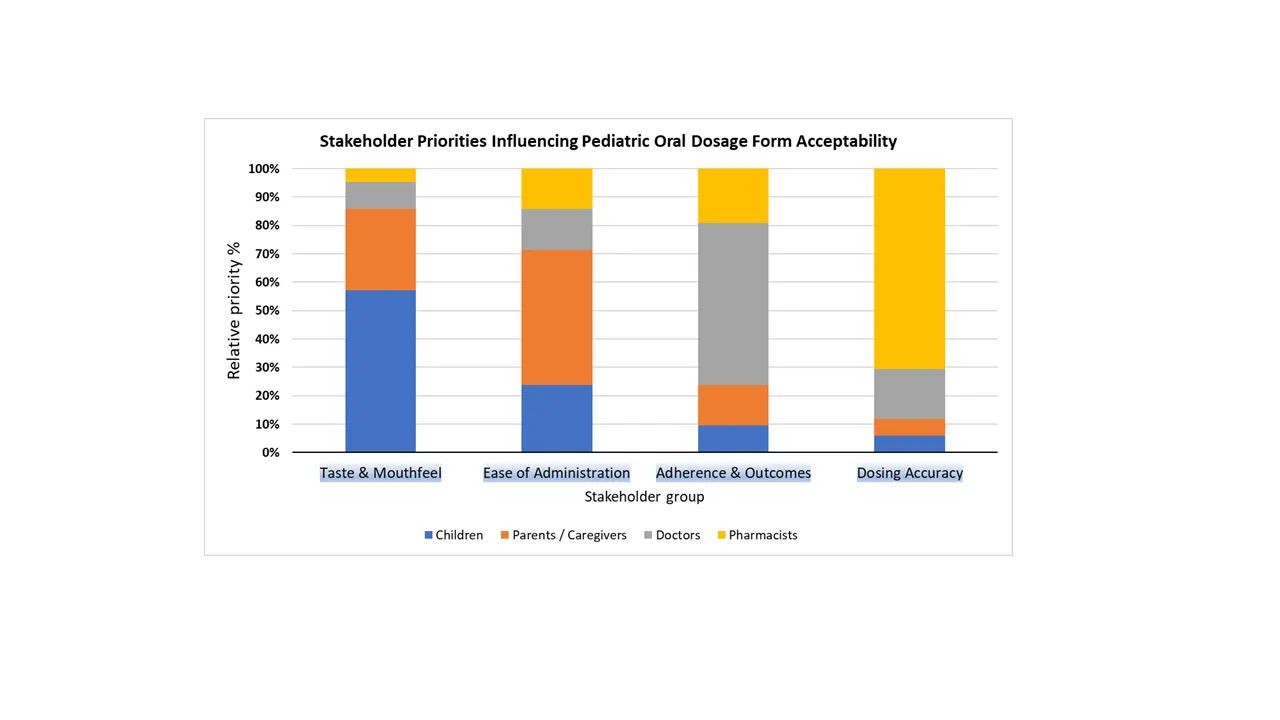
Figure 3. summarizes stakeholder-specific priorities influencing pediatric oral dosage form selection, highlighting differences in emphasis on palatability, ease of administration, adherence outcomes, and dosing accuracy across patients, caregivers, clinicians, and pharmacists.
Taken together, the stakeholder analysis reveals that formulation design must reconcile multiple, and sometimes competing, priorities across the pediatric medication ecosystem. Patient-centric solid oral dosage forms represent an approach that can align these priorities without altering established treatment pathways(14,22,28,31,32,33).
Currently, when it comes to pediatric Metformin therapy there are 2 main formulations available liquid solutions and extended release tablets (20,31). The characteristics of each formulation relate directly to how well each can be used in treating youths acceptability of treatment and adherence to the treatment plan (31,33). Liquid formulations provide significant benefit for dosing flexibility (i.e., weight-adjusted dosing form of liquid solutions) (20,31). This is especially beneficial for young children; plus, liquid solutions are generally easier to swallow than tablets and provide more opportunity for caregivers to accurately dose their child (20,31). Yet, difficulties with poor taste, instability depending on storage conditions, and caregiver-administered precision dosing can negatively impact liquid Metformin products as viable alternatives to solid dosage forms (27,31). Additionally, access to standardized liquid formulations across the Country is inconsistent (27).
On the other hand, Extended-Release (XR) formulations provide improved gastrointestinal tolerability and reduced frequency of dosing; which should, in theory, promote adherence in adolescents (9,33). Alternatively, XR tablets may present less opportunity for modification of the tablet size; (i.e., crushing or splitting XR tablets can eliminate their controlled-release properties) (13,21). Because of their characteristics and due to the associated costs of XR products vs. immediate-release generic products, XR tablets restrict the ability to provide custom dosing solutions for pediatric patients (14,36).
In addition to these established formulations, taste-masked lozenges are being explored as a patient-centric alternativeTaste-masked lozenges may occupy a niche position for some patients rather than being considered an alternative for all patients receiving Metformin. By producing a Metformin product that takes into account palatibility and ease of administration without the use of a caregiver to dose, taste-masked lozenges can provide benefits to certain children and adolescents (30). Therefore, the role of lozenges can be considered a supplemental dose to an already large offering of alternative forms of Metformin to address various adherence barriers for different pediatric patients.
Metformin lozenges are a new, patient-focused dosage form created to overcome limitations seen in typical pediatric options (1,31). Traditional liquid suspensions are often preferred for young children, but they usually have bad taste, caregivers may struggle with accurate dosing, and they don't hold up well in hot or humid conditions (1,31). Solid tablets are cheap and easy to find, but their large size and strong bitterness can lead to refusal, spitting, or vomiting in younger patients (10,31). Orally disintegrating tablets (ODTs) are easier to swallow, but they are fragile, absorb moisture, and need special packaging, which raises manufacturing and distribution costs (15,30). Extended-release tablets offer convenient dosing and better gastrointestinal tolerance, but they cannot be easily adjusted for children because crushing or splitting them disrupts their controlled-release properties (13,21).
In this context, lozenges provide a flavored, slowly dissolving dose that improves taste masking and is easy to take without water (10,28). They are portable and stable, making them better options than liquids or ODTs (15). Their fixed doses also reduce the chance of caregiver errors compared to syrups (31). By avoiding the need for tablet adjustments, lozenges lower the risks of dosing errors and changes in how the body processes the medication, which can happen when caregivers try to modify doses (21). Gradual dissolution in the oral cavity may provide a more controlled drug presentation compared to immediate swallowing of conventional tablets; however, this does not substitute for true pharmacokinetically validated prolonged-release formulations (10). Importantly, lozenges appeal to teenagers who prefer discreet, portable solid forms, helping them stick with therapy during a vital developmental period (1,31).
However, there are limitations that affect their widespread use. Lozenges can only hold about 200–400 mg of the drug per unit (15). This means patients may need multiple strengths or face a higher pill burden to get the full therapeutic dose. Keeping the lozenge in the mouth for a long time requires strong taste-masking methods and sugar-free ingredients to prevent dental or mouth issues (10,29). Cost is also a significant factor; while generic metformin tablets are cheap, lozenges require more complex formulation techniques and specific excipients, raising production costs (10,30). product analysis shows that metformin lozenges are not intended to be a universal replacement. Instead, they offer a unique, patient-centered alternative within the broader metformin market (14). Their value lies in improving acceptability and adherence for certain pediatric and adolescent groups, supporting existing therapies while tackling issues related to formulations.
Beyond Formulation feasibility, commercial viability is essential so in depth market analysis about the product provides us with following Market insights. India presents a specific market opportunity for patient-focused metformin dosage forms in managing diabetes for children and adolescents (5,7). The global metformin market was valued at several billion USD in 2024 and is expected to grow at about 5 to 7 percent per year through 2030 (14,37). The pediatric diabetes treatment segment is growing faster due to increasing childhood obesity and more recognized cases of type 2 diabetes among young people (5,6). In India, the number of adolescents exceeds 240 million, with urban obesity rates between 8 and 12 percent, along with a rising awareness of youth-onset type 2 diabetes (7,38). Reviews show that prediabetes and metabolic issues are common among younger individuals, leading to a growing group of adolescents who might need metformin (38). Clinical studies confirm that metformin is the standard first-line treatment, but patients often struggle with its taste and the difficulty of swallowing pills (8,10). Caregivers sometimes crush or split tablets, which happens in 30 to 40 percent of cases (13,21). This practice can lead to dosing errors, highlighting the need for more patient-friendly formats.
Key players in India include major generic manufacturers like Sun Pharma, Cipla, Dr. Reddy’s, and Lupin, along with global contract development and manufacturing organizations experienced in pediatric formulations (36). The opportunity lies not in simply increasing metformin use but in creating unique formulations in a crowded market (14). The focus narrows from the total number of adolescents with diabetes to those who could take metformin, can handle solid dosage forms, and have caregivers looking for better-tasting options (31). Even a small shift of 5 to 10 percent of pediatric prescriptions towards taste-masked lozenges could bring in additional revenue of INR 20 million to 400 million each year, with the potential to break even in 3 to 5 years (37). This makes lozenges a niche but potentially profitable innovation within India’s large metformin market.
To translate the above market opportunity logic into a structured visual framework, the following
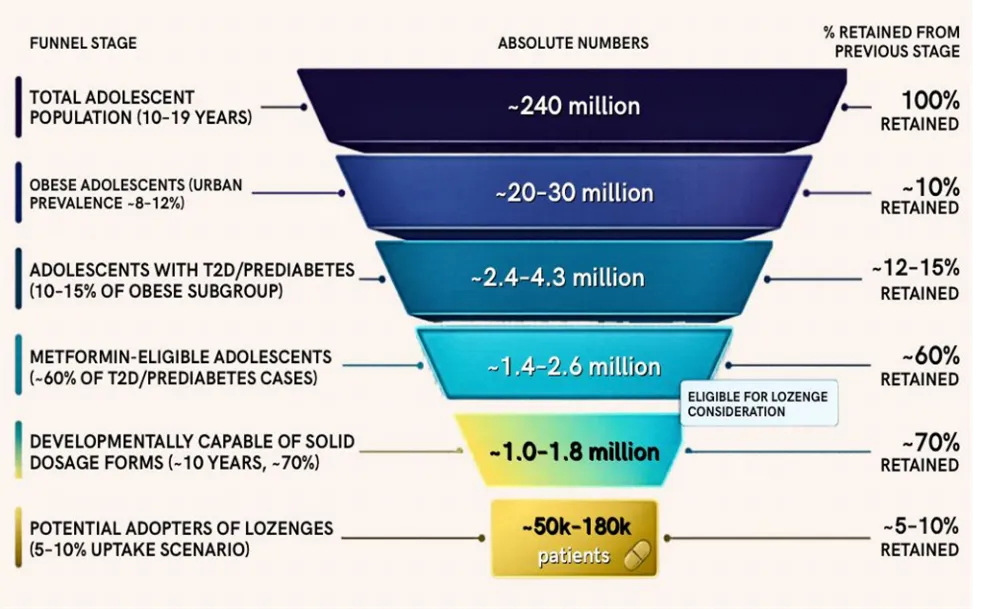
Figure 4. Conceptual market opportunity funnel illustrating progressive narrowing of the pediatric and adolescent population in India eligible for patient-centric metformin dosage forms, based on epidemiological prevalence, clinical eligibility, developmental readiness, and formulation acceptability trends reported in the literature.
“Values represent relative proportions derived from published literature and are intended to illustrate market narrowing rather than quantify absolute population size.”
The funnel diagram conceptually illustrates the progressive narrowing of the addressable market for patient-centric metformin dosage forms in India. The funnel reflects sequential filtering based on epidemiological prevalence, clinical eligibility for oral metformin therapy, developmental readiness for solid oral dosage forms, and formulation acceptability considerations. This visualization is intended to clarify how a large underlying disease burden converges into a focused, formulation-relevant niche rather than a mass-market opportunity.
The Indian market presents a focused but relevant opportunity for patient-centric metformin dosage forms in pediatric and adolescent populations. While metformin itself is well established and widely prescribed, formulation-level differentiation offers scope to address unmet needs related to acceptability and long-term adherence. This opportunity is inherently niche, shaped by clinical eligibility, developmental readiness, and caregiver-driven administration practices.
The introduction of new oral drug formulations for children poses significant regulatory, technical, and economic challenges (35,36). Agencies like the European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) set strict standards for pediatric drug development (29,39). They stress that acceptability, which includes palatability, swallowability, mouthfeel, and dosing flexibility, is as important as pharmacological effectiveness for ensuring compliance (31,39). EMA guidance discourages caregivers from splitting or crushing tablets, as this can change how the drug works in the body. It also sets size limits for pediatric tablets, specifying that they should be less than 5 mm for children under six to ensure safe swallowing (29). The FDA requires sponsors to submit an Initial Pediatric Study Plan (iPSP), which must detail pediatric-specific formulations under development, including considerations for size, swallowability, palatability, and stability. If a formulation fails, sponsors have to document their efforts and reasons, which can lead to partial waivers but also increase the administrative burden (39).
In India, the Central Drugs Standard Control Organization (CDSCO) is increasingly following the frameworks of the EMA and FDA. It now requires risk-based evaluation of excipients and pediatric-specific dossiers (40). Excipient safety is a major concern, especially for neonates with developing metabolic systems (26,40). EMA guidelines call for a full justification of excipient choices (29). Databases like STEP (Safety and Toxicity of Excipients in Pediatrics) have been created to help with risk assessments (41). Regulatory authorities emphasize that justifications for excipients, such as artificial sweeteners, polymers, and flavoring agents, must be provided for long-term pediatric use, adding complexity and cost to development programs (29,40).
Case studies highlight these challenges. Liquid metformin formulations have been approved and shown to be more acceptable than crushed tablets, but their availability is still limited in many areas (27). Orally disintegrating tablets (ODTs) have been developed to improve swallowability, but they are fragile, absorb moisture easily, and need special packaging, which raise production costs (15,30). Extended-release metformin products, like Glumetza® and Fortamet®, show that advanced release mechanisms can improve dosing convenience, but they come at a significantly higher cost than immediate-release generics (36). New technologies like 3D printing provide customization for ODTs but are limited by high production costs and slower output compared to traditional methods (42).
The lack of standardized international methods for testing acceptability continues to create inefficiencies (31). Industry and academic groups use various sporadic approaches. A clear evidence roadmap for taste-masked metformin lozenges would include: (a) palatability and acceptability trials using validated scales in pediatric groups; (b) bioequivalence studies with standard metformin tablets to confirm effectiveness; (c) excipient safety justifications following STEP and CDSCO guidelines; and (d) validation of stability and packaging to ensure mechanical integrity and shelf life (29,41). Balancing patient acceptability, safety, and cost is crucial for creating desirable pediatric dosage forms (35). If optimized for sensory properties, excipient safety, and manufacturing costs, taste-masked lozenges could represent an innovative option within the established metformin market. They would meet regulatory expectations while addressing the needs of patients.
The evaluation of taste-masked metformin lozenges shows how clinical needs, stakeholder views, regulations, and market conditions overlap in developing drugs for children (31,35). Adherence is crucial for managing youth-onset type 2 diabetes (33). However, current formulations often do not meet the needs of young patients (1,31). Lozenges provide a patient-centered option by enhancing taste, making them easier to carry, and ensuring accurate dosing (10,28). These features suit teenagers who prefer discreet solid forms . They could reduce the need for caregivers to help with dosing, which may improve therapy compliance (1,31). Still, challenges remain due to drug-loading limits and safety requirements for ingredients (15,29).
From the viewpoint of stakeholders, children focus on taste and ease of swallowing, caregivers want convenience and reliable dosing, and doctors stress the importance of long-term adherence (31,32). Formulation design must consider these views for practical use. Regulatory bodies like the EMA, FDA, and CDSCO increasingly stress the need for testing acceptability and justifying ingredient use (29,39,40). Yet, the lack of unified methods for assessing taste continues to slow down development. Market analysis shows lozenges could be a unique innovation within India’s established metformin market, where focusing on patient-friendly design might provide some valuable business opportunities (31,14).
We must recognize the limitations of current evidence. Most data on pediatric acceptability come from small studies or from adult formulations (31). There is a lack of strong clinical trials that specifically assess lozenges. Long-term outcomes concerning adherence, cost-effectiveness studies, and real-world application studies are essential research focuses (33). Without this evidence, claims of better adherence and outcomes are mainly theoretical rather than backed by solid research.
Despite their potential to improve acceptance and ease of use, metformin lozenges have several limitations that might restrict their use in managing diabetes in children. These challenges fall into three categories: formulation, clinical, and economic.
Formulation issues mainly arise from metformin’s high dosage needs (500–2000 mg/day) and strong bitterness (10,22). Lozenges can only hold a limited amount of the drug per unit (about 200–400 mg), making it hard to include enough medicine without losing strength, masking taste, or causing discomfort . As mentioned in the formulation science section, improved taste-masking methods like microencapsulation or ion-exchange resins may lessen bitterness (24,25,28). However, partial masking may still allow children to experience unpleasant flavors during lozenge dissolution. Additionally, prolonged contact in the mouth can create concerns about dental health, irritation, and the requirement for sugar-free ingredients, which complicates formulation and increases cost (29).
Clinical issues include less flexibility in dosing compared to liquids that allow for adjustments based on weight (1,31). Fixed-dose lozenges might need different strengths, adding complexity to manufacturing and inventory. Variability in drug absorption also poses a problem: metformin is not intended for absorption through the mucous membranes, and differences in children's sucking behavior, how long they dissolve the lozenge, and swallowing habits could lead to inconsistent drug release (9,22). Younger children may also face safety risks like choking or misunderstandings about how to use the lozenge, limiting their use to older kids (31).
Economic and market challenges stem from the widespread availability of low-cost generic metformin tablets. Creating taste-masked lozenges involves specific ingredients, advanced manufacturing processes, and possibly more complex packaging to ensure stability (14,22,30). These factors can raise production costs, making it harder to adopt them in cost-sensitive healthcare systems unless adherence advantages are clearly demonstrated through clinical studies . Comparing them to extended-release metformin and orally disintegrating tablets shows that patient-focused innovations often come with higher costs, raising concerns about affordability and scalability.
CONCLUSION
This review integrates formulation science, stakeholder perspectives, caregiver experiences, regulatory context, and market framing to evaluate the potential role of taste‑masked metformin lozenges in pediatric diabetes management. Across the literature, a consistent theme emerges: medication acceptability—particularly palatability and ease of administration—plays a central role in long‑term adherence among children and adolescents. Stakeholder analysis highlights how children prioritize taste and comfort, caregivers seek convenience and dosing accuracy, and clinicians emphasize sustained adherence. Within India’s large but mature metformin market, lozenges represent a niche but strategically important innovation, positioned not to replace existing therapies but to enhance acceptability and persistence in selected pediatric segments. Their clinical and commercial relevance lies in formulation‑level differentiation, aligning with the broader shift toward patient‑centric pharmaceutical design.
FUTURE DIRECTIONS
Future development of taste‑masked metformin lozenges should prioritize robust palatability trials and standardized acceptability assessments in pediatric cohorts, integrating both child‑reported outcomes and caregiver perspectives to generate reproducible evidence. Long‑term adherence studies and cost‑effectiveness analyses will be essential to demonstrate that improved acceptability translates into measurable clinical and economic benefits. On the regulatory front, early alignment with EMA, FDA, and CDSCO pediatric guidance is critical, particularly in relation to excipient safety, dosage‑form suitability, and justification of acceptability claims. Beyond regulatory science, opportunities exist for public‑private partnerships in India, where generics manufacturers, CDMOs, and academic institutions could collaborate to accelerate formulation development and scale‑up. Digital health tools may also play a complementary role by supporting caregiver education, monitoring adherence, and collecting real‑world data to inform iterative product refinement. From a market perspective, positioning lozenges as complementary, patient‑centric alternatives within established diabetes care pathways will enable individualized treatment approaches while maintaining therapeutic continuity. Collectively, these directions highlight how technical feasibility, regulatory compliance, and stakeholder engagement must converge to realize the potential of lozenges as a niche but impactful innovation in pediatric diabetes management.
REFERENCES

Nandini Banerjee, Aditya Gawde, Lavanya Gone, Market Potential and Consumer Acceptance of Taste-Masked Metformin Lozenges for Diabetes Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1831-1844, https://doi.org/10.5281/zenodo.20591387
 10.5281/zenodo.20591387
10.5281/zenodo.20591387