
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
IPS Academy College of Pharmacy, Rajendra Nagar, A.B. Road, Indore–452012, (M.P), India.
The problem of antimicrobial resistance is a major public health issue affecting many countries around the globe. Antimicrobial resistance is reducing the ability of traditional antibiotics to treat certain diseases and increasing the chances of an unsuccessful medical treatment due to resistance to the prescribed medication. Recently, researchers have made advancements in using novel drug delivery systems, such as polymeric nanoparticles, liposomes, and solid lipid nanoparticles along with dendrimers, as new delivery methods to improve drug efficacy for treating patients with antibiotic-resistant pathogens. Specifically, delivery systems designed with nanotechnology provide several advantages over traditional methods including stability of the drug, controlled release of the drug, and site-specific delivery of the drug. In addition to these advantages, the review also discusses the use of ligand modified and stimuli sensitive delivery systems as potential methods for overcoming biological barriers and improving the efficacy of therapeutics. The review also discusses new strategies to combat bacterial biofilms and intracellular infections, both of which play an important role in the development of chronic and hard-to-treat infections. Finally, this review highlights the challenges of bringing these promising new delivery systems to the clinic including issues surrounding safety, formulation complexity, and difficulties associated with translation into clinical settings, all while highlighting the significant potential that these advanced delivery systems hold for addressing the growing threat of antimicrobial resistance.
AMR has become a new global health crisis that threatens to reverse the impressive gains made over the last century in the use of antibiotics. The CDC estimates that there are about 2.8 million antibiotic-resistant infections occurring in the U.S. each year and that there are over 35,000 deaths annually as a result of these infections. In 2019 alone, a groundbreaking study in the Lancet reported that 1.27 million people died due to AMR and that without urgent action, we could see over 10 million people die each year by 2050. The development of AMR is the result of many factors, but the most important of these is that AMR has progressed along the lines of Darwin’s theory of “survival of the fittest” because of repeated use and misuse of antibiotics in both clinical and agricultural settings. Bacteria have developed many different methods to defend themselves against antibiotics, for example, enzymes that will destroy antibiotics (e.g., β-lactamases, and carbapenemases), expelling the antibiotic via pumps, alteration of the antibiotic’s target site (e.g., PBP2a in MRSA), and creating biofilms that protect bacteria from the effects of antibiotics. All of these methods are encoded on different mobile genetic elements, e.g., plasmids, integrons, and transposons, which allow for horizontal transfer of resistance determinants between different species of bacteria, thereby facilitating and greatly accelerating the spread of resistance.
Enterococcus Faecium, Staphylococcus Aureus, Klebsiella Pneumoniae, Acinetobacter Baumannii, Pseudomonas Aeruginosa & Enterobacter Species; these ESKAPE pathogens are considered to be the most dangerous organism per CDC’s opinion. The majority of the deaths occurring in hospitals due to an AMR is attributed to these Five bacteria alone. [1] There has been an emergence of PDR (pan-drug resistant) bacterial strains, for whom no pharmaceutical/ antibiotic effective drug harm exists; therefore, creating the need for new innovative treatment plans. [3] Traditional antibiotic drug therapies are not well suited to treat patients who are infected by AMR bacteria.
The administration and delivery route of conventional drugs result in very low concentrations (sub-therapeutic) at the infection site because they have low penetration into tissues, have high clearances from the kidneys, and bind to serum proteins. This combination of pharmacokinetics encourages bacteria to become resistant to other antibiotics. [6,18] Hydrophilic antibiotics also cannot pass through the outer membrane of Gram-negative pathogens, nor due to their being sequestered inside biofilm's EPS can traditional treatments reach the biofilm. [10,22]
Targeted drug delivery (TDDS), a newer delivery method; addresses these challenges by using nano-scale engineered carriers, which will provide higher concentrations of antibiotic at the infection site without being cleared by the immune system, be able to respond to the local microenvironment conditions and penetrate through the biofilm barriers, thereby resolving multi-pathway resistance mechanisms at once. [6,18] This review will provide a comprehensive overview of nanoparticles; biological delivery vehicles; stimuli-responsive systems and combination therapies with their regulating/translating issues and challenges. [7,8]
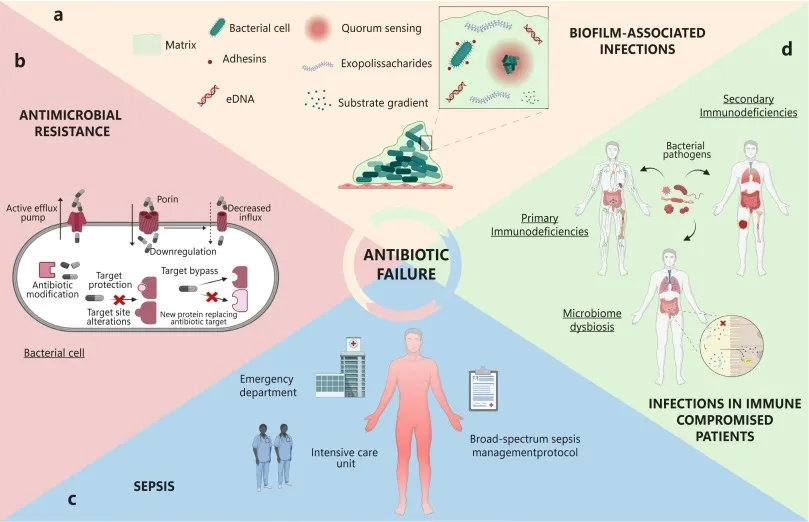
Figure 1: AMR Resistance Cascade — From Antibiotic Administration to Treatment Failure.
2. Mechanism of Antibiotic Resistance
To develop targeted and rational delivery systems, it will first be necessary to understand the molecular and cellular bases of the phenomenon known as antibiotic resistance. Mechanisms of antimicrobial resistance fall into four general categories: the inactivation of the drug; alterations in the drug target; decreased permeability; and expulsion of the drug from the cell through active transport systems. In clinical settings, it is commonly seen that bacteria may have as many as several of these mechanisms at the same time which can complicate successful treatment of infections.
2.1 Enzymatic Drug Inactivation
Beta-lactamase enzymes are the most important cause of resistance against Beta-lactam antibiotics. More than 2,700 distinct beta-lactamases have been identified; however, the Extended-Spectrum Beta-Lactamases (ESBL) and carbapenemases such as KPC, NDM-1 and OXA-48 are particularly difficult to treat. [3,9] All beta-lactamase enzymes facilitate the hydrolysis of the beta-lactam ring, making penicillin, cephalosporin, and carbapenem ineffective drugs. Similar to the situation with beta-lactamase, aminoglycoside-modifying enzymes chemically alter the structure of the aminoglycoside, thereby preventing it from binding to a ribosome. [4]
2.2 Efflux Pump Overexpression
Bacterial efflux pumps are transmembrane protein complexes that actively expel antibiotics from the bacterial cell, maintaining intracellular drug concentrations below lethal thresholds. Major superfamilies include the Resistance-Nodulation-Division (RND) family (MexAB-OprM in P. aeruginosa, AcrAB-TolC in E. coli), the Major Facilitator Superfamily (MFS), and ATP-Binding Cassette (ABC) transporters. [4,18] Efflux pumps exhibit remarkably broad substrate specificity, conferring simultaneous resistance to fluoroquinolones, tetracyclines, chloramphenicol, and macrolides—a key target for co-delivered efflux pump inhibitors. [18]
2.3 Target Site Alteration and Biofilm Formation
In gram-positive organisms, point mutations and enzymatic modifications are two of the main strategies for developing resistance to antibiotics at their target sites. An example of this is the mecA gene found in MRSA, which encodes the modified penicillin binding protein PBP2a. This protein has a significantly lower affinity for all beta-lactam antibiotics than its unmodified counterpart. [3] Mutations that occur in gyrase and topoisomerase IV confer resistance to fluoroquinolone antibiotics, as well as the mutation of rpoB conferring resistance to rifampicin in M. tuberculosis. An additional example is E. faecium's ability to develop resistance against vancomycin through the use of different peptidoglycan precursors (D-Ala-D-Ala to D-Ala-D-Lac), thereby decreasing the sensitivity of the organism to vancomycin by a significant degree. [4,9] The final major mechanism of antibiotic resistance occurs within biofilms, with the formation of biofilms being, arguably, the most clinically significant mechanism of bacterial resistance to antibiotic therapy. Biofilms represent the majority of chronic and recurrent bacterial infections, with greater than 80% attributed to their presence. [10] Within biofilms, the bacteria are embedded inside a self-generated matrix of polysaccharides, proteins, extracellular DNA (eDNA), and lipids, otherwise known as the extracellular polymeric substance (EPS). Within the EPS, physical and chemical barriers to antibiotic penetration are created, preventing the antibiotics from reaching the bacterial cells and resulting in the presence of subpopulations of persistently resistant cells. [10,22] Furthermore, mature biofilms may require antibiotic concentrations that are 100 to 1,000 times greater than MIC to eradicate the mature biofilm than would be required for the planktonic cells. [26]
Table 1: Major Antimicrobial Resistance Mechanisms, Affected Drug Classes, and Associated Pathogens.
|
S. No. |
Resistance Mechanism |
Drug Class Affected |
Key Bacterial Species |
Clinical Impact |
Resistance Mechanism |
|
1. |
β-Lactamase Production |
Penicillin, Cephalosporins |
E. coli, K. pneumoniae |
Very High |
β-Lactamase Production |
|
2. |
Efflux Pump Overexpression |
Fluoroquinolones, Tetracyclines |
P. aeruginosa, MRSA |
High |
Efflux Pump Overexpression |
|
3. |
Target Site Alteration (PBP2a) |
Methicillin, Oxacillin |
Staphylococcus aureus (MRSA) |
Very High |
Target Site Alteration (PBP2a) |
|
4. |
Outer Membrane Impermeability |
Carbapenems, Polymyxins |
A. baumannii (CRAB) |
High |
Outer Membrane Impermeability |
|
5. |
16S rRNA Methylation |
Aminoglycosides |
Gram-negative pathogens |
Moderate–High |
16S rRNA Methylation |
|
6. |
Van Ligase Gene (vanA/B) |
Vancomycin, Teicoplanin |
VRE (Enterococcus spp.) |
High |
Van Ligase Gene (vanA/B) |
|
7. |
Plasmid-Mediated (mcr-1) |
Colistin (last resort) |
Enterobacteriaceae |
Emerging |
Plasmid-Mediated (mcr-1) |
|
8. |
Biofilm Formation |
Multiple drug classes |
S. epidermidis, P. aeruginosa |
Extreme |
Biofilm Formation |
3. Nanoparticulate Drug Delivery Systems
Drug delivery systems based on nanotechnology have become one of the most highly researched options to prevent antimicrobial resistance (AMR). Nanotechnology systems are able to utilise multiple physicochemical and biological mechanisms to provide targeted, controlled and synergistic delivery of antimicrobial drugs to sites of infection with minimal systemic toxicity. [4,9]
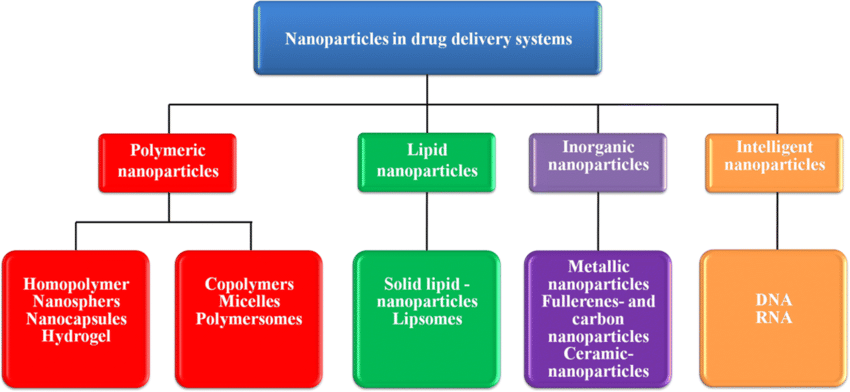
Figure 2: Classification of Nanoparticulate Drug Delivery Systems for AMR Combat
3.1 Liposomal Drug Delivery Systems
Liposomes are vesicles made of phospholipid bilayer membranes that are 50 to 400 nanometers in diameter and have been used as the most clinically advanced nanoparticle delivery system for antibiotics. [5] Due to their structure, which mimics the membrane of bacterial cells, liposomes can fuse with the membranes of Gram-positive bacteria. This avoids the effects of efflux pumps and gives higher concentrations of the drug than would otherwise be achieved through normal administration. The FDA approved AmBisome (an antifungal drug) delivered via liposomes shows that this method is clinically feasible. [5,18] The use of PEGylation increases how long liposomes stay in circulation by providing a hydrophilic steric barrier that inhibits opsonization, thereby decreasing the clearance by the mononuclear phagocyte system (MPS). In addition to this, surface functionalizing liposomes with bacterial ligands such as antibodies, aptamers, lectins, or antimicrobial peptides allows for active targeting. [5,23] The use of pH sensitive liposomes exploits the low pH (5.5-6.5) of infected tissue for controlled release of drug at the sites of infection. [14]
3.2 Polymeric Nanoparticles
Historically, PLGA, or poly (lactic-co-glycolic acid), has been the most widely researched biodegradable polymer platform for antibiotic delivery. In addition to being FDA-approved, PLGA nanoparticles have well-defined degradation kinetics. With the ability to vary the copolymer ratio, molecular weight, and particle size, PLGA nanoparticles can provide tunable sustained-release profiles of antibiotics ranging from hours to weeks. [7,8] Another significant advantage is that encapsulating the drugs within the PLGA matrix protects them from enzymatic inactivation, particularly needed against beta-lactamase-producing microorganisms. [8,18] Chitosan, a naturally occurring, cationic polysaccharide, has both intrinsic antimicrobial properties and also serves as an excellent nanoparticle scaffold. The electrostatic interaction of the positively charged chitosan nanoparticles with the negatively charged outer membrane of the bacteria and the biofilm matrix results in improved penetration and uptake. [7] Additionally, chitosan nanoparticles have been shown to decrease the MIC for ciprofloxacin against Pseudomonas aeruginosa biofilms by 8 to 16 times. [7,22]
3.3 Dendrimers and Advanced Polymer Architectures
Tree-like macromolecules called dendrimers are hyperbranched and are characterized by their precise molecular formations and the multivalent surface functionalities they have. In particular, fourth through sixth generation PAMAM dendrimers have been found to be great antibiotic vehicles with both high drug load capabilities, controlled release through ester or hydrazone linkages as well as intrinsic antimicrobial capabilities due to their charge to disrupt the membrane of bacteria. For example, trimethoprim-loaded fourth generation PAMAM dendrimers exhibited up to 4 times the activity against trimethoprim-resistant E. coli when compared to just trimethoprim alone.
Table 2: Comparative Analysis of Novel Targeted Drug Delivery Systems for AMR
|
S. No. |
Delivery System |
Examples |
Advantages |
Drug Loaded |
Efficacy |
|
1. |
Liposomes |
PEGylated liposomes, archaeosomes |
High encapsulation, biocompatible, bilayer fusion |
Gentamicin, Amphotericin B |
70–85% MIC reduction |
|
2. |
Polymeric Nanoparticles |
PLGA, chitosan, PLA nanoparticles |
Controlled release, biodegradable, functionalization |
Rifampicin, Ciprofloxacin |
10–100× bioavailability |
|
3. |
Dendrimers |
PAMAM, poly-L-lysine dendrimers |
Precise architecture, multifunctional |
Trimethoprim, Vancomycin |
4–8× activity improvement |
|
4. |
Solid Lipid Nanoparticles |
SLN, nanostructured lipid carriers |
Excellent stability, scalable, GRAS |
Azithromycin, Linezolid |
3–5× PK improvement |
|
5. |
Metal Nanoparticles |
AgNPs, AuNPs, ZnO NPs |
Intrinsic antimicrobial, photocatalytic, synergistic |
Drug-free / combination |
6–10× synergistic kill |
|
6. |
Bacteriophage-Based |
Phage cocktails, phage-drug conjugates |
Highly specific, self-amplifying, biofilm penetration |
Phage + Antibiotic |
Eradicates MDR biofilms |
|
7. |
Hydrogel Systems |
Thermo/pH-responsive hydrogels |
Localized delivery, stimuli-responsive |
Mupirocin, Fusidic acid |
Topical AMR infection cure |
|
8. |
OMV / Exosomes |
Bacterial OMVs, engineered exosomes |
Natural membrane tropism, immune evasion |
siRNA, antibiotics |
Pre-clinical efficacy >90% |
4. Targeting Strategies: Active, Passive, And Stimuli-Responsive
The therapeutic effectiveness of nanoparticle-based drug delivery systems is essential to obtain adequate amounts of drug to accumulate in the area of infection. Passive targeting, active targeting by ligand-receptor binding, and stimuli-responsive delivery systems are the three main approaches for targeting drugs.
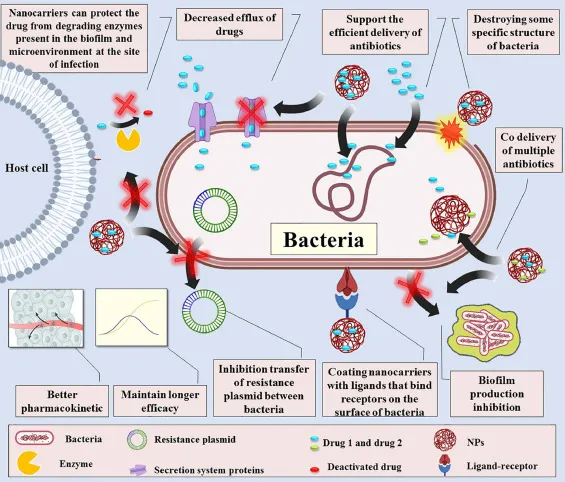
Figure 3: Nanoparticle Active Targeting and Drug Release Mechanism at Bacterial Infection Site
4.1 Passive Targeting via Enhanced Permeability
Bacterial infections lead to an increase in vascular permeability and phagocytic immune cell recruitment due to the inflammatory response, creating a microenvironment that allows for the passive accumulation of nanoparticles in the appropriate size range (50–200 nm) within the infected area. This effect is similar to the EPR effect observed in tumor biology and has been utilized for the delivery of antibiotics to soft tissue infections (e.g., cellulitis), pneumonia and osteomyelitis. [18, 23]
4.2 Active Targeting via Ligand-Receptor Interactions
Active targeting is when the targeting part is directly attached to the surface of a nanoparticle to engage in molecularly cohort style of recognition to one of the surfaces of a bacterial cell or to the surface of an infected tissue. Antibodies: Polyclonal antibodies that recognize proteins, polysaccharides, and/or lipids associated with bacteria (e.g., LPS and teichoic acid) as well as antibody fragments, such as both full-length antibodies (IgG) and Fab and scFv, that recognize bacteria, are examples of high-affinity ligands. Aptamer-based high-affinity ligands that bind to specific bacterium targets. Antimicrobial peptides that preferentially bind to the negatively charged membrane of bacteria. Mannose-based ligands that target mannose receptors expressed on macrophages that contain intracellular bacteria. [6,7,24]
4.3 Stimuli-Responsive Drug Delivery
Nanocarriers that respond to stimuli will provide their cargo according to environmental signals associated with the infectious state of the tissue. Researchers have taken advantage of each of the following triggers: pH (that is, the acidic environment of infected tissues, phagolysosome and biofilm); enzymes (for example, nanocarriers that can be cut by hyaluronidase, lipase, proteases and beta-lactamases from bacteria); positive charged/reactive oxygen status (which is also called oxidative stress); heat sensitive hot/cold) and redox-reactive (referring to oxidation/reduction). [14,6] Hydrazone, acetal, and ketal-based polymers will release their drug at or below pH 6.5, which is a characteristically chronic condition for an infected area of tissue (abscess cavity or within a biofilm structure). [14] Nanoparticles coated with hyaluronic acid with linkers that can be cleaved by hyaluronidase will enable the selective release of drugs into a biofilm infected area of tissue, since there is an overabundance of hyaluronidase produced by either S. aureus or S. pyogenes. [6,14]
5. Biofilm-Targeted Drug Delivery
Biofilms can be a significant obstacle to successful antibiotics reaching their targets because they comprise the vast majority of chronic infections such as device-related, chronic wound, cystic fibrosis-related, and infective endocarditis. [10,26] The multi-layered structure of mature biofilms creates successive barriers that hinder drug penetration and effectiveness; therefore, delivery strategies should involve multiple valences. [10,22]
Table 3: Conventional vs. Nanoparticle Drug Penetration Through Bacterial Biofilm Layers.
|
S. No. |
Biofilm Layer |
Conventional Antibiotic |
Nanoparticle-Based Drug |
Outcome / Efficacy |
|
1. |
Outer EPS Matrix |
Blocked / degraded (>80%) |
DNase-coated NPs dissolve EPS |
Penetration ↑ 4–6× |
|
2. |
Intermediate Zone |
Minimal penetration |
pH-triggered release in acidic biofilm |
Local conc. maintained |
|
3. |
Persister Cell Core |
No effect (dormant cells) |
Hyperthermia / photodynamic NPs |
Persister cell eradication |
|
4. |
Quorum Sensing Network |
Not disrupted |
QS inhibitor-loaded nanocarriers |
Biofilm dispersion induced |
5.1 EPS-Degrading Nanocarrier Systems
Penetration of nanocarriers into biofilms can be significantly enhanced by enzyme-modifying their surfaces to degrade extracellular polymeric substances (EPS). Substantial effects have been noted with enzymes like DNase I, which digests extracellular DNA (eDNA), dispersin B, which denatures poly-N-acetylglucosamine, and alginate lyase, which cleaves alginate in Pseudomonas aeruginosa biofilms, as they help break down parts of the biofilm matrix. Ultimately, molecules can penetrate deeper into the biofilm due to the breakdown of the biofilm matrix, with approximately 4–6 times greater penetration reported as a result. In one particular study, the use of DNase I to modify nanocarriers made from PLGA resulted in significant decreases in the biomass of Staphylococcus aureus biofilms. A 78% reduction in biofilm biomass was observed in a flow cell system treated with DNase I-coated nanocarriers; however, treatment with DNase I alone resulted in only a 12% reduction.
5.2 Quorum Sensing Inhibition
A system of communication between cells based upon the density of cells in a population is known as quorum sensing (QS) and controls the development of biofilms and virulence factors. In this study, nanocarriers containing both QS inhibitors (furanones, brominated furanone C-30, garlic-derived ajoene, and synthetic AHL analogs that disrupt the maintenance of biofilm's signaling and deliver antibiotics to 100% of the dispersed bacterial population were created, resulting in a synergistic effect and total eradication of the biofilm that could not have been achieved by either approach alone.
5.3 Photodynamic and Photothermal Anti-biofilm Strategies
Photosensitizers are used in photodynamic therapy to generate reactive oxygen species that kill cells when exposed to light. The reactive oxygen species do not cause the development of resistance like antibiotics do, so photodynamic therapy is very effective against biofilms that are resistant to antibiotics. Photothermal therapy uses gold nanorods or carbon mixtures that absorb near-infrared light and produce heat (42–50°C) that destroys the membranes of bacterial cells, disrupts the matrix surrounding the cells and kills persister cells.
6. Biological Approaches: Bacteriophage Therapy and OMVs
6.1 Bacteriophage-Antibiotic Synergy (PAS)
Bacteriophages are also known as the viruses of bacteria and offer a revolutionary way to provide therapy for infections caused by AMR organisms. With recent examples, such as the 2017 landmark therapy provided at UC San Diego using a personalized bacteriophage cocktail to help save the life of a patient suffering from MDR A. baumannii, this therapy is now considered to be “clinically viable” when treating severe infections caused by pan-drug-resistant organisms. Combination therapy using bacteriophages and antibiotics has an added advantage because bacteriophages can penetrate biofilms through the ability of the phage to degrade the biofilm’s extracellular polysaccharide (EPS) protective barrier; expose the bacteria to the antibiotic, and maintain the presence of a bacteriophage in the infected area—the combination of these advantages can make it possible for the antibiotic to work on the infection by creating mutations of resistance to the antibiotics that then allow the bacteria to revert back to being susceptible to the antibiotic; bacteria can take on multiple phages that attach to multiple bacterial cell surface receptors; bacteria; and phages can replicate in the infected area, thus creating their own mini-dosing environment for the administration of treatment. [11,19]
6.2 Outer Membrane Vesicles and Exosome-Based Delivery
Gram-negative bacteria produce small (20–300 nm), spherical nanostructures called outer membrane vesicles (OMVs). These vesicles can be engineered for various purposes such as drug delivery due to their ability to naturally target homologous bacteria, provide a means of activating TLRs in the immune system inherently, and allow for the loading of drugs that are both hydrophobic and hydrophilic. [6] In addition, OMVs that were loaded with the antibiotics colistin and rifampicin showed a 16-fold decrease in the minimum inhibitory concentration (MIC) against carbapenem-resistant A. baumannii. [28]
7. CRISPR-Cas Systems as Targeted Antimicrobial Tools
A major breakthrough in the field of AMR research has been the adaptation of the CRISPR-Cas (Clustered Regularly Interspaced Short Palindromic Repeats) gene-editing tool into a precision-based antimicrobial platform. Unlike conventional antibiotic therapy that kills all susceptible microbes indiscriminately, often causing a selection pressure and leading to the emergence of antibiotic resistance, CRISPR-based antimicrobial therapies allow users to design a CRISPR-based antimicrobial agent with single nucleotide resolution to target very specific sequences within the pathogen’s genome, or the resistance genes of specific pathogens. The CRISPR-Cas9 or the Cas12a systems can be delivered via engineered phagemid particles or lipid nanoparticles to introduce lethal double-strand breaks in DNA at specific locations within the genome by targeting the resistance genes associated with pan-resistant organisms (e.g., blaNDM-1, mecA, vanA) in order to resensitize these resistant organisms to the conventional antibiotics to which they had become resistant, by targeting essential genes in the bacterial genome (e.g., gyrB, ftsZ, rpoB) for sequence-specific killing of bacteria. Researchers have been able to demonstrate greater than 99.9% selective killing of the targeted bacterial strains within complex polymicrobial communities while achieving less than 0.1% off-target activity against non-targeted bacterial species or against mammalian cells. In the delivery of CRISPR-based antimicrobial therapies, significant progress has been made toward the development of new delivery vectors such as naturally occurring M13 phage particles (which have a natural tropism for enteric bacteria), lipid nanoparticles (which were developed from messenger RNA vaccine technologies), and conjugative plasmids (which exploit horizontal gene transfer as a mechanism for bacterial spread) to deliver CRISPR-based antimicrobial agents. The combination of highly specific targeting capability, ability to self-amplify via phage replication, and versatility with respect to target selection makes CRISPR-based antimicrobial agents one of the most revolutionary and next-generation platforms for anti-infective therapy. [13,27]
8. Efflux Pump Inhibitors Co-Delivered via Nanocarriers
Resistance due to efflux-pump activity is a major cause for diminishing the effectiveness of fluoroquinolone, tetra-cycline, and macrolide antibiotics for treating MDR Gram-negative bacteria. Using the strategy of co-formulating EPIs (efflux pump inhibitors) with antibacterial agents in nano-carriers provides a unique method for overcoming this mechanism of resistance. Some examples of EPIs that have been investigated include PAβN (phenylalanine-arginine-β-napthylamide), which has broad activity against efflux pumps in the RND family present in P. aeruginosa and E. coli, CCCP (carbonyl cyanide m-chlorophenylhydrazone), as well as plant-derived natural products such as berberine, piperine and resveratrol. PLGA (polylactide-co-glycolide) nano-particles that have been co-loaded with ciprofloxacin and PAβN produced a reduction of 32-fold in MIC against ciprofloxacin-resistant P. aeruginosa, due to both the action of the EPI to inhibit the efflux pump and due to the nanoparticles being able to facilitate endosomal escape of the drugs that occurred before the detection of the drugs by the efflux pump. [8,18] Furthermore, liposomal (lipid-bilayer) formulations that contained both verapamil and clarithromycin were able to re-establish clarithromycin susceptibility in macrolide-resistant strains of M. abscessus isolated from patients in the clinics. [5]
9. Antimicrobial Peptide Delivery Systems
Antimicrobial peptides (AMPs) are amino acid chains between 10 and 50 amino acids long that are generally both cationic and amphipathic in structure. They are critical to the innate immune response. AMPs work differently than traditional antibiotics by acting mainly through interaction with bacterial cell membranes. The negatively charged membranes of microbes have a high ionic strength and AMPs have a low molecular weight; therefore, they can rapidly attach to the membrane through electrostatic forces, then penetrate the membrane and create an aqueous channel or pore, resulting in lysis of the cell. These types of actions can combat many different types of multi-drug resistant (MDR) organisms and they also have a low incidence of developing resistance to AMPs after long exposures.
Examples of AMPs are: (1) magainins; (2) defensins; (3) polymyxin antibiotics (i.e., colistin); and (4) cathelicidin (e.g., LL-37). There are also synthetic peptides that are derivatives of AMPs such as pexiganan and WLBU2. AMPs are effective against ESKAPE pathogens; mycobacteria; fungi; and certain enveloped viruses. However, even though they exhibit similar antimicrobial activity in the laboratory, there are several factors that limit their clinical usage. These factors include:
Nanocarriers have been evaluated as a means to contend with these obstacles. Nanocarrier encapsulation of AMP keeps AMPs from being biochemically broken down; it facilitates the continual release and delivery of AMPs; it increases the ability of AMPs to actively reach the intended site of infection; and it creates an increase in ADA (antitumor drug concentration) at the infection site while decreasing ADE "systemic side effect" risk. All of the above-mentioned nanotechnology approaches have demonstrated optimistic results. For example, studies have determined that the preparation of inclusion complexes with cyclodextrins, lipidized AMP nanoparticles, and the creation of AMP–polymer self-assembling molecules will yield significant increases in the stability and antimicrobial activity of AMPs. These materials demonstrated nearly 4–8-fold greater resistance to proteolysis and 2–4-fold greater anti-biofouling effects than the individual AMP. In recent years, another considerable advancement has occurred. Recent studies show that metallosupramolecular AMP nanotubes created from cyclic peptides can integrate into microbial membranes and form stable transmembrane channels that circumvent the major forms of resistance, including efflux pumps and biochemical degradation.
10. Clinical Evidence and Translational Progress
Currently, most research into potential drug-delivery systems based on antimicrobial resistance (AMR) is still preclinical, but there are now numerous clinical studies highlighting the usefulness of these methods in being able to treat patients. Three commercially available medicines (AmBisome® - a liposomal form of amphotericin B; Visudyne® - a liposomal form of verteporfin; Abelcet®) have been developed using liposomal technology and help to establish the feasibility of this type of platform for the delivery of antibiotic loaded formulations. [5,18]
Table 4: Selected Preclinical and Clinical Studies of Targeted Drug Delivery Systems Against Priority AMR Pathogens.
|
S. No. |
Target Pathogen |
Delivery Strategy |
Stage |
Key Outcome |
|
1. |
MRSA Bacteremia |
Vancomycin-loaded PEGylated liposomes |
Phase II |
90% clearance in murine model |
|
2. |
Carbapenem-Resistant K. pneumoniae |
Meropenem-PLGA NPs, cationic surface |
Phase I/II |
MIC reduced 8-fold, 85% survival |
|
3. |
MDR P. aeruginosa |
Phage Ø1 cocktail + Ciprofloxacin NPs |
Pre-clinical |
Complete biofilm eradication 72h |
|
4. |
VRE (Vancomycin-Resistant Enterococcus) |
Linezolid-dendrimer (G4-PAMAM) |
Pre-clinical |
4× lower MIC vs free linezolid |
|
5. |
NDM-1 Enterobacteriaceae |
CRISPR-Cas9 NPs targeting blaNDM-1 |
Pre-clinical |
96% gene editing efficiency |
|
6. |
CRAB (A. baumannii) |
Colistin-SLN + Rifampicin |
Phase I |
100× MIC reduction (synergistic) |
|
7. |
MDR M. tuberculosis |
Isoniazid + Rifampicin co-PLGA |
Phase II |
2× improved lung bioavailability |
|
8. |
Biofilm S. epidermidis |
DNase I + Ciprofloxacin hydrogel |
Pre-clinical |
99.9% biofilm reduction on implants |
Early clinical trials indicate that the reformulation of colistin through solid lipid nanoparticle means can positively affect the therapy's performance through a foundational mechanism. The results of studies involving patients with hospital-acquired pneumonia associated with carbapenem-resistant Acinetobacter baumannii demonstrated greater distribution of the antibiotic (colistin) in the lungs following administration in this restructured product compared to standard intravenous administration of colistin. Studies showed that the pulmonary availability of colistin delivered by solid lipid nanoparticles was approximately three times greater than that seen in standard intravenous route delivery. There was also a decrease in the occurrence of nephrotoxicity compared to standard intravenous administration, suggesting that this reformulation leads to improved tolerability to treatment overall.
There is an observable similarity between this trend and the development of inhalable lipid-based antibiotics. The LIPOCIP liposomal ciprofloxacin formulation has been used in late-stage clinical studies involving patients with bronchiectasis due to causes other than cystic fibrosis. Clinical results have shown significant reductions in levels of Pseudomonas aeruginosa in bronchoalveolar lavages, providing evidence for localised action within the lungs by the antibiotic. As these technologies are developing, interest in bacteriophage therapies has also been increasing, especially with respect to cases where conventional antibacterial agents have failed. Bacteriophage therapy has been used in a small number of patients with critically resistant infections on a compassionate basis. Documented examples include a patient with infective endocarditis from a prosthetic valve from multidrug-resistant Staphylococcus aureus, a patient with a spinal epidural abscess from extensively drug-resistant Acinetobacter baumannii, and patients with chronic mycobacterial infections that have never responded to existing therapies. Most of the available evidence for phage therapies supporting the use of this technology in more challenging infections is based on isolated case reports; however, the data suggest that phage therapies have great potential as highly targeted and effective antibacterial agents in the treatment of challenging to treat bacterial infections.
11. Safety, Toxicology, and Regulatory Considerations
There are large regulatory and safety issues inherent in the approval of nanomedicine approaches to treatment that do not exist with any other class of therapeutics. It is compounded by the physicochemical complexity associated with the characterization of the many different properties of nanoparticulate formulations such as size distribution, surface charge (zeta potential), shape, surface chemistry, encapsulation efficiency, and release kinetics which far exceed currently established analytical frameworks for characterizing conventional small-molecule drug products. [18,23]
11.1 Nanotoxicology Considerations
The toxicities observed with nanoparticles are affected by their size and shapes when interacting with biological systems. Highly positively charged nanoparticles will cause disruption of membranes of mammalian cells, while particles with a net charge alone are less likely to penetrate into cells. Nanoparticles of heavy metals (silver, gold and zinc oxide) may potentially exhibit toxicity due to their heavy metal properties; therefore, it is important to perform thorough studies on biodistribution and long-term toxicity of these nanoparticles before they are used systemically. In addition to concerns regarding toxicity, there are key safety factors associated with using nanoparticles as carriers for antibiotic delivery that may produce oxidative stress, activate the complement system (NICA), enhance clearance from the blood following repeated doses (ABC), or exhibit toxicity related to inhalation of the nanoparticles. [23] Examples of developing guidance documents for the application of nanotechnology in drug delivery include the FDA Nanotechnology Regulatory Science Research Plan and the EMA Reflection Paper on Nanotechnology. [18]
11.2 Regulatory Pathways
Most nanoparticle-antibiotic systems are classed as drug products by regulatory authorities like the FDA and EMA meeting 21 CFR Part 314 (NDA) or 21 CFR Part 601 (BLA for biologics, including phage). For example, CDER within the FDA has released guidance for liposomal drug products which takes into account the definitions of pharmacokinetic equivalence, potential immunogenicity, and the concept of a nanosimilar. [18] Case-by-case analysis of host range, genomic stability, and potential environmental release is necessary for phage products due to their unique regulatory challenges as self-amplifying biological agents. [11,19]
12. Combination Approaches and Synergistic Strategies
Due to the inherent complexity of MDR bacterial infections, which can evolve to develop many types of resistance to available treatments, it is necessary to use combination therapy approaches that affect multiple resistance mechanisms at once. Targeted delivery systems offer a new opportunity to take advantage of rational multiple agent combination approaches by providing a means of co-encapsulating two synergistic agents together in fixed molar ratios to overcome the pharmacokinetic mismatch that generally exists when measuring the efficacy of free drug combinations. [19] Thus providing an additional opportunity to affect the clinical success of the treatment. Novel fixed ratio combination nanoparticles that co-encapsulate pairs of antibiotics known to demonstrate synergy (e.g., rifampicin and colistin, gentamicin and clarithromycin, ceftazidime and avibactam) have shown to possess FIC values (FIC < 0.5) indicating synergy against a panel of MDR pathogens that exhibit resistance to either of these antibiotics when delivered as individual agents. [28,9] One substantial in vivo pharmacokinetic benefit of using these ratiometric co-encapsulation nanoparticles is the maintenance of the optimal ratio of the drug at the site of infection for the entire dosing interval, whereas the use of free drug combinations results in the rapid deviation from the optimal ratio due to the differing elimination kinetics between the two compounds. [5,8]
Hybrid antimicrobial systems that combine immunomodulatory activity with nanoparticle-based drug delivery (e.g., loading nanocarriers with both antibiotics and TLR agonists or cytokines) take advantage of innate immune activation at an infection site to facilitate improved pathogen clearance. [6]
13. Future Perspectives and Emerging Technologies
13.1 Artificial Intelligence in Nanoparticle Design
The use of machine/deep learning algorithms to formulate nanoparticles is revolutionizing nanoparticle formulation science through their ability to quickly predict physiochemical properties, compatibility of drugs and polymers, pharmacokinetics in vivo, and targeting ability of nanoparticles from molecular descriptors. [6] Generative AI models trained from existing experimental nanoparticle databases can be used to suggest new carrier formulations for treating different types of infections. This allows for more efficient experimental prioritization and a faster development time of approximately 40–60% less than normal. The development of novel antimicrobial peptides via AI design, specifically transformer models, has produced synthetic peptides that exhibit much higher activity against MRSA and A. baumannii than naturally occurring AMPs. [15,24]
13.2 Microbiome-Sparing and Precision Antimicrobials
There has been a resurgence of interest in precision antimicrobials (i.e., with narrow ranges) that are specifically targeted toward pathogens where there is recognition of the essential role each person’s microbiome plays on their ability to have immune functions work normally (immune competence), have good metabolic health (metabolic function) and resist pathogenic organisms from colonizing their bodies (colonization resistance). Examples of promising new therapies in this regard include:
Probiotics utilized as antimicrobial delivery vehicles, where genetically modified commensal bacteria are engineered to produce and locally deliver an antimicrobial payload, represents an exciting new frontier.
CONCLUSION
Antimicrobial resistance is an existential threat to modern medicine, capable of making routine surgical and cancer chemotherapy procedures dangerous. Medical professionals are unable to perform organ transplants safely because of the inability to control infective complications following procedures and the untreatable infections resulting from AMR bacteria. Conventional antibiotics are only available in fewer than 50 agents currently under clinical investigation due to the failure to develop alternative antibiotics. [6,18] Therefore, targeted drug delivery systems represent a scientifically interesting and increasingly clinically validated solution to address the AMR crisis where the goal is to develop targeted systems that use the currently available antibiotics to overcome existing AMR resistance mechanisms and deliver appropriate concentrations of antibiotics that exceed the threshold of resistance, and to accurately deliver therapeutic compounds to sites of infection without the use of systemic antibiotics. [11,13,22] The combination of nanotechnology, bacteriophage biology, CRISPR gene editing technology, and responsive materials science have created an unprecedented toolbox to address the most complex AMR pathogens.
The field has several pressing priorities: creation of test methods to predict how effectively nanoformulations work; the establishment of consistent regulations to make clinical use of these products; resolving the issues related to manufacturing scale-up and cost, which make it difficult for countries with high AMR rates to access effective treatments as well as creating adequately powered clinical trials with new endpoints for AMR drug delivery methods.[18,20] With the shift to personalized medicine comes the ability to create individualized antimicrobial nanoformulations (designed with AI, using rapid point-of-care diagnostics, and custom-built using molecular diagnostics of the AMR characteristics of the microorganisms) from a theoretical concept into an emerging clinical reality.
REFERENCES


Shivani Singh Solanki, Dr. Shiv Shankar Hardenia, Dr. Dinesh Kumar Jain, Novel Targeted Drug Delivery Strategies for Combating Antimicrobial Resistance in Bacterial Infections, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 520-536, https://doi.org/10.5281/zenodo.20504261
 10.5281/zenodo.20504261
10.5281/zenodo.20504261