
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 Research Scholar, Department of Pharmacy, Shri JJT University, Jhunjhunu, Rajasthan, India
2Research Guide, Department of Pharmacy, Shri JJT University, Jhunjhunu, Rajasthan, India
Oral absorption of drugs is severely affected by the physiologic barrier posed by the gastrointestinal (GI) tract, wherein only less than 10% of orally delivered drugs reach the colon as a result of degradation in the upper regions of the GI tract. The purpose of this systematic review is to analyse the emerging concept of developing microparticle-based drug delivery systems, particularly for the targeted delivery of an antimicrobial drug: cefixime, a poorly absorbed third generation cephalosporin used to treat lower gastrointestinal infections. Specifically, this review will evaluate advancements in designing micromotus tablets used for the targeted delivery of this antimicrobial agent.This review will examine numerous aspects of microparticle design, including the various methods of propulsion (chemical, magnetic, acoustic, and biohybrid), production methodologies during manufacture, and novel aspects regarding the dynamics of drug release, mucoadhesive properties, and effectiveness of propulsion and biodistribution will be included.Special attention will be given to developing a dual-response formulation design that includes magnetic Janus micromotors enteric coated with magnesium.Finally, considerations associated with micrometer-based therapeutics include biocompatibility issues, mass production obstacles, regulatory consideration, and potential future developments relative to micromotor-based delivery systems for antimicrobials.
Until recently, the primary means of medication utilization has been through the oral route (typically via pills), as it is considered to be less painful and more suitable (i.e., non-invasive, easy, and preferred over injections) than other drug administration methods.4 Nevertheless, the gastrointestinal tract ("GI tract") is not simply a place for ingested substances to move through; in point of fact, the GI tract takes active action against the introduction of foreign materials. Some of the challenges that the GI tract presents in regard to the bioavailability/bioactivity of medications include significant variations in the pH (compared to that of the blood), graduated dilution through saliva and other bodily fluids, enzymatic breakdown of the ingested substances (using both pepsin in the stomach and trypsin in the intestines), and mucosal tissues trapping material prior to reaching epithelial surfaces, all of which contribute to the likely fate of some medications once they have been administered enterally.1 Numerous studies have provided evidence suggesting that significantly lower percentages of newly developed medications will survive to market than originally anticipated (i.e., nearly a total of 70% of drug molecules will never progress beyond Phase I of clinical studies due to inadequate bioavailability after oral administration).
During this time, we expect the number of drugs that will either be developed for colon delivery or will require to reach colon (i.e., to treat infectious diseases) and GI tract (occurring within the tract) will increase. For those that are intended for colon delivery, by using the current development process, less than 10% of the administered doses will reach the target site of action.3 In recent years, lipid-based nanoparticle systems have minimally improved upon this situation, via providing some stability enhancement for the drug; however, they remain dependent upon passive diffusion, a slow, inefficient process. Most of these nanoparticle systems are encapsulated by the mucus layer and over 98% of the delivered drug never reaches its target tissue.5 Despite extensive efforts, the major problem still exists: getting the drug to the location of action. Micro/nanomotors (MNMs) are able to solve this problem.These tiny devices – some as small as a few hundred nanometers, others up to hundreds of microns – can move on their own. They convert chemical energy or external fields into motion.⁶ Over the past decade, researchers have shown that MNMs can swim through mucus, stick to tissues, and release their payload right where it is needed.⁷ Table 1 provides an overview of the four main propulsion mechanisms with their advantages and limitations.
In this review, we focus on one specific application: using micromotors in oral tablets to deliver cefixime to the colon. Cefixime is a third‑generation cephalosporin that is highly effective against Gram‑negative bacteria.⁸ But its oral bioavailability is only about 40–50% because it is a BCS Class IV drug – low solubility and low permeability.⁹ That means a lot of the antibiotic gets absorbed in the upper intestine, and not enough reaches the lower GI tract. A micromotor‑assisted tablet could change that.
We will walk through the basic principles of micromotor propulsion, how to design and fabricate these tablets, what parameters to evaluate, and where the field is heading. Figure 1 shows the architecture of the proposed dual‑responsive micromotor pill for cefixime. The goal is to give the reader a clear, practical overview – and maybe spark some new ideas for formulation development.
Table 1: Comparison of propulsion mechanisms for GI micromotors
|
Propulsion type |
Fuel / Energy source |
Speed range (µm/s) |
Advantages |
Limitations |
|
Chemical (Mg) |
Gastric acid or water |
20–50 |
Biocompatible, fuel is endogenous |
Hydrogen bubbles may cause gas accumulation |
|
Chemical (Urease) |
Urea (endogenous) |
10–30 |
No external fuel, enzyme‑powered |
Enzyme stability in GI tract |
|
Chemical (Pt) |
H₂O₂ (exogenous) |
50–200 |
High speed, well‑studied |
Not suitable for in vivo without added fuel |
|
Magnetic |
Alternating magnetic field |
5–100 (controlled) |
External control, no chemical fuel |
Requires specialised equipment, limited to accessible regions |
|
Acoustic‑magnetic |
Ultrasound + magnetic field |
30–80 |
Deep tissue penetration, fuel‑free |
Complex setup, potential heating |
|
Biohybrid (bacteria) |
Bacterial metabolism |
10–40 |
Autonomous targeting (chemotaxis) |
Immunogenicity, batch variability |
(Adapted from references 10–16)
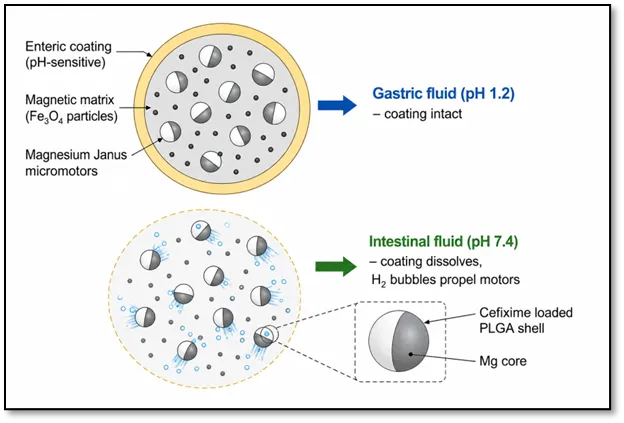
Figure 1: Schematic of the dual‑responsive micromotor pill for colonic cefixime delivery.
2. PRINCIPLES OF MICROMOTOR‑BASED DRUG DELIVERY SYSTEMS
Before we get into manufacturing, it helps to understand how these little motors actually move. There are several different propulsion mechanisms, each with its own strengths and weaknesses. Table 1 summarises them.
2.1 Chemical Propulsion
Micromotors (like magnesium-based) harness a chemical reaction (magnesium with gastric acid) to propel themselves through the body. Hydrogen gas is produced by this reaction and acts like a rocket by trailing behind the micromotor, lifting it through the lumen. The most appealing aspect of magnesium is that it’s biocompatible and that we all need magnesium in our diet. Also, the products of the reaction are not harmful (Mg2+, Cl–, OH– and H2). In one study with mice, magnesium-based micromotors neutralized the gastric acid where they were released from. In fact, after 24 hours, the stomach returned to pH levels consistent with normal stomach function (Hplus=0.00001 mol/l).10
Urease-powered micromotors operate differently. They catalyze the degradation of urea, which generates ammonia and carbon dioxide. Since there’s a lot of urea from protein digestion that’s present in the GI tract, these micromotors won’t ever run out of fuel.11 Platinum-based micromotors require hydrogen peroxide, which isn’t naturally going to be at levels necessary to fuel platinum micromotors; therefore, they are used mostly as lab-based micromotors at present.12
2.2 Magnetically Actuated Propulsion
External control via magnetic fields is available by using a magnet outside of the body rather than using a chemical energy source.¹³ Researchers have developed ways of controlling magnetic micromotors through alternately applied magnetic fields so that they can be directed to specific locations in the intestines. Some designs include the capability of releasing a drug at a specific temperature (the micromotor maintains its integrity at 37 °C, but releases the drug when the temperature reaches 40 °C).¹⁴ This provides an opportunity to combine with local hyperthermia.
2.3 Acoustic and Biohybrid Propulsion
The combination of ultrasound and magnetic fields has been successful in that the ultrasound provides better penetration through tissues and the magnetic field gives direction or control to the ultrasound.15 In diabetic rats, a combination of these two hybrid nanomotors led to an increase of 78% in the oral bioavailability of metformin vs the plain form of the drug (i.e., an increase of 78% in the amount that was made available to treat diabetes). The biohybrid motors draw their inspiration from the natural world. For example, one form of microrobot uses motile bacteria such as E. coli to transport drug payloads. The bacteria are naturally attracted to chemical signals (i.e., they can swim to those chemicals), so the bacteria can be directed toward areas of inflamed tissue.16 There are also examples of DNA-based motors using a combination of hyaluronic acid and light-activated crosslinking, but this is relatively new technology.
2.4 Motion Control and Navigation
Once you have reached the correct location for the device, you still require to have the means to know when to deliver the drug. A great example of device design that accomplishes this is the dual responsivity micro-motor pill. This pill contains a water-powered magnesium Janus motor and a magnetic matrix with an enteric coating.17 The micro-motor pill will be propelled to its target via low-frequency magnetic fields and will then have impetus provided for propulsion via higher-frequency fields through heating or activation of the micro motor. The enteric coating allows for the presence of the micro-motor pill intact until it reaches the colon, so the drug will not escape in the stomach.
Systems that respond to pH are designed to function similarly; however, they take advantage of the pH shifts that naturally occur in the GI tract. For example, pH responsive coatings (often made of Eudragit®) delay the release of the drug until the pH becomes neutral or slightly alkaline.18 Therefore, there is no leakage of drug from the micro-motor pill while in the stomach or small intestine.
3. DESIGN AND FABRICATION OF MICROMOTOR‑ASSISTED TABLETS
Designing a tablet that not only contains millions of micromotors, but also keeps them alive and functional through the watery gastric transit and releases them at the appropriate time and place is non-trivial work.
3.1 Tablet Configuration
The concept for the micromotor pill (MP) is arguably the most advanced of the three apps. A magnesium Janus motor, loaded with drug (cefixime), is trapped within a matrix of enteric polymer containing magnetic particles.17 The entire assembly is compression molded into a normal pill shape (round edges and smooth finish). The enteric coating prevents the activation of the motors while they are in the stomach. When the tablet reaches the small intestine or colon, the enteric coating dissolves and lets water in, causing the motors to create bubbles. A cross section of the proposed tablet is shown in Figure 2.
Making a tablet that contains millions of micromotors – and keeps them alive and functional – is not trivial. The tablet has to protect the motors during gastric transit, then release them at the right time and place.
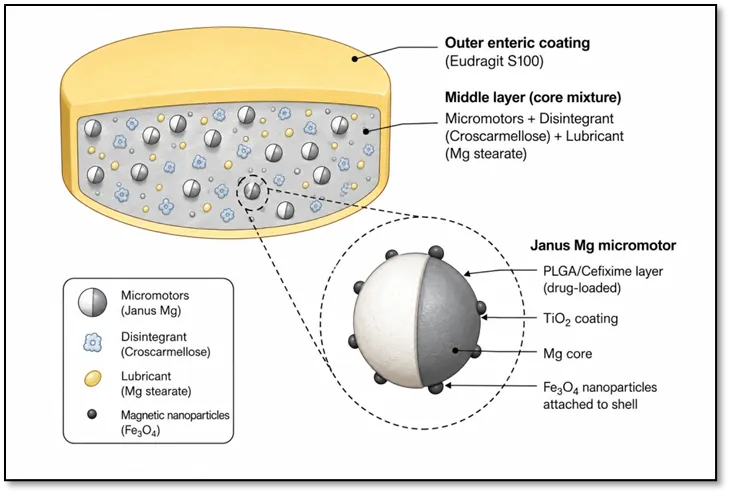
Figure 2: Cross‑section of the cefixime micromotor tablet.
3.2 Fabrication Techniques
Polymerizing Materials with Two-Photon Printing: The 2PP technique allows for highly precise 3D printing. It is particularly useful for creating tumbling microrobots with small magnets that can carry a drug in a hollow cavity; when heated, they have been successfully tested in live rat colons.19
Building Up Layers of Material: This assembly method deposits material in alternating positively/negatively charged layers to construct multiple layers of material. Hydrogel microrobots have been made from two layers, an outer (shell) layer that breaks open in a magnetic field releasing pH-neutralizers, and an inner (core) layer that releases drugs.20
Making Pickering Emulsions: An innovative method of making Pickering emulsions that uses solid particles (rather than surfactants) to stabilize the boundary interface between two immiscible liquids. PLGA nanoparticles can be trapped at the oil/water interface and then coated with urease to perform as active nanomotors.21 The most exciting element of this approach is the ability to produce microfluidic Pickering emulsions; this allows for the continuous, scalable manufacturing of microfluidics.22 One article reported the successful creation of triple-responsive motors (thermophoretic, chemotactic, magnetic) using this technique— a significant advancement toward industrial production.
3.3 Material Selection
Material selection is basically the balancing act. Being biodegradable, approved by the FDA, and tuned for degradation within weeks to months, PLGA is expensive.23 Magnesium is cheap and biocompatible, but it reacts quickly with water, resulting in the need for a coating in many cases.10 Poloxamer 407 helps stabilize the particles during synthesis due to a narrow size distribution and neutral surface charge. Eudragit S100 is a popular enteric polymer because, even at pH 7.0 and above, it dissolves well-suited to colonic delivery.24 Chitosan binds to negatively charged mucus due to its positive charge, which keeps the tablet in place longer. Key materials and their functions are listed in Table 2.
Table 2: Materials used in cefixime micromotor tablets and their roles
|
Material |
Function |
Key property |
Reference |
|
Magnesium (Mg) |
Propulsion engine (fuel) |
Reacts with water/acid to produce H₂ bubbles |
10 |
|
PLGA |
Drug carrier, controlled release |
Biodegradable, tunable degradation |
23 |
|
Cefixime trihydrate |
Active pharmaceutical ingredient |
BCS Class IV, broad‑spectrum antibiotic |
8,9 |
|
Iron oxide (Fe₃O₄) |
Magnetic guidance |
Superparamagnetic, FDA‑approved for imaging |
13 |
|
Eudragit S100 |
Enteric coating |
Dissolves at pH > 7.0 (colonic) |
24 |
|
Chitosan |
Mucoadhesion |
Positive charge binds to mucus |
25 |
|
Poloxamer 407 |
Surfactant / stabiliser |
Reduces particle aggregation |
7 |
|
Croscarmellose sodium |
Disintegrant |
Swells on contact with water |
– |
|
Magnesium stearate |
Lubricant |
Prevents sticking during compression |
– |
4. EVALUATION PARAMETERS FOR MICROMOTOR TABLETS
4.1 In Vitro Characterisation
Testing of Drug Release Kinetics: We have examined the use of buffer medium at four pHs: 1.2 (gastric),5.5 (duodenal), 6.8 (jejunum) and 7.4 (colon). Our target is no more than 10% release at an acidic pH, followed by >80% release over 12-24 hrs in the colon. Figure 3 shows an example of a release profile for one product tested.
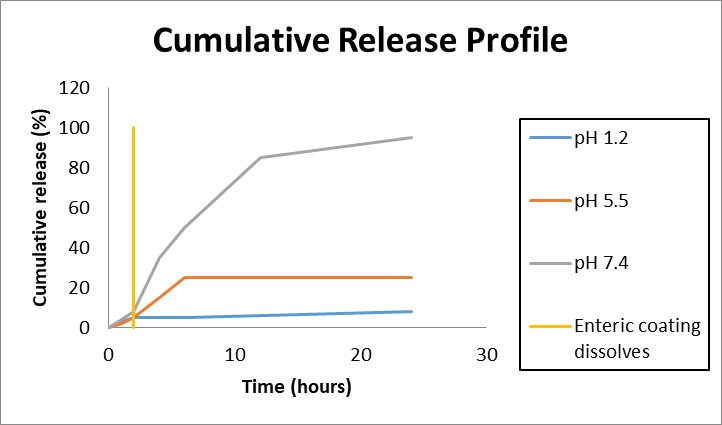
Figure 3: In vitro drug release profile of cefixime from micromotor tablets under simulated GI conditions.
Propulsion Efficiency: Video microscopy will be the standard here. By tracking motors within simulated fluids you can quantify their velocity (microns per second) and determine how directional their motion is (by calculating the mean-square displacement). For magnetic motors we will vary field strength and frequency.
Mucopenetration: Ex vivo tissue (typically pig intestines or rat intestines) will be affixed to a Ussing chamber (or Transwell chamber). Once these tissues are in place, fluorescently tagged motors will be administered, and their penetration depth will be quantified using confocal microscopy. FRAP (Fluorescence Recovery After Photobleaching) may be used to determine diffusion coefficient.
Biocompatibility: Conventional methods (MTT or Live/Dead Assay) will be employed on both Caco 2 and RAW264.7 cells for biocompatibility testing. The previously mentioned µTUM motors exhibit an absence of toxic effects in these assays.19
4.2 In Vivo Evaluation
Biodistribution: The motors can be traced from their point of administration through a combination of fluorescent coloring or using radioactive isotope labels, such as 99mTc. Therefore, the motors are given orally to rats and then tracked as they travel throughout the rats using either IVIS imaging or SPECT/CT. For example, urease-powered nanomotors accumulated significantly (>50%) close to the epithelial surface compared with non-motile controls.11
Pharmacokinetics: Bioavailability refers to standard pharmacokinetic parameters of Cmax, Tmax, AUC, half-life and bioavailability. Cefixime normally has a bioavailability of approximately 40–50% for conventional tablets.9 By enhancing targeting to the area of absorption using micromotors, bioavailability could be increased to 70–85%.
5. CASE STUDY: CEFIXIME MICROMOTOR TABLETS FOR
COLON‑TARGETED DELIVERY
5.1 Pharmacological Profile of Cefixime
The antibiotic Cefixime is effective at killing bacteria through its action on the bacterial cell wall by way of inhibiting bacterial cell wall synthesis, primarily through the binding to penicillin binding proteins. Cefixime's resistance to many beta-lactamases is one of its strengths, allowing it to work against certain resistant strains.8 Cefixime reaches peak blood concentrations between 2 and 6 hours after oral administration with approximately 20-25% of a given amount excreted unchanged in the urine. The low solubility and permeability of cefixime (BCS Class IV) have been problematic.9 However, some researchers suggest that by improving its solubility, cefixime's absorption would resemble that of a Class II drug, whereby the absorption is limited by the dissolution and not the permeability.
5.2 Why Target the Large Intestine?
The current forms of cefixime work fine for urinary or respiratory tract infections; however, for colonic infections (bacterial colitis, diverticulitis, and in severe cases, traveler's diarrhea), a high concentration of cefixime needs to reach the large intestine. Higher doses of systemic administration increase the risk of side effects and give rise to resistance to the antibiotic. In addition, using a broad-spectrum antibiotic will also wipe out the beneficial bacteria in the gastrointestinal tract, resulting in an overgrowth of Clostridium difficile, leading to severe diarrhea and the potential to develop pseudomembranous colitis.16 If cefixime can only be delivered to the infected portion of the large intestine, then these potential side effects can be minimized.
5.3 Proposed Design of Tablets
Based on literature and the architecture outlined in Figures 1 and 2, the following is proposed:
5.4 Locations for Manufacturing
Being a beta lactam, the manufacture of cefixime products should occur in a facility that is dedicated to cefixime product manufacture, and meet strict containment criteria; this would include HEPA filtration, exhaust air 100 per cent, and validated cleaning procedures.26 These current practices are standard for cefixime tablet manufacture. Adding micromotor technology presents the challenge of handling nanoparticles when manufacturing micromotor tablets and may result in additional control requirements. Nevertheless, the infrastructure currently exists.
5.5 Anticipated Advantages
Micromotor tablets may provide the following advantages, theoretically supported by some preclinical animal studies.
6. CLINICAL TRANSLATION AND REGULATORY CHALLENGES
6.1 Regulatory Framework
The fact is: Governments and Regulating bodies are not currently prepared for Microrobots. There are no Specific Guideline's (For Now AT Least) from the FDA, EMA, and Others.27 This class of Products would very likely be deemed (Drug Device Combination Products) — Distributing and/or Combining Drug/Device Classifications (Pharmaceuticals & Medical Devices)— in complying with both Drug Device Classifications. This will result in having to comply with Most Drug Device Compliance Requirements for Safety, Effectiveness, PK, BD, and GMP Manufacturing.
6.2 Translation Barriers
Toxicity and Biocompatibility: Each of the individual components of the motor are considered safe when used alone; however, the put together and made into a motor – plus the putting them into a patient in the order of thousands of motors will present new potential liabilities. As an example, while the individual hydrogen bubbles generated should not present a risk to patients, could there be a risk of gas embolism if multiple motors were to activate simultaneously? Probably not, since the amounts and doses of gases produced are very small, but we still need to evaluate and assess potential issues for that unique event.10
Scale-Up Manufacturing: At present we are capable of manufacturing approximately 1-1000mg/motor in small quantities (milligrams or grams) and we need to manufacture them in quantities greater than this and on a Kg basis (1Kg = 1000g). Microfluidic Pickering emulsification is a promising technology for this purpose, but has not yet achieved validation under GMP.22
In Vivo Navigation: The GI Tract is a very chaotic and variable setting. Peristalsis, varying amounts of fluids, food and mucus as well as changing pH levels present numerous problems when it comes to steering something with precision. While magnetic guidance works for some simple set-ups; it is not as accurate in a live moving animal body.
Clinical Trials: Testing of the magnetic microrobots in pigs and sheep by various groups has been performed with positive results.28 We could be looking at 3-5 years for human clinical trials, at which point, a mTRL framework will be developed to enable the organization of this process.29
7. FUTURE PERSPECTIVES
Some areas are being explored to increase the effectiveness of micromotor-assisted oral drug delivery. These novel solutions seek to enhance targeting, control, safety, and individualization. One specific area of combination therapy can enhance outcomes from multiple drugs at one time (antibiotic (cefixime) and probiotic/beta-lactamase) when treating complex clinical issues (biofilm disruption or preventing dysbiosis). Sequential or simultaneous delivery of two or more active agents can occur using multilayer micromotors that possess different layered active agents.
Future micromotor designs could include time-programmed degradation of polymeric coating allows for sequential delivery (i.e. probiotics would colonize a niche before antibiotics eradicate unwanted pathogens without disturbing the beneficial flora that was just formed).
Accurately tuning the thickness and composition of each individual layer in order for multiple components to work together as one system will enable successful construction of a synergistic system using a layer-by-layer (LbL) assembly method.
Live imaging methods are another requirement for the development of a transferable micromotor system.
The location of micromotors in existing studies is typically determined through evaluation; either through histopathological analysis or removed tissue evaluation (ex vivo).
To enhance existing studies utilizing micromotors, it is critical that additional imaging markers be introduced to monitor and track fleets of motors without invasively imaging patients, such as MRI (using superparamagnetic iron oxide nanoparticles) and ultrasound (using gas vapor-filled bubbles). Tracking the behavior of drugs inside the body will require the creation of new contrast agents that change their imaging characteristics when an active pharmaceutical ingredient is added to the contrast agent.
Combination therapies have great potential within this space. The co-delivery of two or more active agents (e.g., cefixime and a probiotic or beta-lactamase inhibitor) allows clinicians to use combination therapy in an attempt to address complex clinical situations (e.g., biofilm disruption) or prevent the development of dysbiosis.
Multilayer micromotors, where each layer is designed to carry a different payload, are designed to provide either sequential or simultaneous release of therapeutic agents (e.g., probiotics, then antibiotics).30 Future multilayer micromotor designs may also be able to provide time-dependent degradation of the polymer coating with each layer (e.g., release probiotics first to occupy a niche, then the antibiotics to kill the pathogens, preserving the beneficial flora).
Coordinating the thickness and type of material for each layer in an effective manner will be necessary to create these types of synergistic systems; however, the design flexibility associated with layer-by-layer assembly will facilitate the realization of this goal.
Real‑time imaging another important requirement is real-time imaging. Most current studies that use micromotors rely on using ex vivo or histological methods to identify where they are localized. Adding imaging components (e.g., superparamagnetic iron oxide nanoparticles for use with MRI; microbubble-filled gas to use with ultrasound) would allow direct non-invasive tracking of motor fleets as they move throughout the body.³¹ In addition, smart contrast agents that change signal intensity upon the release of drug (e.g., by quenching due to changes in pH or enzymatic cleavage) can provide visual proof of whether the payload has been delivered successfully. This "theranostic" capability would be very helpful when developing treatment regimens for diseases such as inflammatory bowel disease or colorectal cancer since being able to see exactly when and where a drug is administered will assist clinicians with making appropriate dosing adjustments and eliminate needless repeat dosing.
Biomarker‑responsive motors take the concept of intelligent delivery one step further. This type of motor would have no pre-programmed triggers and would not activate until they detect a specific molecular signal of disease, such as an elevation in reactive oxygen species (ROS), the presence of matrix metalloproteinases (MMPs) that are over-expressed in inflamed tissue, or the presence of bacterial toxins (e.g., lipopolysaccharide (LPS).22 A possible approach is for the motor to contain a catalytic engine (for example, magnesium (Mg) or zinc (Zn)) that is contained within a polymer gate, which will only degrade in the presence of these biomarkers. The use of this approach would minimise the potential for unintended leakage of drugs from healthy intestinal segments, maximise the local drug concentration at the site of pathology and reduce the systemic toxicity of the drugs. Early proof-of-principle studies using ex vivo tissue models have been conducted, and the next logical step is to translate these studies into animal models.
Personalised devices The use of 3D Printing to create custom-fit devices supports a movement away from one-size-fits-all oral delivery systems. A physician could design, utilizing patient-specific anatomical data from Computer Tomography (CT) or Magnetic Resonance Imaging (MRI), a micromotor-based delivery system (e.g., pill-like) tailored to the specific size, shape and orifice release pattern of an individual's gastro-intestinal tract, dependent upon the patient's anatomy and the location of the patient's disease33. An example: a patient with a stricture in the ascending colon would receive an elliptical capsule that would resist disintegration prematurely while passing through the narrowed portion; but a patient with diffuse ulcerative lesions in the transverse colon may obtain a multicompartment device releasing multiple motor swarms over a longer distance. The advantage of rapid prototyping with 3D Printing is the ability to quickly create novel geometries (e.g., helical, tubular, spherical) without the expense of photolithographic masks. As desktop "bioprinters" become more widely adopted, the existing model for "pharmacy on demand" may evolve into reality in hospitals.
Fully biodegradable motors that are completely biodegradable will eliminate the concern of having metallic residues left behind. Although zinc, magnesium, and iron are all recognized as safe and are essential trace elements, they do NOT guarantee total dissolution from the gastrointestinal tract. For example, if the motor accumulates in diverticula or adheres to the mucosa, complete dissolution would not occur. However, with the recent development of coatings that can protect the inside of the motor while providing for biodegradability (e.g., polylactic and polyglycolic acid, PLGA) and the development of corrosion-resistant alloys on the outside of the motor can provide for tuning of the rate of motor biodegradation from hours to days.34 For a motor to achieve its intended purpose, the structure of the motor must remain intact until it arrives at a desired site. Thereafter, the engine will unload and continue on to total biodegradation until no materials remain (i.e. through transforming to nontoxic ions or lesser molecules) (i.e. by means of absorption or removal).Preliminary investigations utilizing zinc-based biodegradable engines indicate that they are safe; however, additional long term (several weeks) examinations of biodegradation in larger species will be necessary to find out the complete degree of safety. The biggest challenge will be uniting biodegradability with all other aspects described above such as imaging, responsiveness, and personalization.
8. CONCLUSION
Micromotor-assisted drug delivery is not just a step forward from currently available oral dosage forms. Propulsion systems used for drug delivery allow a drug to traverse the viscous mucosal tissue and propel until the drug is deposited within a target area of need, as opposed to using simply diffusion from static particles into the GI tract, thus enabling delivery of drugs via propulsive force through the GI tract against peristaltic movement, into crypts and directly to the targeted area requiring drug delivery. Additionally, the dual- responsive pill which contains Mg-based Janus micro-motors as well as a magnetically interactive enterically-coated matrix is expected to be the preferred formulation option due to the balance in construction and durability of the design. The enteric coating isolates the micro-motors from the gastric acid, allowing unprohibitcd passage to the intestines, while the magnetic attribute of the matrix will facilitate guiding the micro-motors to the areas of greatest interest within the colon. Finally, via Janus propulsion, hydrogen bubbles are offers a means of self-propulsion. This method supports the current high-throughput manufacturing practices that have been established for most beta-lactam products and each of the components of this device offers historical evidence of appropriate safety and efficacy, including Mg, Fe and enterically-protected polymers.
Because cefixime – a third-generation cephalosporin with notoriously low colonic bioavailability (approximately 1 – 5% after oral administration) – the application of this new delivery system can positively impact clinical care by allowing the direct propulsion of cefixime-containing vehicles to the colonic mucosa while providing a sustained, high concentration of drug in such a way that both low bioavailability and high active efflux of the drug are overcome. Target therapeutic applications for this new delivery system could be to target known pathogenic overgrowth of colonic bacterial, mild to moderate ulcerative colitis with secondary infection(s), and lastly to utilize cefixime's immunomodulatory properties to assist with chemotherapy and/or radiotherapy for colorectal cancer.
There are numerous remaining problems. Increasing from a healthy milligram laboratory batch to gram scale to consistently control the movement motor of micro motors precision and speed of micro motors is difficult however the new process of continuous microfluidic fabrication looks very good. The competition in the human colon is hard; a lot of obstacles that are interacting with one another; creating a lot of difficulties for determining how to best feed back (in real time) the position of the motor so that picture (motor) feedback from each position is possible. The most serious problem will most likely be regulatory issues; combination products (drugs/device / biological component) are a new category of regulatory product, and the guidelines for micromotors are still not fully defined. In addition to the high probability of safety needs to be shown before first in human trials can be done, there is also the potential for gas embolism caused by excess bubble formation due to certain gas(s) and trace metals, and long time accumulations of those trace metals.
Over the last decade, scientific knowledge and data have progressed at an astonishing rate, with multiple studies showing the feasibility of utilizing micromotor-based drug delivery systems via preclinical animal models. What we need to focus on, now, as a team of expert pharmaceutical scientists (with knowledge of formulations and stability), engineers (developing propulsion/control mechanisms) and regulatory personnel (working on developing adaptive paths toward approvals), is establishing collaboration as a standard for this type of work. Historically, these types of collaborations have accelerated the clinical trials and approvals of other types of drug delivery systems, such as doxorubicin delivered via liposomes or through the use of antibody-drug conjugates. The expectation would be that micromotor-based delivery would also achieve similar outcomes. With ongoing funding and innovative thinking, the first human trials of the oral micromotor-based pill are anticipated in a time frame of 5-7 years. The implications for how individuals view "taking a pill," will likely be revolutionary.35
CONFLICT OF INTEREST
I hereby declare no conflict of interest
REFERENCES


Rosemol John, Karmvir, Micromotor-Assisted Targeted Gastrointestinal Drug Delivery: A Systematic Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 7134-7148. https://doi.org/10.5281/zenodo.21011337
 10.5281/zenodo.21011337
10.5281/zenodo.21011337